
Characteristics of Prehospital Death in Trauma Victims

 ,
, 
Abstract
1. Introduction
- -
- trauma mechanisms,
- -
- causes of death,
- -
- injury patterns,
- -
- influence of regional trauma severity on causes of death,
- -
- trauma mechanisms, causes of death, and injury patterns in potentially survivable injuries.
2. Materials and Methods
2.1. Patients and Parameters
2.2. Statistical Analysis
3. Results
3.1. Overview of Trauma Mechanisms and Causes of Death
3.2. Overview of Injury Patterns
3.3. Overview of Injury Severity
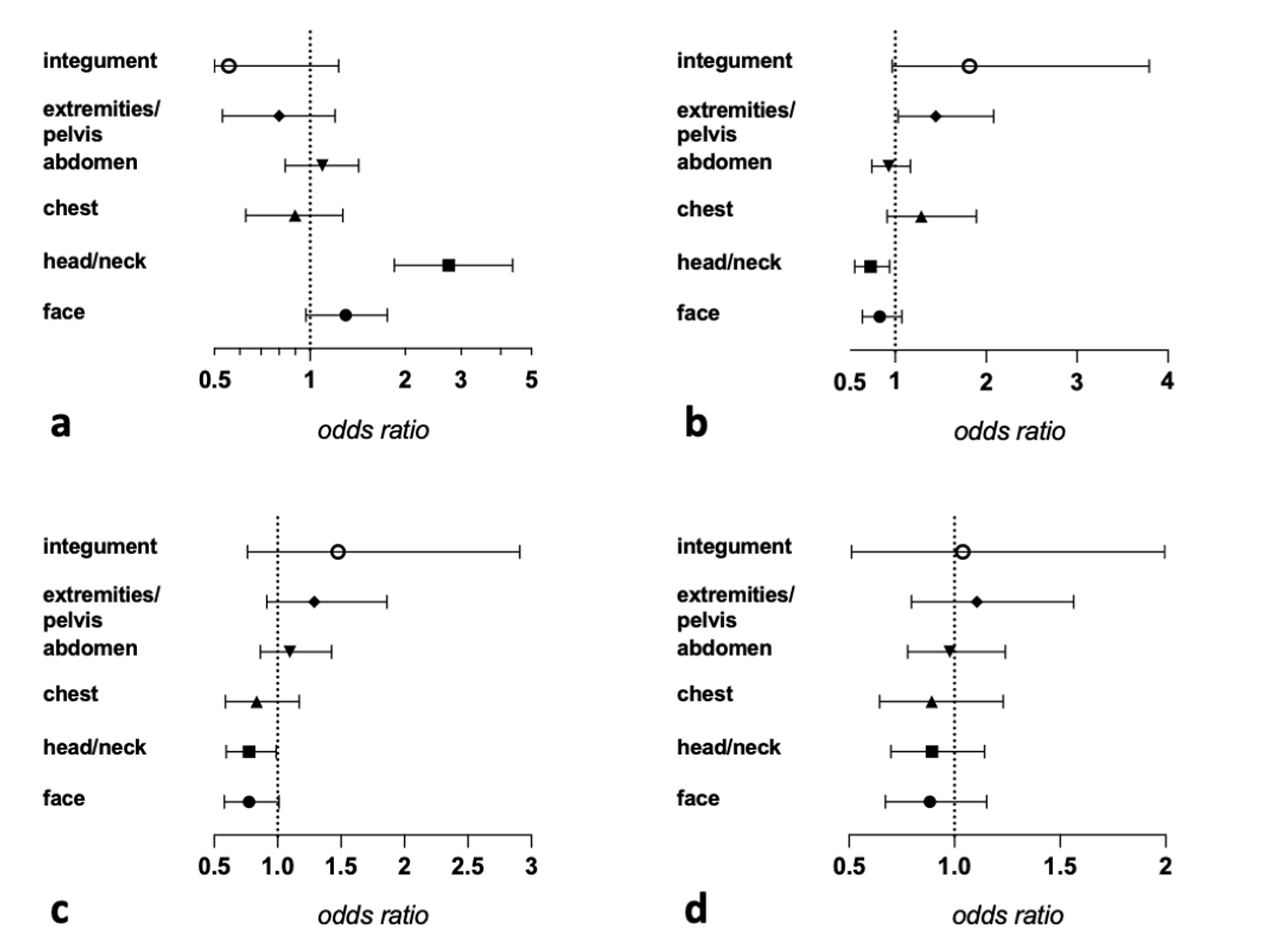
3.4. Influence of Regional Trauma Severity on Causes of Death
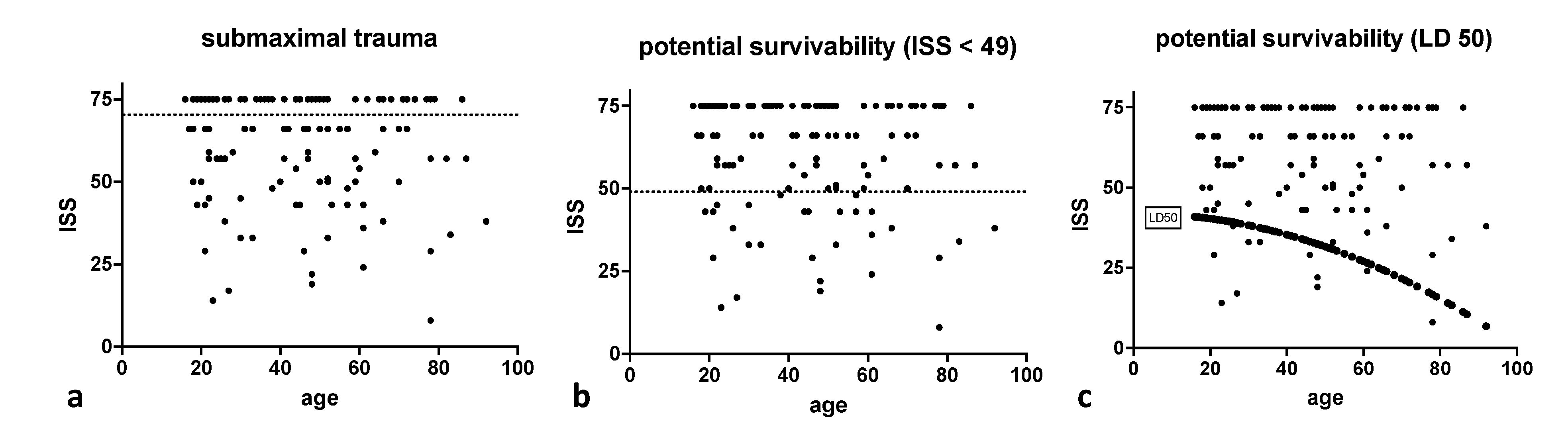
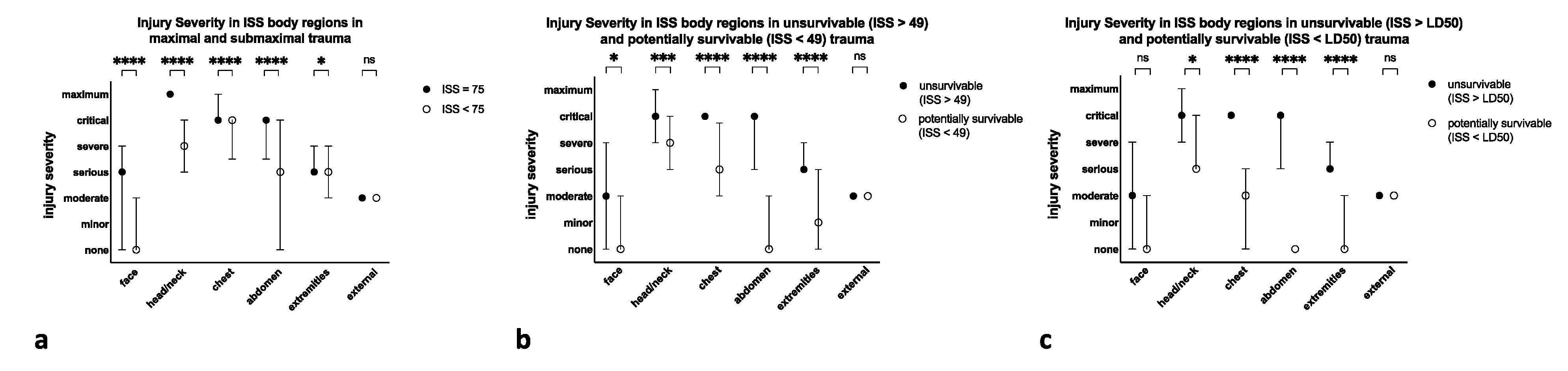
3.5. Comparison of Trauma Victims with Potentially Survivable Injuries versus Trauma Victims with Non-Survivable Injuries
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pape, H.-C.; Lefering, R.; Butcher, N.; Peitzman, A.; Leenen, L.; Marzi, I.; Lichte, P.; Josten, C.; Bouillon, B.; Schmucker, U.; et al. The definition of polytrauma revisited. J. Trauma Acute Care Surg. 2014, 77, 780–786. [Google Scholar] [CrossRef]
- Pfeifer, R.; Tarkin, I.S.; Rocos, B.; Pape, H.-C. Patterns of mortality and causes of death in polytrauma patients—Has anything changed? Injury 2009, 40, 907–911. [Google Scholar] [CrossRef]
- Butcher, N.E.; Balogh, Z.J. Update on the definition of polytrauma. Eur. J. Trauma Emerg. Surg. 2014, 40, 107–111. [Google Scholar] [CrossRef]
- Van Breugel, J.M.M.; Niemeyer, M.J.S.; Houwert, R.M.; Groenwold, R.H.H.; Leenen, L.P.H.; Van Wessem, K.J.P. Global changes in mortality rates in polytrauma patients admitted to the ICU—A systematic review. World J. Emerg. Surg. 2020, 15, 55. [Google Scholar] [CrossRef]
- El Mestoui, Z.; Jalalzadeh, H.; Giannakopoulos, G.F.; Zuidema, W.P. Incidence and etiology of mortality in polytrauma patients in a Dutch level I trauma center. Eur. J. Emerg. Med. 2017, 24, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Pfeifer, R.; Teuben, M.; Andruszkow, H.; Barkatali, B.M.; Pape, H.-C. Mortality Patterns in Patients with Multiple Trauma: A Systematic Review of Autopsy Studies. PLoS ONE 2016, 11, e0148844. [Google Scholar] [CrossRef] [PubMed]
- Gedeborg, R.; Chen, L.-H.; Thiblin, I.; Byberg, L.; Melhus, H.; Michaëlsson, K.; Warner, M. Prehospital injury deaths—Strengthening the case for prevention. J. Trauma Inj. Infect. Crit. Care 2012, 72, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.P.; O’Neill, B.; Haddon, W., Jr.; Long, W.B. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma Acute Care Surg. 1974, 14, 187–196. [Google Scholar] [CrossRef]
- Palmer, C. Major Trauma and the Injury Severity Score—Where Should We Set the Bar? Annu. Proc. Assoc. Adv. Automot. Med. 2007, 51, 13–29. [Google Scholar] [PubMed]
- Copes, W.S.; Champion, H.R.; Sacco, W.J.; Lawnick, M.M.; Keast, S.L.; Bain, L.W. The Injury Severity Score Revisited. J. Trauma Inj. Infect. Crit. Care 1988, 28, 69–77. [Google Scholar] [CrossRef]
- Lansink, K.W.W.; Gunning, A.C.; Leenen, L.P.H. Cause of death and time of death distribution of trauma patients in a Level I trauma centre in the Netherlands. Eur. J. Trauma Emerg. Surg. 2013, 39, 375–383. [Google Scholar] [CrossRef]
- Søreide, K.; Krüger, A.J.; Vårdal, A.L.; Ellingsen, C.L.; Søreide, E.; Lossius, H.M. Epidemiology and Contemporary Patterns of Trauma Deaths: Changing Place, Similar Pace, Older Face. World J. Surg. 2007, 31, 2092–2103. [Google Scholar] [CrossRef]
- Chiara, O.; Scott, J.D.; Cimbanassi, S.; Marini, A.; Zoia, R.; Rodriguez, A.; Scalea, T. Trauma deaths in an Italian urban area: An audit of pre-hospital and in-hospital trauma care. Injury 2002, 33, 553–562. [Google Scholar] [CrossRef]
- Sampalis, J.S.; Boukas, S.; Nikolis, A.; Lavoie, A. Preventable death classification: Interrater reliability and comparison with ISS-based survival probability estimates. Accid. Anal. Prev. 1995, 27, 199–206. [Google Scholar] [CrossRef]
- Bull, J.; Dickson, G. Injury scoring by TRISS and ISS/Age. Injury 1991, 22, 127–131. [Google Scholar] [CrossRef]
- Donchin, Y.; Rivkind, A.I.; Bar-Ziv, J.; Hiss, J.; Almog, J.; Drescher, M. Utility of postmortem computed tomography in trauma victims. J. Trauma Inj. Infect. Crit. Care 1994, 37, 552–556. [Google Scholar] [CrossRef]
- Jalalzadeh, H.; Giannakopoulos, G.F.; Berger, F.H.; Fronczek, J.; van de Goot, F.R.; Reijnders, U.J.; Zuidema, W.P. Post-mortem imaging compared with autopsy in trauma victims—A systematic review. Forensic Sci. Int. 2015, 257, 29–48. [Google Scholar] [CrossRef] [PubMed]
- Scholing, M.; Saltzherr, T.P.; Jin, P.H.P.F.K.; Ponsen, K.J.; Reitsma, J.B.; Lameris, J.S.; Goslings, J.C. The value of postmortem computed tomography as an alternative for autopsy in trauma victims: A systematic review. Eur. Radiol. 2009, 19, 2333–2341. [Google Scholar] [CrossRef]
- Davis, J.S.; Satahoo, S.S.; Butler, F.K.; Dermer, H.; Naranjo, D.; Julien, K.; Van Haren, R.M.; Namias, N.; Blackbourne, L.H.; Schulman, C.I. An analysis of prehospital deaths. J. Trauma Acute Care Surg. 2014, 77, 213–218. [Google Scholar] [CrossRef]
- Ryan, M.; Stella, J.; Chiu, H.; Ragg, M. Injury patterns and preventability in prehospital motor vehicle crash fatalities in Victoria. Emerg. Med. Australas. 2004, 16, 274–279. [Google Scholar] [CrossRef]
- Limb, D.; McGowan, A.; Fairfield, J.E.; Pigott, T.J. Prehospital deaths in the Yorkshire Health Region. Emerg. Med. J. 1996, 13, 248–250. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Papadopoulos, I.N.; Bukis, D.; Karalas, E.; Katsaragakis, S.; Stergiopoulos, S.; Peros, G.; Androulakis, G. Preventable Prehospital Trauma Deaths in a Hellenic Urban Health Region. J. Trauma Inj. Infect. Crit. Care 1996, 41, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Hussain, L.M.; Redmond, A.D. Are pre-hospital deaths from accidental injury preventable? BMJ 1994, 308, 1077–1080. [Google Scholar] [CrossRef]
- Stocchetti, N.; Pagliarini, G.; Gennari, M.; Baldi, G.; Banchini, E.; Campari, M.; Bacchi, M.; Zuccoli, P. Trauma care in Italy: Evidence of in-hospital preventable deaths. J. Trauma Inj. Infect. Crit. Care 1994, 36, 401–405. [Google Scholar] [CrossRef]
- Pfeifer, R.; Schick, S.; Holzmann, C.; Graw, M.; Teuben, M.; Pape, H.-C. Analysis of Injury and Mortality Patterns in Deceased Patients with Road Traffic Injuries: An Autopsy Study. World J. Surg. 2017, 41, 3111–3119. [Google Scholar] [CrossRef]
- Falconer, J. Preventability of pre-hospital trauma deaths in southern New Zealand. N. Z. Med. J. 2010, 123, 11–19. [Google Scholar] [PubMed]
- Berbiglia, L.; Lopez, P.P.; Bair, L.; Ammon, A.; Navas, G.; Keller, M.; Diebel, L.N. Patterns of early mortality after trauma in a neighborhood urban trauma center: Can we improve outcomes? Am. Surg. 2013, 79, 764–767. [Google Scholar] [CrossRef] [PubMed]
- Holcomb, J.B.; Tilley, B.C.; Baraniuk, S.; Fox, E.E.; Wade, C.E.; Podbielski, J.M.; Del Junco, D.J.; Brasel, K.J.; Bulger, E.M.; Callcut, R.A.; et al. Transfusion of Plasma, Platelets, and Red Blood Cells in a 1:1:1 vs. a 1:1:2 Ratio and Mortality in Patients with Severe Trauma. JAMA 2015, 313, 471–482. [Google Scholar] [CrossRef]
- Laudi, S.; Donaubauer, B.; Busch, T.; Kerner, T.; Bercker, S.; Bail, H.; Feldheiser, A.; Haas, N.; Kaisers, U. Low incidence of multiple organ failure after major trauma. Injury 2007, 38, 1052–1058. [Google Scholar] [CrossRef]
- Paffrath, T.; Lefering, R.; Flohe, S. How to define severely injured patients?—An Injury Severity Score (ISS) based approach alone is not sufficient. Injury 2014, 45, S64–S69. [Google Scholar] [CrossRef]
- Chiang, W.-K.; Huang, S.-T.; Chang, W.; Huang, M.-Y.; Chien, D.-K.; Tsai, C.-H. Mortality Factors Regarding the Injury Severity Score in Elderly Trauma Patients. Int. J. Gerontol. 2012, 6, 192–195. [Google Scholar] [CrossRef]
- Deng, Q.; Tang, B.; Xue, C.; Liu, Y.; Liu, X.; Lv, Y.; Zhang, L. Comparison of the Ability to Predict Mortality between the Injury Severity Score and the New Injury Severity Score: A Meta-Analysis. Int. J. Environ. Res. Public Health 2016, 13, 825. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Mean Age (SD, IQR) | n f/m (%) | Median ISS (Q1, Q3) | n CNS Injury (%) | n Exsanguination (%) | n Airway Compromise (%) | n MOF (%) | |
|---|---|---|---|---|---|---|---|---|
| Overall | 130 | 45.3 (19.49, 32.75) | 34/96 (26.15/73.85) | 66 (50, 75) | 67 (51.54) | 54 (41.54) | 41 (31.54) | 38 (29.23) |
| MVA | 70 | 48.48 (20.4, 32.00) | 16/54 (22.9/77.1) | 66 (54.75, 75) | 36 (51.4) | 32 (45.7) | 20 (28.6) | 22 (31.4) |
| Suicide | 23 | 40.48 (17.06, 23.5) | 11/12 (47.8/52.2) | 75 (62.5, 75) | 12 (52.2) | 10 (43.5) | 10 (43.5) | 6 (26.1) |
| Industrial/ workspace | 12 | 42.25 (14.06, 22.25) | 0/12 (0/100) | 62.5 (47.75, 75) | 10 (83.3) | 4 (33.3) | 4 (33.3) | 4 (33.3) |
| Sports | 9 | 36.11 (15.99, 27) | 3/6 (33.3/66.7) | 50 (43, 66) | 1 (11.1) | 4 (44.4) | 2 (22.2) | 5 (55.6) |
| Agriculture | 3 | 64 (17.78, 17) | 1/2 (33.3/66.7) | 57 (53.5, 66) | 1 (33.3) | 1 (33.3) | 1 (33.3) | 1 (33.3) |
| n (%) | Median Total ISS (Q1, Q3) | Median ISS Head/Neck (Q1, Q3) | Median ISS face (Q1, Q3) | Median ISS Chest (Q1, Q3) | Median ISS Abdomen (Q1, Q3) | Median ISS Pelvis/Extremities (Q1, Q3) | Median ISS External (Q1, Q3) | |
|---|---|---|---|---|---|---|---|---|
| Overall | 130 | 66 (50, 75) | 5 (3.25, 6) | 1 (0, 3) | 5 (4, 5) | 4 (0, 5) | 3 (2, 4) | 2 (2, 2) |
| MVA | 70 (54) | 66 (54.75, 75) | 4 (4, 6) | 2 (0, 3.75) | 5 (4, 6) | 4 (0, 5) | 3 (2, 4) | 2 (2, 2) |
| Suicide | 23 (18) | 75 (62.5, 75) | 6 (3.5, 6) | 2 (0, 4) | 5 (4, 5) | 5 (3, 5) | 3 (3, 4) | 2 (2, 2) |
| Workspace | 12 (9) | 62.5 (47.75, 75) | 5 (3, 6) | 0 (0, 2.25) | 5 (3.75, 5) | 5 (4.25, 5) | 3 (0, 4) | 2 (2, 2) |
| Sports | 9 (7) | 50 (43, 66) | 4 (3, 5) | 1 (0, 3) | 5 (4, 5) | 0 (0, 5) | 3 (2, 3) | 2 (2, 2) |
| Agriculture | 3 (2) | 57 (53.5, 66) | 3 (1.5, 4.5) | 0 (0, 0.5) | 5 (5, 5) | 4 (3, 4.5) | 4 (3.5, 4) | 2 (2, 2) |
| CNS injury | 67 (52) | 75 (57, 75) | 6 (5, 6) | 2 (0, 4) | 5 (4, 5) | 5 (1, 5) | 3 (2, 4) | 2 (2, 2) |
| Exsanguination | 54 (42) | 66 (57, 75) | 4 (3, 5) | 0 (0, 2.75) | 5 (5, 6) | 4 (3, 5) | 3 (3, 4) | 2 (2, 2) |
| Airway compromise | 41 (32) | 59 (50, 66) | 4 (3, 5) | 0 (0, 2) | 5 (5, 5) | 4 (3, 5) | 3 (2, 4) | 2 (2, 2) |
| MOF | 38 (29) | 61.5 (43, 75) | 4 (3, 5) | 0 (0, 2) | 5 (4, 5) | 3 (0.5, 5) | 3 (2, 4) | 2 (2, 2) |
| Overall (%) | ISS < 75 | ISS 75 | p-Value | ISS < 49 | ISS > 49 | p-Value | ISS < LD50 | ISS > LD50 | p-Value | |
| Median ISS | 66 | 54 | 75 | 37 | 75 | 24 | 66 | |||
| Mean age | 46 | 47 | 44 | 0.664 | 47 | 45.5 | 0.626 | 33 | 47 | 0.403 |
| n female/male (%) | 34/96 (26.15/73.85) | 21/52 (28.8/71.2) | 13/44 (22.8/77.2) | 0.443 | 9/19 (32.1/67.9) | 25/77 (24.5/76) | 0.568 | 4/7 (36.4/63.6) | 30/89 (25.2/75) | 0.477 |
| n MVA (%) | 70 (54) | 38 (52.1) | 32 (56.1) | 0.643 | 13 (46.4) | 57 (55.9) | 0.374 | 4 (36.4) | 66 (55.5) | 0.224 |
| n suicide (%) | 23 (18) | 9 (12.3) | 14 (24.6) | 0.07 | 3 (10.7) | 20 (19.6) | 0.403 | 1 (9.1) | 22 (18.5) | 0.435 |
| n workspace (%) | 12 (9) | 8 (11) | 4 (7) | 0.441 | 3 (10.7) | 9 (8.8) | 0.721 | 1 (9.1) | 11 (9.2) | 1 |
| n sports (%) | 9 (7) | 8 (11) | 1 (1.8) | 0.077 | 4 (14.3) | 5 (4.9) | 0.1 | 2 (18.2) | 7 (5.9) | 0.169 |
| n agriculture (%) | 3 (2) | 2 (2.7) | 1 (1.8) | 1 | 0 (0) | 3 (2.9) | 1 | 0 | 3 (2.5) | 1 |
| n CNS injury (%) | 67 (52) | 27 (37) | 40 (70.2) | <0.001 | 10 (35.7) | 57 (55.9) | 0.059 | 5 (45.5) | 62 (52.1) | 0.673 |
| n exsanguination (%) | 54 (42) | 32 (43.8) | 22 (38.6) | 0.548 | 9 (32.1) | 45 (44.1) | 0.255 | 3 (27.3) | 51 (42.9) | 0.36 |
| n airway compromise (%) | 41 (32) | 33 (45.2) | 8 (14) | <0.001 | 9 (32.1) | 32 (31.4) | 0.938 | 5 (45.5) | 36 (30.3) | 0.321 |
| n MOF (%) | 38 (29) | 26 (35.6) | 12 (21.1) | 0.07 | 14 (50) | 24 (23.5) | 0.007 | 3 (27.3) | 35 (29.4) | 1 |
| Overall | ISS < 75 | ISS 75 | p-Value | ISS < 49 | ISS > 49 | p-Value | ISS < LD50 | ISS > LD50 | p-Value | |
| Face | 1 (0, 3) | 0 (0, 2) | 3 (0, 4) | <0.001 | 0 (0, 2) | 2 (0, 4) | 0.03 | 0 (0, 1.5) | 2 (0, 4) | 0.148 |
| Head/neck | 5 (3.25, 6) | 4 (3, 5) | 6 (6, 6) | <0.001 | 4 (3, 5) | 5 (4, 6) | <0.001 | 3 (3, 5) | 5 (4, 6) | 0.024 |
| Chest | 5 (4, 5) | 5 (4, 5) | 5 (5, 6) | <0.001 | 3 (2, 4.5) | 5 (5, 5) | <0.001 | 2 (0, 2.5) | 5 (5, 5) | <0.001 |
| Abdomen | 4 (0, 5) | 3 (0, 5) | 5 (4, 5) | <0.001 | 0 (0, 2) | 5 (3, 5) | <0.001 | 0 (0, 0) | 5 (3, 5) | <0.001 |
| Pelvis and extremities | 3 (2, 4) | 3 (2, 4) | 3 (3, 4) | 0.022 | 1 (0, 3) | 3 (3, 4) | <0.001 | 0 (0, 2) | 3 (3, 4) | <0.001 |
| External | 2 (2, 2) | 2 (2, 2) | 2 (2, 2) | 0.155 | 2 (2, 2) | 2 (2, 2) | 0.962 | 2 (2, 2) | 2 (2, 2) | 0.122 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gewiess, J.; Albers, C.E.; Pape, H.-C.; Bangerter, H.; Zech, W.-D.; Keel, M.J.B.; Bastian, J.D. Characteristics of Prehospital Death in Trauma Victims. J. Clin. Med. 2021, 10, 4765. https://doi.org/10.3390/jcm10204765
Gewiess J, Albers CE, Pape H-C, Bangerter H, Zech W-D, Keel MJB, Bastian JD. Characteristics of Prehospital Death in Trauma Victims. Journal of Clinical Medicine. 2021; 10(20):4765. https://doi.org/10.3390/jcm10204765
Chicago/Turabian StyleGewiess, Jan, Christoph Emanuel Albers, Hans-Christoph Pape, Hannes Bangerter, Wolf-Dieter Zech, Marius Johann Baptist Keel, and Johannes Dominik Bastian. 2021. "Characteristics of Prehospital Death in Trauma Victims" Journal of Clinical Medicine 10, no. 20: 4765. https://doi.org/10.3390/jcm10204765
APA StyleGewiess, J., Albers, C. E., Pape, H.-C., Bangerter, H., Zech, W.-D., Keel, M. J. B., & Bastian, J. D. (2021). Characteristics of Prehospital Death in Trauma Victims. Journal of Clinical Medicine, 10(20), 4765. https://doi.org/10.3390/jcm10204765