High Integrity and Fidelity of Long-Term Cryopreserved Umbilical Cord Blood for Transplantation

 ,
,
Abstract
1. Introduction
2. Experimental Section
2.1. Collection, Cryopreservation, and Separation of UCB Cells
2.2. Hematological Cell Counts and Enumeration of CD34+ Cells
2.3. Cell Viability Evaluation
2.4. Frequencies of Cell Types in UCB
2.5. Statistical Analysis
3. Results
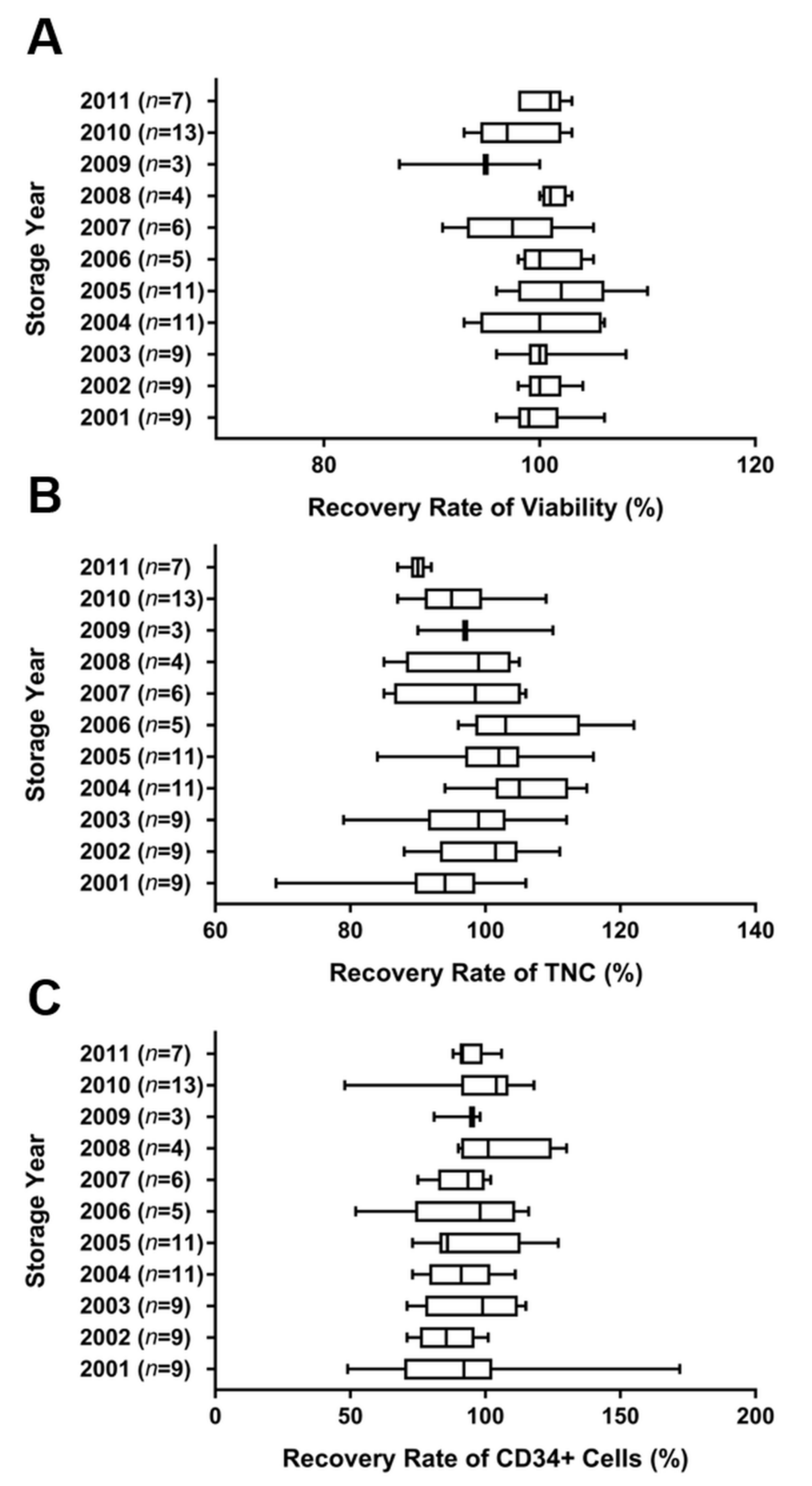
3.1. Recovery of Viability, TNCs, and Total CD34+ Cells from Cryopreserved UCB
3.2. Long-Term Storage Stability (from 1 to 10 Years)
3.3. Population of MNCs Isolated in Cryopreserved and Fresh UCB
3.4. Comparison of MNC Viability in Cryopreserved and Fresh UCB
3.5. Characteristics of Store CB Units Used for Transplantation
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, B.; Yoo, K.H.; Kim, C. Hematopoietic stem cell expansion and generation: The ways to make a breakthrough. Blood Res. 2015, 50, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Alkindi, S.; Dennison, D. Umbilical Cord Blood Banking and Transplantation: A short review. Sultan Qaboos Univ. Med. J. 2011, 11, 455–461. [Google Scholar] [PubMed]
- Sanz, J.; Veys, P.; Rocha, V. Umbilical Cord Blood Transplantation in Children and Adults. In The EBMT Handbook: Hematopoietic Stem Cell Transplantation and Cellular Therapies; Carreras, E., Dufour, C., Mohty, M., Kroger, N., Eds.; Springer Nature: Cham, Switzerland, 2019; pp. 473–478. [Google Scholar] [CrossRef]
- Mayani, H.; Wagner, J.E.; Broxmeyer, H.E. Cord blood research, banking, and transplantation: Achievements, challenges, and perspectives. Bone Marrow Transpl. 2020, 55, 48–61. [Google Scholar] [CrossRef] [PubMed]
- Rosenau, E.H.; Sugrue, M.W.; Haller, M.; Fisk, D.; Kelly, S.S.; Chang, M.; Hou, W.; Eldjerou, L.; Slayton, W.; Cogle, C.R.; et al. Characteristics of thawed autologous umbilical cord blood. Transfusion 2012, 52, 2234–2242. [Google Scholar] [CrossRef]
- Arutyunyan, I.; Fatkhudinov, T.; Sukhikh, G. Umbilical cord tissue cryopreservation: A short review. Stem Cell Res. Ther. 2018, 9, 236. [Google Scholar] [CrossRef]
- Jiang, X.S.; Chai, C.; Zhang, Y.; Zhuo, R.X.; Mao, H.Q.; Leong, K.W. Surface-immobilization of adhesion peptides on substrate for ex vivo expansion of cryopreserved umbilical cord blood CD34+ cells. Biomaterials 2006, 27, 2723–2732. [Google Scholar] [CrossRef]
- Waller-Wise, R. Umbilical cord blood: Information for childbirth educators. J. Perinat. Educ. 2011, 20, 54–60. [Google Scholar] [CrossRef]
- Moise, K.J., Jr. Umbilical cord stem cells. Obstet. Gynecol. 2005, 106, 1393–1407. [Google Scholar] [CrossRef]
- Wall, D.A. Issues in the quality of umbilical cord blood stem cells for transplantation: Challenges in cord blood banking quality management. Transfusion 2005, 45, 826–828. [Google Scholar] [CrossRef]
- Querol, S.; Gomez, S.G.; Pagliuca, A.; Torrabadella, M.; Madrigal, J.A. Quality rather than quantity: The cord blood bank dilemma. Bone Marrow Transpl. 2010, 45, 970–978. [Google Scholar] [CrossRef][Green Version]
- Yang, H.; Loutfy, M.R.; Mayerhofer, S.; Shuen, P. Factors affecting banking quality of umbilical cord blood for transplantation. Transfusion 2011, 51, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Broxmeyer, H.E.; Srour, E.F.; Hangoc, G.; Cooper, S.; Anderson, S.A.; Bodine, D.M. High-efficiency recovery of functional hematopoietic progenitor and stem cells from human cord blood cryopreserved for 15 years. Proc. Natl. Acad. Sci. USA 2003, 100, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.J.; Lee, H.J.; Heo, J.; Lim, J.; Kim, M.; Kim, M.K.; Nam, H.Y.; Hong, G.H.; Cho, Y.S.; Choi, S.J.; et al. Senescence-Associated MCP-1 Secretion Is Dependent on a Decline in BMI1 in Human Mesenchymal Stromal Cells. Antioxid. Redox Signal. 2016, 24, 471–485. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, P.; Dobrila, L.; Rosenfield, R.E.; Adamson, J.W.; Migliaccio, G.; Migliaccio, A.R.; Taylor, P.E.; Stevens, C.E. Processing and cryopreservation of placental/umbilical cord blood for unrelated bone marrow reconstitution. Proc. Natl. Acad. Sci. USA 1995, 92, 10119–10122. [Google Scholar] [CrossRef]
- Butler, M.G.; Menitove, J.E. Umbilical cord blood banking: An update. J. Assist. Reprod. Genet. 2011, 28, 669–676. [Google Scholar] [CrossRef]
- Cohen, Y.C.; Scaradavou, A.; Stevens, C.E.; Rubinstein, P.; Gluckman, E.; Rocha, V.; Horowitz, M.M.; Eapen, M.; Nagler, A.; Shpall, E.J.; et al. Factors affecting mortality following myeloablative cord blood transplantation in adults: A pooled analysis of three international registries. Bone Marrow Transpl. 2011, 46, 70–76. [Google Scholar] [CrossRef]
- Allan, D.; Petraszko, T.; Elmoazzen, H.; Smith, S. A review of factors influencing the banking of collected umbilical cord blood units. Stem Cells Int. 2013, 2013, 463031. [Google Scholar] [CrossRef]
- Goodwin, H.S.; Grunzinger, L.M.; Regan, D.M.; McCormick, K.A.; Johnson, C.E.; Oliver, D.A.; Mueckl, K.A.; Alonso, J.M., 3rd; Wall, D.A. Long term cryostorage of UC blood units: Ability of the integral segment to confirm both identity and hematopoietic potential. Cytotherapy 2003, 5, 80–86. [Google Scholar] [CrossRef]
- Thyagarajan, B.; Berger, M.; Sumstad, D.; McKenna, D.H., Jr. Loss of integrity of umbilical cord blood unit freezing bags: Description and consequences. Transfusion 2008, 48, 1138–1142. [Google Scholar] [CrossRef]
- Broxmeyer, H.E.; Cooper, S. High-efficiency recovery of immature haematopoietic progenitor cells with extensive proliferative capacity from human cord blood cryopreserved for 10 years. Clin. Exp. Immunol. 1997, 107, 45–53. [Google Scholar]
- Broxmeyer, H.E.; Lee, M.R.; Hangoc, G.; Cooper, S.; Prasain, N.; Kim, Y.J.; Mallett, C.; Ye, Z.; Witting, S.; Cornetta, K.; et al. Hematopoietic stem/progenitor cells, generation of induced pluripotent stem cells, and isolation of endothelial progenitors from 21- to 23.5-year cryopreserved cord blood. Blood 2011, 117, 4773–4777. [Google Scholar] [CrossRef]
- Saha, A.; Buntz, S.; Scotland, P.; Xu, L.; Noeldner, P.; Patel, S.; Wollish, A.; Gunaratne, A.; Gentry, T.; Troy, J.; et al. A cord blood monocyte-derived cell therapy product accelerates brain remyelination. JCI Insight 2016, 1, e86667. [Google Scholar] [CrossRef] [PubMed]
- Than, U.T.T.; Le, H.T.; Hoang, D.H.; Nguyen, X.H.; Pham, C.T.; Bui, K.T.V.; Bui, H.T.H.; Nguyen, P.V.; Nguyen, T.D.; Do, T.T.H.; et al. Induction of Antitumor Immunity by Exosomes Isolated from Cryopreserved Cord Blood Monocyte-Derived Dendritic Cells. Int. J. Mol. Sci. 2020, 21, 1834. [Google Scholar] [CrossRef] [PubMed]
- Roh, E.Y.; Oh, S.; Yoon, J.H.; Kim, B.J.; Song, E.Y.; Shin, S. Umbilical Cord Blood Units Cryopreserved in the Public Cord Blood Bank: A Breakthrough in iPSC Haplobanking? Cell Transpl. 2020, 29, 963689720926151. [Google Scholar] [CrossRef] [PubMed]
- Haller, M.J.; Wasserfall, C.H.; Hulme, M.A.; Cintron, M.; Brusko, T.M.; McGrail, K.M.; Sumrall, T.M.; Wingard, J.R.; Theriaque, D.W.; Shuster, J.J.; et al. Autologous umbilical cord blood transfusion in young children with type 1 diabetes fails to preserve C-peptide. Diabetes Care 2011, 34, 2567–2569. [Google Scholar] [CrossRef] [PubMed]
- Haller, M.J.; Wasserfall, C.H.; Hulme, M.A.; Cintron, M.; Brusko, T.M.; McGrail, K.M.; Wingard, J.R.; Theriaque, D.W.; Shuster, J.J.; Ferguson, R.J.; et al. Autologous umbilical cord blood infusion followed by oral docosahexaenoic acid and vitamin D supplementation for C-peptide preservation in children with Type 1 diabetes. Biol. Blood Marrow Transpl. 2013, 19, 1126–1129. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.S.; Rao, M.S.; Brown, H.L. The Future State of Newborn Stem Cell Banking. J. Clin. Med. 2019, 8, 117. [Google Scholar] [CrossRef]
- Migliaccio, A.R.; Adamson, J.W.; Stevens, C.E.; Dobrila, N.L.; Carrier, C.M.; Rubinstein, P. Cell dose and speed of engraftment in placental/umbilical cord blood transplantation: Graft progenitor cell content is a better predictor than nucleated cell quantity. Blood 2000, 96, 2717–2722. [Google Scholar] [CrossRef]
- Purtill, D.; Smith, K.; Devlin, S.; Meagher, R.; Tonon, J.; Lubin, M.; Ponce, D.M.; Giralt, S.; Kernan, N.A.; Scaradavou, A.; et al. Dominant unit CD34+ cell dose predicts engraftment after double-unit cord blood transplantation and is influenced by bank practice. Blood 2014, 124, 2905–2912. [Google Scholar] [CrossRef]
- Barker, J.N.; Scaradavou, A.; Stevens, C.E. Combined effect of total nucleated cell dose and HLA match on transplantation outcome in 1061 cord blood recipients with hematologic malignancies. Blood 2010, 115, 1843–1849. [Google Scholar] [CrossRef]
- Nikiforow, S.; Li, S.; Snow, K.; Liney, D.; Kao, G.S.; Haspel, R.; Shpall, E.J.; Glotzbecker, B.; Sica, R.A.; Armand, P.; et al. Lack of impact of umbilical cord blood unit processing techniques on clinical outcomes in adult double cord blood transplant recipients. Cytotherapy 2017, 19, 272–284. [Google Scholar] [CrossRef] [PubMed]
- Ballen, K.K.; Logan, B.R.; Laughlin, M.J.; He, W.; Ambruso, D.R.; Armitage, S.E.; Beddard, R.L.; Bhatla, D.; Hwang, W.Y.; Kiss, J.E.; et al. Effect of cord blood processing on transplantation outcomes after single myeloablative umbilical cord blood transplantation. Biol. Blood Marrow Transpl. 2015, 21, 688–695. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.; Wagner, J.E.; Brunstein, C.G.; Cao, Q.; McKenna, D.H.; Lund, T.C.; Verneris, M.R. Impact of long-term cryopreservation on single umbilical cord blood transplantation outcomes. Biol. Blood Marrow Transpl. 2015, 21, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Wall, D.A. Regulatory issues in cord blood banking and transplantation. Best Pract. Res. Clin. Haematol. 2010, 23, 171–177. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Storage Duration (Years) | Total Check Point (Annual) | Recovery Rate of Viability (%) | Recovery Rate of TNCs (%) | Recovery Rate of CD34+ Cells (%) |
|---|---|---|---|---|
| 10 | 3 | 94.6 ± 1.0 | 80.5 ± 2.7 | 66.0 ± 14.9 |
| 9 | 7 | 93.4 ± 3.3 | 80.9 ± 4.6 | 81.0 ± 19.4 |
| 8 | 12 | 96.5 ± 4.3 | 80.7 ± 4.4 | 80.8 ± 22.9 |
| 7 | 16 | 96.2 ± 4.6 | 82.3 ± 4.3 | 82.7 ± 18.7 |
| 6 | 20 | 96.6 ± 4.1 | 84.7 ± 5.1 | 83.9 ± 18.0 |
| 5 | 24 | 96.2 ± 4.0 | 86.8 ± 4.9 | 78.0 ± 22.2 |
| 4 | 28 | 96.7 ± 3.5 | 85.9 ± 9.4 | 80.2 ± 20.6 |
| 3 | 32 | 96.8 ± 3.6 | 87.0 ± 7.2 | 81.9 ± 23.5 |
| 2 | 36 | 97.5 ± 3.6 | 87.9 ± 6.7 | 82.5 ± 17.7 |
| 1 | 37 | 96.7 ± 4.9 | 89.4 ± 6.9 | 86.0 ± 17.4 |
| Total | 215 | 96.6 ± 4.0 | 86.2 ± 7.0 | 82.0 ± 19.8 |
| Storage Year | n | CD45+ Lymphocytes | CD14+ Monocyte | CD34+ HSCs | CD45+/CD3+ T Cells | CD45+/CD19+ B Cells | CD56+ Im/m NK Cells |
|---|---|---|---|---|---|---|---|
| 2000 | 10 | 90.8 ± 3.6 | 9.0 ±5.7 | 0.6 ± 0.5 | 46.2 ± 16.8 | 0.3 ± 0.4 | 0.3 ± 0.3 |
| 2001 | 5 | 95.1 ± 1.4 | 11.8 ± 15.8 | 0.4 ± 0.4 | 47.5 ± 11.1 | 1.3 ± 0.9 | 0.4 ± 0.1 |
| 2002 | 5 | 93.1 ± 3.9 | 10.6 ± 4.1 | 0.8 ± 1.0 | 37.1 ± 13.5 | 1.5 ± 1.6 | 0.4 ± 0.3 |
| 2003 | 4 | 92.9 ± 5.6 | 3.6 ± 2.0 | 0.4 ± 0.4 | 37.9 ± 16.2 | 1.7 ± 1.2 | 0.4 ± 0.3 |
| 2004 | 4 | 93.3 ± 5.8 | 8.0 ± 11.1 | 0.3 ± 0.2 | 36.7 ± 5.7 | 0.3 ± 0.2 | 0.1 ± 0.1 |
| 2005 | 8 | 90.6 ± 6.2 | 5.8 ± 4.8 | 0.4 ± 0.3 | 51.0 ± 12.7 | 0.4 ± 0.2 | 0.3 ± 0.4 |
| 2006 | 4 | 92.1 ± 6.2 | 5.0 ± 0.8 | 0.5 ± 0.2 | 60.5 ± 22.9 | 1.0 ± 1.2 | 1.3 ± 2.1 |
| 2007 | 4 | 94.3 ± 5.6 | 5.2 ± 4.5 | 0.2 ± 0.1 | 65.3 ± 12.9 | 1.1 ± 1.0 | 0.2 ± 0.1 |
| 2008 | 4 | 94.1 ± 2.3 | 5.1 ± 5.4 | 0.6 ± 0.4 | 35.3 ± 26.5 | 1.4 ± 1.1 | 0.1 ± 0.1 |
| 2009 | 4 | 93.7 ± 2.8 | 3.8 ± 1.5 | 0.2 ± 0.2 | 34.9 ± 14.8 | 1.2 ± 1.1 | 0.1 ± 0.1 |
| 2010 | 10 | 94.5 ± 6.2 | 12.2 ± 9.8 | 0.5 ± 0.2 | 53.9 ± 9.8 | 0.7 ± 0.6 | 0.3 ± 0.4 |
| 2011 | 4 | 94.6 ± 3.2 | 10.1 ± 12.4 | 0.2 ± 0.1 | 38.9 ± 9.3 | 0.8 ± 0.7 | 0.2 ± 0.2 |
| Total | 66 | 93.0 ± 4.7 | 8.5 ± 8.2 | 0.5 ± 0.4 | 46.4 ± 15.5 | 0.8 ± 0.8 | 0.3 ± 0.6 |
| Fresh | 6 | 98.0 ± 2.3 | 8.6 ± 4.3 | 0.6 ± 0.6 | 56.8 ± 10.0 | 1.5 ± 0.4 | 0.7 ± 0.4 |
| Parameter | Number | Range |
|---|---|---|
| CB unit cryopreservation, yr | n | - |
| ≤5 | 429 | - |
| 5.1 to 10 | 111 | - |
| 10.1 to 15 | 16 | - |
| 15.1 to 21 | 1 | - |
| TNC (×108/unit) | AVE ± SD | Range |
| Pre-TNC | 9.8 ± 3.9 | 1.1 to 32.4 |
| Post-TNC | 9.8 ± 4.0 | 1.1 to 32.2 |
| CD34+ cells (×106/unit) | AVE ± SD | Range |
| Pre-CD34+ cells | 4.1 ± 2.8 | 0.5 to 23.6 |
| Post-CD34+ cells | 3.9 ± 2.7 | 0.4 to 19.0 |
| Post-thaw viability (%) | AVE ± SD | Range |
| Viability | 83.2 ± 5.7 | 60.0 to 96.0 |
| HLA matching | n | - |
| 6/6 or 5/6 | 441 | - |
| 4/6 or less | 116 | - |
| ABO match | n | - |
| Match | 246 | - |
| Minor Mismatch | 297 | - |
| Major Mismatch | 14 | - |
| Recipient gender | n | - |
| Male | 336 | - |
| Female | 200 | - |
| Unknown | 21 | - |
| Recipient age, year | n | - |
| ≤5 | 197 | - |
| 5.1 to 10 | 155 | - |
| >10.1 | 189 | - |
| Unknown | 16 | - |
| Recipient Weight, kg | n | - |
| ≤10 | 57 | - |
| 10.1 to 30 | 225 | - |
| 30.1 to 60 | 124 | - |
| >60 | 67 | - |
| Unknown | 84 | - |
| Autologous vs. Allogenic | n | - |
| Autologous | 78 | - |
| Allogenic | 479 | - |
| Diagnosis | n | - |
| Chronic myeloid leukemia (CML) | 18 | - |
| Acute myeloid leukemia (AML) | 161 | - |
| Acute lymphoblastic leukemia (ALL) | 152 | - |
| Aplastic anemia | 26 | - |
| Hemophagocytic lymphohistiocytosis (HLH) | 11 | - |
| Cerebral palsy | 38 | - |
| Developmental disability | 34 | - |
| Others | 117 | - |
| Storage Year | Cord Blood Transplantation Year | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | Total | |
| 2000 | 3 | 2 | 4 | 5 | 4 | 1 | 3 | 1 | 1 | 24 | |||||||||||
| 2001 | 10 | 8 | 18 | 14 | 15 | 22 | 7 | 11 | 3 | 5 | 3 | 6 | 2 | 1 | 125 | ||||||
| 2002 | 1 | 3 | 3 | 5 | 2 | 2 | 2 | 4 | 4 | 1 | 27 | ||||||||||
| 2003 | 3 | 22 | 16 | 23 | 10 | 11 | 7 | 7 | 12 | 3 | 2 | 1 | 1 | 1 | 119 | ||||||
| 2004 | 8 | 18 | 32 | 13 | 7 | 9 | 11 | 2 | 2 | 2 | 3 | 1 | 108 | ||||||||
| 2005 | 1 | 14 | 15 | 7 | 3 | 8 | 1 | 1 | 1 | 51 | |||||||||||
| 2006 | 3 | 7 | 1 | 3 | 2 | 1 | 2 | 2 | 1 | 1 | 23 | ||||||||||
| 2007 | 3 | 3 | 7 | 7 | 4 | 2 | 2 | 1 | 29 | ||||||||||||
| 2008 | 3 | 2 | 1 | 1 | 7 | ||||||||||||||||
| 2009 | 1 | 3 | 1 | 1 | 6 | ||||||||||||||||
| 2010 | 1 | 3 | 3 | 2 | 1 | 10 | |||||||||||||||
| 2011 | 2 | 2 | 1 | 1 | 2 | 1 | 1 | 10 | |||||||||||||
| 2012 | 2 | 1 | 1 | 4 | |||||||||||||||||
| 2013 | 1 | 1 | 2 | 4 | |||||||||||||||||
| 2014 | 4 | 1 | 5 | ||||||||||||||||||
| 2015 | 1 | 1 | 2 | ||||||||||||||||||
| 2016 | 3 | 3 | |||||||||||||||||||
| Total | 13 | 11 | 28 | 52 | 59 | 97 | 60 | 40 | 34 | 48 | 33 | 22 | 15 | 13 | 14 | 11 | 2 | 3 | 1 | 1 | 557 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, G.-H.; Kwak, J.; Kim, S.H.; Kim, H.J.; Hong, H.K.; Jin, H.J.; Choi, S.J.; Oh, W.; Um, S. High Integrity and Fidelity of Long-Term Cryopreserved Umbilical Cord Blood for Transplantation. J. Clin. Med. 2021, 10, 293. https://doi.org/10.3390/jcm10020293
Kim G-H, Kwak J, Kim SH, Kim HJ, Hong HK, Jin HJ, Choi SJ, Oh W, Um S. High Integrity and Fidelity of Long-Term Cryopreserved Umbilical Cord Blood for Transplantation. Journal of Clinical Medicine. 2021; 10(2):293. https://doi.org/10.3390/jcm10020293
Chicago/Turabian StyleKim, Gee-Hye, Jihye Kwak, Sung Hee Kim, Hee Jung Kim, Hye Kyung Hong, Hye Jin Jin, Soo Jin Choi, Wonil Oh, and Soyoun Um. 2021. "High Integrity and Fidelity of Long-Term Cryopreserved Umbilical Cord Blood for Transplantation" Journal of Clinical Medicine 10, no. 2: 293. https://doi.org/10.3390/jcm10020293
APA StyleKim, G.-H., Kwak, J., Kim, S. H., Kim, H. J., Hong, H. K., Jin, H. J., Choi, S. J., Oh, W., & Um, S. (2021). High Integrity and Fidelity of Long-Term Cryopreserved Umbilical Cord Blood for Transplantation. Journal of Clinical Medicine, 10(2), 293. https://doi.org/10.3390/jcm10020293