
A Pilot Randomized Controlled Trial of Effect of Genioglossus Muscle Strengthening on Obstructive Sleep Apnea Outcomes

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
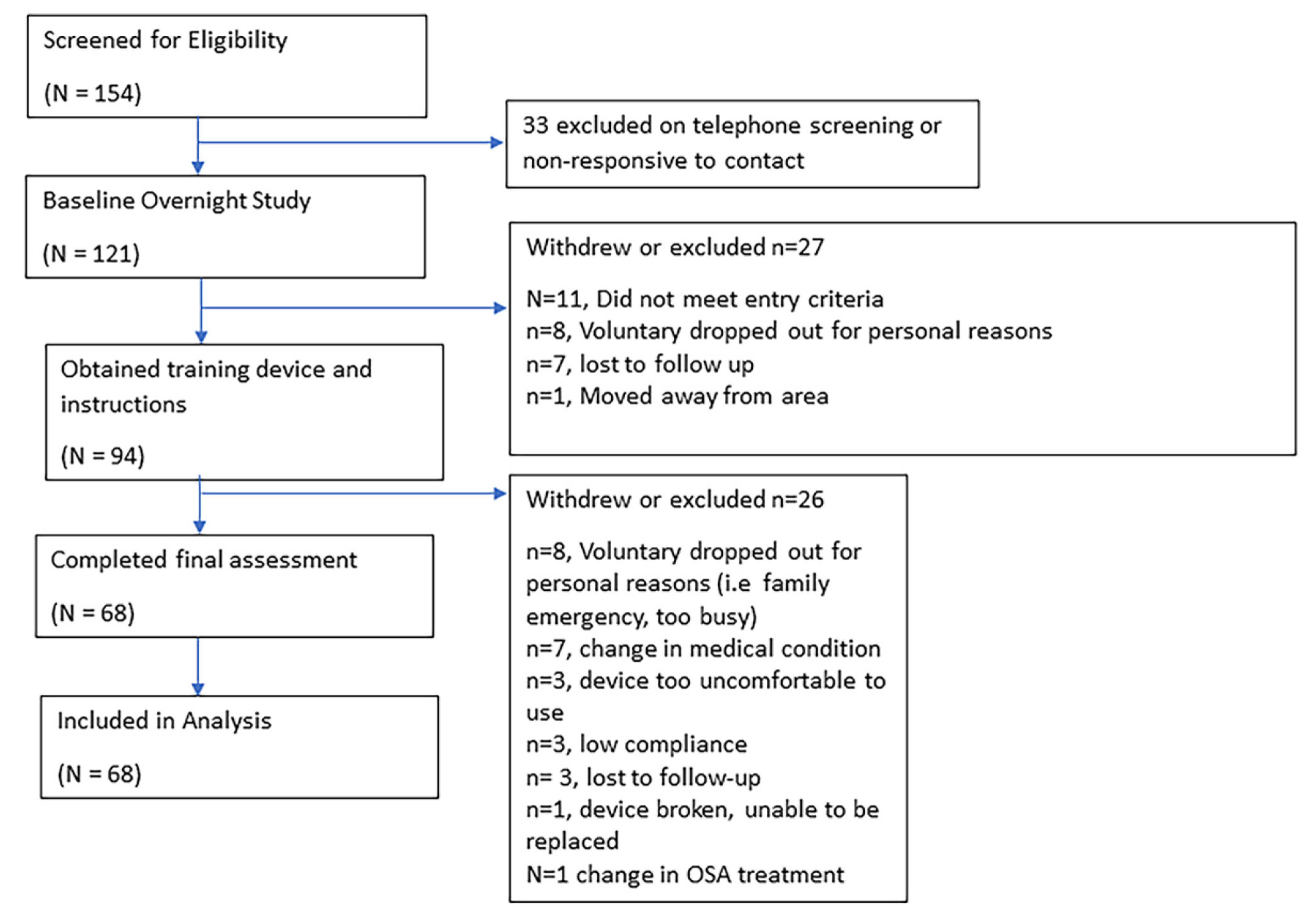
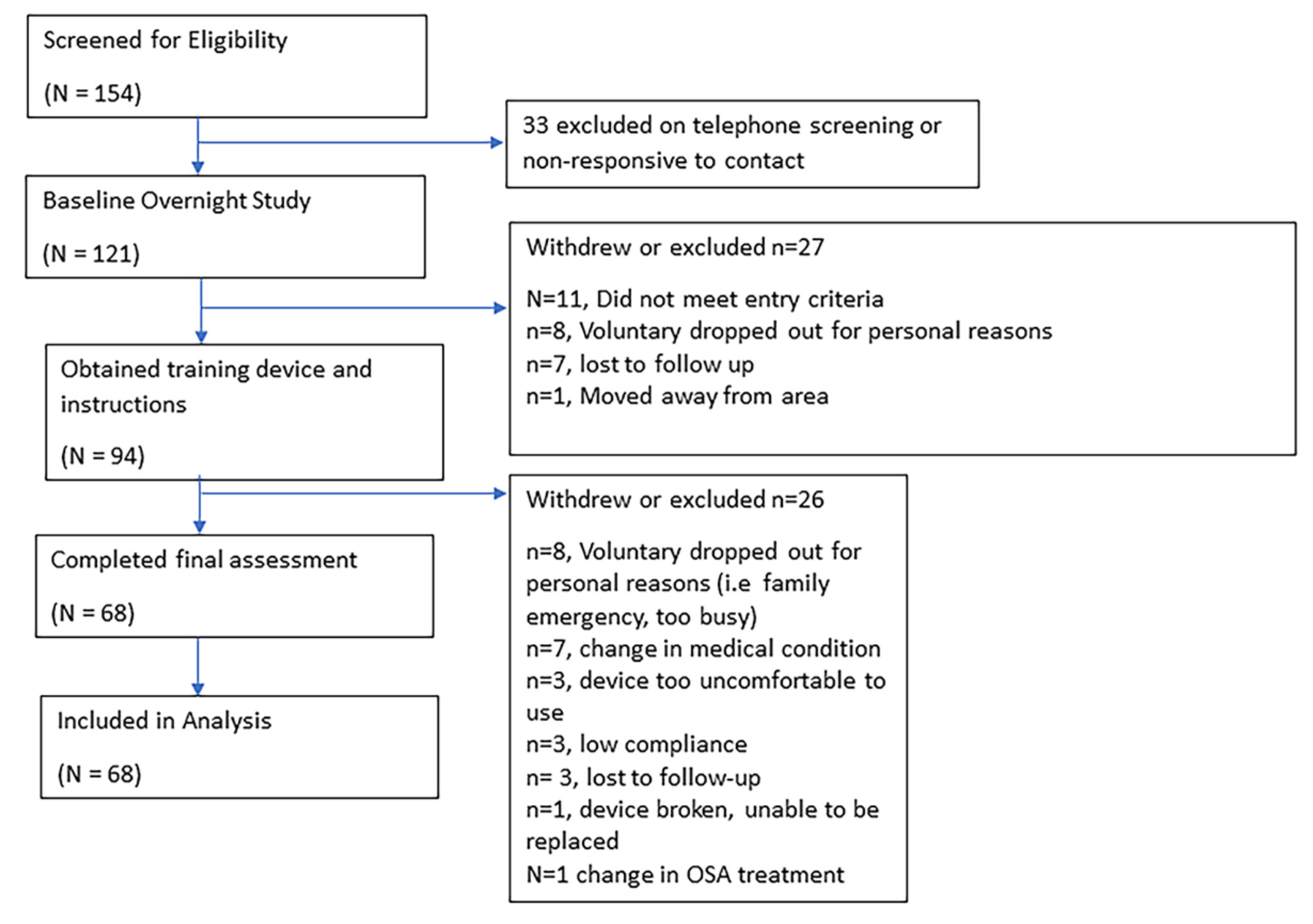
2.1. Participants
2.2. Procedure and Measurements
2.3. Upper Airway Muscle Training
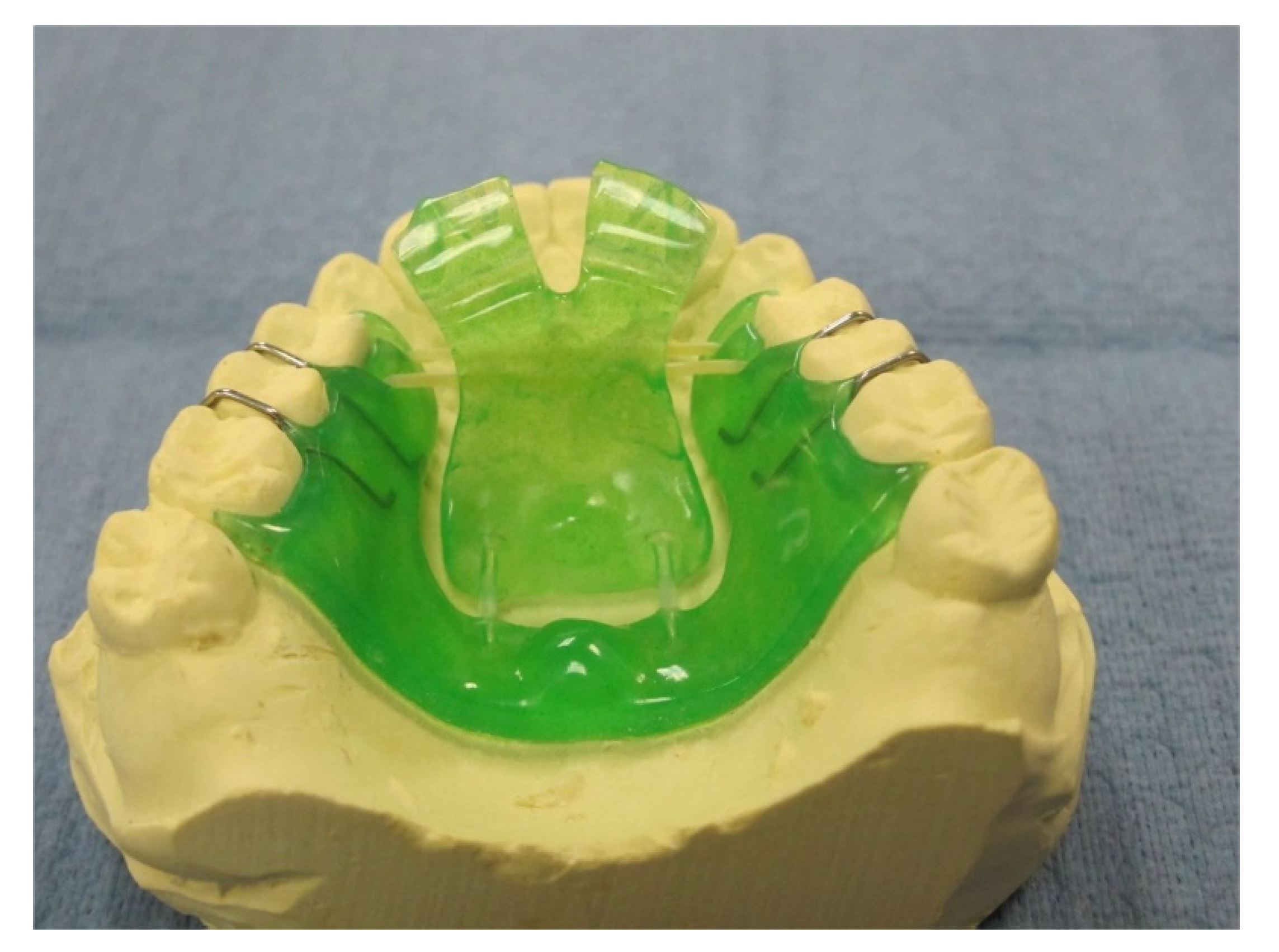
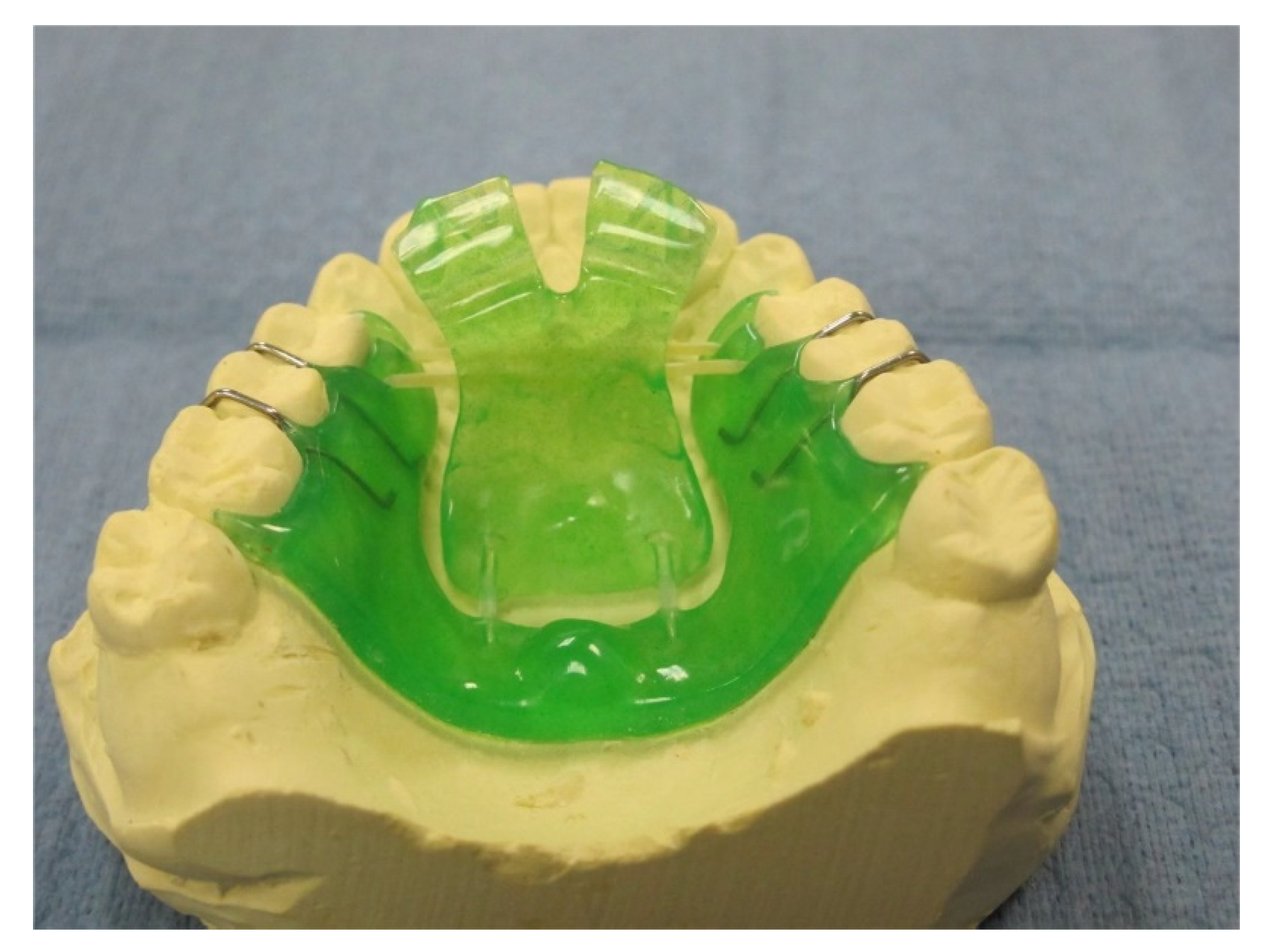
2.3.1. Pharyngeal Exercise Device
2.3.2. Mode of Action (Intervention)
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dempsey, J.A.; Veasey, S.C.; Morgan, B.J.; O’Donnell, C.P. Pathophysiology of sleep apnea. Physiol. Rev. 2010, 90, 47–112. [Google Scholar] [CrossRef]
- Mediano, O.; Romero-Peralta, S.; Resano, P.; Cano-Pumarega, I.; Sanchez-de-la-Torre, M.; Castillo-Garcia, M.; Martinez-Sanchez, A.B.; Ortigado, A.; Garcia-Rio, F. Obstructive Sleep Apnea: Emerging Treatments Targeting the Genioglossus Muscle. J. Clin. Med. 2019, 8, 1754. [Google Scholar] [CrossRef] [Green Version]
- Giles, T.L.; Lasserson, T.J.; Smith, B.J.; White, J.; Wright, J.; Cates, C.J. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst. Rev. 2006, 1, Cd001106. [Google Scholar] [CrossRef]
- Marin, J.M.; Carrizo, S.J.; Vicente, E.; Agusti, A.G. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: An observational study. Lancet 2005, 365, 1046–1053. [Google Scholar] [CrossRef]
- Cao, M.T.; Sternbach, J.M.; Guilleminault, C. Continuous positive airway pressure therapy in obstuctive sleep apnea: Benefits and alternatives. Expert Rev. Respir. Med. 2017, 11, 259–272. [Google Scholar] [CrossRef]
- Doff, M.H.; Hoekema, A.; Wijkstra, P.J.; van der Hoeven, J.H.; Huddleston Slater, J.J.; de Bont, L.G.; Stegenga, B. Oral appliance versus continuous positive airway pressure in obstructive sleep apnea syndrome: A 2-year follow-up. Sleep 2013, 36, 1289–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mezzanotte, W.S.; Tangel, D.J.; White, D.P. Influence of sleep onset on upper-airway muscle activity in apnea patients versus normal controls. Am. J. Respir. Crit. Care Med. 1996, 153 Pt 1, 1880–1887. [Google Scholar] [CrossRef] [PubMed]
- Fogel, R.B.; Trinder, J.; White, D.P.; Malhotra, A.; Raneri, J.; Schory, K.; Kleverlaan, D.; Pierce, R.J. The effect of sleep onset on upper airway muscle activity in patients with sleep apnoea versus controls. J. Physiol. 2005, 564 Pt 2, 549–562. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; Ogawa, T.; Sitalaksmi, R.M.; Miyashita, M.; Ito, T.; Sasaki, K. Effect of mandibular position achieved using an oral appliance on genioglossus activity in healthy adults during sleep. Head Face Med. 2019, 15, 26. [Google Scholar] [CrossRef]
- Bilston, L.E.; Gandevia, S.C. Biomechanical properties of the human upper airway and their effect on its behavior during breathing and in obstructive sleep apnea. J. Appl. Physiol. 2014, 116, 314–324. [Google Scholar] [CrossRef] [Green Version]
- Bailey, E.F.; Rice, A.D.; Fuglevand, A.J. Firing patterns of human genioglossus motor units during voluntary tongue movement. J. Neurophysiol. 2007, 97, 933–936. [Google Scholar] [CrossRef]
- Valbuza, J.S.; de Oliveira, M.M.; Conti, C.F.; Prado, L.B.; de Carvalho, L.B.; do Prado, G.F. Methods for increasing upper airway muscle tonus in treating obstructive sleep apnea: Systematic review. Sleep Breath. 2010, 14, 299–305. [Google Scholar] [CrossRef]
- Guimaraes, K.C.; Drager, L.F.; Genta, P.R.; Marcondes, B.F.; Lorenzi-Filho, G. Effects of oropharyngeal exercises on patients with moderate obstructive sleep apnea syndrome. Am. J. Respir. Crit. Care Med. 2009, 179, 962–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, R.; Brooks, R.; Gamaldo, C.E.; Harding, S.M.; Lloyd, R.M.; Marcus, C.L.; Vaughn, B.V.; for the American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, Version 2.2 ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2015. [Google Scholar]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Hoch, C.C.; Yeager, A.L.; Kupfer, D.J. Quantification of subjective sleep quality in healthy elderly men and women using the Pittsburgh Sleep Quality Index (PSQI). Sleep 1991, 14, 331–338. [Google Scholar] [PubMed]
- Brazier, J.E.; Harper, R.; Jones, N.M.; O’Cathain, A.; Thomas, K.J.; Usherwood, T.; Westlake, L. Validating the SF-36 health survey questionnaire: New outcome measure for primary care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef] [Green Version]
- Basner, M.; Dinges, D.F. Maximizing sensitivity of the psychomotor vigilance test (PVT) to sleep loss. Sleep 2011, 34, 581–591. [Google Scholar] [CrossRef]
- Ieto, V.; Kayamori, F.; Montes, M.I.; Hirata, R.P.; Gregorio, M.G.; Alencar, A.M.; Drager, L.F.; Genta, P.R.; Lorenzi-Filho, G. Effects of Oropharyngeal Exercises on Snoring: A Randomized Trial. Chest 2015, 148, 683–691. [Google Scholar] [CrossRef] [Green Version]
- Remmers, J.E.; deGroot, W.J.; Sauerland, E.K.; Anch, A.M. Pathogenesis of upper airway occlusion during sleep. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1978, 44, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Ye, D.; Chen, C.; Song, D.; Shen, M.; Liu, H.; Zhang, S.; Zhang, H.; Li, J.; Yu, W.; Wang, Q. Oropharyngeal Muscle Exercise Therapy Improves Signs and Symptoms of Post-stroke Moderate Obstructive Sleep Apnea Syndrome. Front. Neurol. 2018, 9, 912. [Google Scholar] [CrossRef] [PubMed]
- Puhan, M.A.; Suarez, A.; Lo Cascio, C.; Zahn, A.; Heitz, M.; Braendli, O. Didgeridoo playing as alternative treatment for obstructive sleep apnoea syndrome: Randomised controlled trial. BMJ 2006, 332, 266–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rueda, J.R.; Mugueta-Aguinaga, I.; Vilaró, J.; Rueda-Etxebarria, M. Myofunctional therapy (oropharyngeal exercises) for obstructive sleep apnoea. Cochrane Database Syst. Rev. 2020, 11, Cd013449. [Google Scholar] [CrossRef] [PubMed]
- Antic, N.A.; Catcheside, P.; Buchan, C.; Hensley, M.; Naughton, M.T.; Rowland, S.; Williamson, B.; Windler, S.; McEvoy, R.D. The effect of CPAP in normalizing daytime sleepiness, quality of life, and neurocognitive function in patients with moderate to severe OSA. Sleep 2011, 34, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.R.; White, D.P.; Malhotra, A.; Stanchina, M.L.; Ayas, N.T. Continuous positive airway pressure therapy for treating sleepiness in a diverse population with obstructive sleep apnea: Results of a meta-analysis. Arch. Intern. Med. 2003, 163, 565–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrell, M.J.; McRobbie, D.W.; Quest, R.A.; Cummin, A.R.; Ghiassi, R.; Corfield, D.R. Changes in brain morphology associated with obstructive sleep apnea. Sleep Med. 2003, 4, 451–454. [Google Scholar] [CrossRef]
- Zinchuk, A.V.; Chu, J.H.; Liang, J.; Celik, Y.; Op de Beeck, S.; Redeker, N.S.; Wellman, A.; Yaggi, H.K.; Peker, Y.; Sands, S.A. Physiological Traits and Adherence to Sleep Apnea Therapy in Individuals with Coronary Artery Disease. Am. J. Respir. Crit. Care Med. 2021, 204, 703–712. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention/Sham (No.) | Intervention (n = 35) (Mean ± SD) | Sham (n = 33) (Mean ± SD) | p-Value |
|---|---|---|---|
| Age (mean ±SD) | 63.2 ± 9.1 | 56.0 ± 13.1 | 0.038 * |
| Gender (M: F) | 26:9 | 17:16 | 0.052 † |
| Group of Treatment | |||
| APAP | 11 | 10 | 0.986 † |
| MAS | 11 | 11 | |
| Untreated | 13 | 12 | |
| Initial BMI | 30.0 ± 4.5 | 30.9 ± 7.1 | 0.930 * |
| Final BMI | 30.1 ± 4.5 | 30.8 ± 6.8 | 0.979 * |
| p value of Change | 0.681 ‡ | 0.750 ‡ | 0.615 § |
| Initial neck circumference | 40.1 ± 3.5 | 39.3 ± 4.5 | 0.411 * |
| Final neck circumference | 40.3 ± 4.1 | 39.3 ± 4.5 | 0.823 * |
| p value of Change | 0.431 ‡ | 0.975 ‡ | 0.674 § |
| Initial Heart Rate | 71.2 ± 14.5 | 72.1 ± 9 | 0.411 * |
| Final Heart Rate | 68.3 ± 14.6 | 69.9 ± 12.5 | 0.823 * |
| p value of Change | 0.591 ‡ | 0.046 ‡ | 0.935 § |
| Initial Snoring (total number) | 1056.4 ± 1093.7 | 1021.2 ± 1266.6 | 0.619 * |
| Final Snoring (total number) | 1014 ± 1070.2 | 784.4 ± 1554.1 | 0.103 * |
| p value of Change | 0.869 ‡ | 0.028 ‡ | 0.505 § |
| Intervention/Sham | Intervention (n = 35) (Mean ±SD) | Sham (n = 33) (Mean ±SD) | p-Value |
|---|---|---|---|
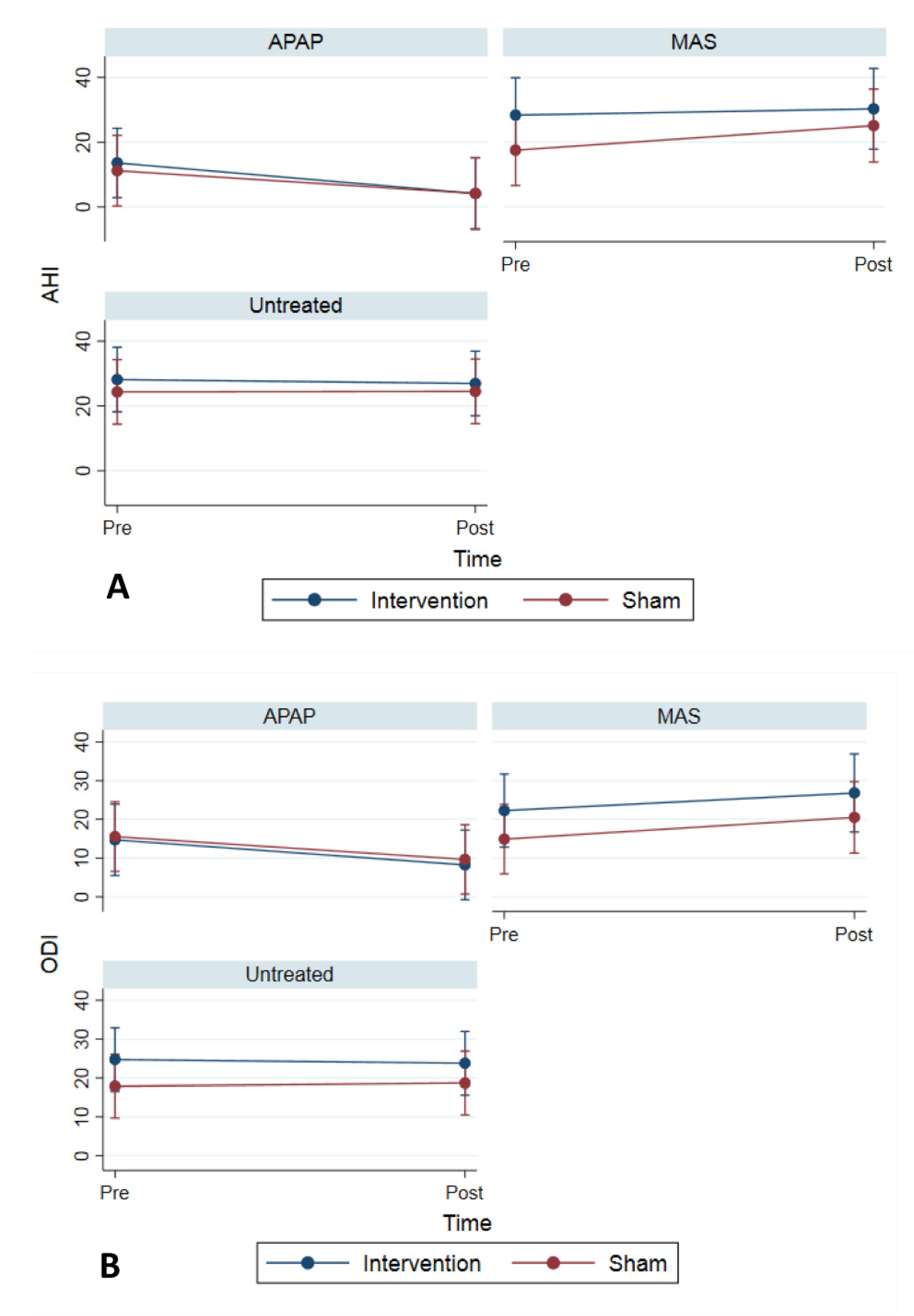
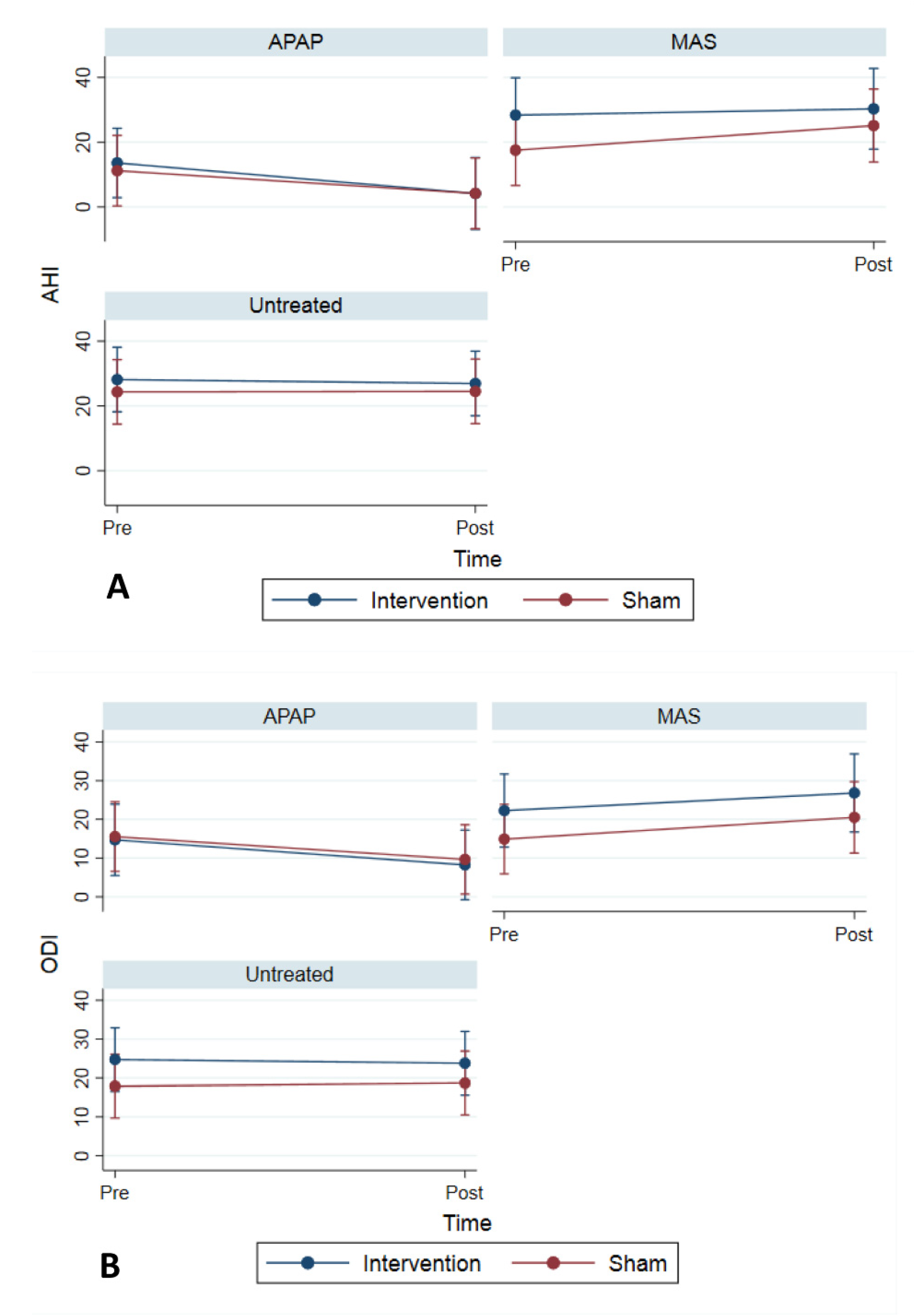
| Initial AHI | 23.8 ± 21.3 | 17.9 ± 17.6 | 0.250 * |
| Final AHI | 19.9 ± 18.3 | 17.7 ± 16.2 | 0.611 * |
| Change | 0.475 † | 0.728 † | 0.682 ‡ |
| Initial AI | 9.8 ± 13 | 5.5 ± 11.4 | 0.070 * |
| Final AI | 8 ± 13.4 | 6.2 ± 9.3 | 0.865 * |
| Change | 0.106 † | 0.585 † | 0.555 ‡ |
| Initial HI | 14 ± 13.1 | 12.4 ± 9.6 | 0.787 * |
| Final HI | 11.9 ± 9.9 | 11.9 ± 11.7 | 0.621 * |
| Change | 0.982 † | 0.522 † | 0.863 ‡ |
| Initial AHI4 | 20 ± 14.8 | 19.6 ± 17.4 | 0.741 * |
| Final AHI4 | 17.9 ± 13.9 | 18 ± 12.8 | 0.844 * |
| Change | 0.637 † | 0.820 † | 0.749 ‡ |
| Initial ODI | 20.7 ± 17.2 | 16 ± 13.1 | 0.401 * |
| Final ODI | 18.1 ± 15.3 | 15.9 ± 12.3 | 0.788 * |
| Change | 0.788 † | 0.788 † | 0.764 ‡ |
| Initial OD total | 150.7 ± 135.6 | 118.4 ± 109.1 | 0.455 * |
| Final OD total | 129.5 ± 116.5 | 99.8 ± 78.6 | 0.674 * |
| Change | 0.674 † | 0.506 † | 0.488 ‡ |
| Initial APAP 95p | 10.7 ± 2.6 | 11.9 ± 2.6 | 0.506 * |
| Final APAP 95p | 10.5 ± 2.5 | 10.8 ± 2 | 0.772 * |
| change | 0.593 † | 0.177 † | 0.649 § |
| Variables | Univariable Model | |
|---|---|---|
| β, 95% CI | p-Value | |
| Age | −0.19 (−0.57, 0.19) | 0.243 |
| Gender: Female | −3.33 (−12.28, 5.63) | 0.466 |
| Group (baseline: Untreated) | ||
| APAP | −5.11 (−14.65, 4.43) | 0.294 |
| MAS | 7.97 (−1.72, 17.67) | 0.107 |
| Intervention (Muscle training) | −1.75 (−10.13, 6.63) | 0.682 |
| Intervention/Sham | Intervention (n = 35) (Mean ± SD) | Sham (n = 33) (Mean ± SD) | p-Value |
|---|---|---|---|
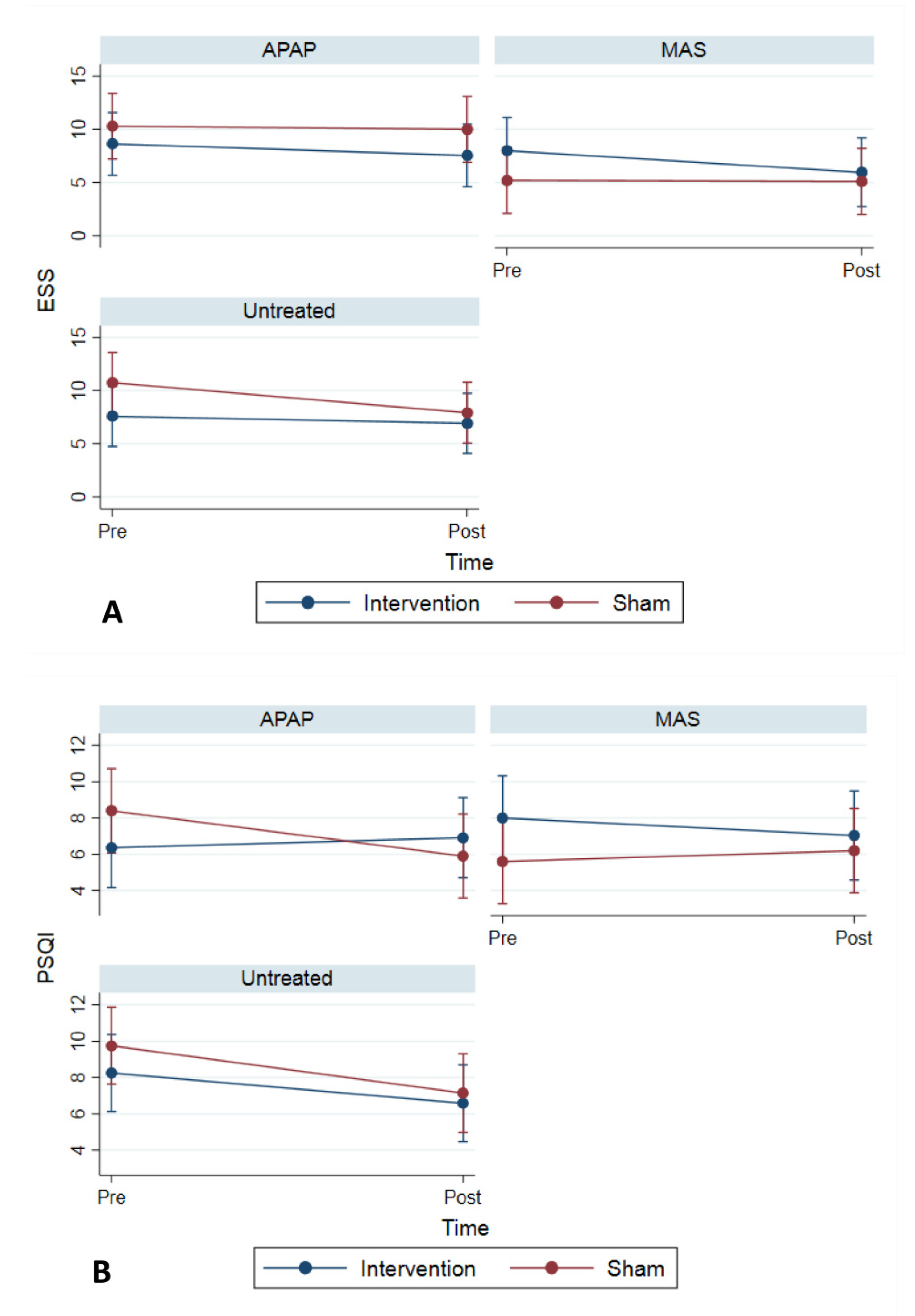
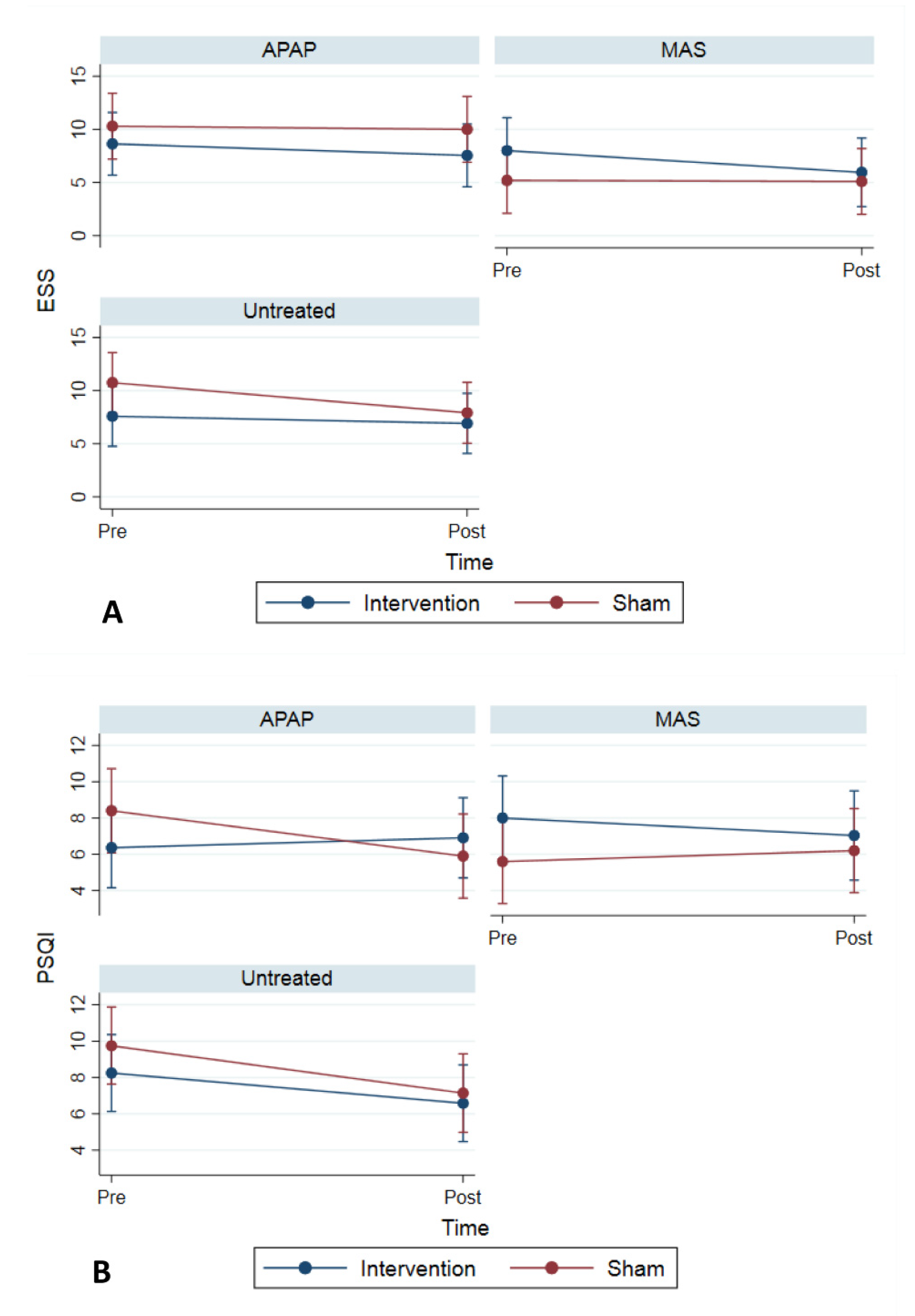
| Initial ESS Score | 7.9 ± 5 | 8.8 ± 5.2 | 0.506 * |
| Final ESS Score | 6.8 ± 4.4 | 7.5 ± 5.4 | 0.926 * |
| Change | 0.072 † | 0.084 † | 0.397 ‡ |
| Initial PSQI score | 6.9 ± 3.5 | 8.1 ± 4 | 0.405 * |
| Final PSQI score | 6.9 ± 3.5 | 6.4 ± 3.8 | 0.538 * |
| Change | 0.476 † | 0.004 † | 0.056 ‡ |
| Initial PVT_RT | 334.4 ± 48.8 | 329.7 ± 43.1 | 0.689 * |
| Final PVT_RT | 317.1 ± 36.2 | 310.5 ± 31.6 | 0.450 * |
| Change | 0.111 † | 0.003 † | 0.653 ‡ |
| Initial PVT_slow10 | 431.4 ± 44.6 | 426.6 ± 39.2 | 0.655 * |
| Final PVT_slow10 | 423.2 ± 32 | 402.2 ± 41.6 | 0.030 * |
| Change | 0.413 † | 0.003 † | 0.058 ‡ |
| Initial PVT lapses | 3.8 ± 5.8 | 3.2 ± 5.7 | 0.640 * |
| Final PVT lapses | 1.8 ± 2.9 | 1.3 ± 1.2 | 0.3051 * |
| Change | 0.013 † | 0.060 † | 0.272 ‡ |
| Initial PVT false starts | 0.5 ± 0.7 | 0.3 ± 0.4 | 0.220 * |
| Final PVT false starts | 1 ± 1.1 | 0.4 ± 0.9 | 0.043 * |
| Change | 0.003 † | 0.404 † | 0.213 ‡ |
| Intervention/Sham | Intervention (n = 35) (Mean ± SD) | Sham (n = 33) (Mean ± SD) | p-Value |
|---|---|---|---|
| Initial “Physical functioning” | 76.6 ± 27.8 | 76.5 ± 24.2 | 0.673 * |
| Final “Physical functioning” | 78.7 ± 23.7 | 79.2 ± 22.9 | 0.994 * |
| Change | 0.370 † | 0.426 † | 0.457 ‡ |
| Initial “Role limitations due to physical health” | 75.7 ± 38.6 | 60.6 ± 42.9 | 0.130 * |
| Final “Role limitations due to physical health” | 74.2 ± 41.7 | 79.7 ± 35 | 0.571 * |
| Change | >0.99 † | 0.020 † | 0.078 ‡ |
| Initial “Role limitations due to emotional problems” | 81 ± 35.5 | 71.7 ± 39.2 | 0.311 * |
| Final “Role limitations due to emotional problems” | 85.9 ± 31.2 | 80.2 ± 33.7 | 0.486 * |
| Change | 0.280 † | 0.324 † | 0.834 ‡ |
| Initial “Energy/fatigue” | 55.5 ± 20.9 | 48.7 ± 25.3 | 0.228 * |
| Final “Energy/fatigue” | 57 ± 24.4 | 56.9 ± 24.3 | 0.987 * |
| Change | 0.671 † | 0.037 † | 0.635 ‡ |
| Initial “Emotional well-being” | 73.1 ± 19.8 | 73.2 ± 18.3 | 0.993 * |
| Final “Emotional well-being” | 80.2 ± 17.2 | 79.1 ± 16.5 | 0.790 * |
| Change | 0.040 † | 0.040 † | 0.561 ‡ |
| Initial “Social functioning” | 80.7 ± 25.4 | 73.9 ± 27.5 | 0.294 * |
| Final “Social functioning” | 83.3 ± 25.5 | 79.3 ± 25.9 | 0.527 * |
| Change | 0.287 † | 0.120 † | 0.793 ‡ |
| Initial “Pain” | 72.9 ± 24.3 | 73.3 ± 24.5 | 0.990 * |
| Final “Pain” | 74.3 ± 22.2 | 73.3 ± 26.4 | 0.884 * |
| Change | 0.330 † | 0.620 † | 0.505 ‡ |
| Initial “General health” | 63.3 ± 21.5 | 64.2 ± 22.4 | 0.857 * |
| Final “General health” | 63.6 ± 21.7 | 66.9 ± 21.3 | 0.538 * |
| Change | 0.733 † | 0.388 † | 0.901 ‡ |
| Initial “Health change” | 57.1 ± 19.7 | 51.5 ± 22.5 | 0.275 * |
| Final “Health change” | 57.6 ± 23 | 53.9 ± 22.1 | 0.514 * |
| Change | 0.275 † | 0.441 † | 0.908 ‡ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maghsoudipour, M.; Nokes, B.; Bosompra, N.-O.; Jen, R.; Li, Y.; Moore, S.; DeYoung, P.N.; Fine, J.; Edwards, B.A.; Gilbertson, D.; et al. A Pilot Randomized Controlled Trial of Effect of Genioglossus Muscle Strengthening on Obstructive Sleep Apnea Outcomes. J. Clin. Med. 2021, 10, 4554. https://doi.org/10.3390/jcm10194554
Maghsoudipour M, Nokes B, Bosompra N-O, Jen R, Li Y, Moore S, DeYoung PN, Fine J, Edwards BA, Gilbertson D, et al. A Pilot Randomized Controlled Trial of Effect of Genioglossus Muscle Strengthening on Obstructive Sleep Apnea Outcomes. Journal of Clinical Medicine. 2021; 10(19):4554. https://doi.org/10.3390/jcm10194554
Chicago/Turabian StyleMaghsoudipour, Maryam, Brandon Nokes, Naa-Oye Bosompra, Rachel Jen, Yanru Li, Stacie Moore, Pamela N. DeYoung, Janelle Fine, Bradley A. Edwards, Dillon Gilbertson, and et al. 2021. "A Pilot Randomized Controlled Trial of Effect of Genioglossus Muscle Strengthening on Obstructive Sleep Apnea Outcomes" Journal of Clinical Medicine 10, no. 19: 4554. https://doi.org/10.3390/jcm10194554
APA StyleMaghsoudipour, M., Nokes, B., Bosompra, N.-O., Jen, R., Li, Y., Moore, S., DeYoung, P. N., Fine, J., Edwards, B. A., Gilbertson, D., Owens, R., Morgan, T., & Malhotra, A. (2021). A Pilot Randomized Controlled Trial of Effect of Genioglossus Muscle Strengthening on Obstructive Sleep Apnea Outcomes. Journal of Clinical Medicine, 10(19), 4554. https://doi.org/10.3390/jcm10194554