
How Close Are We toward an Optimal Balance in Safety and Efficacy in Catheter Ablation of Atrial Fibrillation? Lessons from the CLOSE Protocol

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. The CLOSE Protocol
2.1. Development of the Protocol
2.2. The CLOSE Protocol: Performance and Effectiveness
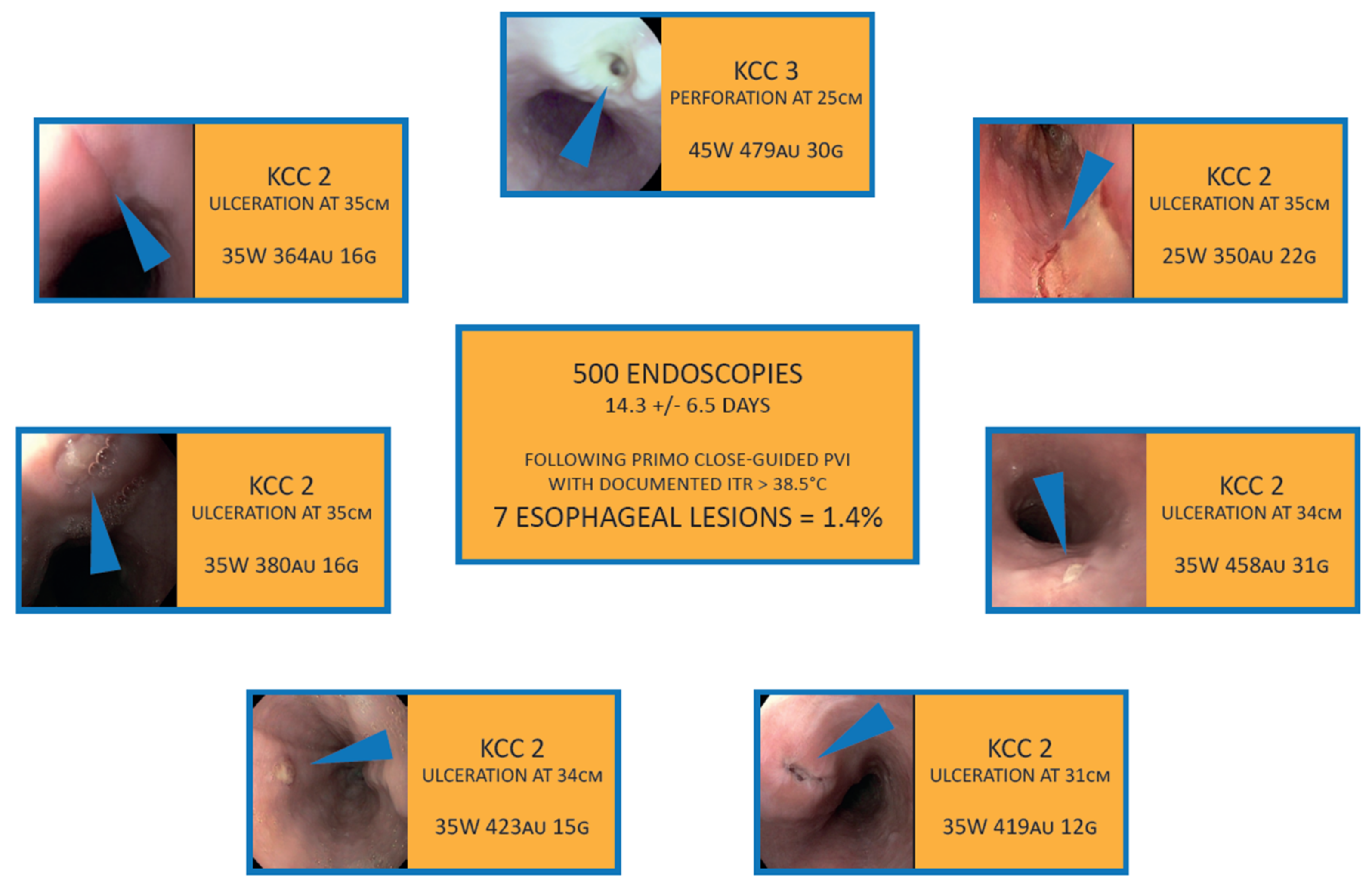
2.3. Safety of CLOSE-Guided PVI
2.4. The CLOSE Protocol: Durability of Isolation at Follow-Up
2.5. Efficacy of the CLOSE-Protocol in Perspective to Other Ablation Strategies in Large-Scale Studies
3. Broadening the Landscape: Evaluation of the CLOSE Technique in Linear Ablation
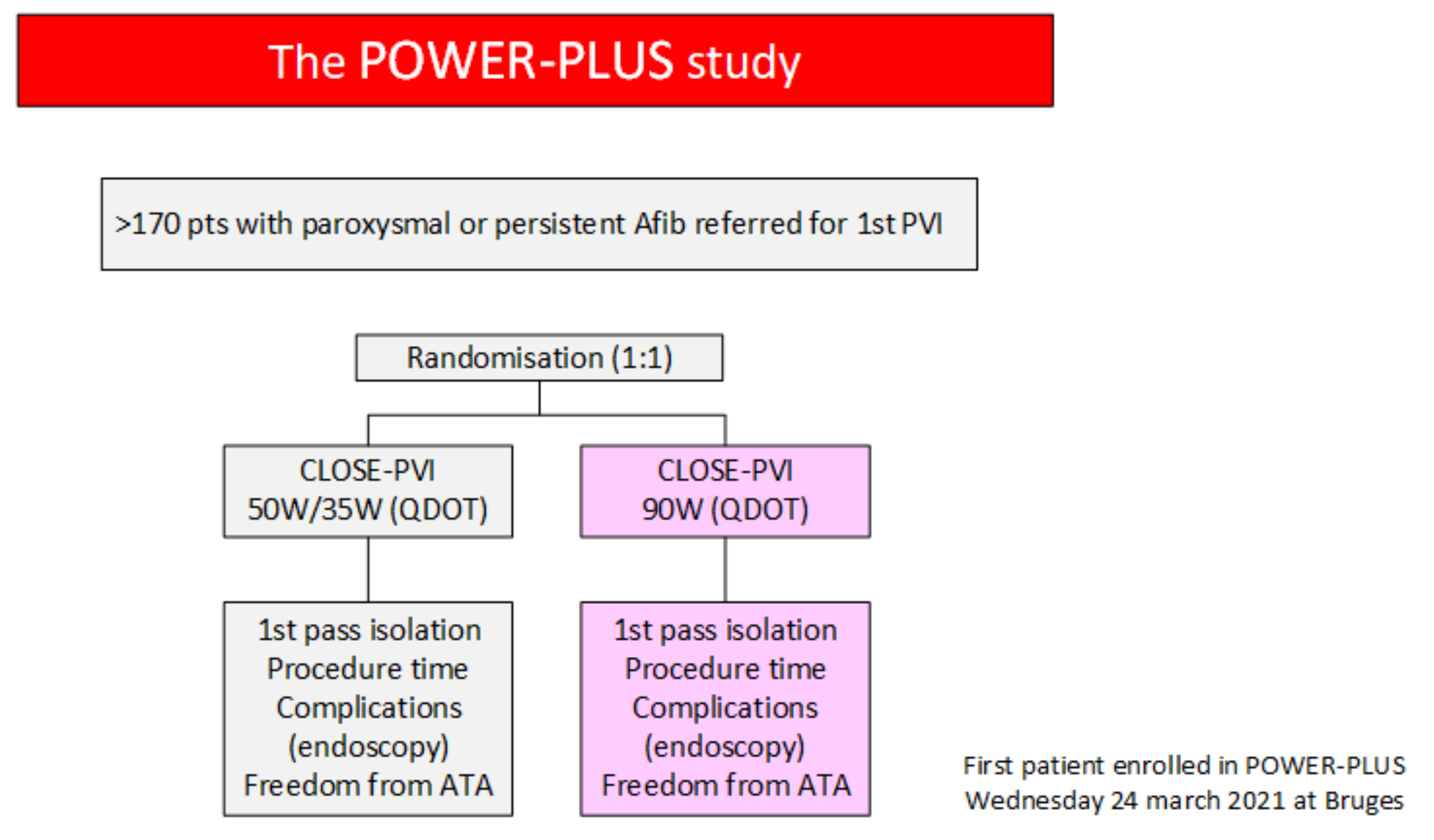
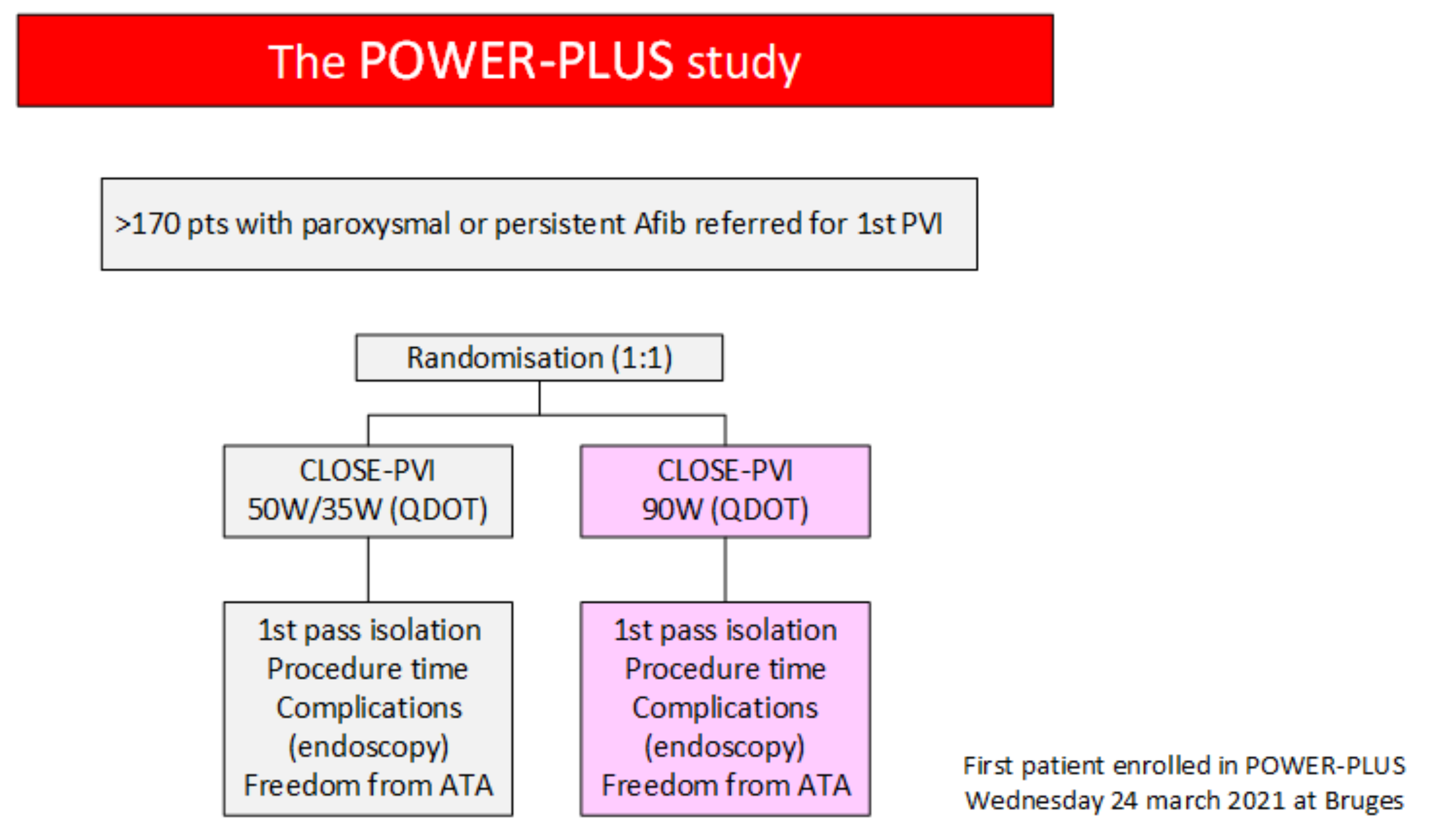
4. High Power CLOSE to Shorten Procedure Time: The POWER-AF Study and Development of Dedicated Catheters
5. Upcoming Technologies for Pulmonary Vein Isolation: The End of the CLOSE Protocol?
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boriani, G.; Vitolo, M.; Lane, D.A.; Potpara, T.S.; Lip, G.Y. Beyond the 2020 guidelines on atrial fibrillation of the European society of cardiology. Eur. J. Intern. Med. 2021, 86, 1–11. [Google Scholar] [CrossRef]
- Haïssaguerre, M.; Jaïs, P.; Shah, D.C.; Takahashi, A.; Hocini, M.; Quiniou, G.; Garrigue, S.; Le Mouroux, A.; Le Métayer, P.; Clémenty, J. Spontaneous Initiation of Atrial Fibrillation by Ectopic Beats Originating in the Pulmonary Veins. N. Engl. J. Med. 1998, 339, 659–666. [Google Scholar] [CrossRef] [Green Version]
- Tondo, C. Atrial fibrillation ablation in real life: Is there room for improvements? J. Cardiovasc. Med. 2020, 21, 749–750. [Google Scholar] [CrossRef]
- El Haddad, M.; Taghji, P.; Phlips, T.; Wolf, M.; Demolder, A.; Choudhury, R.; Knecht, S.; Vandekerckhove, Y.; Tavernier, R.; Nakagawa, H.; et al. Determinants of Acute and Late Pulmonary Vein Reconnection in Contact Force-Guided Pulmonary Vein Isolation. Circ. Arrhythm. Electrophysiol. 2017, 10, e004867. [Google Scholar] [CrossRef]
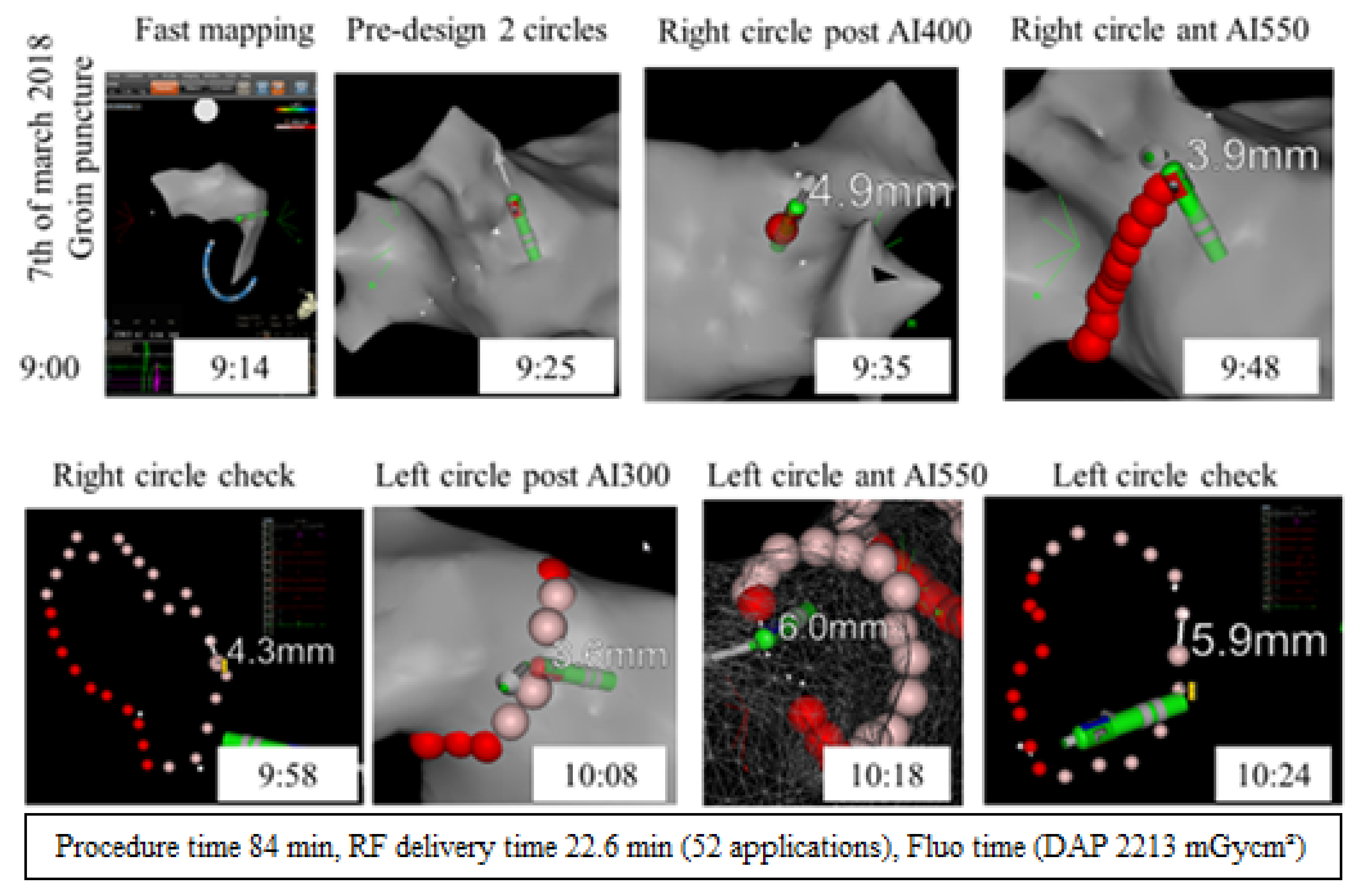
- Taghji, P.; El Haddad, M.; Phlips, T.; Wolf, M.; Knecht, S.; Vandekerckhove, Y.; Tavernier, R.; Nakagawa, H.; Duytschaever, M. Evaluation of a Strategy Aiming to Enclose the Pulmonary Veins with Contiguous and Optimized Radiofrequency Lesions in Paroxysmal Atrial Fibrillation: A Pilot Study. JACC Clin. Electrophysiol. 2018, 4, 99–108. [Google Scholar] [CrossRef]
- Phlips, T.; Taghji, P.; El Haddad, M.; Wolf, M.; Knecht, S.; Vandekerckhove, Y.; Tavernier, R.; Duytschaever, M. Improving procedural and one-year outcome after contact force-guided pulmonary vein isolation: The role of interlesion distance, ablation index, and contact force variability in the ’CLOSE’-protocol. Europace 2018, 20, f419–f427. [Google Scholar] [CrossRef]
- Duytschaever, M.; De Pooter, J.; Demolder, A.; El Haddad, M.; Phlips, T.; Strisciuglio, T.; Debonnaire, P.; Wolf, M.; Vandekerckhove, Y.; Knecht, S.; et al. Long-term impact of catheter ablation on arrhythmia burden in low-risk patients with paroxysmal atrial fibrillation: The CLOSE to CURE study. Heart Rhythm 2019, 17, 535–543. [Google Scholar] [CrossRef]
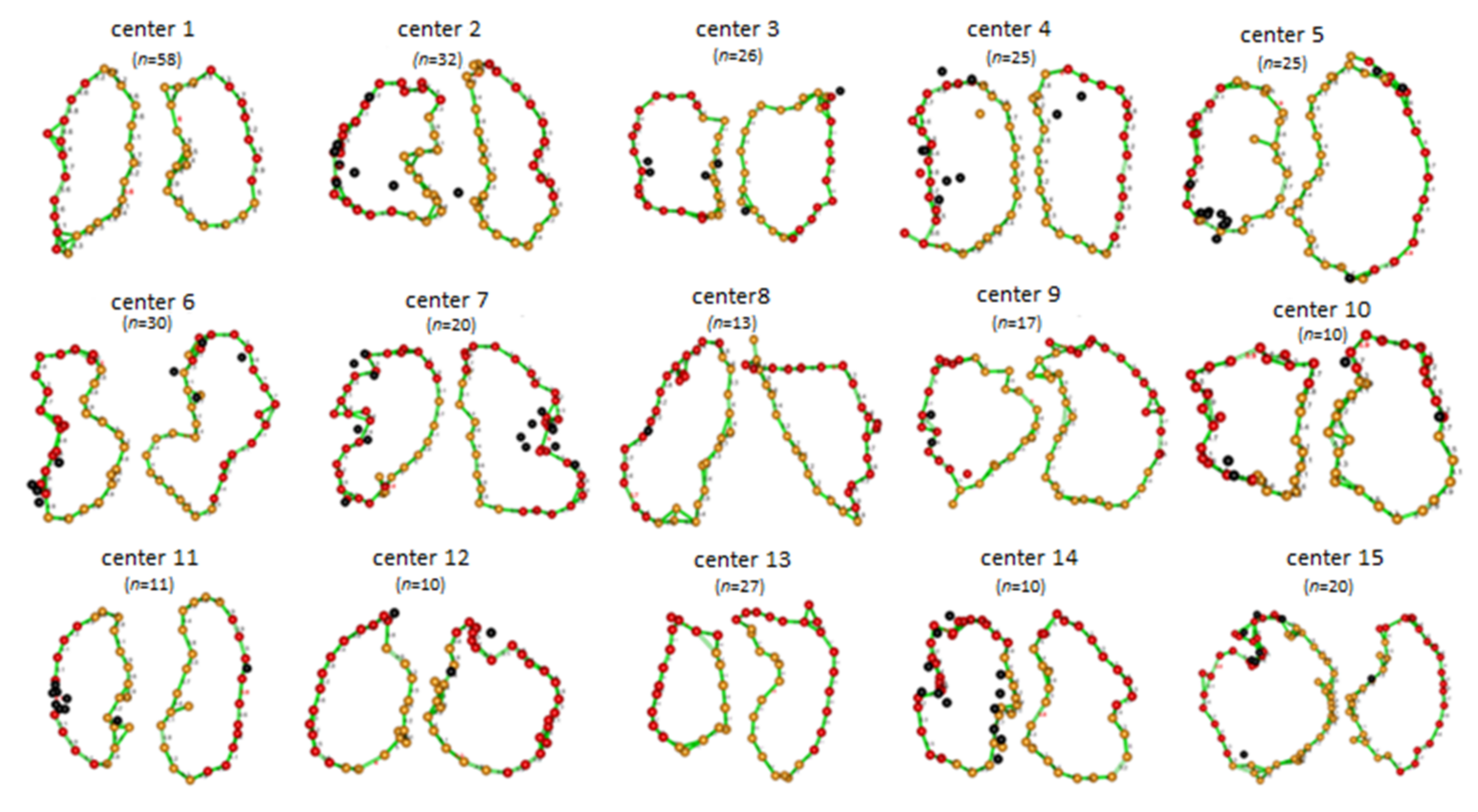
- Duytschaever, M.; Vijgen, J.; De Potter, T.; Scherr, D.; Van Herendael, H.; Knecht, S.; Kobza, R.; Berte, B.; Sandgaard, N.; Albenque, J.-P.; et al. Standardized pulmonary vein isolation workflow to enclose veins with contiguous lesions: The multicentre VISTAX trial. Europace 2020, 22, 1645–1652. [Google Scholar] [CrossRef]
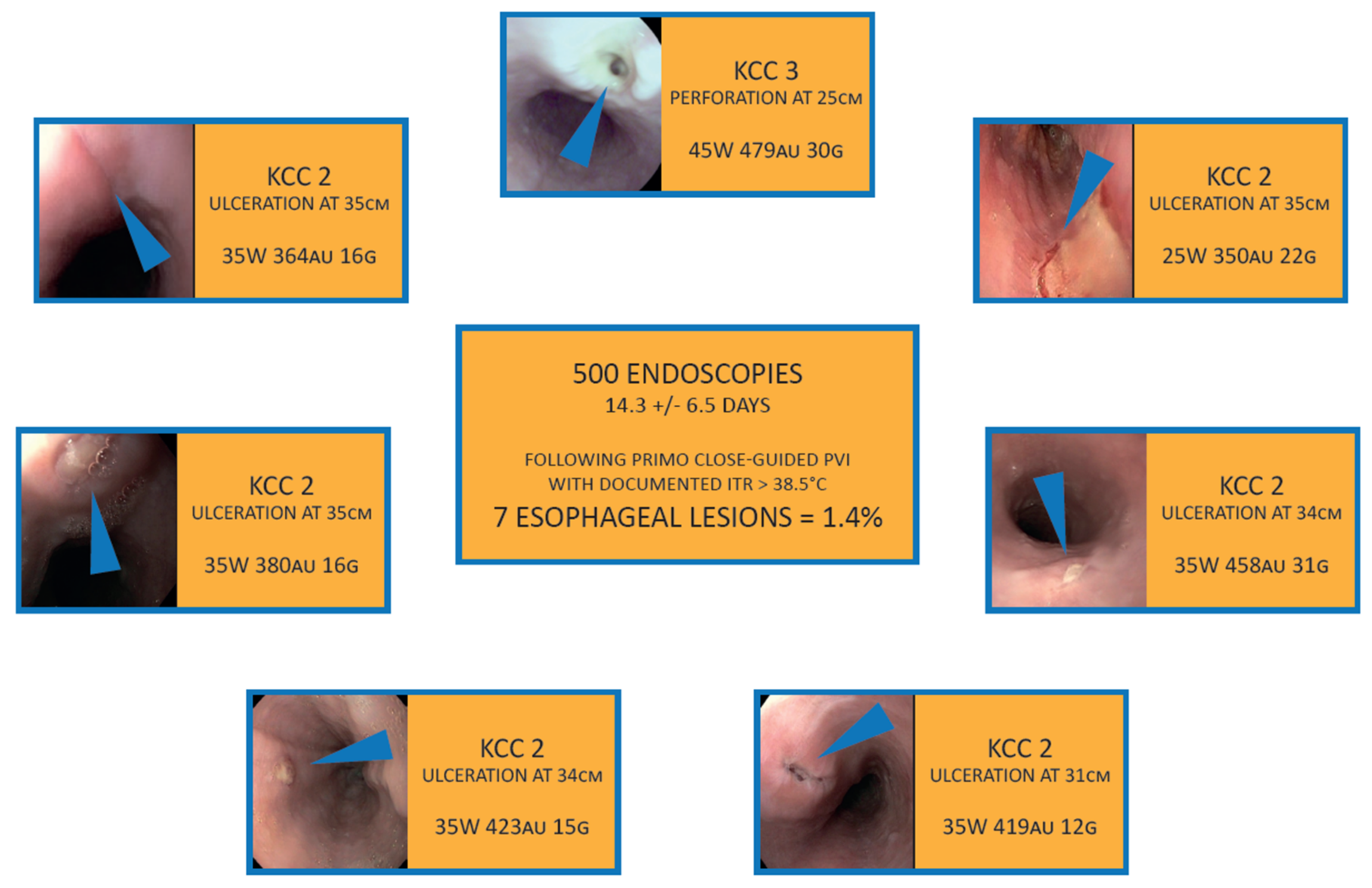
- Wolf, M.; El Haddad, M.; De Wilde, V.; Phlips, T.; De Pooter, J.; Almorad, A.; Strisciuglio, T.; Vandekerckhove, Y.; Tavernier, R.; Crijns, H.J.; et al. Endoscopic evaluation of the esophagus after catheter ablation of atrial fibrillation using contiguous and optimized radiofrequency applications. Heart Rhythm 2019, 16, 1013–1020. [Google Scholar] [CrossRef]
- Yarlagadda, B.; Deneke, T.; Turagam, M.; Dar, T.; Paleti, S.; Parikh, V.; DiBiase, L.; Halfbass, P.; Santangeli, P.; Mahapatra, S.; et al. Temporal relationships between esophageal injury type and progression in patients undergoing atrial fibrillation catheter ablation. Heart Rhythm 2019, 16, 204–212. [Google Scholar] [CrossRef]
- De Pooter, J.; Strisciuglio, T.; El Haddad, M.; Wolf, M.; Phlips, T.; Vandekerckhove, Y.; Tavernier, R.; Knecht, S.; Duytschaever, M. Pulmonary Vein Reconnection No Longer Occurs in the Majority of Patients After a Single Pulmonary Vein Isolation Procedure. JACC Clin. Electrophysiol. 2019, 5, 295–305. [Google Scholar] [CrossRef]
- Kuck, K.-H.; Brugada, J.; Furnkranz, A.; Metzner, A.; Ouyang, F.; Chun, K.R.J.; Elvan, A.; Arentz, T.; Bestehorn, K.; Pocock, S.J.; et al. Cryoballoon or Radiofrequency Ablation for Paroxysmal Atrial Fibrillation. N. Engl. J. Med. 2016, 374, 2235–2245. [Google Scholar] [CrossRef] [PubMed]
- Wazni, O.M.; Dandamudi, G.; Sood, N.; Hoyt, R.; Tyler, J.; Durrani, S.; Niebauer, M.; Makati, K.; Halperin, B.; Gauri, A.; et al. Cryoballoon Ablation as Initial Therapy for Atrial Fibrillation. N. Engl. J. Med. 2021, 384, 316–324. [Google Scholar] [CrossRef]
- Wilber, D.J.; Pappone, C.; Neuzil, P.; De Paola, A.; Marchlinski, F.; Natale, A.; Macle, L.; Daoud, E.G.; Calkins, H.; Hall, B.; et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: A randomized controlled trial. JAMA 2010, 303, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Natale, A.; Reddy, V.Y.; Monir, G.; Wilber, D.J.; Lindsay, B.D.; McElderry, H.T.; Kantipudi, C.; Mansour, M.C.; Melby, D.; Packer, D.L.; et al. Paroxysmal AF catheter ablation with a contact force sensing catheter: Results of the prospective, multicenter SMART-AF trial. J. Am. Coll. Cardiol. 2014, 64, 647–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, M.; El Haddad, M.; Fedida, J.; Taghji, P.; Van Beeumen, K.; Strisciuglio, T.; De Pooter, J.; Lepièce, C.; Vandekerckhove, Y.; Tavernier, R.; et al. Evaluation of left atrial linear ablation using contiguous and optimized radiofrequency lesions: The ALINE study. Europace 2018, 20, f401–f409. [Google Scholar] [CrossRef]
- Nakagawa, H.; Ikeda, A.; Constantine, G.; Govari, A.; Sharma, T.; Pitha, J.; Jackman, W.M. Controlling Lesion Size and Incidence of Steam Pop by Controlling Contact Force, Radiofrequency Power and Application Time (Force-Power-Time Index) In Canine Beating Heart. Heart Rhythm 2010, 122, A15777. [Google Scholar]
- Wielandts, J.Y.; Kyriakopoulou, M.; Almorad, A.; Hilfiker, G.; Strisciuglio, T.; Phlips, T.; El Haddad, M.; Lycke, M.; Unger, P.; Waroux, J.-B.L.P.D.; et al. Prospective Randomized Evaluation of High Power during CLOSE-Guided Pulmonary Vein Isolation: The POWER-AF Study. Circ. Arrhythm. Electrophysiol. 2021, 14, e009112. [Google Scholar] [CrossRef]
- Wielandts, J.-Y.; Almorad, A.; Hilfiker, G.; Gillis, K.; Haddad MEl Vijgen, J.; Berte, B.; Waroux, J.-B.L.P.D.; Tavernier, R.; Duytschaever, M.; Knecht, S. Biosense Webster’s QDOT MicroTM radiofrequency ablation catheter. Future Cardiol. 2021. [Google Scholar] [CrossRef]
- Almorad, A.; Wielandts, J.Y.; El Haddad, M.; Knecht, S.; Tavernier, R.; Kobza, R.; Phlips, T.; Vijgen, J.; Berte, B.; Duytschaever, M. Performance and Safety of Temperature- and Flow-Controlled Radiofrequency Ablation in Ablation Index–Guided Pulmonary Vein Isolation. JACC Clin. Electrophysiol. 2021, 7, 408–409. [Google Scholar] [CrossRef]
- Reddy, V.Y.; Grimaldi, M.; De Potter, T.; Vijgen, J.M.; Bulava, A.; Duytschaever, M.; Martinek, M.; Natale, A.; Knecht, S.; Neuzil, P. Pulmonary Vein Isolation With Very High Power, Short Duration, Temperature-Controlled Lesions: The QDOT-FAST Trial. JACC Clin. Electrophysiol. 2019, 5, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, H.; Ikeda, A.; Sharma, T.; Govari, A.; Ashton, J.; Maffre, J.; Lifshitz, A.; Fuimaono, K.; Yokoyama, K.; Wittkampf, F.H.; et al. Comparison of in vivo tissue temperature profile and lesion geometry for radiofrequency ablation with high power-short duration and moderate power-moderate duration effects of thermal latency and contact force on lesion formation. Circ. Arrhythmia Electrophysiol. 2021, 14, e009899. [Google Scholar] [CrossRef] [PubMed]
- Yavin, H.D.; Leshem, E.; Shapira-Daniels, A.; Sroubek, J.; Barkagan, M.; Haffajee, C.I.; Cooper, J.M.; Anter, E. Impact of High-Power Short-Duration Radiofrequency Ablation on Long-Term Lesion Durability for Atrial Fibrillation Ablation. JACC Clin. Electrophysiol. 2020, 6, 973–985. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.Y.; Dukkipati, S.R.; Neuzil, P.; Anic, A.; Petru, J.; Funasako, M.; Cochet, H.; Minami, K.; Breskovic, T.; Sikiric, I.; et al. Pulsed Field Ablation of Paroxysmal Atrial Fibrillation: 1-Year Outcomes of IMPULSE, PEFCAT, and PEFCAT II. JACC Clin. Electrophysiol. 2021, 7, 614–627. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lycke, M.; O’Neill, L.; Gillis, K.; Wielandts, J.-Y.; Le Polain De Waroux, J.-B.; Tavernier, R.; Knecht, S.; Duytschaever, M. How Close Are We toward an Optimal Balance in Safety and Efficacy in Catheter Ablation of Atrial Fibrillation? Lessons from the CLOSE Protocol. J. Clin. Med. 2021, 10, 4268. https://doi.org/10.3390/jcm10184268
Lycke M, O’Neill L, Gillis K, Wielandts J-Y, Le Polain De Waroux J-B, Tavernier R, Knecht S, Duytschaever M. How Close Are We toward an Optimal Balance in Safety and Efficacy in Catheter Ablation of Atrial Fibrillation? Lessons from the CLOSE Protocol. Journal of Clinical Medicine. 2021; 10(18):4268. https://doi.org/10.3390/jcm10184268
Chicago/Turabian StyleLycke, Michelle, Louisa O’Neill, Kris Gillis, Jean-Yves Wielandts, Jean-Benoit Le Polain De Waroux, Rene Tavernier, Sebastien Knecht, and Mattias Duytschaever. 2021. "How Close Are We toward an Optimal Balance in Safety and Efficacy in Catheter Ablation of Atrial Fibrillation? Lessons from the CLOSE Protocol" Journal of Clinical Medicine 10, no. 18: 4268. https://doi.org/10.3390/jcm10184268
APA StyleLycke, M., O’Neill, L., Gillis, K., Wielandts, J.-Y., Le Polain De Waroux, J.-B., Tavernier, R., Knecht, S., & Duytschaever, M. (2021). How Close Are We toward an Optimal Balance in Safety and Efficacy in Catheter Ablation of Atrial Fibrillation? Lessons from the CLOSE Protocol. Journal of Clinical Medicine, 10(18), 4268. https://doi.org/10.3390/jcm10184268