
Auricular Acupressure Combined with Self-Help Intervention for Treating Chronic Tinnitus: A Longitudinal Observational Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Description
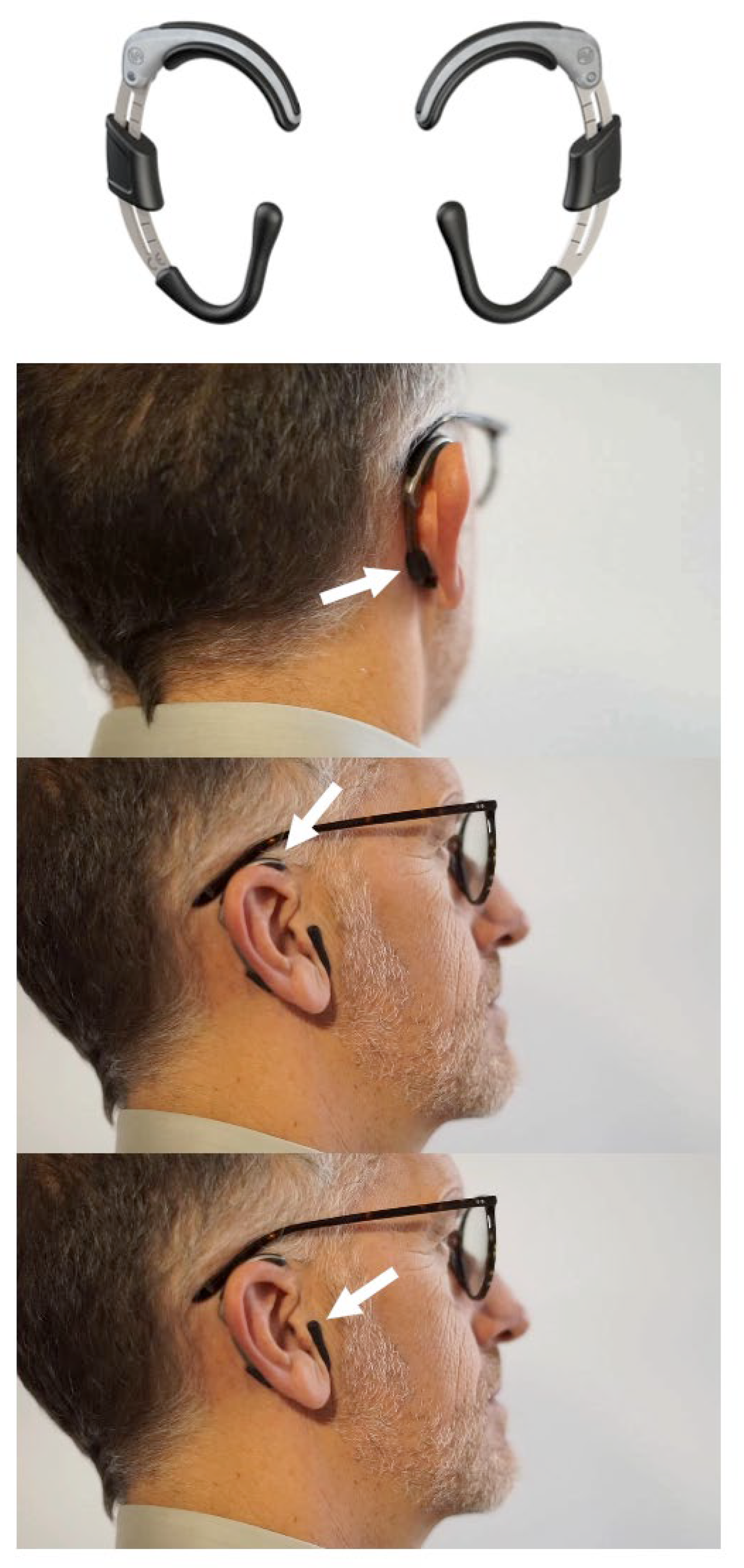
2.2. Combined Treatment
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
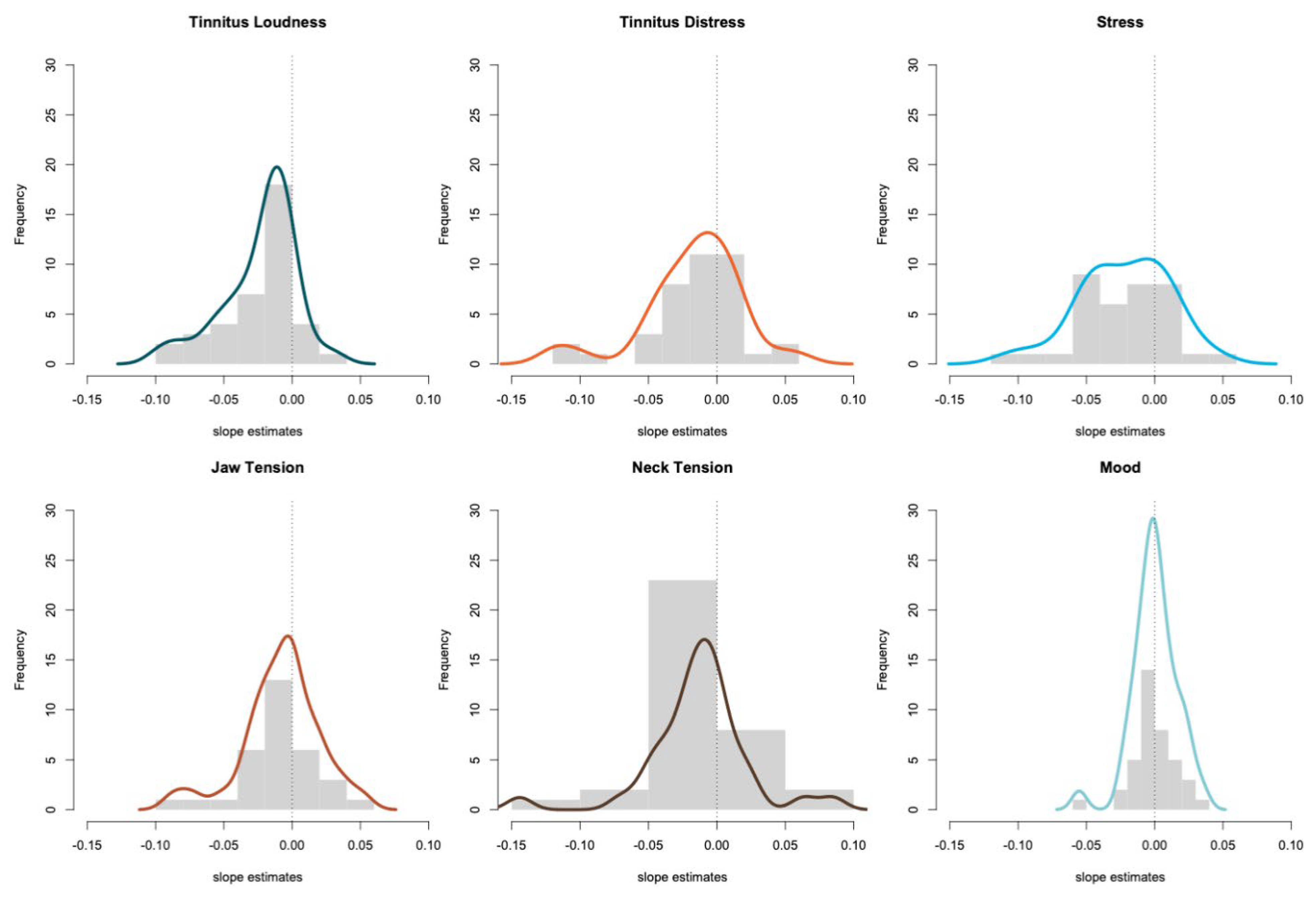
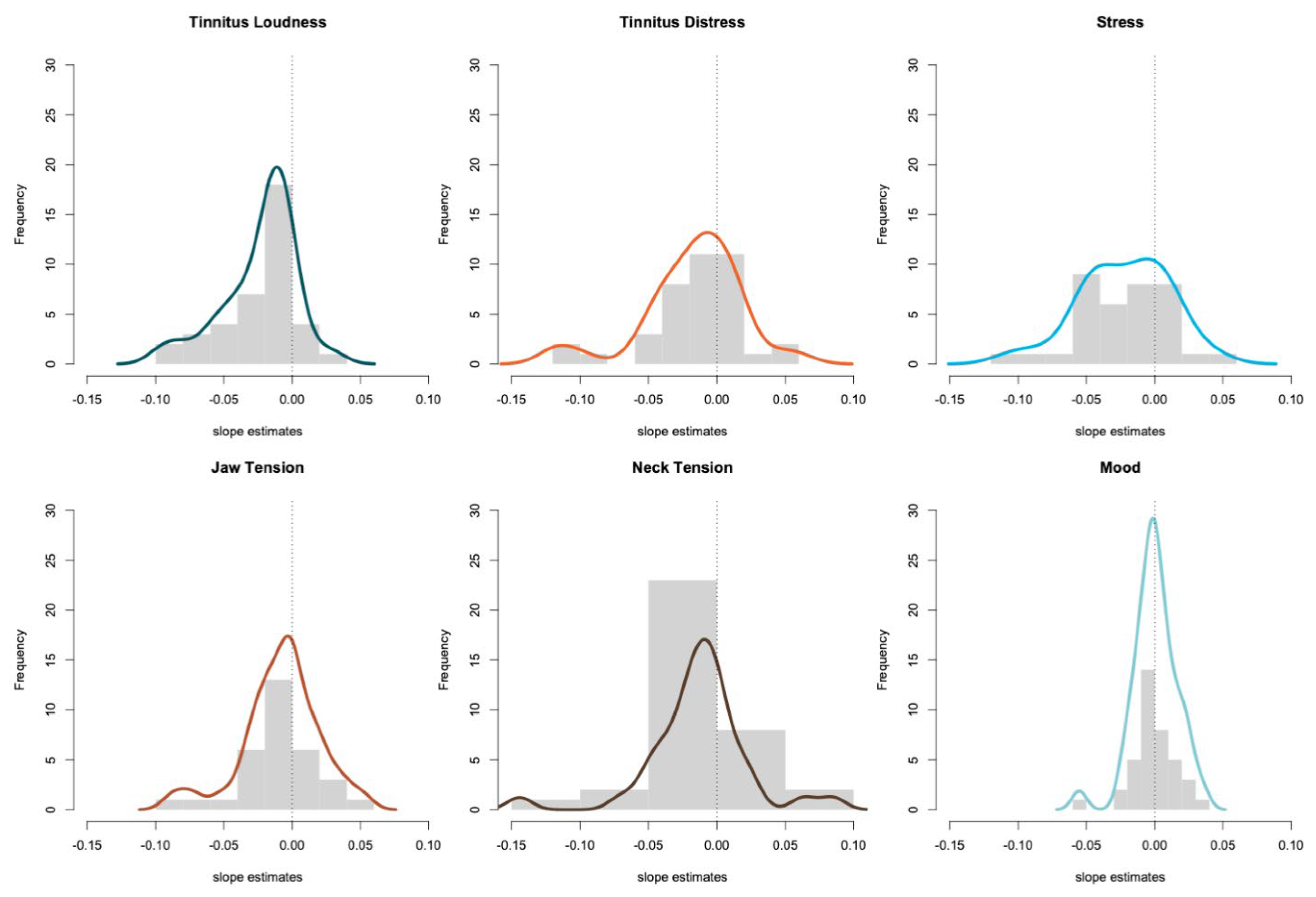
3.2. Description of the Individual Tinnitus Trajectories and Trend Analysis
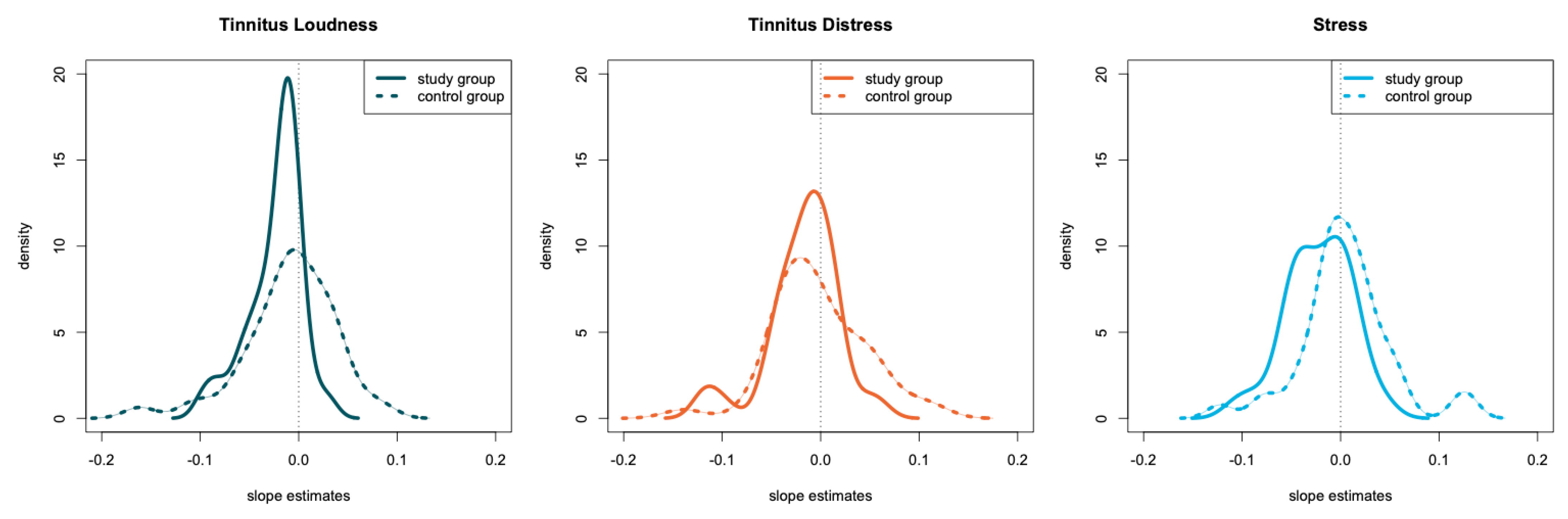
3.3. Comparison between the Study Group to a Matched Control Group
4. Discussion
4.1. Change of Tinnitus Loudness and Distress
4.2. Changes of Tensions in the Jaw and Neck Muscles
4.3. Changes in Mood
4.4. Changes of Stress
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McCormack, A.; Edmondson-Jones, M.; Somerset, S.; Hall, D. A systematic review of the reporting of tinnitus prevalence and severity. Hear. Res. 2016, 337, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Freni, F.; Gazia, F.; Slavutsky, V.; Scherdel, E.P.; Nicenboim, L.; Posada, R.; Portelli, D.; Galletti, B.; Galletti, F. Cochlear Implant Surgery: Endomeatal Approach versus Posterior Tympanotomy. Int. J. Environ. Res. Public Health 2020, 17, 4187. [Google Scholar] [CrossRef] [PubMed]
- Elgoyhen, A.B.; Langguth, B.; De Ridder, D.; Vanneste, S. Tinnitus: Perspectives from human neuroimaging. Nat. Rev. Neurosci. 2015, 16, 632–642. [Google Scholar] [CrossRef] [PubMed]
- Baguley, D.; McFerran, D.; Hall, D. Tinnitus. Lancet 2013, 382, 1600–1607. [Google Scholar] [CrossRef] [Green Version]
- Michiels, S.; Nieste, E.; Van De Heyning, P.; Braem, M.; Visscher, C.; Topsakal, V.; Gilles, A.; Jacquemin, L.; De Hertogh, W. Does Conservative Temporomandibular Therapy Affect Tinnitus Complaints? A Systematic Review. J. Oral Facial Pain Headache 2019, 33, 308–317. [Google Scholar] [CrossRef]
- Tegg-Quinn, S.; Bennett, R.; Eikelboom, R.; Baguley, D.M. The impact of tinnitus upon cognition in adults: A systematic review. Int. J. Audiol. 2016, 55, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Salazar, J.; Meisel, K.; Smith, E.R.; Quiggle, A.; McCoy, D.B.; Amans, M.R. Depression in Patients with Tinnitus: A Systematic Review. Otolaryngol. Neck Surg. 2019, 161, 28–35. [Google Scholar] [CrossRef]
- Mazurek, B.; Szczepek, A.J.; Hebert, S. Stress Und Tinnitus. HNO 2015, 63, 258–265. [Google Scholar] [CrossRef]
- McKenna, L.; Marks, E.M.; Hallsworth, C.; Schaette, R. Mindfulness-Based Cognitive Therapy as a Treatment for Chronic Tinnitus: A Randomized Controlled Trial. Psychother. Psychosom. 2017, 86, 351–361. [Google Scholar] [CrossRef] [Green Version]
- Kreuzer, P.M.; Vielsmeier, V.; Langguth, B. Chronic Tinnitus: An Interdisciplinary Challenge. Dtsch. Ärzteblatt Int. 2013, 110, 278. [Google Scholar]
- Probst, T.; Pryss, R.; Langguth, B.; Schlee, W. Emotional states as mediators between tinnitus loudness and tinnitus distress in daily life: Results from the “TrackYourTinnitus” application. Sci. Rep. 2016, 6, 20382. [Google Scholar] [CrossRef] [Green Version]
- Probst, T.; Pryss, R.; Langguth, B.; Schlee, W. Emotion dynamics and tinnitus: Daily life data from the “TrackYourTinnitus” application. Sci. Rep. 2016, 6, 31166. [Google Scholar] [CrossRef] [Green Version]
- Beukes, E.W.; Baguley, D.M.; Jacquemin, L.; Lourenco, M.P.C.G.; Allen, P.M.; Onozuka, J.; Stockdale, D.; Kaldo, V.; Andersson, G.; Manchaiah, V. Changes in Tinnitus Experiences during the COVID-19 Pandemic. Front. Public Health 2020, 8, 592878. [Google Scholar] [CrossRef]
- Schlee, W.; Hølleland, S.; Bulla, J.; Simoes, J.; Neff, P.; Schoisswohl, S.; Woelflick, S.; Schecklmann, M.; Schiller, A.; Staudinger, S.; et al. The Effect of Environmental Stressors on Tinnitus: A Prospective Longitudinal Study on the Impact of the COVID-19 Pandemic. J. Clin. Med. 2020, 9, 2756. [Google Scholar] [CrossRef]
- Nyenhuis, N.; Golm, D.; Kröner-Herwig, B. A Systematic Review and Meta-Analysis on the Efficacy of Self-Help Interventions in Tinnitus. Cogn. Behav. Ther. 2013, 42, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Greenwell, K.; Sereda, M.; Coulson, N.S.; El Refaie, A.; Hoare, D. A systematic review of techniques and effects of self-help interventions for tinnitus: Application of taxonomies from health psychology. Int. J. Audiol. 2016, 55, 1–11. [Google Scholar] [CrossRef]
- Kalle, S.; Schlee, W.; Pryss, R.C.; Probst, T.; Reichert, M.; Langguth, B.; Spiliopoulou, M. Review of Smart Services for Tinnitus Self-Help, Diagnostics and Treatments. Front. Neurosci. 2018, 12, 541. [Google Scholar] [CrossRef] [PubMed]
- Langguth, B.; Goodey, R.; Azevedo, A.; Bjorne, A.; Cacace, A.; Crocetti, A.; Del Bo, L.; De Ridder, D.; Diges, I.; Elbert, T.; et al. Consensus for tinnitus patient assessment and treatment outcome measurement: Tinnitus Research Initiative meeting, Regensburg, July 2006. Prog. Brain Res. 2007, 166, 525–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Team, R.C. R: A Language and Environment for Statistical Computing. 2009. Available online: http://www.r-project.org (accessed on 16 September 2021).
- Torchiano, M. Effsize: Efficient Effect Size Computation. 2017. Available online: https://cran.r-project.org/web/packages/effsize/effsize.pdf (accessed on 16 September 2021).
- Schlee, W.; Pryss, R.C.; Probst, T.; Schobel, J.; Bachmeier, A.; Reichert, M.; Langguth, B. Measuring the Moment-to-Moment Variability of Tinnitus: The TrackYourTinnitus Smart Phone App. Front. Aging Neurosci. 2016, 8, 294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Probst, T.; Pryss, R.C.; Langguth, B.; Rauschecker, J.P.; Schobel, J.; Reichert, M.; Spiliopoulou, M.; Schlee, W.; Zimmermann, J. Does Tinnitus Depend on Time-of-Day? An Ecological Momentary Assessment Study with the “TrackYourTinnitus” Application. Front. Aging Neurosci. 2017, 9, 253. [Google Scholar] [CrossRef] [Green Version]
- Rademaker, M.M.; Essers, B.A.B.; Stokroos, R.J.; Smit, A.L.; Stegeman, I. What Tinnitus Therapy Outcome Measures Are Important for Patients?—A Discrete Choice Experiment. Front. Neurol. 2021, 12, 668880. [Google Scholar] [CrossRef] [PubMed]
- Liugan, M.; Zhang, M.; Cakmak, Y.O. Neuroprosthetics for Auricular Muscles: Neural Networks and Clinical Aspects. Front. Neurol. 2018, 8, 752. [Google Scholar] [CrossRef] [Green Version]
- Flores-Orozco, E.I.; Tiznado-Orozco, G.E.; Díaz-Peña, R.; Orozco, E.I.F.; Galletti, C.; Gazia, F.; Galletti, F. Effect of a Mandibular Advancement Device on the Upper Airway in a Patient with Obstructive Sleep Apnea. J. Craniofac. Surg. 2020, 31, e32–e35. [Google Scholar] [CrossRef] [PubMed]
- Cha, N.H.; Park, Y.K.; Sok, S.R. Effects of Auricular Acupressure Therapy on Stress and Sleep Disturbance of Middle-Aged Women in South Korea. Holist. Nurs. Pract. 2017, 31, 102–109. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Question Number | German | English | Answer Options |
|---|---|---|---|
| 1 | Wie laut empfinden Sie den Tinnitus aktuell? | How loud do you currently feel the tinnitus? | visual slider on a scale from 0 (low) to 10 (high) |
| 2 | Wie belastend empfinden Sie den Tinnitus im Moment? | How stressful is the tinnitus at the moment? | visual slider on a scale from 0 (low) to 10 (high) |
| 3 | Wie ist ihre aktuelle Stimmungslage? | What is your current mood? | 5 smileys from very sad (rating 1) to very happy (rating 5) |
| 4 | Wie gestresst fühlen Sie sich gerade? | How stressed do you feel right now? | visual slider on a scale from 0 (no stress) to 10 (maximum stress level) |
| 5 | Wie verspannt fühlt sich Ihr Kiefer gerade an? | How tense does your jaw feel right now? | visual slider on a scale from 0 (no at all tense) to 10 (very tense) |
| 6 | Wie verspannt fühlt sich Ihr Nacken gerade an? | How tense does your neck feel right now? | visual slider on a scale from 0 (no at all tense) to 10 (very tense) |
| Units | Study Group | |
|---|---|---|
| Total participants | Number of Participants | 39 |
| Sex ratio | Female:Male (% of enrolled) | 54.5%:45.5% |
| Age at Baseline | Years (mean (SD)) | 50.8 ± 14.6 |
| Tinnitus Duration | Years (mean (SD)) | 9.7 ± 11.9 |
| Device Usage | % of Days (mean (SD)) | 86.9% (±15.3) |
| Sampling points during the 6 weeks period | Mean ± SD (min; max) | 123.6 ± 79.4 (42; 371) |
| Symptom | Slope | p Value | Cohen’s d Effect Size |
|---|---|---|---|
| Tinnitus Loudness | −0.023 ± 0.027 | <0.001 | −0.861 |
| Tinnitus Distress | −0.018 ± 0.036 | 0.005 | −0.478 |
| Stress | −0.022 ± 0.033 | <0.001 | −0.675 |
| Tension in the jaw muscles | −0.008 ± 0.029 | 0.124 | −0.286 |
| Tension in the neck muscles | −0.013 ± 0.037 | 0.009 | −0.356 |
| Mood | 0.000 ± 0.016 | 0.929 | 0.010 |
| Symptom | Participants with A Significant Negative Trend | Participants with No Significant Trend | Participants with A Significant Positive Trend |
|---|---|---|---|
| Tinnitus Loudness | 15 (38.5%) | 23 (59.0%) | 1 (2.6%) |
| Tinnitus Distress | 11 (28.2%) | 24 (61.5%) | 4 (10.3%) |
| Stress | 14 (38.9%) | 20 (55.6%) | 2 (5.6%) |
| Tension in the jaw muscles | 13 (40.6%) | 13 (40.6%) | 6 (18.8%) |
| Tension in the neck muscles | 14 (38.9%) | 18 (50.0%) | 4 (11.1%) |
| Mood | 3 (7.7%) | 32 (82.1%) | 4 (10.3%) |
| Units | Study Group | Matched Control Group | p Value | |
|---|---|---|---|---|
| Total participants | Number of Participants | 39 | 39 | 1 |
| Sex ratio | Female:Male (% of enrolled) | 54.5%:45.5% | 63.2%:36.8% | 0.645 |
| Age at baseline | Years (mean (SD)) | 50.8 ± 14.6 | 51.3 ± 12.4 | 0.891 |
| Tinnitus duration | Years (mean (SD)) | 9.7 ± 11.9 | 9.7 ± 10.4 | 0.989 |
| Tinnitus loudness at baseline | Points (mean (SD)) | 6.5 ± 2.2 | 6.1 ± 2.7 | 0.407 |
| Tinnitus distress at baseline | Points (mean (SD)) | 5.6 ± 2.7 | 5.6 ± 2.7 | 0.947 |
| Hearing problem | Number of Participants | 9 | 11 | 0.795 |
| Hearing aid users | Number of Participants | 3 | 4 | 1 |
| Symptom | Slope Study Group | Slope Matched Control Group | p Values |
|---|---|---|---|
| Tinnitus Loudness | −0.023 ± 0.027 | −0.009 ± 0.047 | 0.027 |
| Tinnitus Distress | −0.018 ± 0.036 | −0.002 ± 0.048 | 0.252 |
| Stress | −0.022 ± 0.033 | 0.005 ± 0.047 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schlee, W.; Simoes, J.; Pryss, R. Auricular Acupressure Combined with Self-Help Intervention for Treating Chronic Tinnitus: A Longitudinal Observational Study. J. Clin. Med. 2021, 10, 4201. https://doi.org/10.3390/jcm10184201
Schlee W, Simoes J, Pryss R. Auricular Acupressure Combined with Self-Help Intervention for Treating Chronic Tinnitus: A Longitudinal Observational Study. Journal of Clinical Medicine. 2021; 10(18):4201. https://doi.org/10.3390/jcm10184201
Chicago/Turabian StyleSchlee, Winfried, Jorge Simoes, and Rüdiger Pryss. 2021. "Auricular Acupressure Combined with Self-Help Intervention for Treating Chronic Tinnitus: A Longitudinal Observational Study" Journal of Clinical Medicine 10, no. 18: 4201. https://doi.org/10.3390/jcm10184201
APA StyleSchlee, W., Simoes, J., & Pryss, R. (2021). Auricular Acupressure Combined with Self-Help Intervention for Treating Chronic Tinnitus: A Longitudinal Observational Study. Journal of Clinical Medicine, 10(18), 4201. https://doi.org/10.3390/jcm10184201