
Impact of the Coronavirus Disease-2019 Pandemic on Pancreaticobiliary Disease Detection and Treatment

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Infection Protection Measures of Endoscopic for Coronavirus in Our Hospital
2.3. Statistical Analysis
3. Results
3.1. Details of Newly Diagnosed Pancreaticobiliary Cancer at Each Period
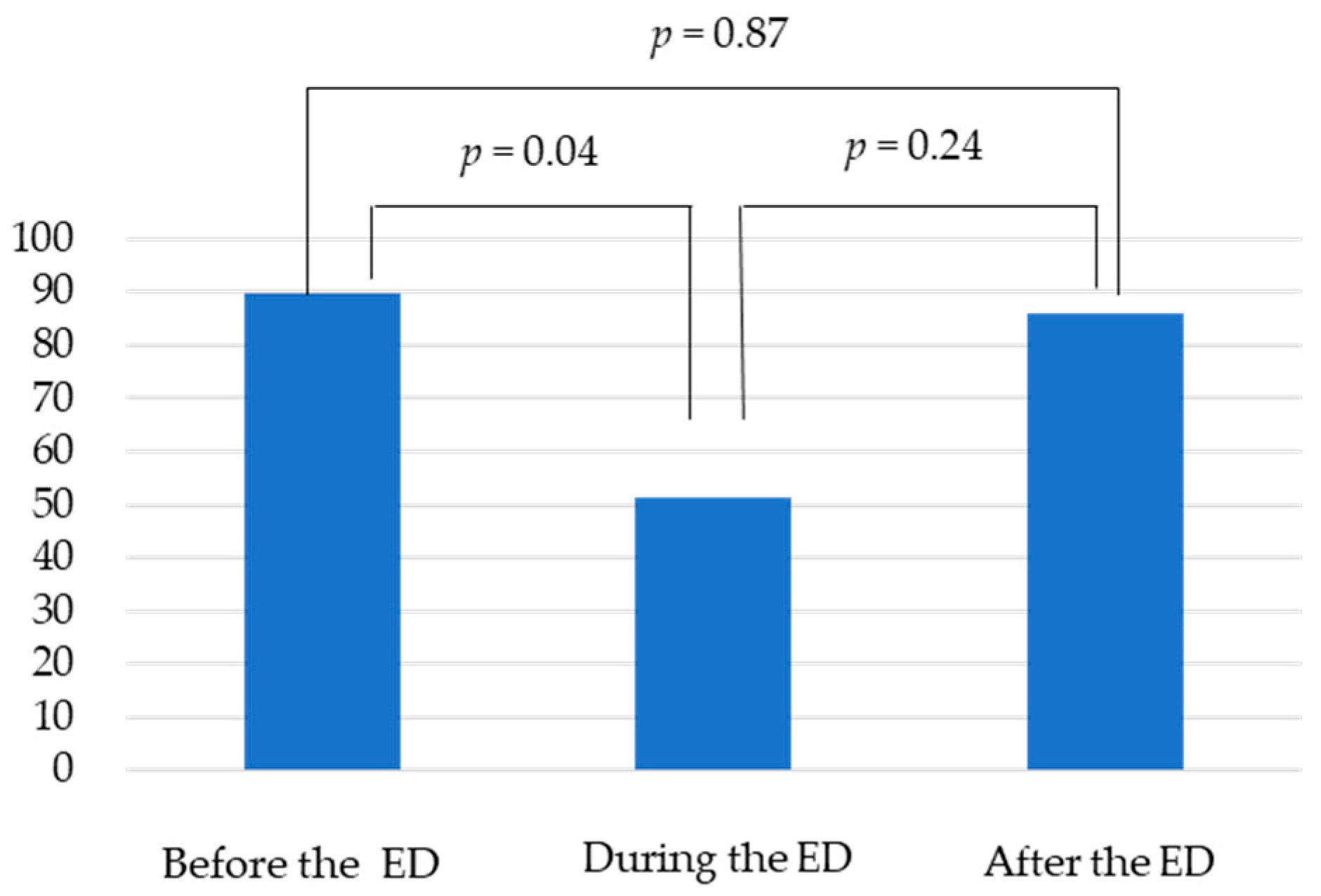
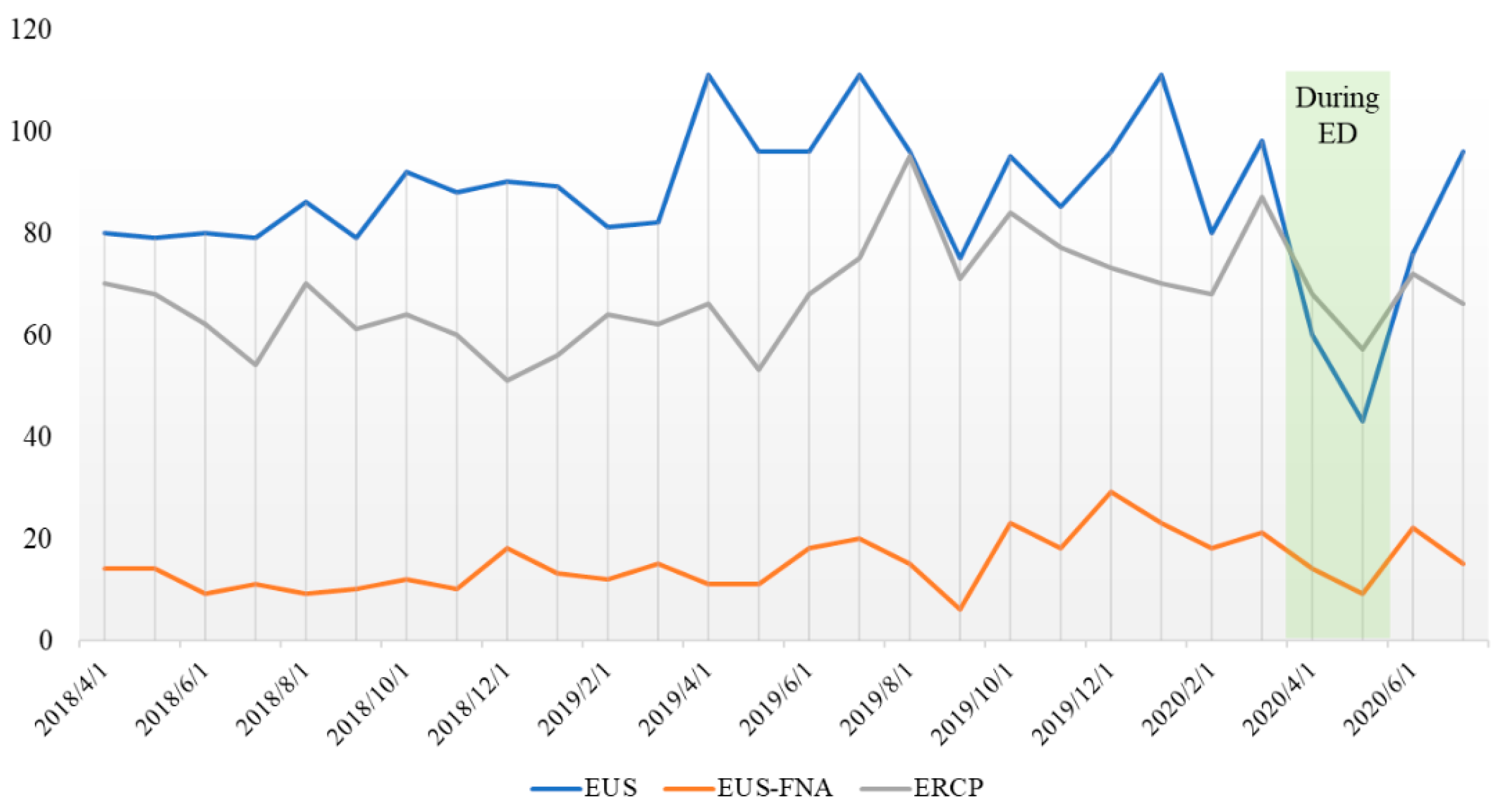
3.2. The Average Number of Biliary and Pancreatic Endoscopes at Each Period (Monthly Average)
3.3. The Breakdown of ERCP during and Post Emergency Declaration (Monthly Average)
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Yu, I.T.; Li, Y.; Wong, T.W.; Tam, W.; Chan, A.; Lee, J.H.; Leung, D.Y.; Ho, T. Evidence of Airborne Transmission of the Severe Acute Respiratory Syndrome Virus. N. Engl. J. Med. 2004, 350, 1731–1739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Du, G. COVID-19 may transmit through aerosol. Ir. J. Med. Sci. 2020, 189, 1143–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.; Han, B.; Wang, J. COVID-19: Gastrointestinal Manifestations and Potential Fecal–Oral Transmission. Gastroenterology 2020, 158, 1518–1519. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.H.; Lui, R.N.; Sung, J.J. Covid-19 and the digestive system. J. Gastroenterol. Hepatol. 2020, 35, 744–748. [Google Scholar] [CrossRef] [PubMed]
- Lui, T.K.L.; Leung, K.; Guo, C.G.; Tsui, V.W.M.; Wu, J.T.; Leung, W.K. Impacts of the Coronavirus 2019 Pandemic on Gastrointesti-nal Endoscopy Volume and Diagnosis of Gastric and Colorectal Cancers: A Population-Based Study. Gastroenterology 2020, 159, 1164–1166.e1163. [Google Scholar] [CrossRef] [PubMed]
- Soetikno, R.; Teoh, A.Y.; Kaltenbach, T.; Lau, J.Y.; Asokkumar, R.; Cabral-Prodigalidad, P.; Shergill, A. Considerations in performing endoscopy during the COVID-19 pandemic. Gastrointest. Endosc. 2020, 92, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Repici, A.; Maselli, R.; Colombo, M.; Gabbiadini, R.; Spadaccini, M.; Anderloni, A.; Carrara, S.; Fugazza, A.; Di Leo, M.; Galtieri, P.A.; et al. Coronavirus (COVID-19) outbreak: What the department of endoscopy should know. Gastrointest. Endosc. 2020, 92, 192–197. [Google Scholar] [CrossRef] [Green Version]
- Prachand, V.N.; Milner, R.; Angelos, P.; Posner, M.C.; Fung, J.J.; Agrawal, N.; Jeevanandam, V.; Matthews, J.B. Medically Necessary, Time-Sensitive Procedures: Scoring System to Ethically and Efficiently Manage Resource Scarcity and Provider Risk During the COVID-19 Pandemic. J. Am. Coll. Surg. 2020, 231, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Buxbaum, J.L.; Abbas Fehmi, S.M.; Sultan, S.; Fishman, D.S.; Qumseya, B.J.; Cortessis, V.K. ASGE guideline on the role of endoscopy in the evaluation and manage-ment of choledocholithiasis. Gastrointest. Endosc. 2019, 89, 1075–1105.e1015. [Google Scholar] [CrossRef] [PubMed]
- Ang, T.L.; Li, J.W.; Vu CK, F.; Ho, G.H.; Chang, J.P.E.; Chong, C.H. Chapter of Gastroenterologists professional guidance on risk mitigation for gastrointes-tinal endoscopy during COVID-19 pandemic in Singapore. Singap. Med. J. 2020, 61, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Catanese, S.; Pentheroudakis, G.; Douillard, J.-Y.; Lordick, F. ESMO Management and treatment adapted recommendations in the COVID-19 era: Pancreatic Cancer. ESMO Open 2020, 5 (Suppl. 3), e000804. [Google Scholar] [CrossRef] [PubMed]
- Khamaysi, I.; Michlin, S. Increased mortality in patients waiting for biliary stent replacement during the COVID-19 pan-demic. Endoscopy 2020, 52, 708. [Google Scholar] [PubMed]
- Sultan, S.; Altayar, O.; Siddique, S.M.; Davitkov, P.; Feuerstein, J.D.; Lim, J.K.; Falck-Ytter, Y.; El-Serag, H.B. AGA Institute Rapid Review of the Gastrointestinal and Liver Manifestations of COVID-19, Meta-Analysis of International Data, and Recommendations for the Consultative Management of Patients with COVID-19. Gastroenterology 2020, 159, 320–334.e27. [Google Scholar] [CrossRef] [PubMed]
- Mao, R.; Qiu, Y.; He, J.-S.; Tan, J.-Y.; Li, X.-H.; Liang, J.; Shen, J.; Zhu, L.-R.; Chen, Y.; Iacucci, M.; et al. Manifestations and prognosis of gastrointestinal and liver involvement in patients with COVID-19: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 667–678. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Before the ED | During the ED | After the ED | p Value | |
|---|---|---|---|---|
| Duration | 1 April 2018–6 April 2020 | 7 April 2020–25 May 2020 | 26 May 2020–31 July 2020 | |
| PC cases, total | 96 | 15 | 15 | |
| PC cases, average/m | 8.0 | 7.5 | 7.5 | 0.5 |
| Age average | 69.6 | 69.7 | 71.6 | 0.3 |
| Sex (Male), % | 51.5 | 53.3 | 55.6 | 0.4 |
| Symptomatic case, % | 77.5 | 93.3 | 80 | 0.3 |
| Stage III/IV, % | 72.5 | 80 | 60 | 0.9 |
| BTC cases, total | 48 | 7 | 6 | |
| BTC cases, average/m | 4.0 | 3.5 | 3.0 | 0.9 |
| Age average | 71.8 | 71.4 | 71.8 | 0.3 |
| Sex (Male), % | 67.3 | 71.4 | 66.7 | 0.3 |
| Symptomatic case, % | 82.5 | 57.1 | 100 | 0.4 |
| Stage III/IV, % | 62 | 83 | 88 | 0.5 |
| Before the ED | During the ED | After the ED | p Value | |
|---|---|---|---|---|
| Duration | 1 April 2018–6 April 2020 | 7 April 2020–25 May 2020 | 26 May 2020–31 July 2020 | |
| EUS | 89.8 | 51.5 | 86.0 | 0.06 |
| EUS-FNA | 15.0 | 11.5 | 18.5 | 0.3 |
| ERCP | 67.8 | 62.5 | 69.0 | 0.7 |
| During the ED | After the ED | p Value | |
|---|---|---|---|
| Duration | 7 April 2020–25 May 2020 | 26 May 2020–31 July 2020 | |
| Malignant stricture | |||
| Diagnosis | 15.0 | 15.0 | 0.2 |
| Exchange stent | 10.0 | 9.0 | 0.6 |
| Benign stricture | |||
| Diagnosis | 1.0 | 5.0 | 0.3 |
| Exchange stent | 19.0 | 16.5 | 1.0 |
| CBDS | 11.5 | 15.0 | 0.2 |
| ETGBD | 0.5 | 2.0 | 0.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikemura, M.; Tomishima, K.; Ushio, M.; Takahashi, S.; Yamagata, W.; Takasaki, Y.; Suzuki, A.; Ito, K.; Ochiai, K.; Ishii, S.; et al. Impact of the Coronavirus Disease-2019 Pandemic on Pancreaticobiliary Disease Detection and Treatment. J. Clin. Med. 2021, 10, 4177. https://doi.org/10.3390/jcm10184177
Ikemura M, Tomishima K, Ushio M, Takahashi S, Yamagata W, Takasaki Y, Suzuki A, Ito K, Ochiai K, Ishii S, et al. Impact of the Coronavirus Disease-2019 Pandemic on Pancreaticobiliary Disease Detection and Treatment. Journal of Clinical Medicine. 2021; 10(18):4177. https://doi.org/10.3390/jcm10184177
Chicago/Turabian StyleIkemura, Muneo, Ko Tomishima, Mako Ushio, Sho Takahashi, Wataru Yamagata, Yusuke Takasaki, Akinori Suzuki, Koichi Ito, Kazushige Ochiai, Shigeto Ishii, and et al. 2021. "Impact of the Coronavirus Disease-2019 Pandemic on Pancreaticobiliary Disease Detection and Treatment" Journal of Clinical Medicine 10, no. 18: 4177. https://doi.org/10.3390/jcm10184177
APA StyleIkemura, M., Tomishima, K., Ushio, M., Takahashi, S., Yamagata, W., Takasaki, Y., Suzuki, A., Ito, K., Ochiai, K., Ishii, S., Saito, H., Fujisawa, T., Nagahara, A., & Isayama, H. (2021). Impact of the Coronavirus Disease-2019 Pandemic on Pancreaticobiliary Disease Detection and Treatment. Journal of Clinical Medicine, 10(18), 4177. https://doi.org/10.3390/jcm10184177