
IL-15 Is Overexpressed in γδ T Cells and Correlates with Disease Severity in Relapsing-Remitting Multiple Sclerosis

 ,
,  ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Flow Cytometry
2.3. Cell Sorting
2.4. RT-qPCR
2.5. Statistical Analysis
3. Results
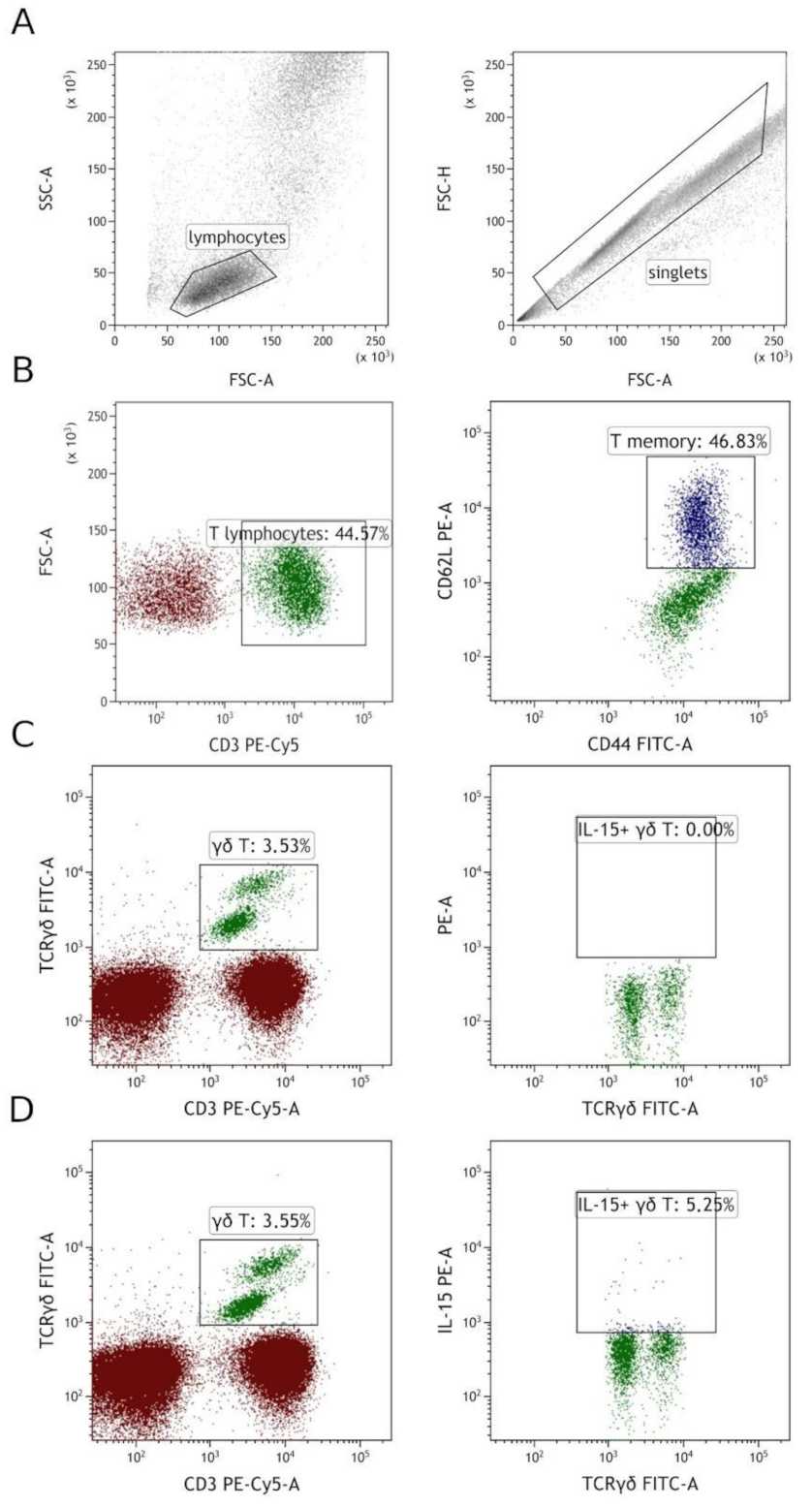
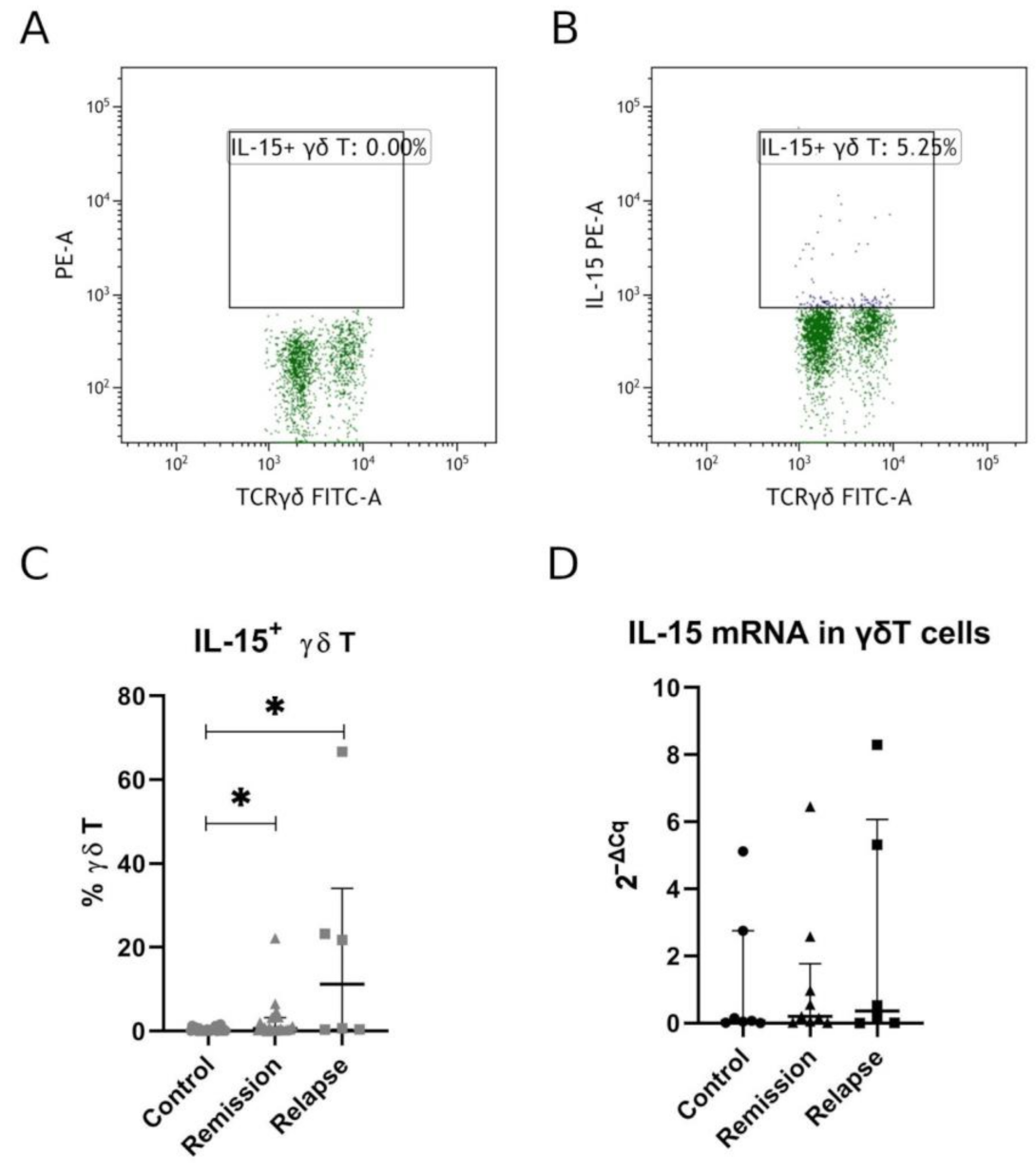
3.1. Human γδ T Express IL-15 and Are Significantly More Prevalent in MS Patients than Healthy Volunteers
3.2. IL-15 Expression by γδ T Was Confirmed by RT-qPCR
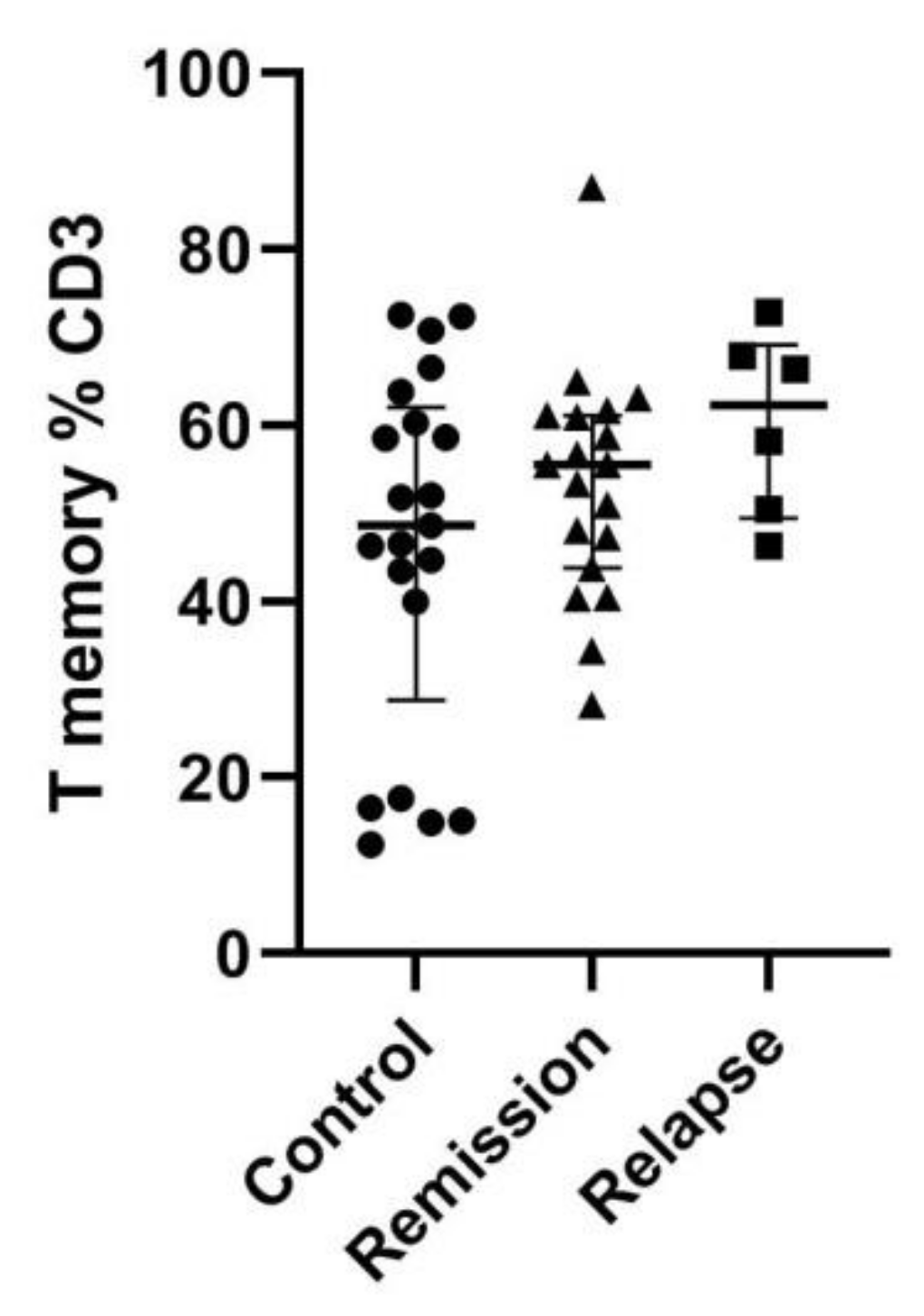
3.3. T Memory Cell Percentage Was Insignificantly Higher among MS Patients
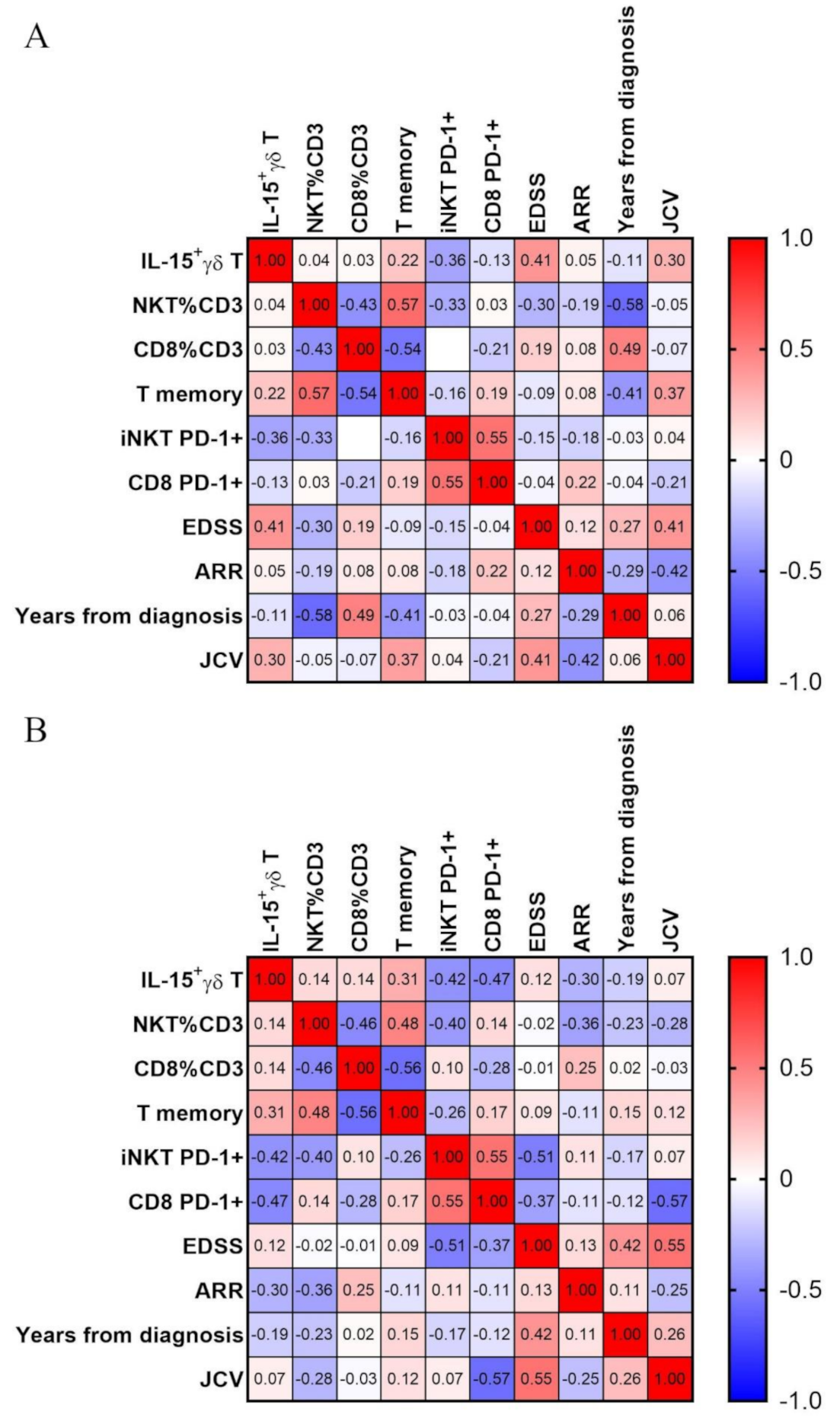
3.4. IL-15 Expressing γδ T Cells Positively Correlate with Disease Severity in MS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Browne, P.; Chandraratna, D.; Angood, C.; Tremlett, H.; Baker, C.; Taylor, B.V.; Thompson, A.J. Atlas of Multiple Sclerosis 2013: A Growing Global Problem with Widespread Inequity. Neurology 2014, 83, 1022–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, S.F. Overview and Diagnosis of Multiple Sclerosis. Am. J. Manag. Care 2016, 22, s141–s150. [Google Scholar] [PubMed]
- Hilt Pfleger, C.C.; Meulengracht Flachs, E.; Koch-Henriksen, N. Social Consequences of Multiple Sclerosis (1): Early Pension and Temporary Unemployment—A Historical Prospective Cohort Study. Mult. Scler. J. 2010, 16, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Valadkeviciene, D.; Jatuzis, D.; Kizlaitiene, R.; Zukauskaite, I.; Venceviciene, L. Working Capacity Level of Patients with Multiple Sclerosis in Lithuania: Its Dynamics and Relationship with the Employment and Lethal Outcomes. Mult. Scler. Relat. Disord. 2021, 49, 102784. [Google Scholar] [CrossRef]
- Kabelitz, D.; Lettau, M.; Janssen, O. Immunosurveillance by Human Γδ T Lymphocytes: The Emerging Role of Butyrophilins. F1000Research 2017, 6. [Google Scholar] [CrossRef] [Green Version]
- Pang, D.J.; Neves, J.F.; Sumaria, N.; Pennington, D.J. Understanding the Complexity of Γδ T-Cell Subsets in Mouse and Human. Immunology 2012, 136, 283–290. [Google Scholar] [CrossRef]
- Kenna, T.; Golden-Mason, L.; Norris, S.; Hegarty, J.E.; O’Farrelly, C.; Doherty, D.G. Distinct Subpopulations of Gamma Delta T Cells Are Present in Normal and Tumor-Bearing Human Liver. Clin. Immunol. 2004, 113, 56–63. [Google Scholar] [CrossRef]
- Clark, B.L.; Thomas, P.G. A Cell for the Ages: Human Γδ t Cells across the Lifespan. Int. J. Mol. Sci. 2020, 21, 8903. [Google Scholar] [CrossRef]
- Zheng, J.; Liu, Y.; Lau, Y.-L.; Tu, W. Γδ-T Cells: An Unpolished Sword in Human Anti-Infection Immunity. Cell. Mol. Immunol. 2013, 10, 50–57. [Google Scholar] [CrossRef]
- Zarobkiewicz, M.K.; Wawryk-Gawda, E.; Kowalska, W.; Janiszewska, M.; Bojarska-Junak, A. Γδ T Lymphocytes in Asthma: A Complicated Picture. Arch. Immunol. Ther. Exp. 2021, 69, 4. [Google Scholar] [CrossRef]
- Zarobkiewicz, M.K.; Kowalska, W.; Roliński, J.; Bojarska-Junak, A.A. Γδ T Lymphocytes in the Pathogenesis of Multiple Sclerosis and Experimental Autoimmune Encephalomyelitis. J. Neuroimmunol. 2019, 330, 67–73. [Google Scholar] [CrossRef]
- Bank, I. The Role of Gamma Delta T Cells in Autoimmune Rheumatic Diseases. Cells 2020, 9, 462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, P.; Bamford, R.N.; Waldmann, T.A. IL-15-Dependent CD8 + CD122 + T Cells Ameliorate Experimental Autoimmune Encephalomyelitis by Modulating IL-17 Production by CD4 + T Cells: Immunomodulation. Eur. J. Immunol. 2014, 44, 3330–3341. [Google Scholar] [CrossRef] [Green Version]
- Kivisäkk, P.; Matusevicius, D.; He, B.; Söderström, M.; Fredrikson, S.; Link, H. IL-15 MRNA Expression Is up-Regulated in Blood and Cerebrospinal Fluid Mononuclear Cells in Multiple Sclerosis (MS). Clin. Exp. Immunol. 1998, 111, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Rentzos, M.; Nikolaou, C.; Rombos, A.; Evangelopoulos, M.E.; Dimitrakopoulos, A.; Kararizou, E.; Koutsis, G.; Zoga, M.; Tsoutsou, A.; Sfangos, K. Circulating Interleukin-15 and RANTES Chemokine in MS Patients: Effect of Treatment with Methylprednisolone in Patients with Relapse. Neurol. Res. 2010, 32, 684–689. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wei, Y.; Liu, X.; Xing, C.; Han, G.; Chen, G.; Hou, C.; Dambuza, I.M.; Shen, B.; Li, Y.; et al. IL-15-Secreting γδ T Cells Induce Memory T Cells in Experimental Allergic Encephalomyelitis (EAE) Mice. Mol. Immunol. 2015, 66, 402–408. [Google Scholar] [CrossRef]
- Zarobkiewicz, M.K.; Kowalska, W.; Halczuk, P.; Woś, J.; Jodłowska-Jędrych, B.; Rejdak, K.; Roliński, J.; Bojarska-Junak, A.A. RORγT Is Overexpressed in INKT and Γδ T Cells during Relapse in Relapsing-Remitting Multiple Sclerosis. J. Neuroimmunol. 2019, 337, 577046. [Google Scholar] [CrossRef] [PubMed]
- Bekkema, R.; Tadema, A.; Daenen, S.M.G.J.; Kluin-Nelemans, H.C.; Mulder, A.B. An Improved Flow Cytometric Method Using FACS Lysing Solution for Measurement of ZAP-70 Expression in B-Cell Chronic Lymphocytic Leukemia. Cytom. B Clin. Cytom. 2008, 74, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.H. Biostatistics 104: Correlational Analysis. Singapore Med. J. 2003, 44, 614–619. [Google Scholar]
- Pashenkov, M.; Mustafa, M.; Kivisäkk, P.; Link, H. Levels of Interleukin-15-Expressing Blood Mononuclear Cells Are Elevated in Multiple Sclerosis. Scand. J. Immunol. 1999, 50, 303–309. [Google Scholar]
- Allard-Chamard, H.; Mishra, H.K.; Nandi, M.; Mayhue, M.; Menendez, A.; Ilangumaran, S.; Ramanathan, S. Interleukin-15 in Autoimmunity. Cytokine 2020, 136, 155258. [Google Scholar] [CrossRef] [PubMed]
- Schneider, R.; Mohebiany, A.N.; Ifergan, I.; Beauseigle, D.; Duquette, P.; Prat, A.; Arbour, N. B Cell-Derived IL-15 Enhances CD8 T Cell Cytotoxicity and Is Increased in Multiple Sclerosis Patients. J. Immunol. 2011, 187, 4119–4128. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Nicola, D.; Spagnolo, A.; Guaza, C.; Nieto-Sampedro, M. Aggravated Experimental Autoimmune Encephalomyelitis in IL-15 Knockout Mice. Exp. Neurol. 2010, 222, 235–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.; Pan, W.; He, Y.; Hsuchou, H.; Kastin, A.J. Cerebral Interleukin-15 Shows Upregulation and Beneficial Effects in Experimental Autoimmune Encephalomyelitis. J. Neuroimmunol. 2010, 223, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurent, C.; Deblois, G.; Clénet, M.-L.; Moratalla, A.C.; Farzam-kia, N.; Girard, M.; Duquette, P.; Prat, A.; Larochelle, C.; Arbour, N. Interleukin-15 Enhances Proinflammatory T-Cell Responses in Patients with MS and EAE. Neurol. Neuroimmunol. Neuroinflamm. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Saikali, P.; Antel, J.P.; Pittet, C.L.; Newcombe, J.; Arbour, N. Contribution of Astrocyte-Derived IL-15 to CD8 T Cell Effector Functions in Multiple Sclerosis. J. Immunol. 2010, 185, 5693–5703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aehnlich, P.; Carnaz Simões, A.M.; Skadborg, S.K.; Holmen Olofsson, G.; thor Straten, P. Expansion With IL-15 Increases Cytotoxicity of Vγ9Vδ2 T Cells and Is Associated With Higher Levels of Cytotoxic Molecules and T-Bet. Front. Immunol. 2020, 11, 1868. [Google Scholar] [CrossRef]
- Blanco-Jerez, C.; Plaza, J.F.; Masjuan, J.; Orensanz, L.M.; Alvarez-Cermeno, J.C. Increased Levels of IL-15 MRNA in Relapsing–Remitting Multiple Sclerosis Attacks. J. Neuroimmunol. 2002, 128, 90–94. [Google Scholar] [CrossRef]
- Khoy, K.; Mariotte, D.; Defer, G.; Petit, G.; Toutirais, O.; Le Mauff, B. Natalizumab in Multiple Sclerosis Treatment: From Biological Effects to Immune Monitoring. Front. Immunol. 2020, 11, 549842. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Nagarkatti, P.; Zhong, Y.; Nagarkatti, M. Characterization of T-Cell Memory Phenotype after in Vitro Expansion of Tumor-Infiltrating Lymphocytes from Melanoma Patients. Anticancer Res. 2011, 31, 4099–4109. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | % Women | Age | EDSS | ARR | Years from Diagnosis |
|---|---|---|---|---|---|
| MS | 68 | 39 (30.5–48) | 3.5 (3–5.75) | 0 (0–1) | 10 (4–14.5) |
| Healthy | 65 | 48 (26–58) | n/a | n/a | n/a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zarobkiewicz, M.K.; Kowalska, W.; Morawska, I.; Halczuk, P.; Rejdak, K.; Bojarska-Junak, A. IL-15 Is Overexpressed in γδ T Cells and Correlates with Disease Severity in Relapsing-Remitting Multiple Sclerosis. J. Clin. Med. 2021, 10, 4174. https://doi.org/10.3390/jcm10184174
Zarobkiewicz MK, Kowalska W, Morawska I, Halczuk P, Rejdak K, Bojarska-Junak A. IL-15 Is Overexpressed in γδ T Cells and Correlates with Disease Severity in Relapsing-Remitting Multiple Sclerosis. Journal of Clinical Medicine. 2021; 10(18):4174. https://doi.org/10.3390/jcm10184174
Chicago/Turabian StyleZarobkiewicz, Michał K., Wioleta Kowalska, Izabela Morawska, Paweł Halczuk, Konrad Rejdak, and Agnieszka Bojarska-Junak. 2021. "IL-15 Is Overexpressed in γδ T Cells and Correlates with Disease Severity in Relapsing-Remitting Multiple Sclerosis" Journal of Clinical Medicine 10, no. 18: 4174. https://doi.org/10.3390/jcm10184174
APA StyleZarobkiewicz, M. K., Kowalska, W., Morawska, I., Halczuk, P., Rejdak, K., & Bojarska-Junak, A. (2021). IL-15 Is Overexpressed in γδ T Cells and Correlates with Disease Severity in Relapsing-Remitting Multiple Sclerosis. Journal of Clinical Medicine, 10(18), 4174. https://doi.org/10.3390/jcm10184174