
TOUCH® Prosthesis for Thumb Carpometacarpal Joint Osteoarthritis: A Prospective Case Series

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
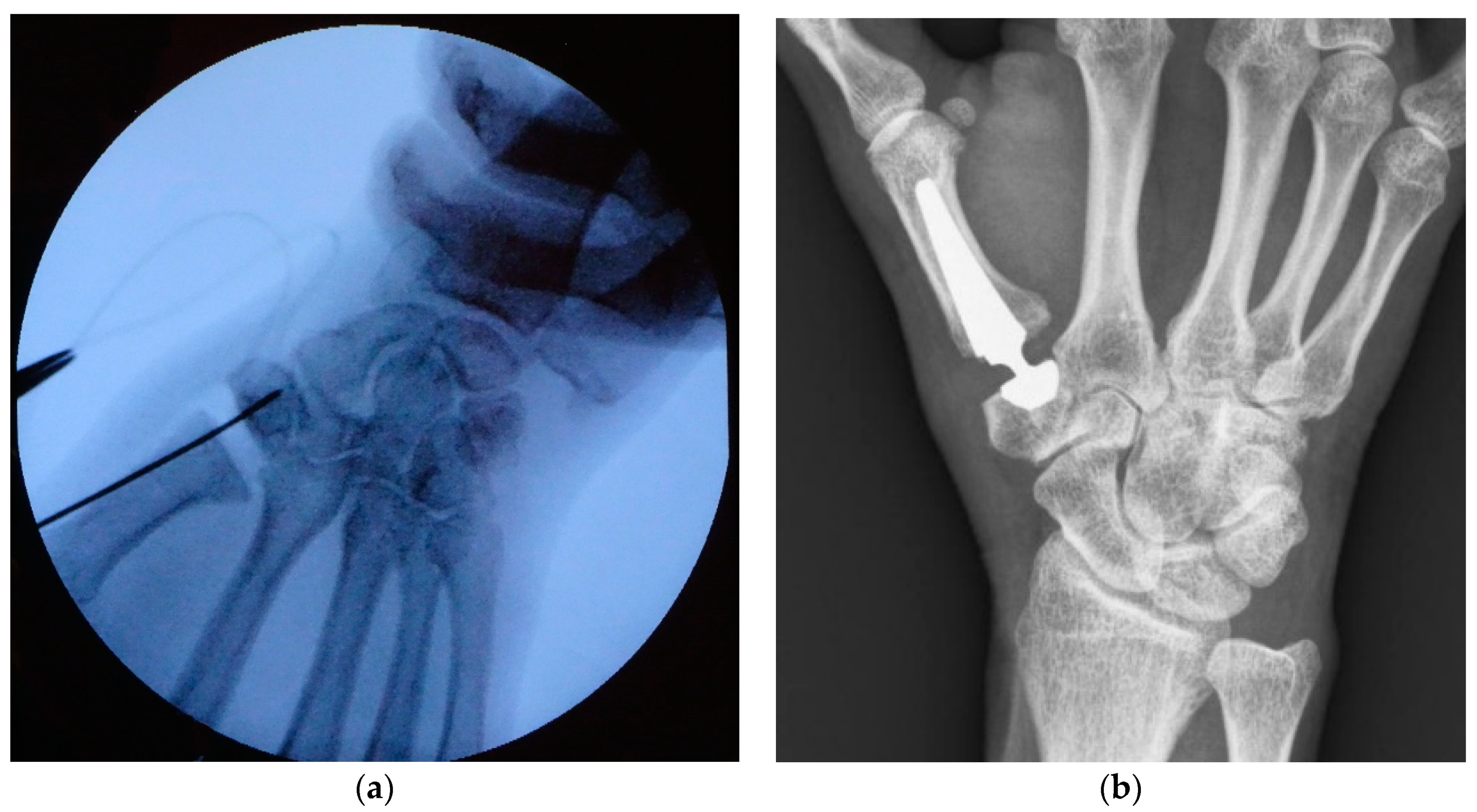
2.1. Surgical Technique
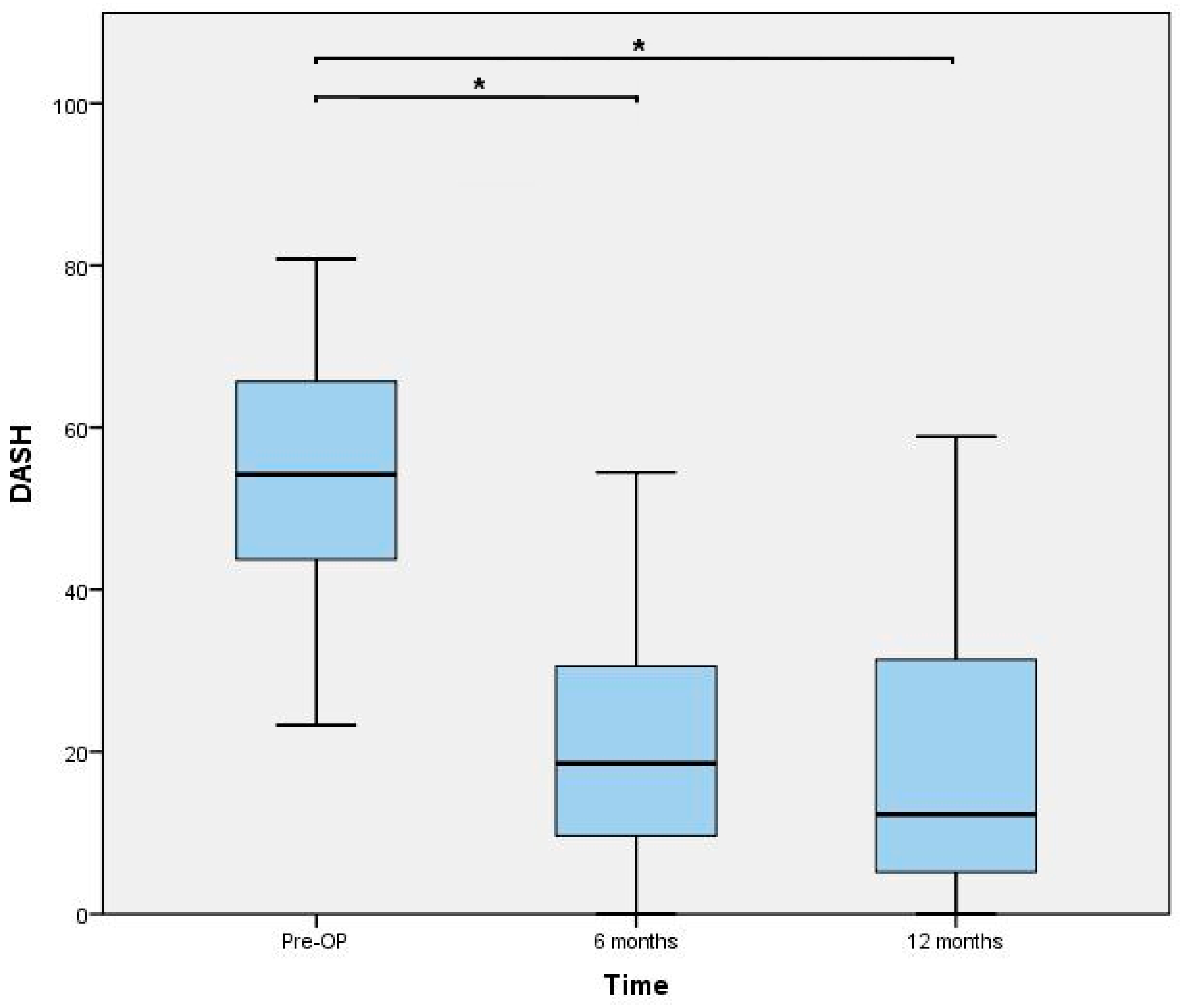
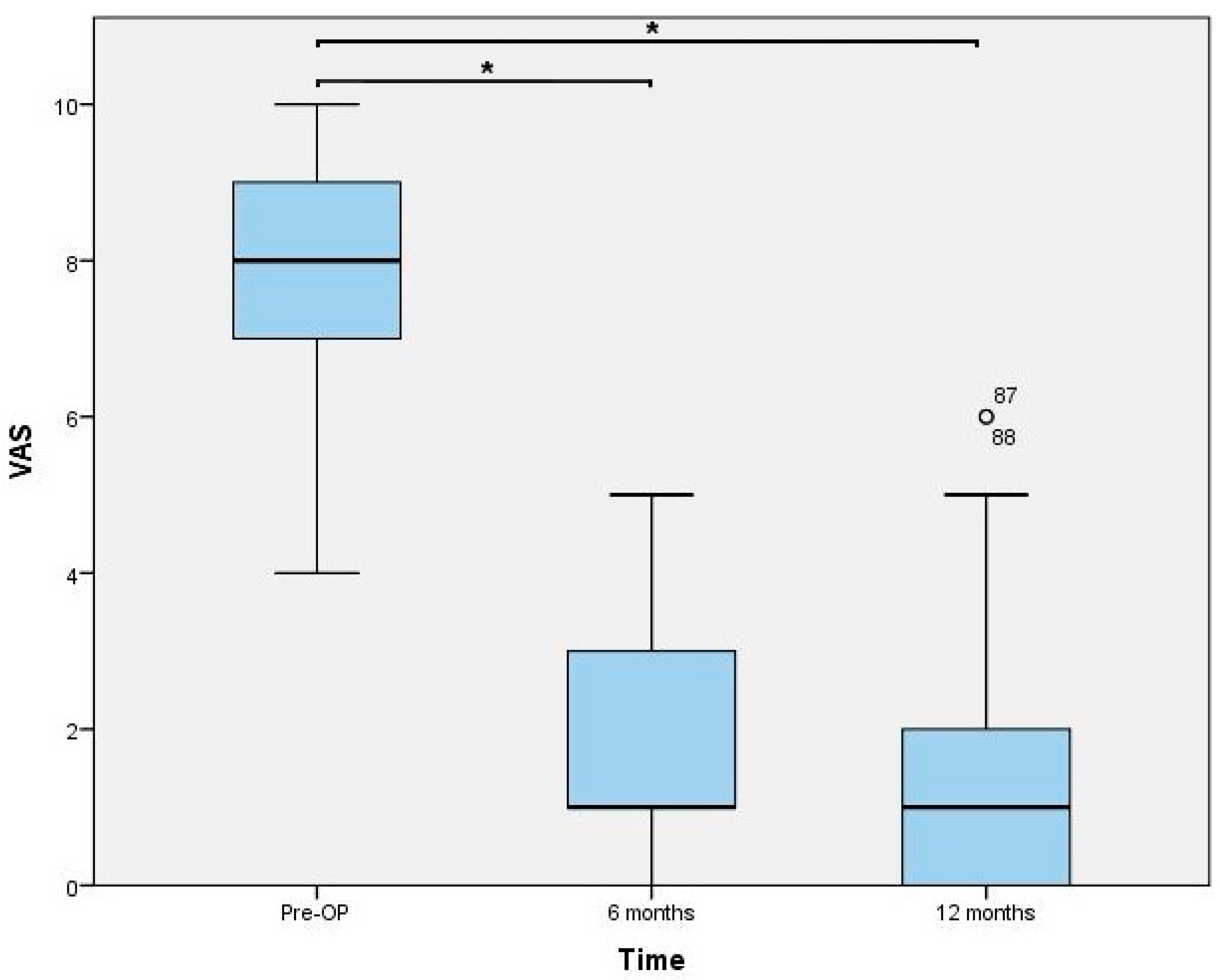
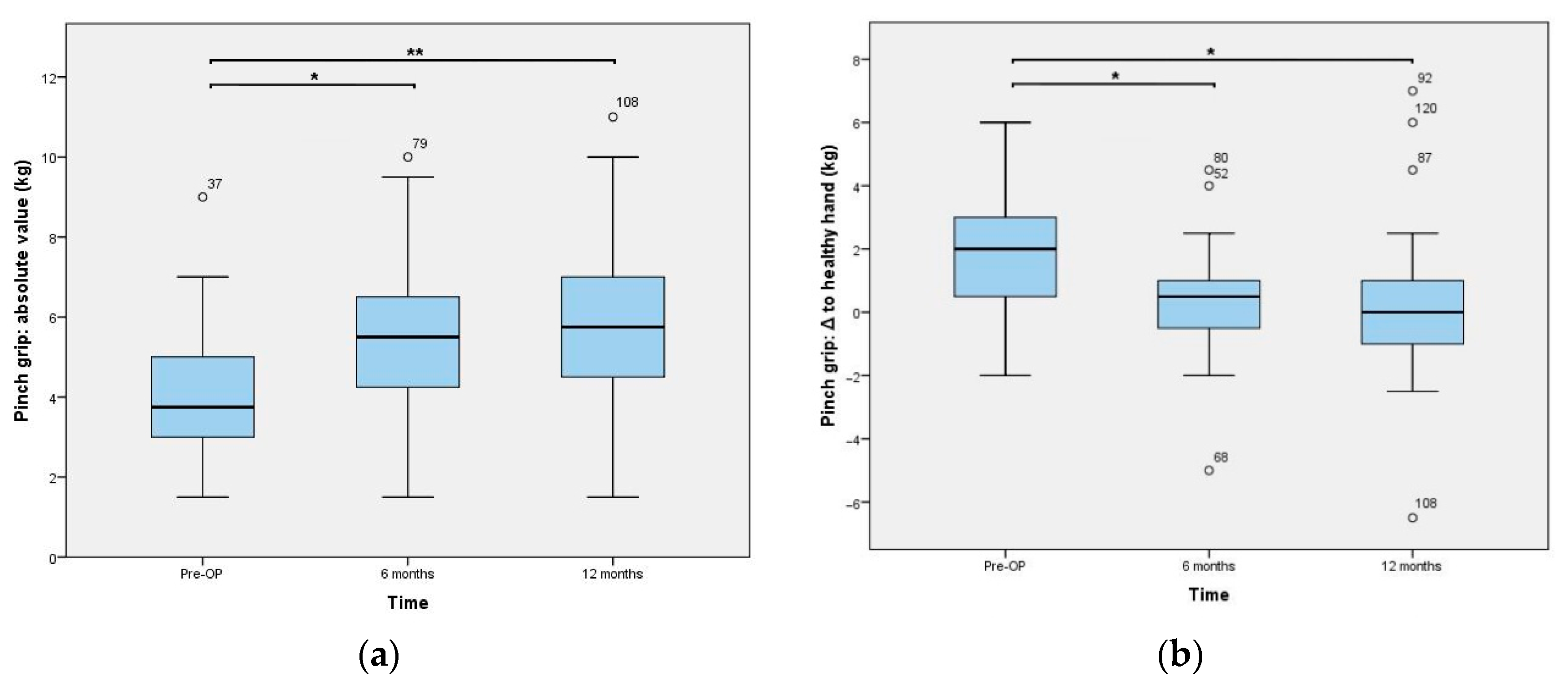
2.2. Clinical and Radiographical Evaluation
2.3. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polatsch, D.B.; Paksima, N. Basal joint arthritis: Diagnosis and treatment. Bull. NYU Hosp. Jt. Dis. 2006, 64, 178–184. [Google Scholar]
- Teissier, J.; Teissier, P.; Toffoli, A. Trapeziometacarpal prostheses. Hand Surg. Rehabil. 2021, 40, 106–116. [Google Scholar] [CrossRef]
- Huang, K.; Hollevoet, N.; Giddins, G. Thumb carpometacarpal joint total arthroplasty: A systematic review. J. Hand Surg. Eur. Vol. 2015, 40, 338–350. [Google Scholar] [CrossRef]
- Giddins, G. Thumb arthroplasties. J. Hand Surg. Eur. Vol. 2012, 37, 603–604. [Google Scholar] [CrossRef] [Green Version]
- de La Caffinière, J.Y. Prothèse totale trapézo-métacarpienne. Rev. Chir. Orthop. Reparatrice Appar. Mot. 1974, 60, 299–308. [Google Scholar] [PubMed]
- Noyer, D.; Caton, J.H. Once upon a time… Dual mobility: History. Int. Orthop. 2017, 41, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Eaton, R.G.; Littler, J.W. Ligament reconstruction for the painful thumb carpometacarpal joint. J. Bone Jt. Surg. Am. 1973, 55, 1655–1666. [Google Scholar] [CrossRef]
- Tang, J.B.; Giddins, G. Why and how to report surgeons’ levels of expertise. J. Hand Surg. Eur. Vol. 2016, 41, 365–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lussiez, B. Dual-mobility trapezio-metacarpal prosthesis—Biomechanical principle. Chir. Main. 2015, 34, 388–389. [Google Scholar] [CrossRef]
- Lussiez, B.; Ledoux, P.; Falaise, C. Prothèse trapèze-métacarpienne à double mobilité: Revue d’une série de 132 cas à plus de 1 an de recul. Rev. Chir. Orthopédique Traumatol. 2017, 103, S61. [Google Scholar] [CrossRef]
- Regnard, P.J. Electra trapezio metacarpal prosthesis: Results of the first 100 cases. J. Hand Surg. Br. 2006, 31, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Offenbächer, M.; Ewert, T.; Sangha, O.; Stucki, G. Validation of a German version of the ‘Disabilities of Arm, Shoulder and Hand’ questionnaire (DASH-G). Z. Rheumatol. 2003, 62, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Holzbauer, M.; Hopfner, M.; Haslhofer, D.; Kwasny, O.; Duscher, D.; Froschauer, S.M. Radial and palmar active range of motion measurement: Reliability of six methods in healthy adults. J. Plast. Surg. Hand Surg. 2021, 55, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, A.A.; Howard, D.; Tan, W.H.; Ketchersid, J.; Calfee, R.P. Minimal clinically important differences of 3 patient-rated outcomes instruments. J. Hand Surg. Am. 2013, 38, 641–649. [Google Scholar] [CrossRef] [Green Version]
- Lussiez, B.; Falaise, C.; Ledoux, P. Dual mobility trapeziometacarpal prosthesis: A prospective study of 107 cases with a follow-up of more than 3 years. J. Hand Surg. Eur. Vol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Martin-Ferrero, M. Ten-year long-term results of total joint arthroplasties with ARPE® implant in the treatment of trapeziometacarpal osteoarthritis. J. Hand Surg. Eur. Vol. 2014, 39, 826–832. [Google Scholar] [CrossRef] [Green Version]
- Cooney, W.P.; Chao, E.Y. Biomechanical analysis of static forces in the thumb during hand function. J. Bone Jt. Surg. Am. 1977, 59, 27–36. [Google Scholar] [CrossRef]
- Dumartinet-Gibaud, R.; Bigorre, N.; Raimbeau, G.; Jeudy, J.; Saint Cast, Y. Arpe total joint arthroplasty for trapeziometacarpal osteoarthritis: 80 thumbs in 63 patients with a minimum of 10 years follow-up. J. Hand. Surg. Eur. Vol. 2020, 45, 465–469. [Google Scholar] [CrossRef]
- Chevrollier, J.; Dap, F.; Lombard, J.; Dautel, G. Arthroplastie trapézométacarpienne à double mobilité Moovis—Résultats préliminaires à 1 an de recul d’une série prospective. Chir. Main. 2015, 34, 357–358. [Google Scholar] [CrossRef]
- Klahn, A.; Nygaard, M.; Gvozdenovic, R.; Boeckstyns, M.E.H. Elektra prosthesis for trapeziometacarpal osteoarthritis: A follow-up of 39 consecutive cases. J. Hand Surg. Eur. Vol. 2012, 37, 605–609. [Google Scholar] [CrossRef]
- Froschauer, S.M.; Holzbauer, M.; Hager, D.; Schnelzer, R.; Kwasny, O.; Duscher, D. Elektra prosthesis versus resection-suspension arthroplasty for thumb carpometacarpal osteoarthritis: A long-term cohort study. J. Hand Surg. Eur. Vol. 2019. [Google Scholar] [CrossRef]
- Gibon, E.; Córdova, L.A.; Lu, L.; Lin, T.-H.; Yao, Z.; Hamadouche, M.; Goodman, S.B. The biological response to orthopedic implants for joint replacement. II: Polyethylene, ceramics, PMMA, and the foreign body reaction. J. Biomed. Mater. Res. B Appl. Biomater. 2017, 105, 1685–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, T.B.; Dremstrup, L.; Stilling, M. Patients with metal-on-metal articulation in trapeziometacarpal total joint arthroplasty may have elevated serum chrome and cobalt. J. Hand Surg. Eur. Vol. 2013, 38, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Tchurukdichian, A.; Gerenton, B.; Moris, V.; See, L.-A.; Stivala, A.; Guillier, D. Outcomes of Double-Mobility Prosthesis in Trapeziometacarpal Joint Arthritis With a Minimal 3 Years of Follow-Up: An Advantage for Implant Stability. Hand 2021, 16, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Dreant, N.; Poumellec, M.-A. Total Thumb Carpometacarpal Joint Arthroplasty: A Retrospective Functional Study of 28 MOOVIS Prostheses. Hand 2019, 14, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.; Charbonnel, S.; Lecomte, F.; Athlani, L. The Moovis® implant for trapeziometacarpal osteoarthritis: Results after 2 to 6 years. J. Hand Surg. Eur. Vol. 2020, 45, 477–482. [Google Scholar] [CrossRef]
- Maes-Clavier, C.; David, E.; Biau, D.; Hustin, C.; Rotari, V. Évaluation de la courbe d’apprentissage des prothèses trapézométacarpiennes Maia par le LC-CUSUM Test. Chir. Main 2015, 34, 383. [Google Scholar] [CrossRef]
- Froschauer, S.M.; Holzbauer, M.; Schnelzer, R.F.; Behawy, M.; Kwasny, O.; Aitzetmüller, M.M.; Machens, H.-G.; Duscher, D. Total arthroplasty with Ivory® prosthesis versus resection-suspension arthroplasty: A retrospective cohort study on 82 carpometacarpal-I osteoarthritis patients over 4 years. Eur. J. Med. Res. 2020, 25, 13. [Google Scholar] [CrossRef] [Green Version]
- Spaans, A.J.; van Minnen, L.P.; Weijns, M.E.; Braakenburg, A.; van der Molen, A.B.M. Retrospective Study of a Series of 20 Ivory Prostheses in the Treatment of Trapeziometacarpal Osteoarthritis. J. Wrist Surg. 2016, 5, 131–136. [Google Scholar] [CrossRef] [Green Version]
- Kaszap, B.; Daecke, W.; Jung, M. High frequency failure of the Moje thumb carpometacarpal joint arthroplasty. J. Hand Surg. Eur. Vol. 2012, 37, 610–616. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Patients | 37 |
| Thumbs | 40 |
| Age | 57.7 (IQR: 13.6) |
| Sex (f/m) | 32/8 |
| Side (l/r) | 19/21 |
| dominant hand (l/r) | 1/39 |
| Pre-OP | 6 Months | 12 Months | |
|---|---|---|---|
| Thumbs (n) | 40 | 40 | 40 |
| Palmar abduction (°) | 50 (10) | 60 (5) | 60 (10) |
| Radial abduction (°) | 55 (10) | 60 (5) | 60 (5) |
| Opposition (cm) | 0.5 (1.8) | 0 (0) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Froschauer, S.M.; Holzbauer, M.; Mihalic, J.A.; Kwasny, O. TOUCH® Prosthesis for Thumb Carpometacarpal Joint Osteoarthritis: A Prospective Case Series. J. Clin. Med. 2021, 10, 4090. https://doi.org/10.3390/jcm10184090
Froschauer SM, Holzbauer M, Mihalic JA, Kwasny O. TOUCH® Prosthesis for Thumb Carpometacarpal Joint Osteoarthritis: A Prospective Case Series. Journal of Clinical Medicine. 2021; 10(18):4090. https://doi.org/10.3390/jcm10184090
Chicago/Turabian StyleFroschauer, Stefan M., Matthias Holzbauer, Julian A. Mihalic, and Oskar Kwasny. 2021. "TOUCH® Prosthesis for Thumb Carpometacarpal Joint Osteoarthritis: A Prospective Case Series" Journal of Clinical Medicine 10, no. 18: 4090. https://doi.org/10.3390/jcm10184090
APA StyleFroschauer, S. M., Holzbauer, M., Mihalic, J. A., & Kwasny, O. (2021). TOUCH® Prosthesis for Thumb Carpometacarpal Joint Osteoarthritis: A Prospective Case Series. Journal of Clinical Medicine, 10(18), 4090. https://doi.org/10.3390/jcm10184090