
Does Mandibular Gonial Angle Influence the Eruption Pattern of the Lower Third Molar? A Three-Dimensional Study

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Sample
2.3. Data Collection Method
2.4. Study Variables and Outcomes
2.5. Statistical Analysis
3. Results
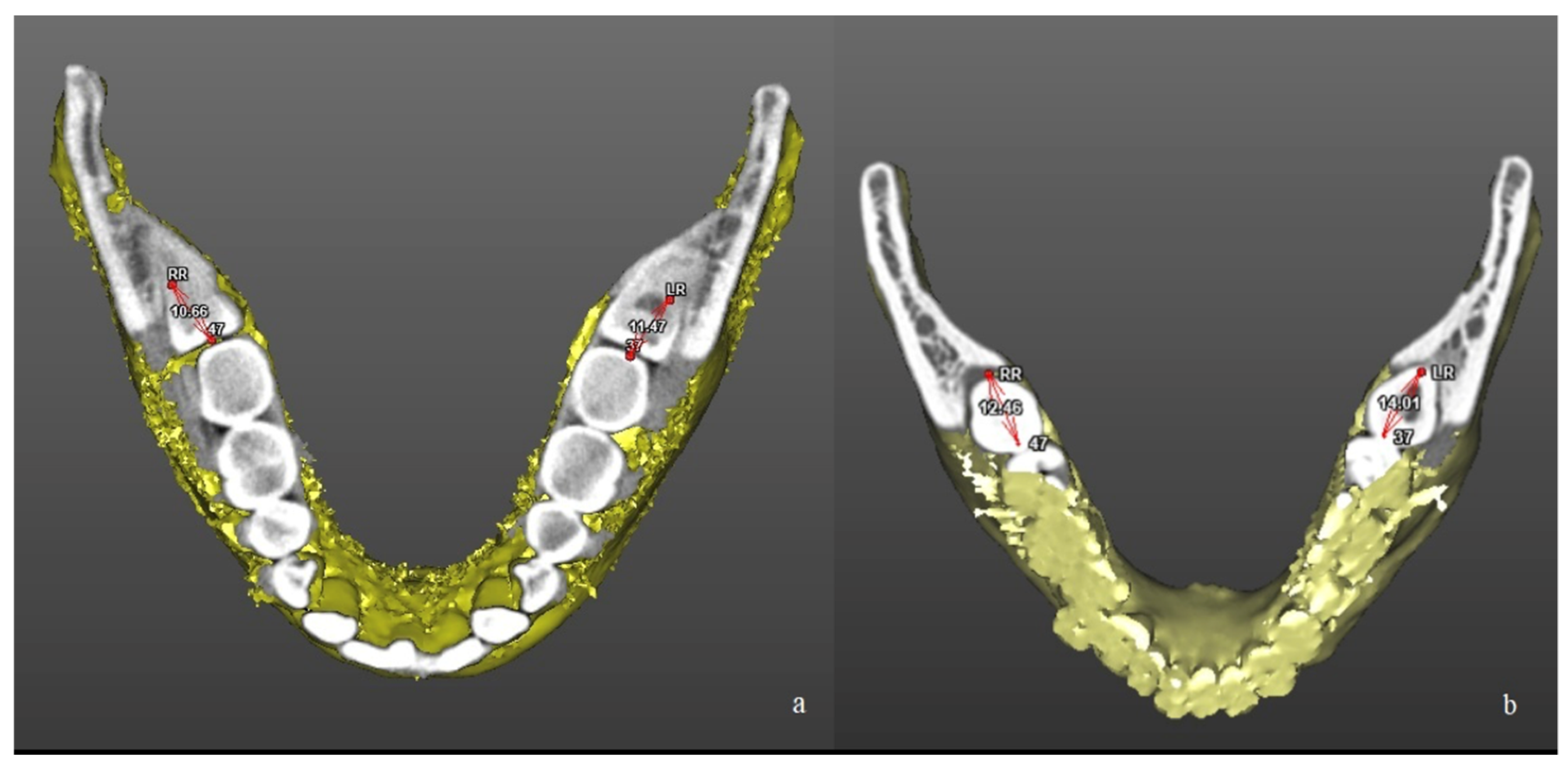
- Position of M3M in relation to M2M—M
- Position of M3M in relation to mandibular ramus—R
- Position of M3M in relation to alveolar crest—A
- Position of M3M in relation to inferior alveolar nerve—C
- Position of M3M in relation to buccal or lingual wall—B
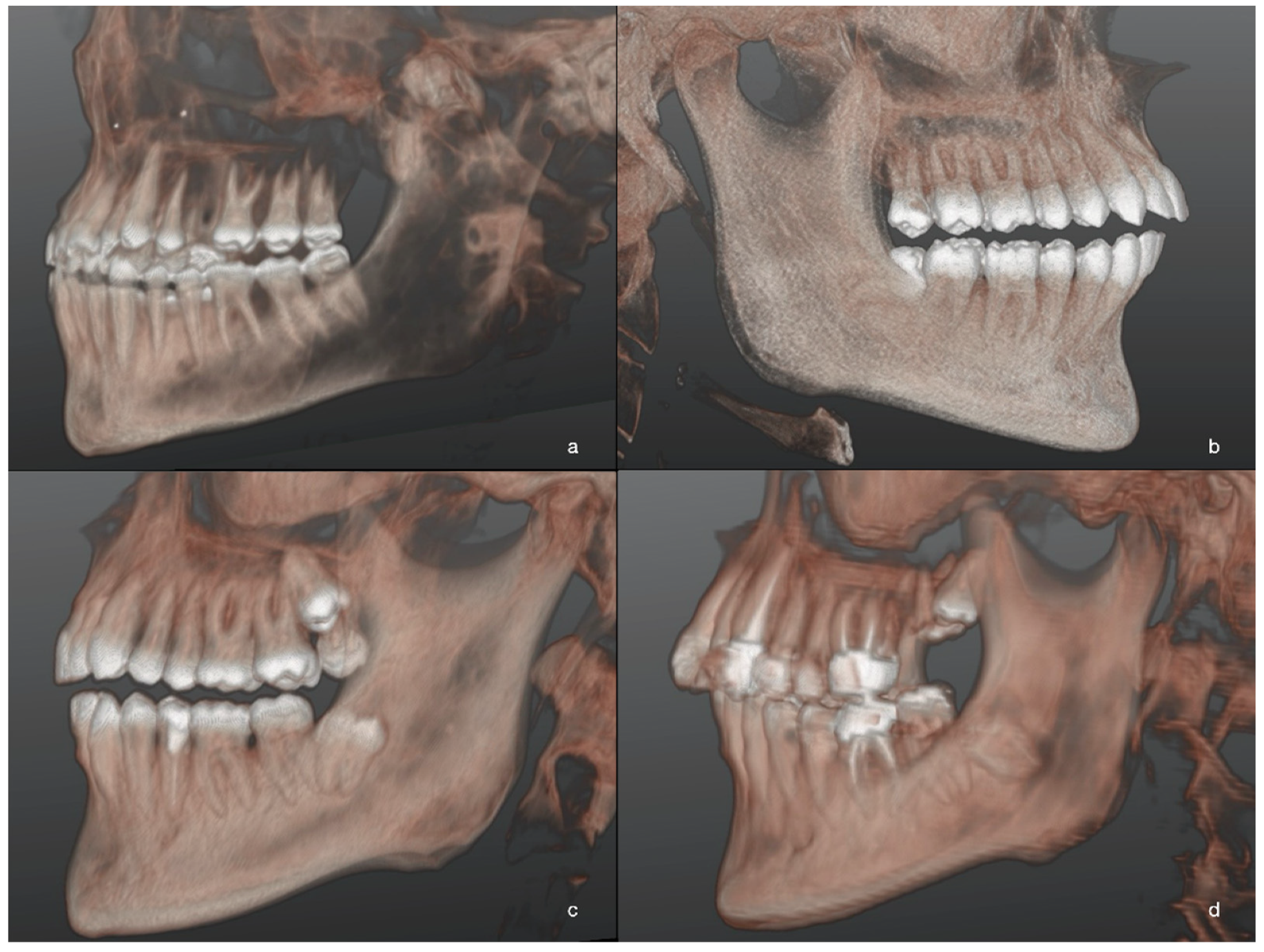
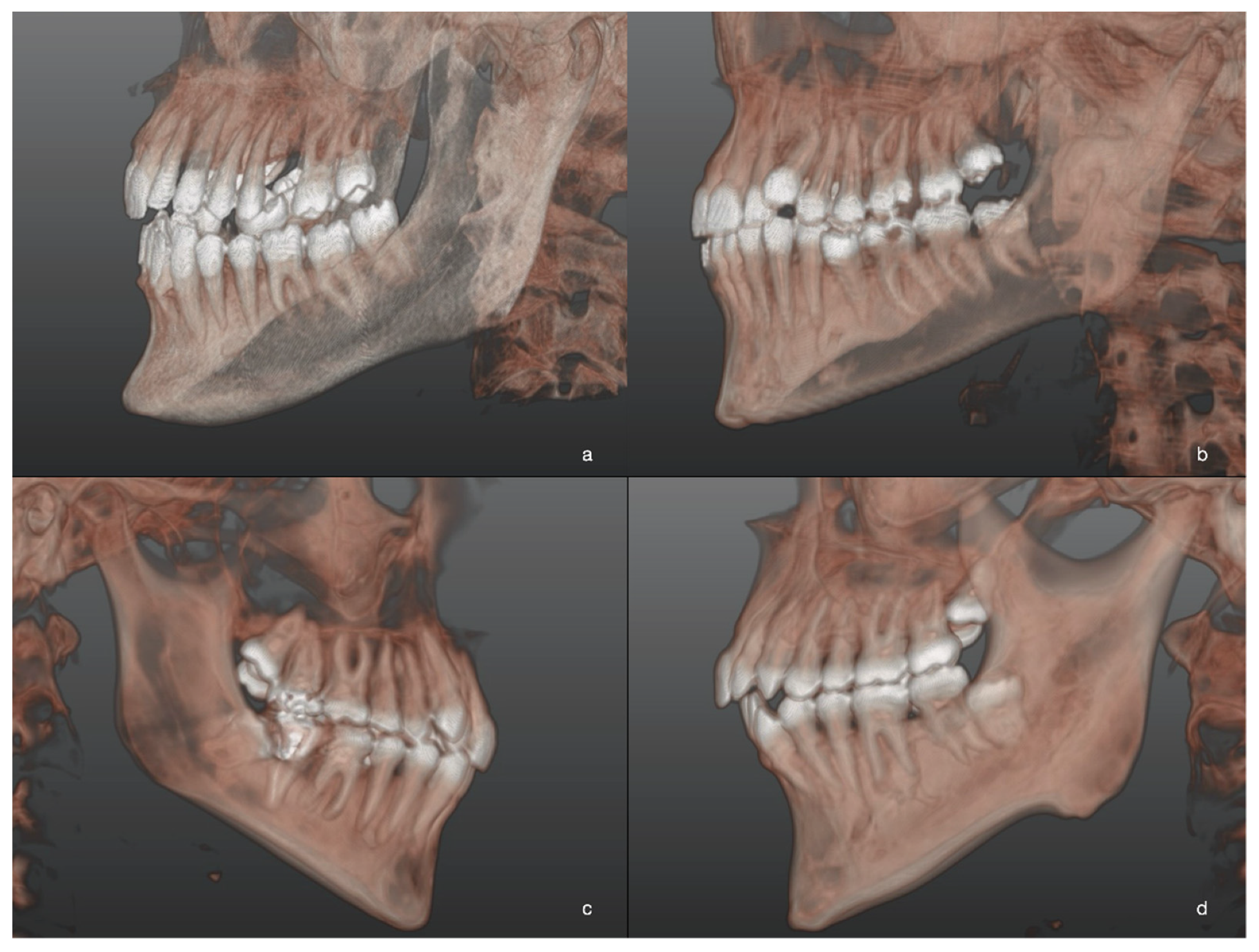
- Spatial position of M3M—S
- JD score—JD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- O’Hare, P.E.; Wilson, B.; Loga, M.G.; Ariyawardana, A. Effect of submucosal dexamethasone injections in the prevention of postoperative pain, trismus, and oedema associated with mandibular third molar surgery: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2019, 48, 1456–1469. [Google Scholar] [CrossRef]
- Gonca, M.; Gunacar, D.N.; Kose, T.E.; Karamehmetoglu, I. Evaluation of mandibular morphologic measurements and trabecular structure among subgroups of impacted mandibular third molars. Oral Radiol. 2021, 1–9. [Google Scholar] [CrossRef]
- Vaibhav, N.; Vivek, G.; Shetty, A.; Mohammad, I.; Ahmed, N.; Umeshappa, H. Efficacy of various routes of dexamethasone administration in reducing postoperative sequelae following impacted third molar surgery. Ann. Maxillofac. Surg. 2020, 10, 61–65. [Google Scholar] [CrossRef]
- Susarla, S.; Dodson, T.B. Estimating third molar extraction difficulty: A comparison of subjective and objective factors. J. Oral Maxillofac. Surg. 2005, 63, 427–434. [Google Scholar] [CrossRef]
- Sánchez-Torres, A.; Mota, I.; Clé-Ovejero, A.; Figueiredo, R.; Gay-Escoda, C.; Valmaseda-Castellón, E. Does Mandibular Gonial Angle Predict Difficulty of Mandibular Third Molar Removal? J. Oral Maxillofac. Surg. 2019, 77, 1745–1751. [Google Scholar] [CrossRef]
- Winter, G.B. Principles of Exodontia as Applied to the Impacted Third Molar: A Complete Treatise on the Operative Technic with Clinical Diagnoses and Radiographic Interpretations; American Medical Book: St. Louis, MO, USA, 1926. [Google Scholar]
- Pell, G.J.; Gregory, B.T. Impacted mandibular third molars: Classification and modified techniques for removal. Dent Dig. 1933, 39, 330–338. [Google Scholar]
- Liye, Q.; Zhongwei, Z.; Xiaojuan, S.; Min, W.; Pingping, L.; Kun, C. Can narrowing of the mandibular canal on pre-operative panoramic radiography predict close anatomical contact of the mandibular canal with the mandibular third molar? A meta-analysis. Oral Radiol. 2019, 36, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Baena, R.R.Y.; Beltrami, R.; Tagliabo, A.; Rizzo, S.; Lupi, S.-M. Differences between panoramic and Cone Beam-CT in the surgical evaluation of lower third molars. J. Clin. Exp. Dent. 2017, 9, e259–e265. [Google Scholar] [CrossRef] [PubMed]
- Stacchi, C.; Daugela, P.; Berton, F.; Lombardi, T.; Andriulionis, T.; Perinetti, G.; Di Lenarda, R.; Juodzbalys, G. A classification for assessing surgical difficulty in the extraction of mandibular impacted third molars: Description and clinical validation. Quintessence Int. 2018, 49, 745–753. [Google Scholar] [CrossRef]
- Ghaeminia, H.; Meijer, G.; Soehardi, A.; Borstlap, W.; Mulder, J.; Bergé, S. Position of the impacted third molar in relation to the mandibular canal. Diagnostic accuracy of cone beam computed tomography compared with panoramic radiography. Int. J. Oral Maxillofac. Surg. 2009, 38, 964–971. [Google Scholar] [CrossRef]
- Demirtas, O.; Harorli, A. Evaluation of the maxillary third molar position and its relationship with the maxillary sinus: A CBCT study. Oral Radiol. 2015, 32, 173–179. [Google Scholar] [CrossRef]
- Neves, F.S.; Souza, T.D.C.; De-Azevedo-Vaz, S.L.; Campos, P.S.F.; Boscolo, F.N. Influence of cone-beam computed tomography milliamperage settings on image quality of the mandibular third molar region. Oral Radiol. 2013, 30, 27–31. [Google Scholar] [CrossRef]
- Behbehani, F.; Årtun, J.; Thalib, L. Prediction of mandibular third-molar impaction in adolescent orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 47–55. [Google Scholar] [CrossRef]
- Khalil, H. Skeletal tracing of impacted and erupted mandibular third molar areas using panoramic radiographs. Biosci. Biotechnol. Res. Asia 2016, 7, 01–06. [Google Scholar]
- Björk, A.; Jensen, E.; Palling, M. Mandibular growth and third molar impaction. Acta Odontol. Scand. 1956, 14, 231–272. [Google Scholar] [CrossRef]
- Richardson, M.E. The etiology and prediction of mandibular third molar impaction. Angle Orthod. 1977, 47, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Demirel, O.; Akbulut, A. Evaluation of the relationship between gonial angle and impacted mandibular third molar teeth. Anat. Sci. Int. 2020, 95, 134–142. [Google Scholar] [CrossRef]
- Gümrükçü, Z.; Balaban, E.; Karabağ, M. Is there a relationship between third-molar impaction types and the dimensional/angular measurement values of posterior mandible according to Pell & Gregory/Winter Classification? Oral Radiol. 2021, 37, 29–35. [Google Scholar] [CrossRef]
- Breik, O.; Grubor, D. The incidence of mandibular third molar impactions in different skeletal face types. Aust. Dent. J. 2008, 53, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Valletta, R.; Rongo, R.; Madariaga, A.C.P.; Baiano, R.; Spagnuolo, G.; D’Antò, V. Relationship between the Condylion–Gonion–Menton Angle and Dentoalveolar Heights. Int. J. Environ. Res. Public Health 2020, 17, 3309. [Google Scholar] [CrossRef]
- Bhullar, M.; Chachra, S.; Kochhar, G.; Kochhar, A.; Uppal, A. Comparison of gonial angle determination from cephalograms and orthopantomogram. Indian J. Dent. 2014, 5, 123–126. [Google Scholar] [CrossRef] [Green Version]
- Schudy, F.F. The rotation of the mandible resulting from growth: Its implications in orthodontic treatment. Angle Orthod. 1965, 35, 36–50. [Google Scholar] [CrossRef]
- Riedel, R.A. Esthetics and its relation to orthodontic therapy. Angle Orthod. 1950, 20, 168–178. [Google Scholar] [CrossRef] [PubMed]
- Demirjian, A.; Goldstein, H.; Tanner, J.M. A new system of dental age assessment. Hum. Biol. 1973, 45, 211–227. [Google Scholar] [CrossRef]
- Juodzbalys, G.; Daugela, P. Mandibular Third Molar Impaction: Review of Literature and a Proposal of a Classification. J. Oral Maxillofac. Res. 2013, 4, e1. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Radhakrishnan, P.D.; Varma, N.K.S.; Ajith, V.V. Dilemma of gonial angle measurement: Panoramic radiograph or lateral cephalogram. Imaging Sci. Dent. 2017, 47, 93–97. [Google Scholar] [CrossRef] [Green Version]
- Gupta, R.; Sharma, M.; Singh, S. Mandibular third molar impactions in relation to different skeletal facial axis groups: A radiographic evaluation. J. Appl. Dent. Med. Sci. 2017, 3, 49–55. [Google Scholar]
- D’Antò, V.; Madariaga, A.C.P.; Rongo, R.; Bucci, R.; Simeon, V.; Franchi, L.; Valletta, R.; Antò, D.; Madariaga, P.; D’Antò, V. Distribution of the Condylion-Gonion-Menton (CoGoMe^) Angle in a Population of Patients from Southern Italy. Dent. J. 2019, 7, 104. [Google Scholar] [CrossRef] [Green Version]
- DeVincenzo, J.P. Changes in mandibular length before, during, and after successful orthopedic correction of Class II malocclusions, using a functional appliance. Am. J. Orthod. Dentofac. Orthop. 1991, 99, 241–257. [Google Scholar] [CrossRef]
- Pippi, R.; Santoro, M.; D’Ambrosio, F. Accuracy of cone-beam computed tomography in defining spatial relationships between third molar roots and inferior alveolar nerve. Eur. J. Dent. 2016, 10, 454–458. [Google Scholar] [CrossRef] [Green Version]
- Brancaccio, Y.; Antonelli, A.; Barone, S.; Bennardo, F.; Fortunato, L.; Giudice, A. Evaluation of local hemostatic efficacy after dental extractions in patients taking antiplatelet drugs: A randomized clinical trial. Clin. Oral Investig. 2021, 25, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Giudice, A.; Esposito, M.; Bennardo, F.; Brancaccio, Y.; Buti, J.; Fortunato, L. Dental extractions for patients on oral antiplatelet: A within-person randomised controlled trial comparing haemostatic plugs, advanced-platelet-rich fibrin (A-PRF+) plugs, leukocyte- and platelet-rich fibrin (L-PRF) plugs and suturing alone. Int. J. Oral Implant. 2019, 12, 77–87. [Google Scholar]
- Ling, X.; Heng, T.; Mohamad, A. Which procedure is better: Germectomy or surgical removal of mandibular third molar? Int. J. Oral Maxillofac. Surg. 2017, 46, 110–111. [Google Scholar] [CrossRef]
- Ahila, S.; Sasikala, C.; Kumar, B.; Tah, R.; Abinaya, K. Evaluation of the correlation of ramus height, gonial angle, and dental height with different facial forms in individuals with deep bite disorders. Ann. Med. Health Sci. Res. 2016, 6, 232–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giudice, A.; Barone, S.; Belhous, K.; Morice, A.; Soupre, V.; Bennardo, F.; Boddaert, N.; Vazquez, M.-P.; Abadie, V.; Picard, A. Pierre Robin sequence: A comprehensive narrative review of the literature over time. J. Stomatol. Oral Maxillofac. Surg. 2018, 119, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Soyoye, O.A.; Otuyemi, O.D.; Kolawole, K.A.; Ayoola, O.O. Relationship between masseter muscle thickness and maxillofacial morphology in pre-orthodontic treatment patients. Int. Orthod. 2018, 16, 698–711. [Google Scholar] [CrossRef]
- Hattab, F.N.; Abu Alhaija, E.S. Radiographic evaluation of mandibular third molar eruption space. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1999, 88, 285–291. [Google Scholar] [CrossRef]
- Al-Gunaid, T.H.; Bukhari, A.K.; El Khateeb, S.M.; Yamaki, M. Relationship of Mandibular Ramus Dimensions to Lower Third Molar Impaction. Eur. J. Dent. 2019, 13, 213–221. [Google Scholar] [CrossRef] [Green Version]
- Tsai, H.-H. Factors associated with mandibular third molar eruption and impaction. J. Clin. Pediatr. Dent. 2006, 30, 109–114. [Google Scholar] [CrossRef]
- Abu Alhaija, E.S.J.; AlBhairan, H.M.; Alkhateeb, S.N. Mandibular third molar space in different antero-posterior skeletal patterns. Eur. J. Orthod. 2010, 33, 570–576. [Google Scholar] [CrossRef]
- Begtrup, A.; Gronastoth, H.A.; Christensen, I.J.; Kjaer, I.; Grønastøð, H.Á.; Kjær, I. Predicting lower third molar eruption on panoramic radiographs after cephalometric comparison of profile and panoramic radiographs. Eur. J. Orthod. 2012, 35, 460–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanwal, S. Frequency of Mandibular Third Molar Impaction in Subjects with Different Facial Types in Southern Punjab. Pak. J. Med. Health Sci. 2013, 7, 655–657. [Google Scholar]
- Tassoker, M.; Kok, H.; Sener, S. Is There a Possible Association between Skeletal Face Types and Third Molar Impaction? A Retrospective Radiographic Study. Med. Princ. Pr. 2018, 28, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Legović, M.; Legović, I.; Brumini, G.; VanĎura, I.; Ćabov, T.; Ovesnik, M.; Meštrović, S.; Šlaj, M.; Škrinjarić, A. Correlation Between the Pattern of Facial Growth and the Position of the Mandibular Third Molar. J. Oral Maxillofac. Surg. 2008, 66, 1218–1224. [Google Scholar] [CrossRef] [PubMed]
- Mollaoglu, N.; Cetiner, S.; Güngör, K. Patterns of third molar impaction in a group of volunteers in Turkey. Clin. Oral Investig. 2002, 6, 109–113. [Google Scholar] [CrossRef]
- Ventä, I.; Turtola, L.; Ylipaavalniemi, P. Radiographic follow-up of impacted third molars from age 20 to 32 years. Int. J. Oral Maxillofac. Surg. 2001, 30, 54–57. [Google Scholar] [CrossRef]
- Uthman, A.T. Retromolar space analysis in relation to selected linear and angular measurements for an Iraqi sample. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 104, e76–e82. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Sample n (%) | |
|---|---|
| Patients | 172 (100) |
| M3M | 266 (100) |
| 3.8 | 128 (48.1) |
| 4.8 | 138 (51.9) |
| Gonial angle (°) | 122.6 ± 4.8 |
| H-GA | 126.8 ± 2.8 |
| L-GA | 118.8 ± 2.5 |
| Age (years) | 26.3 ± 4.6 |
| Sex | |
| Male | 169 (63.5) |
| Ramus length (mm) | 67.8 ± 6.2 |
| Ramus width (mm) | 31.2 ± 3.0 |
| Ramus divergency (°) | 65.5 ± 22.9 |
| Retromolar space (mm) | 11.5 ± 2.1 |
| JD classification | |
| M | |
| 0 | 148 (55.6) |
| 1 | 53 (20) |
| 2 | 50 (18.8) |
| 3 | 15 (5.6) |
| R | |
| 0 | 145 (54.5) |
| 1 | 59 (22.2) |
| 2 | 39 (14.7) |
| 3 | 23 (8.6) |
| A | |
| 0 | 132 (49.7) |
| 1 | 36 (13.5) |
| 2 | 54 (20.3) |
| 3 | 44 (16.5) |
| C | |
| 0 | 90 (33.8) |
| 1 | 108 (40.6) |
| 2 | 45 (16.9) |
| 3 | 23 (8.7) |
| B | |
| 0 | 4 (1.5) |
| 1 | 75 (28.2) |
| 2 | 105 (39.5) |
| 3 | 82 (30.8) |
| S | |
| 0 | 141 (53) |
| 1 | 86 (32.3) |
| 2 | 14 (5.3) |
| 3 | 25 (9.4) |
| JD score | |
| 0–6 | 154 (57.9) |
| 7–12 | 83 (31.2) |
| 13–18 | 29 (10.9) |
| High Gonial Angle | Low Gonial Angle | p-Value | |
|---|---|---|---|
| Study sample | |||
| Patients | 86 | 86 | Not applicable |
| Lower third molar | 127 (47.7%) | 139 (52.3%) | Not applicable |
| Age (years) | 26.1 ± 4.5 | 26.4 ± 4.7 | 0.2 |
| Sex | 0.03 * | ||
| Male | 72 (56.7%) | 97 (69.8%) | |
| Ramus length (mm) | 65.6 ± 6 | 69.8 ± 5.7 | <0.001 * |
| Ramus width (mm) | 30.1 ± 2.8 | 32.1 ± 3 | <0.001 * |
| Ramus divergency (°) | 63.7 ± 23.3 | 67 ± 22.5 | 0.06 |
| Retromolar space (mm) | 11.6 ± 2.1 | 11.4 ± 2.2 | 0.18 |
| High Gonial Angle n (%) | Low Gonial Angle n (%) | p-Value | |
|---|---|---|---|
| Juodzbalys and Daugela classification | |||
| Relation to the second molar (M) | 0.009 * | ||
| 0 | 80 (62.9) | 68 (48.9) | |
| 1 | 26 (20.5) | 27 (19.4) | |
| 2 | 19 (15) | 31 (22.3) | |
| 3 | 2 (1.6) | 13 (9.4) | |
| Relation to the mandibular ramus (R) | 0.0003 * | ||
| 0 | 81 (63.8) | 64 (46.1) | |
| 1 | 31 (24.4) | 28 (20.1) | |
| 2 | 11 (8.7) | 28 (20.1) | |
| 3 | 4 (3.1) | 19 (13.7) | |
| Relation to the adjacent alveolar crest (A) | 0.01 * | ||
| 0 | 72 (56.7) | 60 (43.2) | |
| 1 | 20 (15.8) | 16 (11.5) | |
| 2 | 23 (18.1) | 31 (22.3) | |
| 3 | 12 (9.4) | 32 (23) | |
| Relation to the mandibular canal (C) | 0.2 | ||
| 0 | 45 (35.4) | 45 (32.4) | |
| 1 | 56 (44.1) | 52 (37.4) | |
| 2 | 15 (11.8) | 30 (21.6) | |
| 3 | 11 (8.7) | 12 (8.6) | |
| Relation to mandibular lingual and buccal walls (B) | 0.001 * | ||
| 0 | 3 (2.4) | 1 (0.7) | |
| 1 | 48 (37.8) | 27 (19.4) | |
| 2 | 49 (38.6) | 56 (40.3) | |
| 3 | 27 (21.3) | 55 (39.6) | |
| Spatial position (S) | 0.04 * | ||
| 0 | 72 (56.7) | 69 (49.6) | |
| 1 | 43 (33.9) | 43 (31) | |
| 2 | 7 (5.5) | 7 (5) | |
| 3 | 5 (3.9) | 20 (14.4) | |
| Juodzbalys and Daugela score (JD) | 0.001 * | ||
| 0–6 | 86 (67.7) | 68 (49) | |
| 7–12 | 35 (27.6) | 48 (34.5) | |
| 13–18 | 6 (4.7) | 23 (16.5) |
| Coefficient β | p-Value | |
|---|---|---|
| (Constant) | M: 5.3 | M: 0.02 * |
| R: 8.4 | R: 0.0002 * | |
| A: <0.001 | A: 0.001 * | |
| C: 4.7 | C: 0.04 * | |
| B: 4.9 | B: 0.01 * | |
| S: 3.8 | S: 0.08 | |
| JD: 36.7 | JD: 0.0005 * | |
| Sex | M: −0.14 | M: 0.3 |
| R: −0.3 | R: 0.09 | |
| A: <0.0001 | A: 0.2 | |
| C: 0.05 | C: 0.8 | |
| B: −0.3 | B: 0.01 * | |
| S: −0.4 | S: 0.008 * | |
| JD: −1.3 | JD: 0.07 | |
| Age | M: −0.03 | M: 0.04 * |
| R: −0.02 | R: 0.2 | |
| A: <0.0001 | A: 0.055 | |
| C: −0.01 | C: 0.4 | |
| B: −0.01 | B: 0.3 | |
| S: −0.01 | S: 0.7 | |
| JD: −0.1 | JD: 0.09 | |
| Lower third molar (3.8 or 4.8) | M: −0.1 | M: 0.3 |
| R: −0.04 | R: 0.7 | |
| A: <0.0001 | A: 0.5 | |
| C: −0.1 | C: 0.4 | |
| B: −0.06 | B: 0.5 | |
| S: −0.03 | S: 0.8 | |
| JD: −0.5 | JD: 0.4 | |
| Gonial angle | M: −0.02 | M: 0.05 * |
| R: −0.04 | R: 0.001 * | |
| A: <0.0001 | A: 0.004 * | |
| C: −0.01 | C: 0.5 | |
| B: −0.03 | B: 0.007* | |
| S: −0.02 | S: 0.1 | |
| JD: −0.2 | JD: 0.004 * | |
| Ramus high | M: 0.01 | M: 0.4 |
| R: 0.0005 | R: 0.9 | |
| A: <0.0001 | A: 0.9 | |
| C: −0.01 | C: 0.5 | |
| B: 0.004 | B: 0.7 | |
| S: 0.03 | S: 0.04 * | |
| JD: 0.03 | JD: 0.6 | |
| Ramus width | M: 0.006 | M: 0.8 |
| R: 0.005 | R: 0.8 | |
| A: <0.0001 | A: 0.9 | |
| C: −0.04 | C: 0.1 | |
| B: 0.04 | B: 0.04 * | |
| S: −0.03 | S: 0.3 | |
| JD: −0.01 | JD: 0.9 | |
| Retromolar space | M: −0.2 | M: <0.0001 * |
| R: −0.2 | R: <0.0001 * | |
| A: <0.0001 | A: <0.0001 * | |
| C: −0.07 | C: 0.02 * | |
| B: 0.0002 | B: 0.9 | |
| S: −0.1 | S: <0.0001 * | |
| JD: −0.7 | JD: <0.0001 * | |
| Ramus divergency | M: 0.003 | M: 0.3 |
| R: 0.001 | R: 0.6 | |
| A: <0.0001 | A: 0.2 | |
| C: 0.004 | C: 0.1 | |
| B: −0.002 | B: 0.4 | |
| S: −0.01 | S: 0.8 | |
| JD: 0.01 | JD: 0.4 | |
| R-squared | M: 0.15 | M: <0.0001 * |
| R: 0.17 | R: <0.0001 * | |
| A: 0.14 | A: <0.0001 * | |
| C: 0.03 | C: 0.05 * | |
| B: 0.07 | B: 0.001 * | |
| S: 0.1 | S: <0.0001 * | |
| JD: 0.15 | JD: <0.0001 * |
| Author, Year | Study Design; Sample (Number of Patients) Radiologic Assessment | Study Outcomes and Conclusions |
|---|---|---|
| Hattab et al. 1999 [39] | Retrospective study; 134; orthopantomography | The mean GA was 122.14° in the impacted group and 120.08° in the erupted group. The retromolar space was significantly smaller in the group with impacted M3M and it was also associated with lateral asymmetry of M3M in both groups. The third molar space/crown width ratio was <1 in the impacted group and >1 in the erupted group (p < 0.001). The mesiodistal crown width was not significantly different between impacted or erupted group. |
| Mollaoglu et al., 2002 [47] | Retrospective study; 213; orthopantomography | GA did not differ significantly between the erupted and the impacted groups. It was observed that the M3M mesiodistal angulation was significantly higher in impacted group in which there was a significantly lower retromolar space (p < 0.05). The retromolar space/third molar crown width ratio differed significantly between impacted and erupted groups. |
| Tsai et al., 2005 [41] | Retrospective study; 152; orthopantomography | In male patients, mandibular body length, mandibular ramus width, and first molar width were significantly greater in the impacted group. The retromolar space was significantly lower in the impacted group (p < 0.05). In female patients, mandibular ramus high and first molar width were significantly greater in the impacted group. The retromolar space was significantly lower in the impacted group (p < 0.05). GA did not show any difference between the groups. |
| Uthman et al., 2007 [49] | Cohort study; 50; orthopantomography | The retromolar space was significantly lower in marginal-eruption group than in full-eruption group (p < 0.01). The retromolar space/M3M width ratio was significantly greater in the full-eruption group (mean ratio >1) than in the marginal-eruption group (mean ratio <1) (p < 0.01). GA was not significantly different between the two groups. |
| Legovic et al., 2008 [46] | Retrospective study; 130; Orthopantomography and lateral radiograph | In male patients, a significant correlation was found between the retromolar space and the vertical position of lower right M3M (p < 0.05). In female patients significant correlations were determined: (1) between the retromolar space and the vertical position of M3M (p < 0.05); (2) between the retromolar area and M3M inclination (p < 0.05); (3) between the retromolar space and spatial relation of M3M (p < 0.05). A significant correlation between lower right M3M inclination and anterior facial rotation was observed (p < 0.05). |
| Breik et al., 2008 [20] | Retrospective study; 98; Orthopantomography and lateral radiograph | The mandibular third molar impaction was 58.76%. Brachyfacial patients showed lower incidence of mandibular third molar impaction than dolichofacial patients (p < 0.01). No difference was found between mesofacial and dolichofacial patients. Most of the impacted M3Ms were in a horizontal position. |
| Abu Alhaija et al., 2011 [42] | Retrospective study; 270; Orthopantomography and lateral radiograph | M3M impaction was recorded in 26% of Skeletal Class I, 32% of Skeletal Class II, and 42% of Skeletal Class III. Impacted M3M was significantly associated with reduced retromolar space width, increased angle between M2M and M3M, and decreased M3M angulation in all skeletal patterns (p < 0.05). Only in skeletal Class I GA was significantly greater in the impacted group than in the erupted group (p < 0.01). |
| Begtrup et al., 2013 [43] | Retrospective study; 53; Orthopantomography and lateral radiograph | No correlation between jaw angles and M3M eruption was found. A larger distance from the articulare point to the interdentale point is correlated with M3M eruption. |
| Kanwal et al., 2013 [44] | Descriptive cross-sectional study; 60; Orthopantomography | Frequency of M3M impaction was significantly higher in dolichofacial type (46.67%) than in brachyfacial type (16.67%) (p < 0.05). Most female patients showed impacted M3M. |
| Gupta et al., 2017 [29] | Retrospective study; 150; Orthopantomography and lateral radiograph | Impacted M3Ms were mostly in mesioangular position, (49.3%) followed by distoangular (22.7%) and vertical position (20.2%). M3M impaction occurred in brachyfacial patients (44%), in dolichofacial (49%), and in mesofacial subjects (77%), with a significant difference among the groups (p < 0.05). |
| Tassoker et al., 2019 [45] | Retrospective study; 158; Orthopantomography and lateral radiograph | Brachyfacial patients showed a lower prevalence of third molar impaction, with respect to dolichofacial and mesofacial patients (p < 0.05). No correlations were found between skeletal facial type and the angular position of M3M (p > 0.05). |
| Demirel et al., 2019 [18] | Retrospective study; 90; Orthopantomography to evaluate mandibular morphology and CBCT to evaluate M3M | Mean gonial angle value was 121.38° ± 7.64°. The most common position was mesioangular M3M. No significant correlation was found between gonial angle and other variables (age, gender, third molar angulation) (p > 0.05). Despite no significant relationship being observed between Pell–Gregory groups and gonial angle values (p > 0.05), a significantly higher gonial angle (p < 0.05) was found only in the sub-group in which M3M was partially inside the ramus and its occlusal level was below than cervical level of M2M. |
| Al-Gunaid et al., 2019 [40] | Retrospective study; 240; Orthopantomography | The erupted group showed longer condylar and coronoid length, longer ramus height, wider ramal width, larger retro¬molar space, higher retromolar area to M3M ratio, and larger angle of impaction than impacted group (p < 0.05). The impacted group showed significantly larger GA, and larger inclination of lower posterior teeth than the erupted group (p < 0.05). |
| Gümrükçü et al., 2020 [19] | Retrospective study; 601; Orthopantomography and lateral radiograph | The mean value of GA is 123.8 ± 6.9°. According to Pell-Gregory classification, a statistically significant difference was observed in terms of ramus height–gonial angle between Class A and B, between Class B and C (p < 0.05). Ramus high was significantly different between Class A and C (p < 0.05). According to Winter Classification, gonial angle was significantly higher in class Vertical and significantly lower in class Horizontal (p < 0.05). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barone, S.; Antonelli, A.; Averta, F.; Diodati, F.; Muraca, D.; Bennardo, F.; Giudice, A. Does Mandibular Gonial Angle Influence the Eruption Pattern of the Lower Third Molar? A Three-Dimensional Study. J. Clin. Med. 2021, 10, 4057. https://doi.org/10.3390/jcm10184057
Barone S, Antonelli A, Averta F, Diodati F, Muraca D, Bennardo F, Giudice A. Does Mandibular Gonial Angle Influence the Eruption Pattern of the Lower Third Molar? A Three-Dimensional Study. Journal of Clinical Medicine. 2021; 10(18):4057. https://doi.org/10.3390/jcm10184057
Chicago/Turabian StyleBarone, Selene, Alessandro Antonelli, Fiorella Averta, Federica Diodati, Danila Muraca, Francesco Bennardo, and Amerigo Giudice. 2021. "Does Mandibular Gonial Angle Influence the Eruption Pattern of the Lower Third Molar? A Three-Dimensional Study" Journal of Clinical Medicine 10, no. 18: 4057. https://doi.org/10.3390/jcm10184057
APA StyleBarone, S., Antonelli, A., Averta, F., Diodati, F., Muraca, D., Bennardo, F., & Giudice, A. (2021). Does Mandibular Gonial Angle Influence the Eruption Pattern of the Lower Third Molar? A Three-Dimensional Study. Journal of Clinical Medicine, 10(18), 4057. https://doi.org/10.3390/jcm10184057