
Medication-Related Osteonecrosis of the Jaw: A Critical Narrative Review

 ,
,  , , , ,
, , , ,  and
and 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
3. Definition
4. Pathogenesis
4.1. Infection, Inflammation, and Trauma
4.2. Altered Bone Remodelling or Oversuppression of Bone Resorption
4.3. Altered Angiogenesis
5. Incidence
6. Risk Factors
7. Prevention
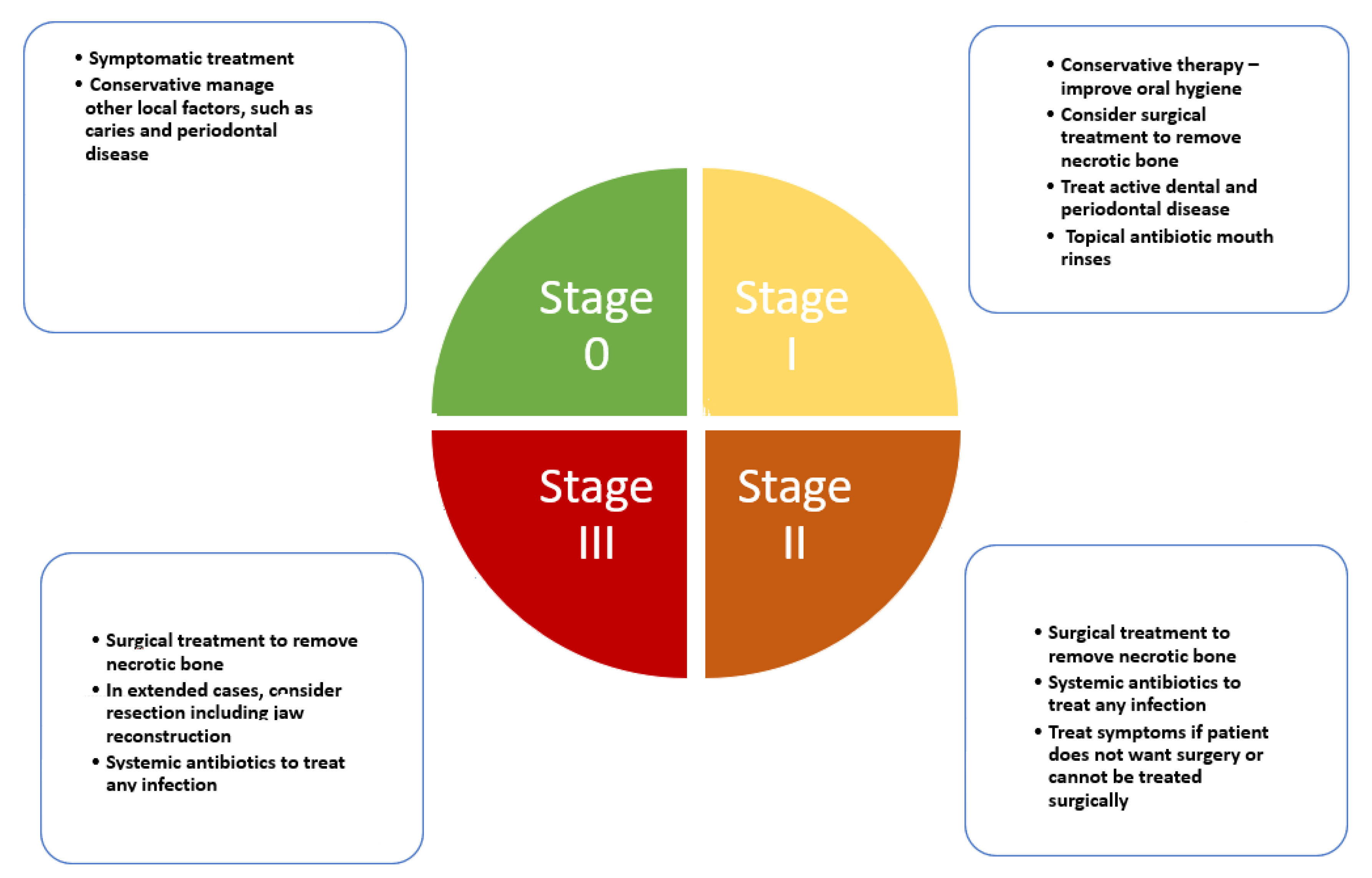
8. Staging and Prognostication
8.1. Stage 0
8.2. Stage 1
8.3. Stage 2
8.4. Stage 3
9. Management
10. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AAOMS | American association of oral and maxillofacial surgeons; |
| APC | Autologous platelet concentrate; |
| ASBMR | American society for bone and mineral research; |
| BP | Bisphosphonate; |
| BRONJ | Biphosphonate-related osteonecrosis of the jaw; |
| CI | Confidential interval; |
| CT | Computed tomography; |
| CTX | Collagen type I c-telopeptide; |
| Er:YAG | Erbium YAG; |
| IDT | Invasive dental treatment; |
| MMP9 | Matrix metallopeptidase 9; |
| MRI | Magnetic resonance imaging; |
| MRONJ | Medication-related osteonecrosis of the jaw; |
| mTOR | Mammalian Target of Rapamycin; |
| PD | Periodontal disease; |
| RANKL | Receptor activator for nuclear factor κB ligand; |
| VEGF | Vascular endothelial growth factor. |
References
- Lafforgue, P. Pathophysiology and natural history of avascular necrosis of bone. Jt. Bone Spine 2006, 73, 500–507. [Google Scholar] [CrossRef]
- Goodman, S.B.; Maruyama, M. Inflammation, bone healing and osteonecrosis: From bedside to bench. J. Inflamm. Res. 2020, 13, 913–923. [Google Scholar] [CrossRef]
- Hayashida, S.; Soutome, S.; Yanamoto, S.; Fujita, S.; Hasegawa, T.; Komori, T.; Kojima, Y.; Miyamoto, H.; Shibuya, Y.; Ueda, N.; et al. Evaluation of the treatment strategies for medication-related osteonecrosis of the jaws (MRONJ) and the factors affecting treatment outcome: A multicenter retrospective study with propensity score matching analysis. J. Bone Miner. Res. 2017, 32, 2022–2029. [Google Scholar] [CrossRef] [Green Version]
- James, J.; Steijn-Myagkaya, G.L. Death of osteocytes. Electron microscopy after in vitro ischaemia. J. Bone Jt. Surg. Br. 1986, 68, 620–624. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Mehrotra, B.; Rosenberg, T.J.; Engroff, S.L. Osteonecrosis of the jaws associated with the use of bisphosphonates: A review of 63 cases. J. Oral Maxillofac. Surg. 2004, 62, 527–534. [Google Scholar] [CrossRef]
- Marx, R.E. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: A growing epidemic. J. Oral Maxillofac. Surg. 2003, 61, 1115–1117. [Google Scholar] [CrossRef]
- Vance, M.A. Osteonecrosis of the jaw and bisphosphonates: A comparison with white phosphorus, radium, and osteopetrosis. Clin. Toxicol. 2007, 45, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Ashcroft, J. Bisphosphonates and phossy-jaw: Breathing new life into an old problem. Lancet Oncol. 2006, 7, 447–449. [Google Scholar] [CrossRef]
- Russell, R.G. Bisphosphonates: The first 40 years. Bone 2011, 49, 2–19. [Google Scholar] [CrossRef]
- Gaudin, E.; Seidel, L.; Bacevic, M.; Rompen, E.; Lambert, F. Occurrence and risk indicators of medication-related osteonecrosis of the jaw after dental extraction: A systematic review and meta-analysis. J. Clin. Periodontol. 2015, 42, 922–932. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, A.; Nogueras Gonzalez, G.M.; Geng, Y.; Won, A.M.; Cabanillas, M.E.; Naing, A.; Myers, J.N.; Li, Y.; Chambers, M.S. Prevalence of medication related osteonecrosis of the jaw in patients treated with sequential antiresorptive drugs: Systematic review and meta-analysis. Support. Care Cancer 2021, 29, 2305–2317. [Google Scholar] [CrossRef]
- Migliorati, C.A.; Brennan, M.T.; Peterson, D.E. Medication-related osteonecrosis of the jaws. J. Natl. Cancer. Inst. Monogr. 2019, 2019, lgz009. [Google Scholar] [CrossRef] [PubMed]
- Kanwar, N.; Bakr, M.M.; Meer, M.; Siddiqi, A. Emerging therapies with potential risks of medicine-related osteonecrosis of the jaw: A review of the literature. Br. Dent. J. 2020, 228, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Aghaloo, T.L.; Tetradis, S. Osteonecrosis of the jaw in the absence of antiresorptive or antiangiogenic exposure: A series of 6 cases. J. Oral Maxillofac. Surg. 2017, 75, 129–142. [Google Scholar] [CrossRef] [Green Version]
- Fantasia, J.E. The role of antiangiogenic therapy in the development of osteonecrosis of the jaw. Oral Maxillofac. Surg. Clin. North. Am. 2015, 27, 547–553. [Google Scholar] [CrossRef]
- Bennardo, F.; Buffone, C.; Giudice, A. New therapeutic opportunities for COVID-19 patients with Tocilizumab: Possible correlation of interleukin-6 receptor inhibitors with osteonecrosis of the jaws. Oral Oncol. 2020, 106, 104659. [Google Scholar] [CrossRef] [PubMed]
- Eguia, A.; Bagan-Debon, L.; Cardona, F. Review and update on drugs related to the development of osteonecrosis of the jaw. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e71–e83. [Google Scholar] [CrossRef]
- Koorbusch, G.F.; Deatherage, J.R.; Cure, J.K. How can we diagnose and treat osteomyelitis of the jaws as early as possible? Oral Maxillofac. Surg. Clin. N. Am. 2011, 23, 557–567. [Google Scholar] [CrossRef]
- Farah, C.S.; Savage, N.W. Oral ulceration with bone sequestration. Aust. Dent. J. 2003, 48, 61–64. [Google Scholar] [CrossRef] [Green Version]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F.; American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw—2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Morrison, A.; Hanley, D.A.; Felsenberg, D.; McCauley, L.K.; O’Ryan, F.; Reid, I.R.; Ruggiero, S.L.; Taguchi, A.; Tetradis, S.; et al. Diagnosis and management of osteonecrosis of the jaw: A systematic review and international consensus. J. Bone Miner. Res. 2015, 30, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Khosla, S.; Burr, D.; Cauley, J.; Dempster, D.W.; Ebeling, P.R.; Felsenberg, D.; Gagel, R.F.; Gilsanz, V.; Guise, T.; Koka, S.; et al. Bisphosphonate-associated osteonecrosis of the jaw: Report of a task force of the American Society for Bone and Mineral Research. J. Bone Miner. Res. 2007, 22, 1479–1491. [Google Scholar] [CrossRef] [Green Version]
- Yarom, N.; Shapiro, C.L.; Peterson, D.E.; Van Poznak, C.H.; Bohlke, K.; Ruggiero, S.L.; Migliorati, C.A.; Khan, A.; Morrison, A.; Anderson, H.; et al. Medication-related osteonecrosis of the jaw: MASCC/ISOO/ASCO Clinical Practice Guideline. J. Clin. Oncol. 2019, 37, 2270–2290. [Google Scholar] [CrossRef]
- Campisi, G.; Mauceri, R.; Bertoldo, F.; Bettini, G.; Biasotto, M.; Colella, G.; Consolo, U.; Di Fede, O.; Favia, G.; Fusco, V.; et al. Medication-related osteonecrosis of jaws (MRONJ) prevention and diagnosis: Italian consensus update 2020. Int. J. Environ. Res. Public. Health. 2020, 17, 5998. [Google Scholar] [CrossRef]
- Fedele, S.; Porter, S.R.; D’Aiuto, F.; Aljohani, S.; Vescovi, P.; Manfredi, M.; Arduino, P.G.; Broccoletti, R.; Musciotto, A.; Di Fede, O.; et al. Nonexposed variant of bisphosphonate-associated osteonecrosis of the jaw: A case series. Am. J. Med. 2010, 123, 1060–1064. [Google Scholar] [CrossRef] [Green Version]
- Bagan, J.V.; Hens-Aumente, E.; Leopoldo-Rodado, M.; Poveda-Roda, R.; Bagan, L. Bisphosphonate-related osteonecrosis of the jaws: Study of the staging system in a series of clinical cases. Oral Oncol. 2012, 48, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Yarom, N.; Fedele, S.; Lazarovici, T.S.; Elad, S. Is exposure of the jawbone mandatory for establishing the diagnosis of bisphosphonate-related osteonecrosis of the jaw? J. Oral Maxillofac. Surg. 2010, 68, 705. [Google Scholar] [CrossRef] [PubMed]
- Fedele, S.; Bedogni, G.; Scoletta, M.; Favia, G.; Colella, G.; Agrillo, A.; Bettini, G.; Di Fede, O.; Oteri, G.; Fusco, V.; et al. Up to a quarter of patients with osteonecrosis of the jaw associated with antiresorptive agents remain undiagnosed. Br. J. Oral Maxillofac. Surg. 2015, 53, 13–17. [Google Scholar] [CrossRef]
- Bedogni, A.; Fedele, S.; Bedogni, G.; Scoletta, M.; Favia, G.; Colella, G.; Agrillo, A.; Bettini, G.; Di Fede, O.; Oteri, G.; et al. Staging of osteonecrosis of the jaw requires computed tomography for accurate definition of the extent of bony disease. Br. J. Oral Maxillofac. Surg. 2014, 52, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Schiodt, M.; Otto, S.; Fedele, S.; Bedogni, A.; Nicolatou-Galitis, O.; Guggenberger, R.; Herlofson, B.B.; Ristow, O.; Kofod, T. Workshop of European task force on medication-related osteonecrosis of the jaw-Current challenges. Oral Dis. 2019, 25, 1815–1821. [Google Scholar] [CrossRef] [Green Version]
- Pazianas, M. Osteonecrosis of the jaw and the role of macrophages. J. Natl. Cancer Inst. 2011, 103, 232–240. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.; Hakam, A.E.; McCauley, L.K. Current understanding of the pathophysiology of osteonecrosis of the jaw. Curr. Osteoporos. Rep. 2018, 16, 584–595. [Google Scholar] [CrossRef]
- Otto, S.; Pautke, C.; Van den Wyngaert, T.; Niepel, D.; Schiodt, M. Medication-related osteonecrosis of the jaw: Prevention, diagnosis and management in patients with cancer and bone metastases. Cancer Treat. Rev. 2018, 69, 177–187. [Google Scholar] [CrossRef]
- Otto, S.; Aljohani, S.; Fliefel, R.; Ecke, S.; Ristow, O.; Burian, E.; Troeltzsch, M.; Pautke, C.; Ehrenfeld, M. Infection as an important factor in medication-related osteonecrosis of the jaw (MRONJ). Medicina 2021, 57, 463. [Google Scholar] [CrossRef]
- McGowan, K.; McGowan, T.; Ivanovski, S. Risk factors for medication-related osteonecrosis of the jaws: A systematic review. Oral Dis. 2018, 24, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Zirk, M.; Wenzel, C.; Buller, J.; Zoller, J.E.; Zinser, M.; Peters, F. Microbial diversity in infections of patients with medication-related osteonecrosis of the jaw. Clin. Oral Investig. 2019, 23, 2143–2151. [Google Scholar] [CrossRef]
- De Bruyn, L.; Coropciuc, R.; Coucke, W.; Politis, C. Microbial population changes in patients with medication-related osteonecrosis of the jaw treated with systemic antibiotics. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 268–275. [Google Scholar] [CrossRef] [Green Version]
- Mawardi, H.; Giro, G.; Kajiya, M.; Ohta, K.; Almazrooa, S.; Alshwaimi, E.; Woo, S.B.; Nishimura, I.; Kawai, T. A role of oral bacteria in bisphosphonate-induced osteonecrosis of the jaw. J. Dent. Res. 2011, 90, 1339–1345. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Ma, X.L.; Ma, J.X.; Sun, L.; Lu, B.; Wang, Y.; Xing, G.S.; Wang, Y.; Dong, B.C.; Xu, L.Y.; et al. TET3 mediates alterations in the epigenetic marker 5hmC and Akt pathway in steroid-associated osteonecrosis. J. Bone Miner. Res. 2017, 32, 319–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Q.; Yu, W.; Lee, S.; Xu, Q.; Naji, A.; Le, A.D. Bisphosphonate induces osteonecrosis of the jaw in diabetic mice via NLRP3/Caspase-1-dependent IL-1beta mechanism. J. Bone Miner. Res. 2015, 30, 2300–2312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aghaloo, T.L.; Cheong, S.; Bezouglaia, O.; Kostenuik, P.; Atti, E.; Dry, S.M.; Pirih, F.Q.; Tetradis, S. RANKL inhibitors induce osteonecrosis of the jaw in mice with periapical disease. J. Bone Miner. Res. 2014, 29, 843–854. [Google Scholar] [CrossRef]
- Ribet, A.B.P.; Ng, P.Y.; Pavlos, N.J. Membrane transport proteins in osteoclasts: The ins and outs. Front. Cell. Dev. Biol. 2021, 9, 644986. [Google Scholar] [CrossRef] [PubMed]
- Otto, S.; Hafner, S.; Mast, G.; Tischer, T.; Volkmer, E.; Schieker, M.; Sturzenbaum, S.R.; von Tresckow, E.; Kolk, A.; Ehrenfeld, M.; et al. Bisphosphonate-related osteonecrosis of the jaw: Is pH the missing part in the pathogenesis puzzle? J. Oral Maxillofac. Surg. 2010, 68, 1158–1161. [Google Scholar] [CrossRef] [PubMed]
- Otto, S.; Pautke, C.; Opelz, C.; Westphal, I.; Drosse, I.; Schwager, J.; Bauss, F.; Ehrenfeld, M.; Schieker, M. Osteonecrosis of the jaw: Effect of bisphosphonate type, local concentration, and acidic milieu on the pathomechanism. J. Oral Maxillofac. Surg. 2010, 68, 2837–2845. [Google Scholar] [CrossRef] [PubMed]
- Dayisoylu, E.H.; Ungor, C.; Tosun, E.; Ersoz, S.; Kadioglu Duman, M.; Taskesen, F.; Senel, F.C. Does an alkaline environment prevent the development of bisphosphonate-related osteonecrosis of the jaw? An experimental study in rats. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.W.; Vuong, H.E.; Kim, S.; Lenon, A.; Ho, K.; Hsiao, E.Y.; Sung, E.C.; Kim, R.H. Indigenous microbiota protects against inflammation-induced osteonecrosis. J. Dent. Res. 2020, 99, 676–684. [Google Scholar] [CrossRef]
- Kalyan, S.; Wang, J.; Quabius, E.S.; Huck, J.; Wiltfang, J.; Baines, J.F.; Kabelitz, D. Systemic immunity shapes the oral microbiome and susceptibility to bisphosphonate-associated osteonecrosis of the jaw. J. Transl. Med. 2015, 13, 212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Q.; Atsuta, I.; Liu, S.; Chen, C.; Shi, S.; Shi, S.; Le, A.D. IL-17-mediated M1/M2 macrophage alteration contributes to pathogenesis of bisphosphonate-related osteonecrosis of the jaws. Clin. Cancer Res. 2013, 19, 3176–3188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.W.; Landayan, M.E.; Lee, J.Y.; Tatad, J.C.; Kim, S.J.; Kim, M.R.; Cha, I.H. Role of microcracks in the pathogenesis of bisphosphonate-related osteonecrosis of the jaw. Clin. Oral Investig. 2016, 20, 2251–2258. [Google Scholar] [CrossRef]
- Schoenhof, R.; Munz, A.; Yuan, A.; ElAyouti, A.; Boesmueller, H.; Blumenstock, G.; Reinert, S.; Hoefert, S. Microarchitecture of medication-related osteonecrosis of the jaw (MRONJ); a retrospective micro-CT and morphometric analysis. J. Cranio-Maxillofac. Surg. 2021, 49, 508–517. [Google Scholar] [CrossRef]
- Aghaloo, T.; Hazboun, R.; Tetradis, S. Pathophysiology of osteonecrosis of the jaws. Oral Maxillofac. Surg. Clin. North. Am. 2015, 27, 489–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giudice, A.; Antonelli, A.; Chiarella, E.; Baudi, F.; Barni, T.; Di Vito, A. The case of medication-related osteonecrosis of the jaw addressed from a pathogenic point of view: Innovative therapeutic strategies: Focus on the most recent discoveries on oral mesenchymal stem cell-derived exosomes. Pharmaceuticals 2020, 13, 423. [Google Scholar] [CrossRef]
- Di Vito, A.; Chiarella, E.; Baudi, F.; Scardamaglia, P.; Antonelli, A.; Giudice, D.; Barni, T.; Fortunato, L.; Giudice, A. Dose-dependent effects of zoledronic acid on human periodontal ligament stem cells: An In Vitro pilot study. Cell Transplant. 2020, 29. [Google Scholar] [CrossRef] [PubMed]
- Otto, S.; Pautke, C.; Arens, D.; Poxleitner, P.; Eberli, U.; Nehrbass, D.; Zeiter, S.; Stoddart, M.J. A drug holiday reduces the frequency and severity of medication-related osteonecrosis of the jaw in a minipig model. J. Bone Miner. Res. 2020, 35, 2179–2192. [Google Scholar] [CrossRef]
- Ottesen, C.; Schiodt, M.; Gotfredsen, K. Efficacy of a high-dose antiresorptive drug holiday to reduce the risk of medication-related osteonecrosis of the jaw (MRONJ): A systematic review. Heliyon 2020, 6, e03795. [Google Scholar] [CrossRef] [PubMed]
- Gkouveris, I.; Hadaya, D.; Soundia, A.; Bezouglaia, O.; Chau, Y.; Dry, S.M.; Pirih, F.Q.; Aghaloo, T.L.; Tetradis, S. Vasculature submucosal changes at early stages of osteonecrosis of the jaw (ONJ). Bone 2019, 123, 234–245. [Google Scholar] [CrossRef]
- Papadopoulou, E.; Nicolatou-Galitis, O.; Papassotiriou, I.; Linardou, H.; Karagianni, A.; Tsixlakis, K.; Tarampikou, A.; Michalakakou, K.; Vardas, E.; Bafaloukos, D. The use of crevicular fluid to assess markers of inflammation and angiogenesis, IL-17 and VEGF, in patients with solid tumors receiving zoledronic acid and/or bevacizumab. Support. Care Cancer 2020, 28, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Basi, D.L.; Hughes, P.J.; Thumbigere-Math, V.; Sabino, M.; Mariash, A.; Lunos, S.A.; Jensen, E.; Gopalakrishnan, R. Matrix metalloproteinase-9 expression in alveolar extraction sockets of Zoledronic acid-treated rats. J. Oral Maxillofac. Surg. 2011, 69, 2698–2707. [Google Scholar] [CrossRef]
- Fliefel, R.M.; Entekhabi, S.A.; Ehrenfeld, M.; Otto, S. Geranylgeraniol (GGOH) as a mevalonate pathway activator in the rescue of bone cells treated with zoledronic acid: An in Vitro study. Stem Cells Int. 2019, 2019, 4351327. [Google Scholar] [CrossRef]
- de Molon, R.S.; Shimamoto, H.; Bezouglaia, O.; Pirih, F.Q.; Dry, S.M.; Kostenuik, P.; Boyce, R.W.; Dwyer, D.; Aghaloo, T.L.; Tetradis, S. OPG-Fc but not zoledronic acid discontinuation reverses osteonecrosis of the jaws (ONJ) in mice. J. Bone Miner. Res. 2015, 30, 1627–1640. [Google Scholar] [CrossRef] [Green Version]
- Rosella, D.; Papi, P.; Giardino, R.; Cicalini, E.; Piccoli, L.; Pompa, G. Medication-related osteonecrosis of the jaw: Clinical and practical guidelines. J. Int. Soc. Prev. Community Dent. 2016, 6, 97–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodwell, C.; Ayme, S. Rare disease policies to improve care for patients in Europe. Biochim. Biophys. Acta 2015, 1852, 2329–2335. [Google Scholar] [CrossRef] [Green Version]
- Ulmner, M.; Jarnbring, F.; Torring, O. Osteonecrosis of the jaw in Sweden associated with the oral use of bisphosphonate. J. Oral Maxillofac. Surg. 2014, 72, 76–82. [Google Scholar] [CrossRef]
- Dodson, T.B. The frequency of medication-related osteonecrosis of the jaw and its associated risk factors. Oral Maxillofac. Surg. Clin. North. Am. 2015, 27, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Limones, A.; Saez-Alcaide, L.M.; Diaz-Parreno, S.A.; Helm, A.; Bornstein, M.M.; Molinero-Mourelle, P. Medication-related osteonecrosis of the jaws (MRONJ) in cancer patients treated with denosumab VS. zoledronic acid: A systematic review and meta-analysis. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e326–e336. [Google Scholar] [CrossRef] [PubMed]
- Fung, P.; Bedogni, G.; Bedogni, A.; Petrie, A.; Porter, S.; Campisi, G.; Bagan, J.; Fusco, V.; Saia, G.; Acham, S.; et al. Time to onset of bisphosphonate-related osteonecrosis of the jaws: A multicentre retrospective cohort study. Oral Dis. 2017, 23, 477–483. [Google Scholar] [CrossRef]
- Kim, H.Y.; Kim, J.W.; Kim, S.J.; Lee, S.H.; Lee, H.S. Uncertainty of current algorithm for bisphosphonate-related osteonecrosis of the jaw in population-based studies: A systematic review. J. Bone Miner. Res. 2017, 32, 584–591. [Google Scholar] [CrossRef]
- Vahtsevanos, K.; Kyrgidis, A.; Verrou, E.; Katodritou, E.; Triaridis, S.; Andreadis, C.G.; Boukovinas, I.; Koloutsos, G.E.; Teleioudis, Z.; Kitikidou, K.; et al. Longitudinal cohort study of risk factors in cancer patients of bisphosphonate-related osteonecrosis of the jaw. J. Clin. Oncol. 2009, 27, 5356–5362. [Google Scholar] [CrossRef] [PubMed]
- Karna, H.; Gonzalez, J.; Radia, H.S.; Sedghizadeh, P.P.; Enciso, R. Risk-reductive dental strategies for medication related osteonecrosis of the jaw among cancer patients: A systematic review with meta-analyses. Oral Oncol. 2018, 85, 15–23. [Google Scholar] [CrossRef]
- Niibe, K.; Ouchi, T.; Iwasaki, R.; Nakagawa, T.; Horie, N. Osteonecrosis of the jaw in patients with dental prostheses being treated with bisphosphonates or denosumab. J. Prosthodont. Res. 2015, 59, 3–5. [Google Scholar] [CrossRef]
- Ripamonti, C.I.; Maniezzo, M.; Campa, T.; Fagnoni, E.; Brunelli, C.; Saibene, G.; Bareggi, C.; Ascani, L.; Cislaghi, E. Decreased occurrence of osteonecrosis of the jaw after implementation of dental preventive measures in solid tumour patients with bone metastases treated with bisphosphonates. The experience of the National Cancer Institute of Milan. Ann. Oncol. 2009, 20, 137–145. [Google Scholar] [CrossRef]
- Kannel, W.B.; Dawber, T.R.; Kagan, A.; Revotskie, N.; Stokes, J. Factors of risk in the development of coronary heart disease--six year follow-up experience. The Framingham Study. Ann. Intern. Med. 1961, 55, 33–50. [Google Scholar] [CrossRef] [PubMed]
- Barasch, A.; Cunha-Cruz, J.; Curro, F.A.; Hujoel, P.; Sung, A.H.; Vena, D.; Voinea-Griffin, A.E.; CONDOR Collaborative Group; Beadnell, S.; Craig, R.G.; et al. Risk factors for osteonecrosis of the jaws: A case-control study from the CONDOR dental PBRN. J. Dent. Res. 2011, 90, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Nowicki, B.; Nehrbass, D.; Arens, D.; Stadelmann, V.A.; Zeiter, S.; Otto, S.; Kircher, P.; Stoddart, M.J. Medication-related osteonecrosis of the jaw in a minipig model: Parameters for developing a macroscopic, radiological, and microscopic grading scheme. J. Cranio-Maxillofac. Surg. 2019, 47, 1162–1169. [Google Scholar] [CrossRef]
- Nicolatou-Galitis, O.; Razis, E.; Galiti, D.; Galitis, E.; Labropoulos, S.; Tsimpidakis, A.; Sgouros, J.; Karampeazis, A.; Migliorati, C. Periodontal disease preceding osteonecrosis of the jaw (ONJ) in cancer patients receiving antiresorptives alone or combined with targeted therapies: Report of 5 cases and literature review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Romero-Ruiz, M.M.; Romero-Serrano, M.; Serrano-Gonzalez, A.; Serrera-Figallo, M.A.; Gutierrez-Perez, J.L.; Torres-Lagares, D. Proposal for a preventive protocol for medication-related osteonecrosis of the jaw. Med. Oral Patol. Oral Cir. Bucal 2021, 26, e314–e326. [Google Scholar] [CrossRef]
- Peer, A.; Khamaisi, M. Diabetes as a risk factor for medication-related osteonecrosis of the jaw. J. Dent. Res. 2015, 94, 252–260. [Google Scholar] [CrossRef] [Green Version]
- Di Fede, O.; Bedogni, A.; Giancola, F.; Saia, G.; Bettini, G.; Toia, F.; D’Alessandro, N.; Firenze, A.; Matranga, D.; Fedele, S.; et al. BRONJ in patients with rheumatoid arthritis: A multicenter case series. Oral Dis. 2016, 22, 543–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- On, S.W.; Cho, S.W.; Byun, S.H.; Yang, B.E. Various therapeutic methods for the treatment of medication-related osteonecrosis of the jaw (MRONJ) and their limitations: A narrative review on new molecular and cellular therapeutic approaches. Antioxidants 2021, 10, 680. [Google Scholar] [CrossRef]
- Fusco, V.; Cabras, M.; Erovigni, F.; Dell’Acqua, A.; Arduino, P.G.; Pentenero, M.; Appendino, P.; Basano, L.; Ferrera, F.D.; Fasciolo, A.; et al. A multicenter observational study on Medication-Related Osteonecrosis of the Jaw (MRONJ) in advanced cancer and myeloma patients of a cancer network in North-Western Italy. Med. Oral Patol. Oral Cir. Bucal 2020, 26, e466–e473. [Google Scholar] [CrossRef]
- Owosho, A.A.; Liang, S.T.Y.; Sax, A.Z.; Wu, K.; Yom, S.K.; Huryn, J.M.; Estilo, C.L. Medication-related osteonecrosis of the jaw: An update on the memorial sloan kettering cancer center experience and the role of premedication dental evaluation in prevention. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Japanese Allied Committee on Osteonecrosis of the Jaw; Yoneda, T.; Hagino, H.; Sugimoto, T.; Ohta, H.; Takahashi, S.; Soen, S.; Taguchi, A.; Nagata, T.; Urade, M.; et al. Antiresorptive agent-related osteonecrosis of the jaw: Position Paper 2017 of the Japanese Allied Committee on Osteonecrosis of the Jaw. J. Bone Miner. Metab. 2017, 35, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Kun-Darbois, J.D.; Fauvel, F. Medication-related osteonecrosis and osteoradionecrosis of the jaws: Update and current management. Morphologie 2021, 105, 170–187. [Google Scholar] [CrossRef]
- Sandro Pereira da Silva, J.; Pullano, E.; Raje, N.S.; Troulis, M.J.; August, M. Genetic predisposition for medication-related osteonecrosis of the jaws: A systematic review. Int. J. Oral Maxillofac. Surg. 2019, 48, 1289–1299. [Google Scholar] [CrossRef]
- Lorenzo-Pouso, A.I.; Perez-Sayans, M.; Gonzalez-Palanca, S.; Chamorro-Petronacci, C.; Bagan, J.; Garcia-Garcia, A. Biomarkers to predict the onset of biphosphonate-related osteonecrosis of the jaw: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e26–e36. [Google Scholar] [CrossRef]
- Moraschini, V.; de Almeida, D.C.F.; Figueredo, C.M.; Calasans-Maia, M.D. Association between biomarkers and medication-related osteonecrosis of the jaws: A systematic review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 504–515. [Google Scholar] [CrossRef]
- Awad, M.E.; Sun, C.; Jernigan, J.; Elsalanty, M. Serum C-terminal cross-linking telopeptide level as a predictive biomarker of osteonecrosis after dentoalveolar surgery in patients receiving bisphosphonate therapy: Systematic review and meta-analysis. J. Am. Dent. Assoc. 2019, 150, 664–675.e8. [Google Scholar] [CrossRef] [PubMed]
- El-Rabbany, M.; Sgro, A.; Lam, D.K.; Shah, P.S.; Azarpazhooh, A. Effectiveness of treatments for medication-related osteonecrosis of the jaw: A systematic review and meta-analysis. J. Am. Dent. Assoc. 2017, 148, 584–594.e2. [Google Scholar] [CrossRef]
- Fortunato, L.; Bennardo, F.; Buffone, C.; Giudice, A. Is the application of platelet concentrates effective in the prevention and treatment of medication-related osteonecrosis of the jaw? A systematic review. J. Cranio-Maxillofac. Surg. 2020, 48, 268–285. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Ri, S.; Umeda, M.; Komatsubara, H.; Kobayashi, M.; Shigeta, T.; Yoshitomi, I.; Ikeda, H.; Shibuya, Y.; Asahina, I.; et al. The observational study of delayed wound healing after tooth extraction in patients receiving oral bisphosphonate therapy. J. Cranio-Maxillofac. Surg. 2013, 41, 558–563. [Google Scholar] [CrossRef]
- Corso, A.; Varettoni, M.; Zappasodi, P.; Klersy, C.; Mangiacavalli, S.; Pica, G.; Lazzarino, M. A different schedule of zoledronic acid can reduce the risk of the osteonecrosis of the jaw in patients with multiple myeloma. Leukemia 2007, 21, 1545–1548. [Google Scholar] [CrossRef] [PubMed]
- Tsourdi, E.; Langdahl, B.; Cohen-Solal, M.; Aubry-Rozier, B.; Eriksen, E.F.; Guanabens, N.; Obermayer-Pietsch, B.; Ralston, S.H.; Eastell, R.; Zillikens, M.C. Discontinuation of Denosumab therapy for osteoporosis: A systematic review and position statement by ECTS. Bone 2017, 105, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Mannion, C.J. Medication-related osteonecrosis of the jaws and quality of life: Review and structured analysis. Br. J. Oral Maxillofac. Surg. 2020, 58, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Diniz-Freitas, M.; Limeres, J. Prevention of medication-related osteonecrosis of the jaws secondary to tooth extractions. A systematic review. Med. Oral Patol. Oral Cir. Bucal 2016, 21, 250. [Google Scholar] [CrossRef]
- Fedele, S.; Kumar, N.; Davies, R.; Fiske, J.; Greening, S.; Porter, S. Dental management of patients at risk of osteochemonecrosis of the jaws: A critical review. Oral Dis. 2009, 15, 527–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruggiero, S.L.; Faia, J.; Carlson, E. Bisphosphonate-related osteonecrosis of the jaw: Background and guidelines for diagnosis, staging and management. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, 433–441. [Google Scholar] [CrossRef]
- Bedogni, A.; Fusco, V.; Agrillo, A.; Campisi, G. Learning from experience. Proposal of a refined definition and staging system for bisphosphonate-related osteonecrosis of the jaw (BRONJ). Oral Dis. 2012, 18, 621–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimamoto, H.; Grogan, T.R.; Tsujimoto, T.; Kakimoto, N.; Murakami, S.; Elashoff, D.; Aghaloo, T.L.; Tetradis, S. Does CBCT alter the diagnostic thinking efficacy, management and prognosis of patients with suspected Stage 0 medication-related osteonecrosis of the jaws? Dentomaxillofac. Radiol. 2018, 47, 20170290. [Google Scholar] [CrossRef]
- Bagan, L.; Leopoldo-Rodado, M.; Poveda-Roda, R.; Murillo-Cortes, J.; Diaz-Fernandez, J.M.; Bagan, J. Grade of sclerosis in the contralateral mandibular area in osteonecrosis of the jaws. Int. J. Oral Maxillofac. Surg. 2017, 46, 167–172. [Google Scholar] [CrossRef]
- Schiodt, M.; Reibel, J.; Oturai, P.; Kofod, T. Comparison of nonexposed and exposed bisphosphonate-induced osteonecrosis of the jaws: A retrospective analysis from the Copenhagen cohort and a proposal for an updated classification system. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 204–213. [Google Scholar] [CrossRef]
- O’Ryan, F.S.; Khoury, S.; Liao, W.; Han, M.M.; Hui, R.L.; Baer, D.; Martin, D.; Liberty, D.; Lo, J.C. Intravenous bisphosphonate-related osteonecrosis of the jaw: Bone scintigraphy as an early indicator. J. Oral Maxillofac. Surg. 2009, 67, 1363–1372. [Google Scholar] [CrossRef]
- Junquera, L.; Gallego, L. Nonexposed bisphosphonate-related osteonecrosis of the jaws: Another clinical variant? J. Oral Maxillofac. Surg. 2008, 66, 1516–1517. [Google Scholar] [CrossRef]
- Migliorati, C.A.; Epstein, J.B.; Abt, E.; Berenson, J.R. Osteonecrosis of the jaw and bisphosphonates in cancer: A narrative review. Nat. Rev. Endocrinol. 2011, 7, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Ristow, O.; Ruckschloss, T.; Muller, M.; Berger, M.; Kargus, S.; Pautke, C.; Engel, M.; Hoffmann, J.; Freudlsperger, C. Is the conservative non-surgical management of medication-related osteonecrosis of the jaw an appropriate treatment option for early stages? A long-term single-center cohort study. J. Cranio-Maxillofac. Surg. 2019, 47, 491–499. [Google Scholar] [CrossRef]
- Van den Wyngaert, T.; Claeys, T.; Huizing, M.T.; Vermorken, J.B.; Fossion, E. Initial experience with conservative treatment in cancer patients with osteonecrosis of the jaw (ONJ) and predictors of outcome. Ann. Oncol. 2009, 20, 331–336. [Google Scholar] [CrossRef]
- Kim, K.M.; Rhee, Y.; Kwon, Y.D.; Kwon, T.G.; Lee, J.K.; Kim, D.Y. Medication related osteonecrosis of the jaw: 2015 position statement of the Korean Society for Bone and Mineral Research and the Korean Association of Oral and Maxillofacial Surgeons. J. Bone Metab. 2015, 22, 151–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagan, J.; Blade, J.; Cozar, J.M.; Constela, M.; Garcia Sanz, R.; Gomez Veiga, F.; Lahuerta, J.J.; Lluch, A.; Massuti, B.; Morote, J.; et al. Recommendations for the prevention, diagnosis, and treatment of osteonecrosis of the jaw (ONJ) in cancer patients treated with bisphosphonates. Med. Oral Patol. Oral Cir. Bucal 2007, 12, 336. [Google Scholar]
- Ewald, F.; Wuesthoff, F.; Koehnke, R.; Friedrich, R.E.; Gosau, M.; Smeets, R.; Rohde, H.; Assaf, A.T. Retrospective analysis of bacterial colonization of necrotic bone and antibiotic resistance in 98 patients with medication-related osteonecrosis of the jaw (MRONJ). Clin. Oral Investig. 2021, 25, 2801–2809. [Google Scholar] [CrossRef] [PubMed]
- Campisi, G.; Fedele, S.; Fusco, V.; Pizzo, G.; Di Fede, O.; Bedogni, A. Epidemiology, clinical manifestations, risk reduction and treatment strategies of jaw osteonecrosis in cancer patients exposed to antiresorptive agents. Future Oncol. 2014, 10, 257–275. [Google Scholar] [CrossRef] [Green Version]
- Russmueller, G.; Seemann, R.; Weiss, K.; Stadler, V.; Speiss, M.; Perisanidis, C.; Fuereder, T.; Willinger, B.; Sulzbacher, I.; Steininger, C. The association of medication-related osteonecrosis of the jaw with Actinomyces spp. infection. Sci. Rep. 2016, 6, 31604. [Google Scholar] [CrossRef] [Green Version]
- Hadaya, D.; Soundia, A.; Freymiller, E.; Grogan, T.; Elashoff, D.; Tetradis, S.; Aghaloo, T.L. Nonsurgical management of medication-related osteonecrosis of the jaws using local wound care. J. Oral Maxillofac. Surg. 2018, 76, 2332–2339. [Google Scholar] [CrossRef]
- Pippi, R.; Giuliani, U.; Tenore, G.; Pietrantoni, A.; Romeo, U. What is the risk of developing medication-related osteonecrosis in patients with extraction sockets left to heal by secondary intention? A retrospective case series study. J. Oral Maxillofac. Surg. 2021. [Google Scholar] [CrossRef]
- Favia, G.; Tempesta, A.; Limongelli, L.; Crincoli, V.; Maiorano, E. Medication-related osteonecrosis of the jaw: Surgical or non-surgical treatment? Oral Dis. 2018, 24, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo-Pouso, A.I.; Perez-Sayans, M.; Chamorro-Petronacci, C.; Gandara-Vila, P.; Lopez-Jornet, P.; Carballo, J.; Garcia-Garcia, A. Association between periodontitis and medication-related osteonecrosis of the jaw: A systematic review and meta-analysis. J. Oral Pathol. Med. 2020, 49, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Kohn, N. Disease stage and mode of therapy are important determinants of treatment outcomes for medication-related osteonecrosis of the jaw. J. Oral Maxillofac. Surg. 2015, 73, S94–S100. [Google Scholar] [CrossRef]
- Giudice, A.; Barone, S.; Diodati, F.; Antonelli, A.; Nocini, R.; Cristofaro, M.G. Can surgical management improve resolution of medication-related osteonecrosis of the jaw at early stages? A prospective cohort study. J. Oral Maxillofac. Surg. 2020, 78, 1986–1999. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Dodson, T.B.; Assael, L.A.; Landesberg, R.; Marx, R.E.; Mehrotra, B.; American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws—2009 update. J. Oral Maxillofac. Surg. 2009, 67, 2–12. [Google Scholar] [CrossRef]
- Wilde, F.; Heufelder, M.; Winter, K.; Hendricks, J.; Frerich, B.; Schramm, A.; Hemprich, A. The role of surgical therapy in the management of intravenous bisphosphonates-related osteonecrosis of the jaw. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 111, 153–163. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M. How to optimize the preparation of leukocyte- and platelet-rich fibrin (L-PRF, Choukroun’s technique) clots and membranes: Introducing the PRF Box. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Jornet, P.; Sanchez Perez, A.; Amaral Mendes, R.; Tobias, A. Medication-related osteonecrosis of the jaw: Is autologous platelet concentrate application effective for prevention and treatment? A systematic review. J. Craniomaxillofac. Surg. 2016, 44, 1067–1072. [Google Scholar] [CrossRef]
- Goker, F.; Grecchi, E.; Grecchi, F.; Francetti, L.; Del Fabbro, M. Treatment of medication-related osteonecrosis of the jaw (MRONJ). A systematic review. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 2662–2673. [Google Scholar] [PubMed]
- Vidal-Real, C.; Perez-Sayans, M.; Suarez-Penaranda, J.M.; Gandara-Rey, J.M.; Garcia-Garcia, A. Osteonecrosis of the jaws in 194 patients who have undergone intravenous bisphosphonate therapy in Spain. Med. Oral Patol. Oral Cir. Bucal 2015, 20, 267. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Garcia, A.; Somoza-Martin, M.; Gandara-Rey, J.M.; Perez-Sayans, M. Surgical neurolysis for the treatment of neuropathic pain in 2 postmenopausal women with mandibular necrosis resulting from oral bisphosphonates. J. Craniofac. Surg. 2014, 25, 1369–1371. [Google Scholar] [CrossRef]
- Aljohani, S.; Troeltzsch, M.; Hafner, S.; Kaeppler, G.; Mast, G.; Otto, S. Surgical treatment of medication-related osteonecrosis of the upper jaw: Case series. Oral Dis. 2019, 25, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Otto, S.; Schnodt, E.M.; Haidari, S.; Brunner, T.F.; Aljohani, S.; Mosleh, M.; Ristow, O.; Troeltzsch, M.; Pautke, C.; Ehrenfeld, M.; et al. Autofluorescence-guided surgery for the treatment of medication-related osteonecrosis of the jaw (MRONJ): A retrospective single-center study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 519–526. [Google Scholar] [CrossRef]
- Blus, C.; Giannelli, G.; Szmukler-Moncler, S.; Orru, G. Treatment of medication-related osteonecrosis of the jaws (MRONJ) with ultrasonic piezoelectric bone surgery. A case series of 20 treated sites. Oral Maxillofac. Surg. 2017, 21, 41–48. [Google Scholar] [CrossRef]
- Giudice, A.; Bennardo, F.; Barone, S.; Antonelli, A.; Figliuzzi, M.M.; Fortunato, L. Can autofluorescence guide surgeons in the treatment of medication-related osteonecrosis of the jaw? A prospective feasibility study. J. Oral Maxillofac. Surg. 2018, 76, 982–995. [Google Scholar] [CrossRef]
- Tomo, S.; da Cruz, T.M.; Figueira, J.A.; Cunha, J.L.S.; Miyahara, G.I.; Simonato, L.E. Fluorescence-guided surgical management of medication-related osteonecrosis of the jaws. Photodiagnosis Photodyn. Ther. 2020, 32, 102003. [Google Scholar] [CrossRef]
- Vescovi, P.; Merigo, E.; Meleti, M.; Fornaini, C.; Nammour, S.; Manfredi, M. Nd:YAG laser biostimulation of bisphosphonate-associated necrosis of the jawbone with and without surgical treatment. Br. J. Oral Maxillofac. Surg. 2007, 45, 628–632. [Google Scholar] [CrossRef]
- Altay, M.A.; Tasar, F.; Tosun, E.; Kan, B. Low-level laser therapy supported surgical treatment of bisphosphonate related osteonecrosis of jaws: A retrospective analysis of 11 cases. Photomed. Laser Surg. 2014, 32, 468–475. [Google Scholar] [CrossRef]
- Kakehashi, H.; Ando, T.; Minamizato, T.; Nakatani, Y.; Kawasaki, T.; Ikeda, H.; Kuroshima, S.; Kawakami, A.; Asahina, I. Administration of teriparatide improves the symptoms of advanced bisphosphonate-related osteonecrosis of the jaw: Preliminary findings. Int. J. Oral Maxillofac. Surg. 2015, 44, 1558–1564. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.; Yoo, H.Y.; Kim, G.T.; Lee, J.W.; Lee, Y.A.; Kim, D.Y.; Kwon, Y.D. Short-term teriparatide and recombinant human bone morphogenetic protein-2 for regenerative approach to medication-related osteonecrosis of the Jaw: A preliminary study. J. Bone Miner. Res. 2017, 32, 2445–2452. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorenzo-Pouso, A.I.; Bagán, J.; Bagán, L.; Gándara-Vila, P.; Chamorro-Petronacci, C.M.; Castelo-Baz, P.; Blanco-Carrión, A.; Blanco-Fernández, M.Á.; Álvarez-Calderón, Ó.; Carballo, J.; et al. Medication-Related Osteonecrosis of the Jaw: A Critical Narrative Review. J. Clin. Med. 2021, 10, 4367. https://doi.org/10.3390/jcm10194367
Lorenzo-Pouso AI, Bagán J, Bagán L, Gándara-Vila P, Chamorro-Petronacci CM, Castelo-Baz P, Blanco-Carrión A, Blanco-Fernández MÁ, Álvarez-Calderón Ó, Carballo J, et al. Medication-Related Osteonecrosis of the Jaw: A Critical Narrative Review. Journal of Clinical Medicine. 2021; 10(19):4367. https://doi.org/10.3390/jcm10194367
Chicago/Turabian StyleLorenzo-Pouso, Alejandro I., José Bagán, Leticia Bagán, Pilar Gándara-Vila, Cintia M. Chamorro-Petronacci, Pablo Castelo-Baz, Andrés Blanco-Carrión, María Ángeles Blanco-Fernández, Óscar Álvarez-Calderón, Javier Carballo, and et al. 2021. "Medication-Related Osteonecrosis of the Jaw: A Critical Narrative Review" Journal of Clinical Medicine 10, no. 19: 4367. https://doi.org/10.3390/jcm10194367
APA StyleLorenzo-Pouso, A. I., Bagán, J., Bagán, L., Gándara-Vila, P., Chamorro-Petronacci, C. M., Castelo-Baz, P., Blanco-Carrión, A., Blanco-Fernández, M. Á., Álvarez-Calderón, Ó., Carballo, J., & Pérez-Sayáns, M. (2021). Medication-Related Osteonecrosis of the Jaw: A Critical Narrative Review. Journal of Clinical Medicine, 10(19), 4367. https://doi.org/10.3390/jcm10194367