
Radioactive Iodine Treatment and the Risk of Long-Term Cardiovascular Morbidity and Mortality in Thyroid Cancer Patients: A Nationwide Cohort Study

 , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
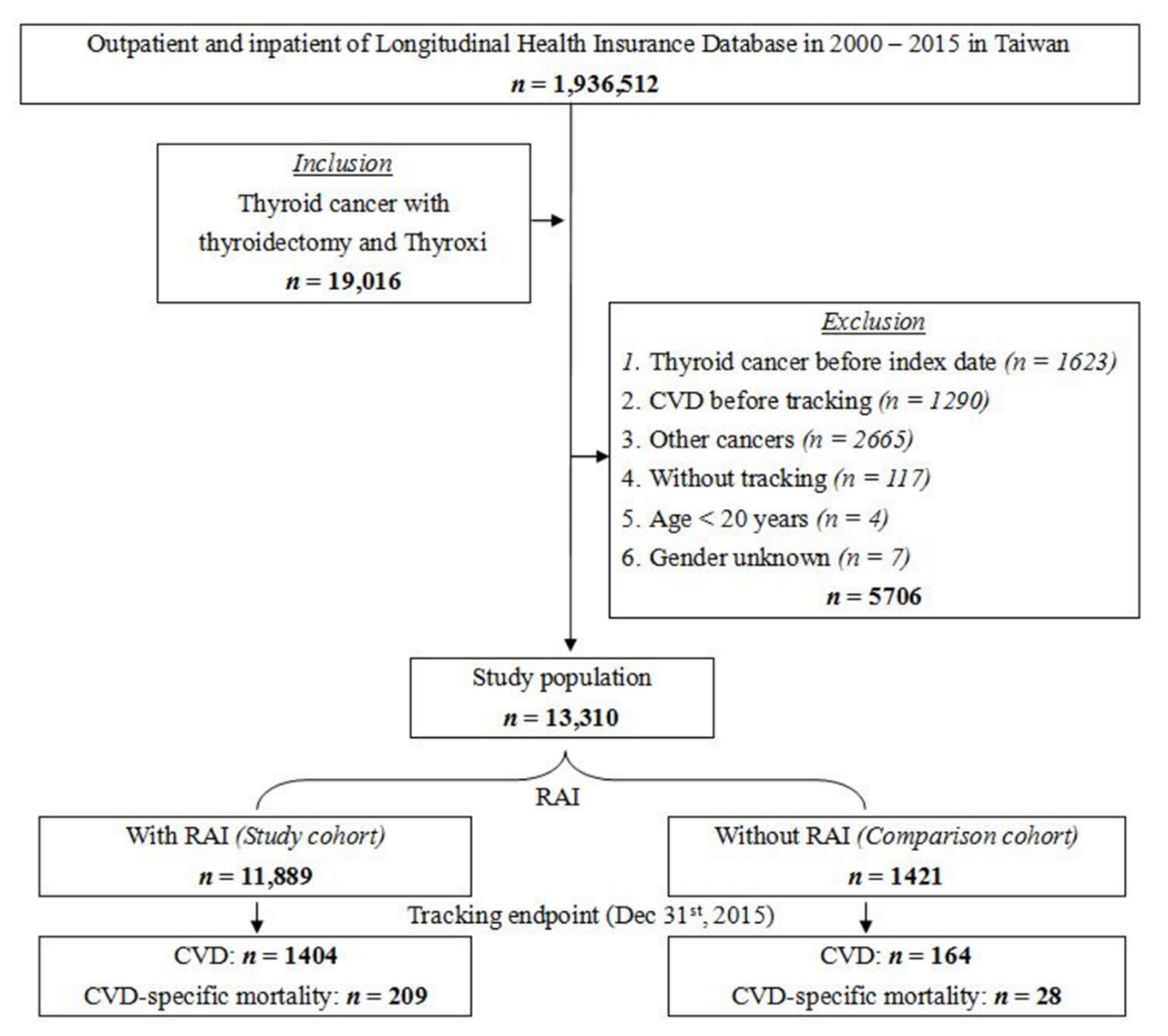
2.2. Study Design and Population
2.3. Comorbidities
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Control and Study Groups
3.2. Risk Factors of CVD and CVD-Specific Mortality
3.3. Cumulative RAI Dosages and Risks of CVD and CVD-Specific Mortality
3.4. Risks of Subgroups of CVD and CVD-Specific Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- La Vecchia, C.; Malvezzi, M.; Bosetti, C.; Garavello, W.; Bertuccio, P.; Levi, F.; Negri, E. Thyroid cancer mortality and incidence: A global overview. Int. J. Cancer 2015, 136, 2187–2195. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, M.E.; McFadden, D.G.; Durante, C. Thyroid cancer. Lancet 2016, 388, 2783–2795. [Google Scholar] [CrossRef]
- Mazzaferri, E.L.; Kloos, R.T. Clinical review 128: Current approaches to primary therapy for papillary and follicular thyroid cancer. J. Clin. Endocrinol. Metab. 2001, 86, 1447–1463. [Google Scholar] [CrossRef] [PubMed]
- Fard-Esfahani, A.; Emami-Ardekani, A.; Fallahi, B.; Fard-Esfahani, P.; Beiki, D.; Hassanzadeh-Rad, A.; Eftekhari, M. Adverse effects of radioactive iodine-131 treatment for differentiated thyroid carcinoma. Nucl. Med. Commun. 2014, 35, 808–817. [Google Scholar] [CrossRef] [Green Version]
- la Cour, J.L.; Jensen, L.T.; Vej-Hansen, A.; Nygaard, B. Radioiodine therapy increases the risk of cerebrovascular events in hyperthyroid and euthyroid patients. Eur. J. Endocrinol. 2015, 172, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Klein Hesselink, E.N.; Lefrandt, J.D.; Schuurmans, E.P.; Burgerhof, J.G.; Groen, B.; Gansevoort, R.T.; van der Horst-Schrivers, A.N.; Dullaart, R.P.; Van Gelder, I.C.; Brouwers, A.H.; et al. Increased Risk of Atrial Fibrillation After Treatment for Differentiated Thyroid Carcinoma. J. Clin. Endocrinol. Metab. 2015, 100, 4563–4569. [Google Scholar] [CrossRef] [Green Version]
- Desouky, O.; Ding, N.; Zhou, G. Targeted and non-targeted effects of ionizing radiation. J. Radiat. Res. Appl. Sci. 2015, 8, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Brusselaers, N.; Lagergren, J. The Charlson Comorbidity Index in Registry-based Research. Methods Inf. Med. 2017, 56, 401–406. [Google Scholar] [CrossRef]
- Klein Hesselink, E.N.; Klein Hesselink, M.S.; de Bock, G.H.; Gansevoort, R.T.; Bakker, S.J.; Vredeveld, E.J.; van der Horst-Schrivers, A.N.; van der Horst, I.C.; Kamphuisen, P.W.; Plukker, J.T.; et al. Long-term cardiovascular mortality in patients with differentiated thyroid carcinoma: An observational study. J. Clin. Oncol. 2013, 31, 4046–4053. [Google Scholar] [CrossRef] [Green Version]
- Abonowara, A.; Quraishi, A.; Sapp, J.L.; Alqambar, M.H.; Saric, A.; O’Connell, C.M.; Rajaraman, M.M.; Hart, R.D.; Imran, S.A. Prevalence of atrial fibrillation in patients taking TSH suppression therapy for management of thyroid cancer. Clin. Investig. Med. 2012, 35, E152–E156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.Y.; Smith, A.W.; Palmer, F.L.; Tuttle, R.M.; Mahrous, A.; Nixon, I.J.; Patel, S.G.; Ganly, I.; Fagin, J.A.; Boucai, L. Thyrotropin suppression increases the risk of osteoporosis without decreasing recurrence in ATA low- and intermediate-risk patients with differentiated thyroid carcinoma. Thyroid 2015, 25, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Cooper, D.S.; Biondi, B. Subclinical thyroid disease. Lancet 2012, 379, 1142–1154. [Google Scholar] [CrossRef]
- Izkhakov, E.; Meyerovitch, J.; Barchana, M.; Shacham, Y.; Stern, N.; Keinan-Boker, L. Long-term cardiovascular and cerebrovascular morbidity in Israeli thyroid cancer survivors. Endocr. Connect. 2019, 8, 398–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pajamaki, N.; Metso, S.; Hakala, T.; Ebeling, T.; Huhtala, H.; Ryodi, E.; Sand, J.; Jukkola-Vuorinen, A.; Kellokumpu-Lehtinen, P.L.; Jaatinen, P. Long-term cardiovascular morbidity and mortality in patients treated for differentiated thyroid cancer. Clin. Endocrinol. 2018, 88, 303–310. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Blackburn, B.E.; Ganz, P.A.; Rowe, K.; Snyder, J.; Wan, Y.; Deshmukh, V.; Newman, M.; Fraser, A.; Smith, K.; et al. Risk Factors for Cardiovascular Disease Among Thyroid Cancer Survivors: Findings From the Utah Cancer Survivors Study. J. Clin. Endocrinol. Metab. 2018, 103, 2468–2477. [Google Scholar] [CrossRef]
- Klein Hesselink, M.S.; Bocca, G.; Hummel, Y.M.; Brouwers, A.H.; Burgerhof, J.G.M.; van Dam, E.; Gietema, J.A.; Havekes, B.; van den Heuvel-Eibrink, M.M.; Corssmit, E.P.M.; et al. Diastolic Dysfunction is Common in Survivors of Pediatric Differentiated Thyroid Carcinoma. Thyroid 2017, 27, 1481–1489. [Google Scholar] [CrossRef] [Green Version]
- Suh, B.; Shin, D.W.; Park, Y.; Lim, H.; Yun, J.M.; Song, S.O.; Park, J.H.; Cho, B.; Guallar, E. Increased cardiovascular risk in thyroid cancer patients taking levothyroxine: A nationwide cohort study in Korea. Eur. J. Endocrinol. 2019, 180, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Shargorodsky, M.; Serov, S.; Gavish, D.; Leibovitz, E.; Harpaz, D.; Zimlichman, R. Long-term thyrotropin-suppressive therapy with levothyroxine impairs small and large artery elasticity and increases left ventricular mass in patients with thyroid carcinoma. Thyroid 2006, 16, 381–386. [Google Scholar] [CrossRef]
- Smit, J.W.; Eustatia-Rutten, C.F.; Corssmit, E.P.; Pereira, A.M.; Frolich, M.; Bleeker, G.B.; Holman, E.R.; van der Wall, E.E.; Romijn, J.A.; Bax, J.J. Reversible diastolic dysfunction after long-term exogenous subclinical hyperthyroidism: A randomized, placebo-controlled study. J. Clin. Endocrinol. Metab. 2005, 90, 6041–6047. [Google Scholar] [CrossRef] [Green Version]
- Abdulrahman, R.M.; Delgado, V.; Hoftijzer, H.C.; Ng, A.C.; Ewe, S.H.; Marsan, N.A.; Holman, E.R.; Hovens, G.C.; Corssmit, E.P.; Romijn, J.A.; et al. Both exogenous subclinical hyperthyroidism and short-term overt hypothyroidism affect myocardial strain in patients with differentiated thyroid carcinoma. Thyroid 2011, 21, 471–476. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- la Cour, J.L.; Andersen, U.B.; Sorensen, C.H.; Nygaard, B.; Jensen, L.T. Radioiodine Therapy Does Not Change the Atherosclerotic Burden of the Carotid Arteries. Thyroid 2016, 26, 965–971. [Google Scholar] [CrossRef] [Green Version]
- Sanal, B.; Isik, I.; Korkmaz, M.; Kucur, C.; Can, F.; Kilit, T.P.; Kahraman, C.; Kacar, E.; Kocak, A. Effect of radioactive iodine therapy on carotid intima media thickness in patients with hyperthyroidism. Ann. Nucl. Med. 2016, 30, 75–80. [Google Scholar] [CrossRef]
- Lin, C.Y.; Lin, C.L.; Lo, Y.C.; Kao, C.H. Association between radioiodine treatment for thyroid cancer and risk of stroke. Head Neck 2017, 39, 2311–2318. [Google Scholar] [CrossRef]
- Shen, D.; Chen, C.-Y.; Jhiang, S.; Huang, W.-S. Sodium Iodide Symporter (Na+/I- Symporter) in Radionuclide Imaging and Radionuclide therapy. Nucl. Med. Sci. 2003, 16, 85–96. [Google Scholar]
- Ravera, S.; Reyna-Neyra, A.; Ferrandino, G.; Amzel, L.M.; Carrasco, N. The Sodium/Iodide Symporter (NIS): Molecular Physiology and Preclinical and Clinical Applications. Annu. Rev. Physiol. 2017, 79, 261–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spitzweg, C.; Joba, W.; Eisenmenger, W.; Heufelder, A.E. Analysis of human sodium iodide symporter gene expression in extrathyroidal tissues and cloning of its complementary deoxyribonucleic acids from salivary gland, mammary gland, and gastric mucosa. J. Clin. Endocrinol. Metab. 1998, 83, 1746–1751. [Google Scholar] [CrossRef] [PubMed]
- Little, M.P.; Tawn, E.J.; Tzoulaki, I.; Wakeford, R.; Hildebrandt, G.; Paris, F.; Tapio, S.; Elliott, P. A systematic review of epidemiological associations between low and moderate doses of ionizing radiation and late cardiovascular effects, and their possible mechanisms. Radiat. Res. 2008, 169, 99–109. [Google Scholar] [CrossRef]
- Stewart, F.A. Mechanisms and dose-response relationships for radiation-induced cardiovascular disease. Ann. ICRP 2012, 41, 72–79. [Google Scholar] [CrossRef]
- Stewart, F.A.; Heeneman, S.; Te Poele, J.; Kruse, J.; Russell, N.S.; Gijbels, M.; Daemen, M. Ionizing radiation accelerates the development of atherosclerotic lesions in ApoE-/- mice and predisposes to an inflammatory plaque phenotype prone to hemorrhage. Am. J. Pathol. 2006, 168, 649–658. [Google Scholar] [CrossRef] [Green Version]
- An, J.H.; Song, K.H.; Kim, D.L.; Kim, S.K. Effects of thyroid hormone withdrawal on metabolic and cardiovascular parameters during radioactive iodine therapy in differentiated thyroid cancer. J. Int. Med. Res. 2017, 45, 38–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.Y.; Chang, J.S.; Huang, S.M.; Hung, C.J.; Hung, C.L.; Chang, C.T.; Yang, H.R.; Hsieh, T.C.; Huang, Y.H.; Tsai, H.J. Experience of sorafenib treatment in differentiated thyroid cancer from Taiwan. J. Formos. Med. Assoc. 2021, 120, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.M.; Yeh, P.T.; Doyle, P.; Tsan, Y.T.; Chen, P.C. Association Between 131I Treatment for Thyroid Cancer and Risk of Receiving Cataract Surgery: A Cohort Study from Taiwan. J. Nucl. Med. 2016, 57, 836–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, K.Y.; Kao, C.H.; Lin, C.L.; Huang, W.S.; Yen, R.F. (131)I treatment for thyroid cancer and the risk of developing salivary and lacrimal gland dysfunction and a second primary malignancy: A nationwide population-based cohort study. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1172–1178. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | RAI Group | Non-RAI Group | p | |||
| n | % | n | % | |||
| Total | 11,889 | 89.3 | 1421 | 10.7 | ||
| Gender | Male | 2259 | 19.0 | 289 | 20.3 | 0.12 |
| Female | 9630 | 81.0 | 1132 | 79.7 | ||
| Age (years) | 47.3 ± 13.2 | 47.2± 13.2 | 0.70 | |||
| Age groups (years) | 20–39 | 3673 | 30.9 | 437 | 30.8 | 1.00 |
| 40–59 | 6217 | 52.3 | 744 | 52.4 | ||
| 60–79 | 1910 | 16.1 | 229 | 16.1 | ||
| ≥80 | 89 | 0.8 | 11 | 0.8 | ||
| DM | Without | 11,216 | 94.3 | 1350 | 95.0 | 0.17 |
| With | 673 | 5.7 | 71 | 5.0 | ||
| CKD | Without | 11,757 | 98.89 | 1413 | 99.4 | 0.04 |
| With | 132 | 1.1 | 8 | 0.6 | ||
| Hyperlipidemia | Without | 11,752 | 98.85 | 1408 | 99.1 | 0.25 |
| With | 137 | 1.2 | 13 | 0.9 | ||
| Duration of levothyroxine without dosage adjustment (years) | 1 ≤ years <2 | 1815 | 15.3 | 219 | 15.4 | 0.11 |
| 2 ≤ years < 6 | 4249 | 35.7 | 552 | 38.9 | ||
| 6 ≤ years <11 | 3328 | 28.0 | 364 | 25.6 | ||
| ≥11 years | 2497 | 21.0 | 286 | 20.1 | ||
| CCI_R | 0.08 ± 0.28 | 0.07 ± 0.28 | 0.25 | |||
| Outcome | CVD | CVD-Specific Mortality | |||||
|---|---|---|---|---|---|---|---|
| Variables | Adjusted HR | 95% CI | P | Adjusted HR | 95% CI | p | |
| RAI | Without | Reference | Reference | ||||
| With | 0.99 | 0.84–1.16 | 0.88 | 0.92 | 0.62–1.37 | 0.68 | |
| Gender | Female | Reference | Reference | ||||
| Male | 1.32 | 1.17–1.48 | <0.001 | 1.22 | 0.91–1.63 | 0.19 | |
| Age groups (yrs) | 20–39 | Reference | Reference | ||||
| 40–59 | 1.66 | 1.37–2.00 | <0.001 | 2.58 | 1.09–6.13 | 0.03 | |
| 60–79 | 2.73 | 0.26–0.30 | <0.001 | 10.42 | 4.55–23.87 | <0.001 | |
| ≥80 | 4.42 | 3.56–5.48 | <0.001 | 31.48 | 13.62–72.75 | <0.001 | |
| DM | Without | Reference | Reference | ||||
| With | 0.84 | 0.70–1.01 | 0.06 | 0.63 | 0.39–1.04 | 0.07 | |
| CKD | Without | Reference | Reference | ||||
| With | 1.85 | 1.51–2.27 | <0.001 | 3.94 | 2.75–5.64 | <0.001 | |
| Hyper- lipidemia | Without | Reference | Reference | ||||
| With | 1.538 | 1.24–1.91 | <0.001 | 0.12 | 0.02–0.83 | 0.03 | |
| CCI_R | 1.43 | 1.28–1.60 | <0.001 | 0.98 | 0.71–1.34 | 0.88 | |
| Outcome | Dose of RAI | Populations | Events | PYs | Rate | Adjusted HR | 95% CI | p |
|---|---|---|---|---|---|---|---|---|
| CVD | Without | 1421 | 164 | 2744.86 | 5974.81 | Reference | ||
| With | 11,889 | 1404 | 22,899.15 | 6131.23 | 0.99 | 0.84–1.16 | 0.88 | |
| 0.037–1.11 GBq | 5491 | 503 | 9678.65 | 5197.00 | 0.97 | 0.59–1.03 | 0.85 | |
| 1.147–3.7 GBq | 678 | 155 | 2468.54 | 6279.01 | 1.30 | 0.94–1.74 | 0.73 | |
| 3.737–5.55 GBq | 231 | 99 | 1482.99 | 6675.72 | 1.56 | 1.17–2.12 | <0.001 | |
| >5.55 GBq | 5489 | 647 | 9268.97 | 6980.28 | 1.69 | 1.24–2.40 | <0.001 | |
| CVD- specificmortality | Without | 1421 | 28 | 3058.93 | 915.35 | Reference | ||
| With | 11,889 | 209 | 25,642.17 | 815.06 | 0.92 | 0.62–1.37 | 0.68 | |
| 0.037–1.11 GBq | 5491 | 72 | 10,989.12 | 655.19 | 0.75 | 0.39–1.19 | 0.70 | |
| 1.147–3.7 GBq | 678 | 20 | 2601.86 | 768.68 | 0.88 | 0.45–1.36 | 0.51 | |
| 3.737–5.55 GBq | 231 | 17 | 1768.25 | 961.40 | 1.28 | 0.80–1.78 | 0.29 | |
| >5.55 GBq | 5489 | 100 | 10,282.94 | 972.48 | 1.75 | 1.10–2.28 | 0.001 |
| RAI Group | Non-RAI Group | RAI vs. Non-RAI(Reference) | ||||||||
| Outcome Subgroup | Events | PYs | Rate | Events | PYs | Rate | Ratio | Adjusted HR | 95% CI | P |
| Any combination of the listed CVD | 1404 | 22,899.15 | 6131.23 | 164 | 2744.86 | 5974.81 | 1.03 | 0.99 | 0.84–1.16 | 0.88 |
| Ischemic heart diseases | 570 | 24,463.32 | 2330.02 | 63 | 2933.78 | 2147.40 | 1.09 | 1.02 | 0.78–1.32 | 0.89 |
| Diseases of pulmonary circulation | 59 | 25,529.81 | 231.10 | 6 | 3054.33 | 196.44 | 1.18 | 1.13 | 0.49–2.64 | 0.77 |
| AF | 68 | 24,602.99 | 276.39 | 7 | 2910.87 | 240.48 | 1.15 | 1.11 | 0.94–1.31 | 0.14 |
| Other forms of heart disease | 497 | 24,607.98 | 2019.67 | 60 | 2876.80 | 2085.65 | 0.97 | 0.93 | 0.79–1.10 | 0.73 |
| Cerebrovascular diseases | 385 | 24,857.84 | 1548.81 | 43 | 2998.36 | 1434.12 | 1.08 | 1.02 | 0.74–1.40 | 0.91 |
| Diseases of arteries, arterioles, and capillaries | 70 | 25,497.55 | 274.54 | 7 | 3048.98 | 229.59 | 1.20 | 1.17 | 0.53–2.55 | 0.70 |
| Veins and lymphatics, and other | 337 | 25,024.94 | 1346.66 | 38 | 2997.21 | 1267.84 | 1.06 | 1.08 | 0.77–1.51 | 0.66 |
| CVD-specific mortality | 209 | 25,642.17 | 815.06 | 28 | 3058.93 | 915.35 | 0.89 | 0.92 | 0.62–1.37 | 0.68 |
| Ischemic heart diseases | 55 | 25,642.17 | 214.49 | 10 | 3058.93 | 326.91 | 0.66 | 0.70 | 0.35–1.39 | 0.30 |
| Diseases of pulmonary circulation | 10 | 25,642.17 | 39.00 | 0 | 3058.93 | 0.00 | ∞ | ∞ | - | 0.84 |
| AF | 10 | 25,642.17 | 39.00 | 1 | 3058.93 | 32.69 | 1.193 | 1.15 | 0.97–1.35 | 0.08 |
| Other forms of heart diseases | 88 | 25,642.17 | 343.18 | 11 | 3058.93 | 359.60 | 0.954 | 0.92 | 0.78–1.08 | 0.80 |
| Cerebrovascular diseases | 44 | 25,642.17 | 171.59 | 6 | 3058.93 | 196.15 | 0.88 | 0.84 | 0.35–2.00 | 0.70 |
| Diseases of arteries, arterioles, and capillaries | 9 | 25,642.17 | 35.10 | 1 | 3058.93 | 32.69 | 1.07 | 1.09 | 0.14–8.80 | 0.94 |
| Veins and lymphatics, and other | 32 | 25,642.17 | 124.79 | 3 | 3058.93 | 98.07 | 1.27 | 1.18 | 0.36–3.90 | 0.78 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kao, C.-H.; Chung, C.-H.; Chien, W.-C.; Shen, D.H.-Y.; Lin, L.-F.; Chiu, C.-H.; Cheng, C.-Y.; Sun, C.-A.; Chang, P.-Y. Radioactive Iodine Treatment and the Risk of Long-Term Cardiovascular Morbidity and Mortality in Thyroid Cancer Patients: A Nationwide Cohort Study. J. Clin. Med. 2021, 10, 4032. https://doi.org/10.3390/jcm10174032
Kao C-H, Chung C-H, Chien W-C, Shen DH-Y, Lin L-F, Chiu C-H, Cheng C-Y, Sun C-A, Chang P-Y. Radioactive Iodine Treatment and the Risk of Long-Term Cardiovascular Morbidity and Mortality in Thyroid Cancer Patients: A Nationwide Cohort Study. Journal of Clinical Medicine. 2021; 10(17):4032. https://doi.org/10.3390/jcm10174032
Chicago/Turabian StyleKao, Chun-Hao, Chi-Hsiang Chung, Wu-Chien Chien, Daniel Hueng-Yuan Shen, Li-Fan Lin, Chuang-Hsin Chiu, Cheng-Yi Cheng, Chien-An Sun, and Ping-Ying Chang. 2021. "Radioactive Iodine Treatment and the Risk of Long-Term Cardiovascular Morbidity and Mortality in Thyroid Cancer Patients: A Nationwide Cohort Study" Journal of Clinical Medicine 10, no. 17: 4032. https://doi.org/10.3390/jcm10174032
APA StyleKao, C.-H., Chung, C.-H., Chien, W.-C., Shen, D. H.-Y., Lin, L.-F., Chiu, C.-H., Cheng, C.-Y., Sun, C.-A., & Chang, P.-Y. (2021). Radioactive Iodine Treatment and the Risk of Long-Term Cardiovascular Morbidity and Mortality in Thyroid Cancer Patients: A Nationwide Cohort Study. Journal of Clinical Medicine, 10(17), 4032. https://doi.org/10.3390/jcm10174032