
Treatment of Urethral Strictures in Transmasculine Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy, Selection of Studies, and Data Extraction
2.2. Types of Study Designs Included
2.3. Types of Participants Included
2.4. Types of Interventions Included
2.5. Types of Outcome Measures Included
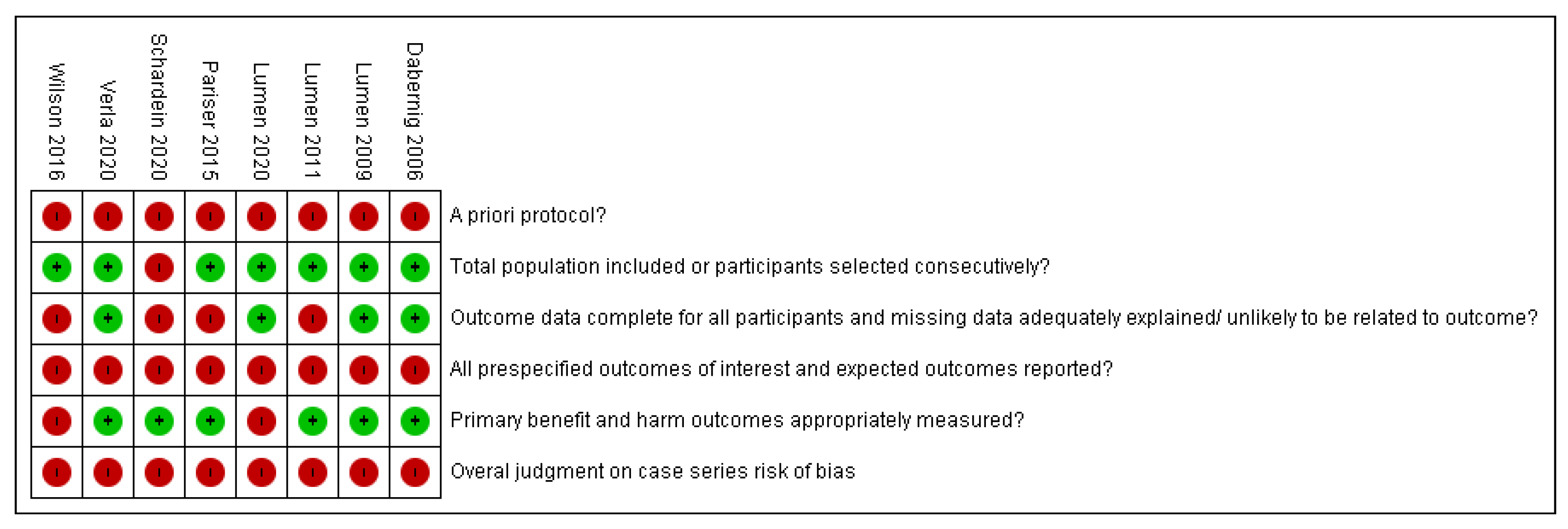
2.6. Assessment of Risk of Bias
- Was there an a priori protocol?
- Was the total population included or were study participants selected consecutively?
- Was outcome data complete for all participants and any missing data adequately explained/unlikely to be related to the outcome?
- Were all pre-specified outcomes of interest and expected outcomes reported?
- Were primary benefit and harm outcomes appropriately measured?
2.7. Data Analysis
3. Results
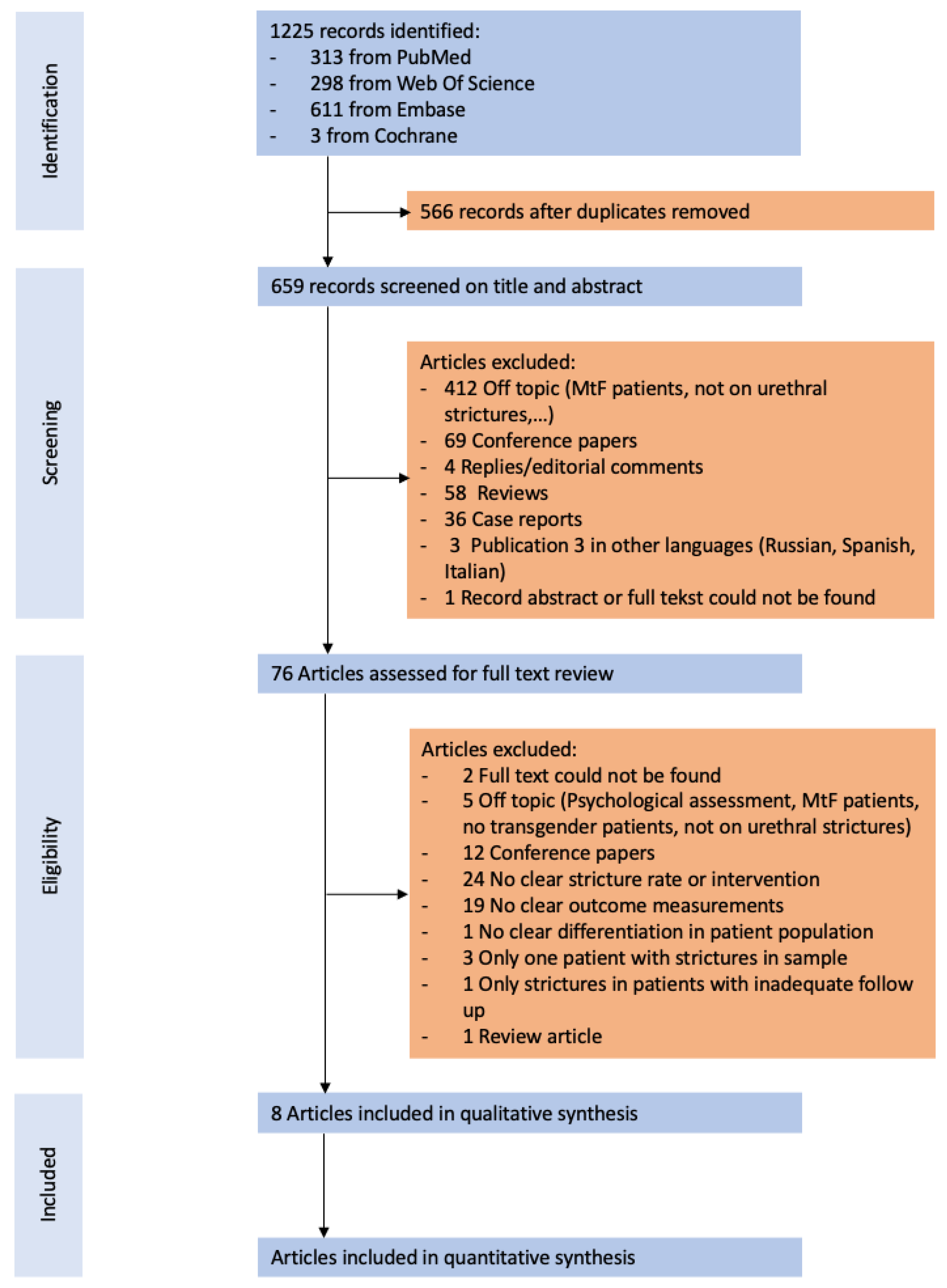
3.1. Quantity of Evidence Identified
3.2. Characteristics of Included Studies
3.3. Patterns of Strictures after GGAS
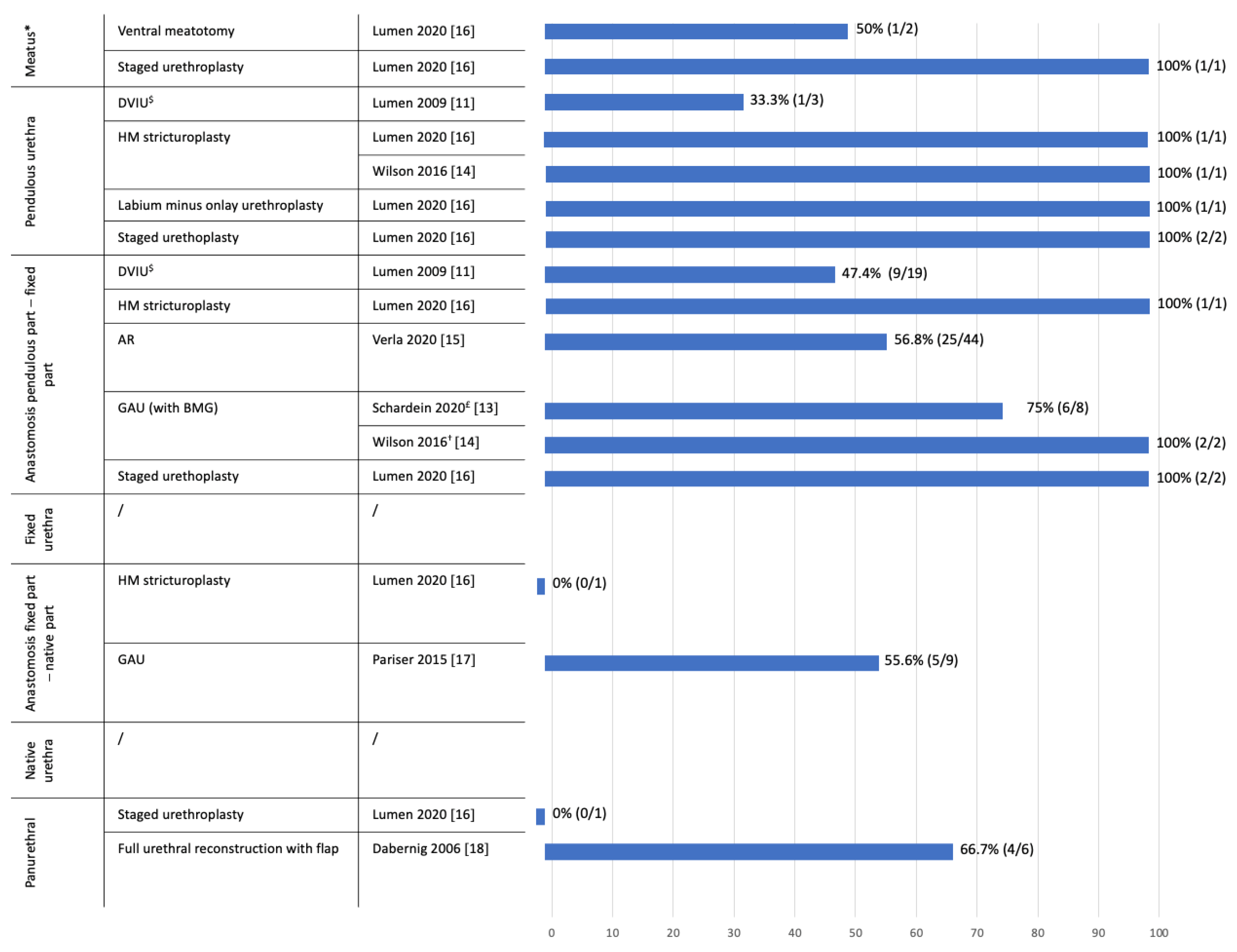
3.4. Patency Rates of Different Techniques
3.4.1. Minimally Invasive Procedures
3.4.2. Urethroplasty
Graft Augmented Urethroplasty (GAU)
Pedicled and Free Flaps
Anastomotic Repairs (AR)
Staged Repairs
3.5. Postoperative Complications
3.6. PROMs and Satisfaction
3.7. Risk of Bias Assessment
4. Discussion
4.1. Study Findings
4.2. Risk of Bias
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| GGAS | Genital gender affirming surgery |
| DVIU | Direct vision internal urethrotomy |
| RFFF | Radial forearm free flap |
| ALT | Anterolateral thigh |
| SCIAP | Superficial circumflex iliac artery perforator |
| AF | Abdominal flap |
| QoL | Quality of Life |
| PROM | Patient reported outcome measure |
| HMS | Heineke Miculicz stricturoplasty |
| BMG | Buccal mucosal graft |
| GAU | Graft augmented urethroplasty |
| FAU | Flap augmented urethroplasty |
| AR | Anastomotic repair |
| EPA | Excision and primary anastomosis |
| RCT | Randomized controlled trial |
| PU | Perineal urethrotomy |
| SU | Scrotal urethrotomy |
References
- Djordjevic, M.L.; Stojanovic, B.; Bizic, M. Metoidioplasty: Techniques and outcomes. Transl. Androl. Urol. 2019, 8, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Morrison, S.D.; Shakir, A.; Vyas, K.S.; Kirby, J.; Crane, C.N.; Lee, G.K. Phalloplasty: A Review of Techniques and Outcomes. Plast. Reconstr. Surg. 2016, 138, 594–615. [Google Scholar] [CrossRef] [PubMed]
- van de Grift, T.C.; Pigot, G.L.S.; Boudhan, S.; Elfering, L.; Kreukels, B.P.C.; Gijs, L.A.C.L.; Buncamper, M.E.; Özer, M.; van der Sluis, W.; Meuleman, E.J.H.; et al. A Longitudinal Study of Motivations Before and Psychosexual Outcomes after Genital Gender-Confirming Surgery in Transmen. J. Sex. Med. 2017, 14, 1621–1628. [Google Scholar] [CrossRef] [PubMed]
- Nassiri, N.; Maas, M.; Basin, M.; Cacciamani, G.E.; Doumanian, L.R. Urethral complications after gender reassignment surgery: A systematic review. Int. J. Impot. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Wessells, H.; Angermeier, K.W.; Elliott, S.; Gonzalez, C.M.; Kodama, R.; Peterson, A.C.; Reston, J.; Rourke, K.; Stoffel, J.T.; Vanni, A.J.; et al. Male Urethral Stricture: American Urological Association Guideline. J. Urol. 2017, 197, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Lumen, N.; Campos-Juanatey, F.; Dimitropoulos, K.; Greenwell, T.; Martins, F.; Osman, N.; Riechardt, S.; Waterloos, M. EAU Guidelines on Urethral Strictures; EAU: Arnhem, The Netherlands, 2021; ISBN 978-94-92671-13-4. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, M.; Ansari, M.; Berkman, N.; Chang, S.; Hartling, L.; McPheeters, L.; Santaguida, P.; Shamliyan; Singh, K.; Tsertsvadze, A.; et al. Assessing the Risk of Bias of Individual Studies in Systematic Reviews of Health Care Interventions. In Methods Guide for Effectiveness and Comparative Effectiveness Reviews; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2008. [Google Scholar]
- Dalziel, K.; Round, A.; Stein, K.; Garside, R.; Castelnuovo, E.; Payne, L. Do the findings of case series studies vary significantly according to methodological characteristics? Health Technol. Assess. 2005, 9, 1–146. [Google Scholar] [CrossRef] [PubMed]
- Marconi, L.; Maclennan, S.; Omar, M.I.; Yuan, C.; Canfield, S.; Plass, K.; N’Dow, J.; Sylvester, R. EAU Guidelines Systematic Reviews Methods and Processes Handbook; EAU: Arnhem, The Netherlands, 2019. [Google Scholar]
- Lumen, N.; Oosterlinck, W.; Decaestecker, K.; Monstrey, S.; Hoebeke, P. Endoscopic incision of short (<3 cm) urethral strictures after phallic reconstruction. J. Endourol. 2009, 23, 1329–1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lumen, N.; Monstrey, S.; Goessaert, A.-S.; Oosterlinck, W.; Hoebeke, P. Urethroplasty for strictures after phallic reconstruction: A single-institution experience. Eur. Urol. 2011, 60, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Schardein, J.; Beamer, M.; Nikolavsky, D. Double-face buccal mucosal graft urethroplasty for neophallus anastomotic strictures. J. Urol. 2020, 203, e644. [Google Scholar]
- Wilson, S.C.; Stranix, J.T.; Khurana, K.; Morrison, S.D.; Levine, J.P.; Zhao, L.C. Fasciocutaneous flap reinforcement of ventral onlay buccal mucosa grafts enables neophallus revision urethroplasty. Ther. Adv. Urol. 2016, 8, 331–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verla, W.; Hoebeke, P.; Spinoit, A.-F.; Waterloos, M.; Monstrey, S.; Lumen, N. Excision and Primary Anastomosis for Isolated, Short, Anastomotic Strictures in Transmen. Plast. Reconstr. Surgery. Glob. Open 2020, 8, e2641. [Google Scholar] [CrossRef] [PubMed]
- Lumen, N.; Waterschoot, M.; Verla, W.; Hoebeke, P. Surgical repair of urethral complications after metoidioplasty for genital gender affirming surgery. Int. J. Impot. Res. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Pariser, J.J.; Cohn, J.A.; Gottlieb, L.J.; Bales, G.T. Buccal mucosal graft urethroplasty for the treatment of urethral stricture in the neophallus. Urology 2015, 85, 927–931. [Google Scholar] [CrossRef] [PubMed]
- Dabernig, J.; Shelley, O.P.; Cuccia, G.; Schaff, J. Urethral Reconstruction Using the Radial Forearm Free Flap: Experience in Oncologic Cases and Gender Reassignment. Eur. Urol. 2007, 52, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Waterschoot, M.; Hoebeke, P.; Spinoit, A.-F.; Monstrey, S.; Buncamper, M.; Roth, J.; Verla, W.; Waterloos, M.; Lumen, N. Metoidioplasty followed by secondary phalloplasty: The way to fewer complications? J. Urol. 2020, 203, e437. [Google Scholar] [CrossRef]
- Lumen, N.; Campos-Juanatey, F.; Greenwell, T.; Martins, F.E.; Osman, N.I.; Riechardt, S.; Waterloos, M.; Barratt, R.; Chan, G.; Esperto, F.; et al. European Association of Urology Guidelines on Urethral Stricture Disease (Part 1): Management of Male Urethral Stricture Disease. Eur. Urol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Santucci, R.A. Urethral Complications After Transgender Phalloplasty: Strategies to Treat Them and Minimize Their Occurrence. Clin. Anat. 2018, 31, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Granieri, M.A.; Webster, G.D.; Peterson, A.C. Critical Analysis of Patient-reported Complaints and Complications after Urethroplasty for Bulbar Urethral Stricture Disease. Urology 2015, 85, 1489–1493. [Google Scholar] [CrossRef] [PubMed]
- Verla, W.; Van Nieuwenhuyse, F.; Hoebeke, P.; Oosterlinck, W.; Sinatti, C.; Spinoit, A.-F.; Waterloos, M.; Waterschoot, M.; Lumen, N. Urethroplasty for Failed Hypospadias Repair Related Strictures in Adults: A Retrospective Analysis with Long-term Follow-up. Urology 2020, 143, 248–254. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Year | Author | Type of Study | Follow-Up Nature | Funding | Study Participants | Date of Recuitment | Type of Gender Affirming Surgery | If Phalloplasty, Type of Urethral Lengthening | If Metoidioplasty, Type of Urethral Lenghthening | Mean/Median Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|
| 2020 | Lumen [16] | Case series | Retrospective | None | 12/13 (92%) 1 stricture left conservative, 12/12 (100%) FtM | January 2006–March 2020 | 12/12 (100%) Metoidioplasty | NA | NR | 15 (IQR: 10–42) |
| 2020 | Verla [15] | Case series | Prospective | None | 44/44 (100%) FtM | January 2002–October 2019 | 44/44 (100%) Phalloplasty | 33/44 (75%) RFFF tube in tube, 5/44 (11%) ALT tube in tube, 5/44 (11%) Pedicled SCIAP flap, 1/44 (2.3%) Other (not specified) | NA | 40 (IQR: 7–125) |
| 2020 | Schardein [13] | Case series | Retrospective | None | 9/9 (100%) FtM | December 2014–December 2019 | 9/9 (100%) Phalloplasty | 9/9 (100%) RFFF tube in tube | NA | 31 (range: 10–56) |
| 2016 | Wilson [14] | Case series | Retrospective | None | Mixed group(2/3–66.6% FtM) (1/3–33.3% oncologic penectomy) | May 2011–August 2015 | 2/2 (100%) Phalloplasty | 2/2 (100%) RFFF tube in tube + Partially prelaminated with buccal mucosa | NA | 8.7 (range: 6–13) |
| 2015 | Pariser [17] | Case series | Retrospective | None | Mixed group (9/10–90% FtM, 1/10–10% traumatic penile loss) | March 1998–June 2013 | 8/9 (88.9%) Phalloplasty, 1/9 (11.1%) Metoidioplasty | 8/8 (100%) RFFF tube in tube | NR | 9.5(range: 2.7-84) |
| 2011 | Lumen [12] | Case series | Retrospective | None | Mixed group (76/79–96.2% FtM, 3/79–3.8% penile insufficiency) | Aril 1994–May 2010 | 76/76 (100%) Phalloplasty | 73/79 (92.4%) RFFF tube in tube, 6/79 (7.6%) UNCLEAR | NA | 39 (range: 2–195) |
| 2009 | Lumen [11] | Case series | Retrospective | None | Mixed group (21/22–95.4% FtM, 1/22–4.5% traumatic penile loss) | September 2000–December 2008 | 21/21 (100%) Phalloplasty | 20/22 (90.9%) RFFF tube in tube, 2/22 (9.1%) ALT tube in tube | NA | 51 (range: 8–95) |
| 2006 | Dabernig [18] | Case series | Retrospective | None | Mixed group (6/9–66,7% FtM, 3/9–33.3% oncologic penectomy) | 1999–2004 | 6/6 (100%) Phalloplasty | 3/6 (50%) SCIP, 3/6 (50%) Abdominal | NA | 41.8 (range: 13–55) |
| Author and Year | Mean/Median Age at Urethral Procedure (Months) | Stricture Time to Onset (Months) | Stricture Localization | Previous Endoscopic Procedures | Previous Meatotomy/Meatoplasty | Previous Urethroplasty | Urethrotomy (Otis/DVIU/Meatotomy/HM Stricturoplasty) | Augmented Urethroplasty with Graft | Augmented Urethroplasty with Local Flap | Primary Anastomotic Repair | Staged Urethroplasty with or without Augmentation | Definitive Preineal/Scrotal Urethrostomy | Perioperative Complications (Clavien Dindo) | Stricture Recurrence | Postoperative Complications |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lumen et al. 2020 [16] | 30 (IQR:24–40) | 9 (IQR: 12–17) | 1/12 (8.3%) Anastomosis Native–Pars fixa, 4/12 (33.3%) Anastomosis Pars fixa–Pars pendulans, 4/12 (33.3%) Pars pendulans, 3/12 (24.9%) Meatal, 1/12 (8.3%) Panurethral | None | None | None | 2/12 (17%) Meatotomy, 3/12 (25%) HM | None | 1/12 (8.3%) Labium Minus flap (pan-urethral stricture) | None | 6/12 (50%) | None | No CD ≥3, Lower grades not reported | 1/3 (33.3%) after HM, 1/2 (50%) after meatotomy, 2/6 (33.3%) after staged repair, 0/1 (0%) after local flap repair | No Clavien Dindo complications ≥ 3, Lower NR |
| Verla et al. 2020 [15] | 31 (IQR: 23–40) | 10 (IQR: 6–22) | 44/44 (100%) Anastomosis Pars fixa–Pars pendulans | 11/44 (25%) | None | 17/44 (39%) | None | None | None | 44/44 (100%) EPA | None | None | 11% CD 1, 14% CD2, 2.3% CD3 (Placement of suprapubic catheter) | 19/44 (43%) After EPA repair | 11% of patients CD I, 14% of patients CD II, 2.3% of patients CD III (placement of SPC) (3/44 (6.8%) UTI, 3/44 (6.8%) Wound infection, 2/44 (4.5%) Hematoma, 4/44 (9.1%) Retention, 5/44 (11%) Fistula) |
| Schardein et al. 2020 [13] | 37 (range: 28–59) | NR | 9/9 (100%) Anastomosis Pars fixa–Pars pendulans | NR | NR | NR | None | 9/9 (100%) Double faced BMG | None | None | None | None | NR | 2/8 (25%) after BMG repair, 1 case no information on follow-up | NR |
| Wilson 2016 [14] | 32 Yo, 47 Yo | NR | 2/4 (50%) Anastomosis Pars fixa–Pars pendulans, 1/4 (25%) Pars pendulans, 1/4 (25%) Meatal | NR | None | None | 1/4 (25%) HM, 1/4 (25%) intervention not reported | 2/4 (50%) BMG, both reinforced with fasciocuteaneous flap | None | None | None | None | NR | 0/2 (0%) after BMG with flap, 0/1 (0%) after HM, 1 case no information on intervention or outcome | NR |
| Pariser 2015 [17] | 39 (range: 26–56) Including cis gender patiënt | NR | 9/9 (100%) Anastomosis Native–Pars fixa | 9/9 100% | None | 2/9 (22.2%) | None | 1/9 (11.1%) Excision with dorsal anastomosis with ventral onlay BMG; 8/9 (88.9%) Incision with ventral onlay BMG | None | None | None | None | 1/9 of patients CD1 (11.1%) | 4/9 (44.4%) after BMG | 1/9 of patients CD1 (11.1%) Mild rhabdomyolysis |
| Lumen 2011 [12] | 37.6 (range: 19–65) Including cis gender patients | Overall median 23.5 (range: 13.5-31.2) 24.4 (meatal), 35.3 (pars pendulans), 13.5 (anastomosis pars pendulans - pars fixa), 28.1 (pars fixa) | 18/118 (15.3%) Meatal, 28/118 (23.7%) Pars pendulans, 48/118 (40.7%) Anastomosis Pars fixa–Pars pendulans, 15/118 (12.7%) Pars fixa, 9/118 (7.6%) Multifocal | NR | NR | NR | 8/118 (6.8%) Meatotomy, 19/118 (16.1%) HM | 2/118 (1.7%) Free graft (type not reported) | 10/118 (8.5%) Pedicled flap urethroplasty (3/10 were neo-scrotal pedicled flaps, 7/10 were neophallic skin flaps) | 14/118 (11.9%) EPA | 33/118 (28.0%) Johanson staged urethroplasty, 21/118 (17.8%) Perineostomy followed by urethral reconstruction, 10/118 (8.5%) Still at first stage of stage urethroplasty or perineal urethrostomy and awaiting further treatment | 1/118 (0.8%) | NR | 2/8 (25%) after meatotomy, 8/19 (42.1%) after HM, 6/14 (42.9%) after EPA, 1/2 (50%) after free graft, 4/10 (40%) after pedicled flap, 10/33 (30.3%) after staged repair, 13/21 (61.9%) after perineostomy with urethral reconstruction | NR |
| Lumen 2009 [11] | 33 (range: 20–52) Including cis gender patients | 20 (range: 1–90) | 19/22 (86.4%) Anastomosis pars pendulans–Pars fixa 3/22 (13.6%) Pars pendulans | None | None | 8/22 (36.4%) | 32/32 (100%) DVIU (total of 32 procedures), (15/22 had 1 incision, 6/22 had 2 incisions, 1/22 had repetitive incisions) including cisgender patient | None | None | None | None | None | NR | 12/22 (56.2%) after 1 DVIU | NR |
| Dabernig 2006 [18] | 35.1 (range: 22–55) Including cis gender patients | NR | 6/6 (100%) Pan-urethral | Yes, but percentage not reported | NR | Yes, but percentages not reported | None | None | 6/6 (100%) Complete urethral reconstruction using RFFF | None | None | None | None | 2/6 (33.3%) after complete free flap reconstruction | None |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waterschoot, M.; Claeys, W.; Hoebeke, P.; Verla, W.; Waterloos, M.; Wirtz, M.; Buncamper, M.; Lumen, N. Treatment of Urethral Strictures in Transmasculine Patients. J. Clin. Med. 2021, 10, 3912. https://doi.org/10.3390/jcm10173912
Waterschoot M, Claeys W, Hoebeke P, Verla W, Waterloos M, Wirtz M, Buncamper M, Lumen N. Treatment of Urethral Strictures in Transmasculine Patients. Journal of Clinical Medicine. 2021; 10(17):3912. https://doi.org/10.3390/jcm10173912
Chicago/Turabian StyleWaterschoot, Mieke, Wietse Claeys, Piet Hoebeke, Wesley Verla, Marjan Waterloos, Michel Wirtz, Marlon Buncamper, and Nicolaas Lumen. 2021. "Treatment of Urethral Strictures in Transmasculine Patients" Journal of Clinical Medicine 10, no. 17: 3912. https://doi.org/10.3390/jcm10173912
APA StyleWaterschoot, M., Claeys, W., Hoebeke, P., Verla, W., Waterloos, M., Wirtz, M., Buncamper, M., & Lumen, N. (2021). Treatment of Urethral Strictures in Transmasculine Patients. Journal of Clinical Medicine, 10(17), 3912. https://doi.org/10.3390/jcm10173912