
Serum Amphiregulin and Heparin-Binding Epidermal Growth Factor as Biomarkers in Patients with Idiopathic Inflammatory Myopathy

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Healthy Controls
2.2. Measurement of Serum AREG and HB-EGF Levels
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
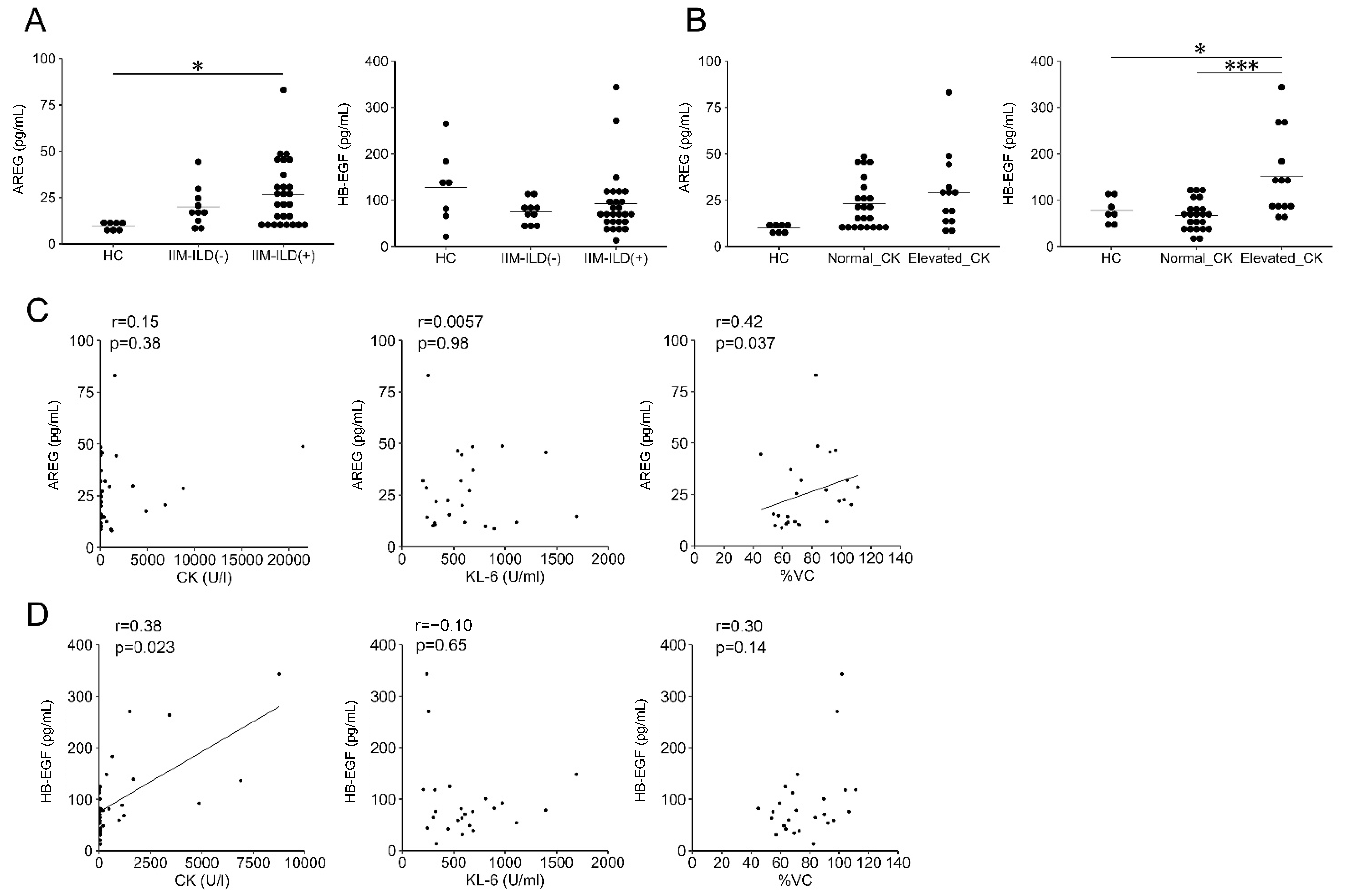
3.2. Elevated Serum AREG Levels in Patients with IIM-Related ILD
3.3. Correlation of Serum HB-EGF Levels with Elevated CK
3.4. Relationship between AREG and HB-EGF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dalakas, M.C. Inflammatory muscle diseases. N. Engl. J. Med. 2015, 30, 1734–1747. [Google Scholar] [CrossRef] [Green Version]
- Vencovsky, J.; Alexanderson, H.; Lundberg, I.E. Idiopathic inflammatory myopathy. Rheum. Dis. Clin. N. Am. 2019, 45, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Feria, A.S.; Albrecht, I.; Fernandes-Cerqueira, C.; Notarnicola, A.; James, E.A.; Herrath, J.; Dastmalchi, M.; Sandalova, T.; Rönnblom, L.; Jakobsson, P.J. Proinflammatory histidyl-tranfer RNA synthetase-specific CD4+ T cells in the blood and lungs of patients with idiopathic inflammatory myopathies. Arthritis Rheumatol. 2020, 72, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Enomoto, Y.; Suzuki, Y.; Hozumi, H.; Mori, K.; Kono, M.; Karayama, M.; Furuhashi, K.; Fujisawa, T.; Enomoto, N.; Nakamura, Y.; et al. Clinical significance of soluble CD163 in polymyositis-related or dermatomyositis-related interstitial lung disease. Arthritis Res. Ther. 2017, 19, 9. [Google Scholar] [CrossRef] [Green Version]
- Berasain, C.; Avila, M.A. Amphiregulin. Semin. Cell Dev. Biol. 2014, 28, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Dao, D.T.; Anez-Bustillos, L.; Adam, R.M.; Puder, M.; Bielenberg, D.R. Heparin-binding epidermal growth factor-like growth factor as a critical mediator of tissue repair and regeneration. Am. J. Pathol. 2018, 188, 2446–2456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaiss, D.M.W.; Gause, W.C.; Osborne, L.C.; Artis, D. Emerging functions of amphiregulin in orchestrating immunity, inflammation, and tissue repair. Immunity 2015, 42, 216–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minutti, C.M.; Modak, R.V.; Macdonald, F.; Li, F.; Smyth, D.J.; Dorward, D.A.; Blair, N.; Husovsky, C.; Muir, A.; Giampazolias, E.; et al. A macrophage-pericyte axis directs tissue restoration via amphiregulin-induced transforming growth factor beta activation. Immunity 2019, 50, 645–654.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Lee, J.Y.; Lee, C.M.; Cho, W.K.; Kang, M.J.; Koff, J.L.; Koff, J.L.; Yoon, P.O.; Chae, J.; Park, H.O.; et al. Amphiregulin, an epidermal growth factor receptor ligand, plays an essential role in the pathogenesis of transforming growth factor-β-induced pulmonary fibrosis. J. Biol. Chem. 2012, 287, 41991–42000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riese, D.J.; Stern, D.F. Specificity within the egf family/erbb receptor family signaling network. Bioessays 1998, 20, 41–48. [Google Scholar] [CrossRef]
- Satoh, K.; Kikuchi, S.; Sekimata, M.; Kabuyama, Y.; Homma, M.K.; Homma, Y. Involvement of erbb-2 in rheumatoid synovial cell growth. Arthritis Rheum. 2001, 44, 260–265. [Google Scholar] [CrossRef]
- Ishii, T.; Onda, H.; Tanigawa, A.; Ohshima, S.; Fujiwara, H.; Mima, T.; Katada, Y.; Deguchi, H.; Suemura, M.; Miyake, T.; et al. Isolation and expression profiling of genes upregulated in the peripheral blood cells of systemic lupus erythematosus patients. DNA Res. 2005, 12, 429–439. [Google Scholar] [CrossRef] [Green Version]
- Sisto, M.; Lisi, S.; Lofrumento, D.D.; Ingravallo, G.; Mitolo, V.; D’Amore, M. Expression of pro-inflammatory tace-tnf-α-amphiregulin axis in sjögren’s syndrome salivary glands. Histochem. Cell Biol. 2010, 134, 345–353. [Google Scholar] [CrossRef]
- Bhagavathula, N.; Nerusu, K.C.; Fisher, G.J.; Liu, G.; Thakur, A.B.; Gemmell, L.; Kumar, S.; Xu, Z.H.; Hinton, P.; Tsurushita, N.; et al. Amphiregulin and epidermal hyperplasia: Amphiregulin is required to maintain the psoriatic phenotype of human skin grafts on severe combined immunodeficient mice. Am. J. Pathol. 2005, 166, 1009–1016. [Google Scholar] [CrossRef]
- Wen, H.J.; Gao, S.; Wang, Y.; Ray, M.; Magnuson, M.A.; Wright, C.V.E.; Di Magliano, M.P.; Frankel, T.L.; Crawford, H.C. Myeloid cell-derived hb-egf drives tissue recovery after pancreatitis. Cell Mol. Gastroenterol. Hepatol. 2019, 8, 173–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, F.; Wei, K.; Slowikowski, K.; Fonseka, C.Y.; Rao, D.A.; Kelly, S.; Goodman, S.M.; Tabechian, D.; Hughes, L.B.; Salomon-Escoto, K.; et al. Defining inflammatory cell states in rheumatoid arthritis joint synovial tissues by integrating single-cell transcriptomics and mass cytometry. Nat. Immunol. 2019, 20, 928–942. [Google Scholar] [CrossRef] [PubMed]
- Kuo, D.; Ding, J.; Cohn, I.S.; Zhang, F.; Wei, K.; Rao, D.A.; Rozo, C.; Sokhi, U.K.; Shanaj, S.; Oliver, D.J.; et al. Hbegf+ macrophages in rheumatoid arthritis induce fibroblast invasiveness. Sci. Transl. Med. 2019, 11, eaau8587. [Google Scholar] [CrossRef] [PubMed]
- Bollée, G.; Flamant, M.; Schordan, S.; Fligny, C.; Rumpel, E.; Milon, M.; Schordan, E.; Sabaa, N.; Vandermeersch, S.; Galaup, A.; et al. Epidermal growth factor receptor promotes glomerular injury and renal failure in rapidly progressive crescentic glomerulonephritis. Nat. Med. 2011, 17, 1242–1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qing, X.; Chinenov, Y.; Redecha, P.; Madaio, M.; Roelofs, J.J.; Farber, G.; Issuree, P.D.; Donlin, L.; Mcllwain, D.R.; Mak, T.W.; et al. Irhom2 promotes lupus nephritis through tnf-α and egfr signaling. J. Clin. Investig. 2018, 128, 1397–1412. [Google Scholar] [CrossRef]
- Hirabayashi, M.; Asano, Y.; Yamashita, T.; Miura, S.; Nakamura, K.; Taniguchi, T.; Saigusa, R.; Takahashi, T.; Ichimura, Y.; Miyagawa, T.; et al. Possible pro-inflammatory role of heparin-binding epidermal growth factor-like growth factor in the active phase of systemic sclerosis. J. Dermatol. 2018, 45, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Burzyn, D.; Kuswanto, W.; Kolodin, D.; Shadrach, J.L.; Cerletti, M.; Jang, Y.; Sefik, E.; Tan, T.G.; Wagers, A.J.; Benoist, C.; et al. A special population of regulatory t cells potentiates muscle repair. Cell 2013, 155, 1282–1295. [Google Scholar] [CrossRef] [Green Version]
- Cramer, M.L.; Xu, R.; Martin, P.T. Soluble heparin binding epidermal growth factor-like growth factor is a regulator of galgt2 expression and galgt2-dependent muscle and neuromuscular phenotypes. Mol. Cell Biol. 2019, 39, e00140-19. [Google Scholar] [CrossRef] [Green Version]
- Bohan, A.; Peter, J.B. Polymyositis and dermatomyositis (first of two parts). N. Engl. J. Med. 1975, 292, 344–347. [Google Scholar] [CrossRef]
- Lundberg, I.E.; Tjärnlund, A.; Bottai, M.; Werth, V.P.; Pilkington, C.; Visser, M.; Alfredsson, L.; Amato, A.A.; Barohn, R.J.; Liang, M.H.; et al. 2017 european league against rheumatism/american college of rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups. Ann. Rheum. Dis. 2017, 76, 1955–1964. [Google Scholar] [CrossRef] [PubMed]
- van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A., Jr.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An american college of rheumatology/european league against rheumatism collaborative initiative. Ann. Rheum. Dis. 2013, 72, 1747–1755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 rheumatoid arthritis classification criteria: An american college of rheumatology/european league against rheumatism collaborative initiative. Ann. Rheum. Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, Y.; Hirahara, K.; Kiuchi, M.; Wada, T.; Ichikawa, T.; kanno, T.; Okano, M.; Kokubo, K.; Onodera, A.; Sakurai, D.; et al. Amphiregulin-producing pathogenic memory T helper 2 cells instruct eosinophils to secrete osteopontin and facilitate airway fibrosis. Immunity 2018, 49, 134–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, L.; Liu, T.; Wu, Z.; Hu, B.; Nakashima, T.; Ullenbruch, M.; De Los Santos, F.G.; Phan, S.H. Bone marrow cd11c+ cell-derived amphiregulin promotes pulmonary fibrosis. J. Immunol. 2016, 7, 303–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohno, N.; Kyoizumi, S.; Awaya, Y.; Fukuhara, H.; Yamakido, M.; Akiyama, M. New serum indicator of interstitial pneumonitis activity. Sialylated carbohydrate antigen KL-6. Chest 1989, 96, 68–73. [Google Scholar] [PubMed]
- Ishikawa, N.; Hattori, N.; Yokoyama, A.; Kohno, N. Utility of KL-6/MUC1 in the clinical management of interstitial lung diseases. Respir. Investig. 2012, 50, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arai, S.; Kurasawa, K.; Maezawa, R.; Owada, T.; Okada, H.; Fukuda, T. Marked increase in serum KL-6 and surfactant protein D levels during the first 4 weeks after treatment predicts poor prognosis in patients with active interstitial pneumonia associated with polymyositis/dermatomyositis. Mod. Rheumatol. 2013, 23, 872–883. [Google Scholar] [CrossRef] [PubMed]
- Fukatsu, Y.; Noguchi, T.; Hosooka, T.; Ogura, T.; Kotani, K.; Abe, T.; Shibakusa, T.; Inoue, K.; Sakai, M.; Tobimatsu, K.; et al. Muscle-specific overexpression of heparin-binding epidermal growth factor-like growth factor increases peripheral glucose disposal and insulin sensitivity. Endocrinology 2009, 150, 2683–2691. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| IIM (n = 37) | p-Value | SSc (n = 17) | p-Value | RA (n = 10) | p-Value | HC (n = 7) | |
|---|---|---|---|---|---|---|---|
| Female, n (%) | 26 (71.3) | 0.41 | 16 (94.1) | 0.52 | 8 (80) | 0.78 | 6 (85.7) |
| Age, years (range) | 59.0 (51.0–71.0) | 0.75 | 70.0 (55.0–75.0) | 0.13 | 69.0 (55.5–76.8) | 0.16 | 57 (56.5–60.0) |
| Disease duration, months (range) | 16 (7–84) | 60 (34–288) | 53 (14–177) | - | |||
| Untreated, n (%) | 14 (37.8) | 6 (35.3) | 0 (0) | - | |||
| ILD, n (%) | 27 (72.9) | 10 (58.8) | 3 (30) | - | |||
| CK, mean (S.D.), U/L | 1520 (3955) | n.d. | n.d. | n.d. | |||
| KL-6, U/mL (range) | 506 (289–687) | 533 (371–1144) | 271 (212–372) | n.d. | |||
| %VC, % (range) | 79.6 (65.1–96.8) | 76.7 (67.0–84.5) | 100.9 (77.5–132.6) | n.d. | |||
| %DLCO, % (range) | 74.7 (64.3–90.8) | 80.4 (71.0–93.1) | 82.4 (72.6–92.2) | n.d. | |||
| IIM (n = 37) | N (%) | SSc (n = 17) | N (%) | RA (n = 10) | N (%) | ||
| Autoantibody profile, n (%) | ARS | 14 (37.8) | Scl-70 | 6 (35.3) | RF | 9 (90) | |
| Jo-1 | 5 (13.5) | Centromere | 9 (52.9) | ACPA | 9 (90) | ||
| PL-7 | 3 (8.1) | RNA polymerase III | 2 (11.8) | ||||
| PL-12 | 1 (2.7) | ||||||
| EJ | 2 (5.4) | ||||||
| Unknown | 3 (8.1) | ||||||
| MDA-5 | 9 (24.3) | ||||||
| TIF-1γ | 1 (2.7) | ||||||
| Mi-2 | 3 (8.1) | ||||||
| SRP | 1 (2.7) | ||||||
| HMG-CR | 1 (2.7) | ||||||
| M2 | 2 (5.4) | ||||||
| Negative | 6 (16.2) | ||||||
| AREG | HB-EGF | |||||
|---|---|---|---|---|---|---|
| Normal (n = 30) | Elevated (n = 7) | p Value | Normal (n = 31) | Elevated (n = 6) | p Value | |
| Female, n (%) | 21 (70.0) | 5 (71.4) | 1.00 | 22 (71.0) | 4 (66.7) | 1.00 |
| Age, years (range) | 58 (50–68) | 71 (63–77) | 0.064 | 59 (51–71) | 61 (57–68) | 0.76 |
| Disease duration, month (range) | 21 (8–93) | 7 (1–18) | 0.001 | 16 (7–84) | 18 (9–41) | 0.79 |
| Untreated, n (%) | 11 (36.7) | 3 (42.9) | 1.00 | 11 (35.5) | 3 (50) | 0.65 |
| ILD, n (%) | 21 (70.0) | 5 (85.7) | 0.08 | 7 (22.6) | 3 (50) | 0.31 |
| CK, U/L | 69 (46–639) | 186 (42–1571) | 0.43 | 65 (73–192) | 2451 (850–6009) | 0.16 |
| Elevated CK, n (%) | 10 (34.5) | 3 (42.9) | 0.69 | 7 (23.3) | 6 (100) | <0.001 |
| KL-6, U/mL (range) | 453 (259–644) | 634 (550–900) | 0.27 | 557 (321–687) | 248 (231–617) | 0.93 |
| Elevated KL-6, n (%) | 9 (40.9) | 5 (83.3) | 0.16 | 13 (54.2) | 1 (25.0) | 0.60 |
| %VC, % (range) | 83 (68–102) | 71 (57–87) | 0.23 | 77 (64–90) | 100 (92–105) | 0.14 |
| %DLCO, % (range) | 76 (65–94) | 70 (57–78) | 0.24 | 74 (64–85) | 94 (85–99) | 0.16 |
| AREG, pg/mL (range) | 16.8 (11.6–25.2) | 46.5 (45.1–48.6) | <0.001 | 20.1 (11.7–31.9) | 24.6 (16.3–29.4) | 0.50 |
| HB-EGF, pg/mL (range) | 78.7 (49.5–116.6) | 78.4 (69.5–115.6) | 0.59 | 70.9 (50.8–90.6) | 223 (157–269) | 0.0055 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanata, N.; Nagafuchi, Y.; Sugimori, Y.; Kobayashi, S.; Tsuchida, Y.; Iwasaki, Y.; Shoda, H.; Fujio, K. Serum Amphiregulin and Heparin-Binding Epidermal Growth Factor as Biomarkers in Patients with Idiopathic Inflammatory Myopathy. J. Clin. Med. 2021, 10, 3730. https://doi.org/10.3390/jcm10163730
Hanata N, Nagafuchi Y, Sugimori Y, Kobayashi S, Tsuchida Y, Iwasaki Y, Shoda H, Fujio K. Serum Amphiregulin and Heparin-Binding Epidermal Growth Factor as Biomarkers in Patients with Idiopathic Inflammatory Myopathy. Journal of Clinical Medicine. 2021; 10(16):3730. https://doi.org/10.3390/jcm10163730
Chicago/Turabian StyleHanata, Norio, Yasuo Nagafuchi, Yusuke Sugimori, Satomi Kobayashi, Yumi Tsuchida, Yukiko Iwasaki, Hirofumi Shoda, and Keishi Fujio. 2021. "Serum Amphiregulin and Heparin-Binding Epidermal Growth Factor as Biomarkers in Patients with Idiopathic Inflammatory Myopathy" Journal of Clinical Medicine 10, no. 16: 3730. https://doi.org/10.3390/jcm10163730
APA StyleHanata, N., Nagafuchi, Y., Sugimori, Y., Kobayashi, S., Tsuchida, Y., Iwasaki, Y., Shoda, H., & Fujio, K. (2021). Serum Amphiregulin and Heparin-Binding Epidermal Growth Factor as Biomarkers in Patients with Idiopathic Inflammatory Myopathy. Journal of Clinical Medicine, 10(16), 3730. https://doi.org/10.3390/jcm10163730