
Statin Use Can Attenuate the Decline in Left Ventricular Ejection Fraction and the Incidence of Cardiomyopathy in Cardiotoxic Chemotherapy Recipients: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Inclusion Criteria
- (1)
- Randomized controlled trials (RCTs), case-control studies, cohort studies (prospective or retrospective), and cross-sectional studies that reported changes in LVEF, the pre- and post-chemotherapy LVEF, and/or the incidence of new-onset heart failure (HF) in patients who were and were not receiving the concurrent statin during chemotherapy;
- (2)
- Statistics such as odds ratio (OR), risk ratio (RR), hazard ratio (HR), or weighted mean difference (WMD) and its corresponding 95% confidence intervals (95% CI) and p-values or sufficient raw data for these calculations had to be provided.
2.3. Quality Assessment of the Included Studies
2.4. Definition of Chemotherapy-Induced Cardiotoxicity
2.5. Data Extraction
2.6. Statistical Analysis
3. Results
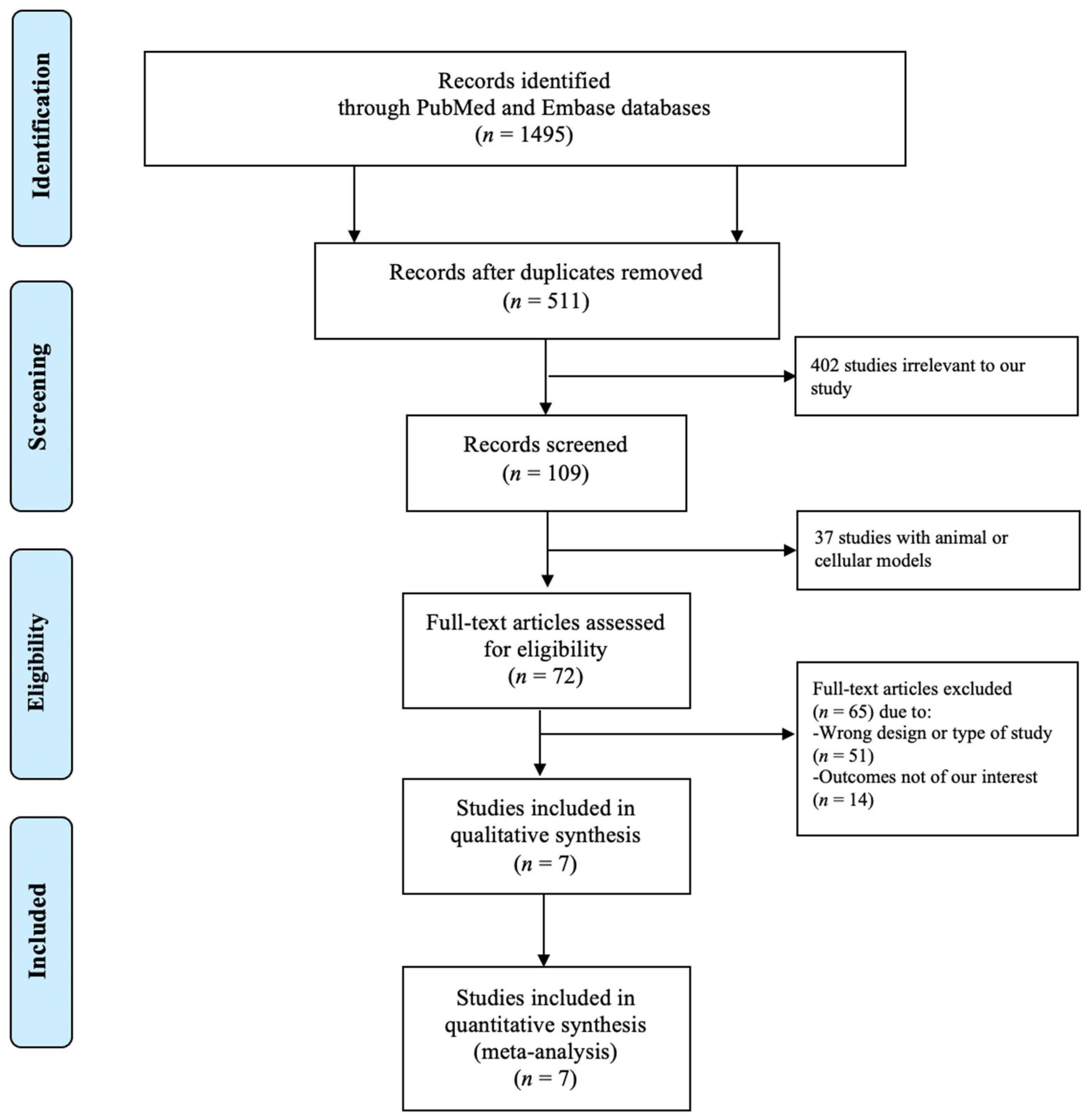
3.1. Study Search Results
3.2. Description of the Included Studies and Quality Assessment
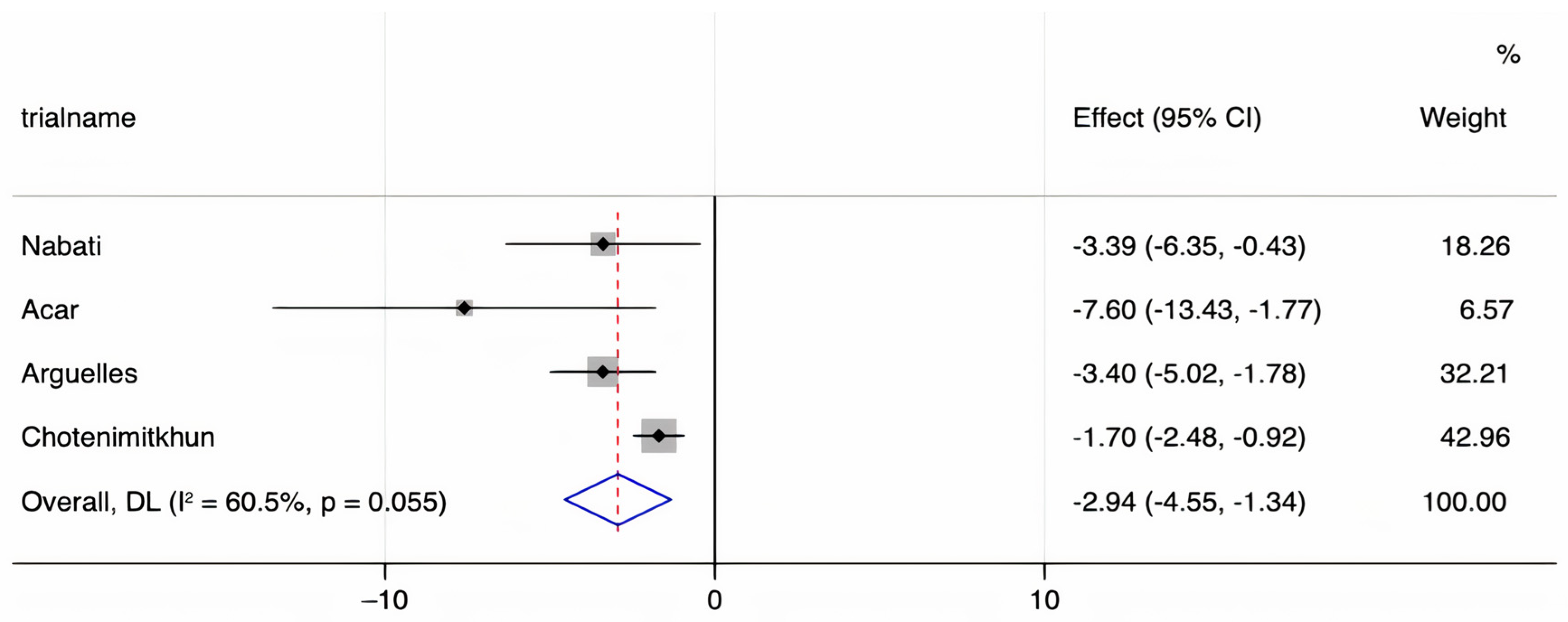
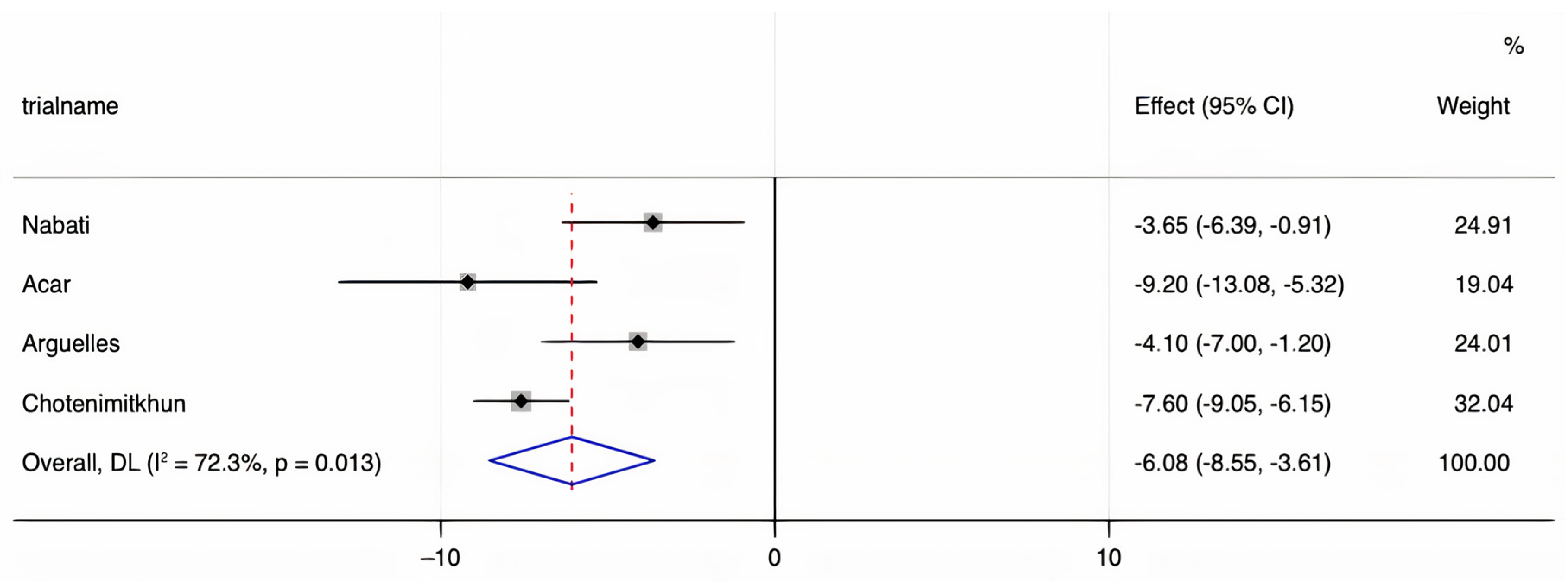
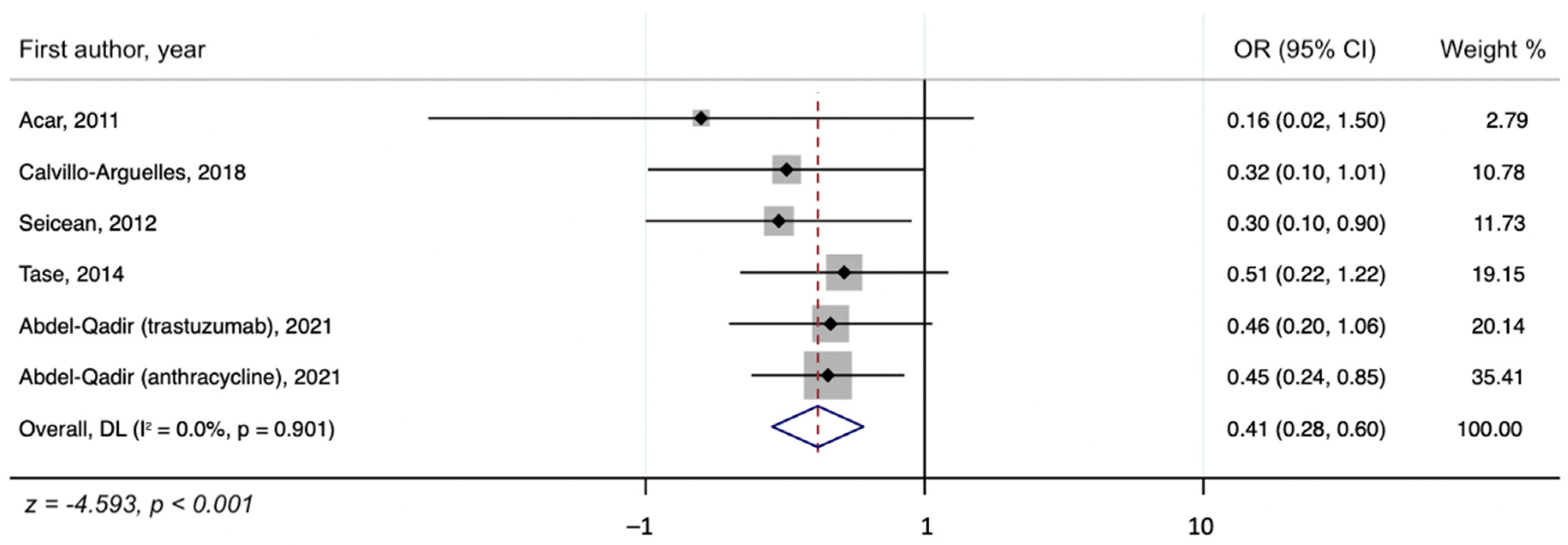
3.3. Quantitative Meta-Analysis Results
3.4. Publication Bias
3.5. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shih, Y.C.; Hurria, A. Preparing for an epidemic: Cancer care in an aging population. Am. Soc. Clin. Oncol. Educ. Book 2014, 34, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Pineros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, H.; Nishimura, Y.; Horiuchi, H.; Higashira, T.; Kita, Y.; Nishizawa, H. G20 Okayama Health Ministers’ Meeting: Lessons learned and way forward. Glob. Health Med. 2019, 1, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, H.; Nishimura, Y.; Matsumura, H.; Horiuchi, H.; Higashira, T.; Kita, Y.; Sahara, Y.; Suzuki, Y. G20 Okayama Health Ministers’ Meeting: Conclusions and commitments. J. Glob. Health 2020, 10, 010320. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.A.; Auseon, A.J. Chemotherapy-induced takotsubo cardiomyopathy. Heart Fail. Clin. 2013, 9, 233–242. [Google Scholar] [CrossRef]
- Goel, S.; Sharma, A.; Garg, A.; Chandra, A.; Shetty, V. Chemotherapy induced Takotsubo cardiomyopathy. World J. Clin. Cases 2014, 2, 565–568. [Google Scholar] [CrossRef]
- Coen, M.; Rigamonti, F.; Roth, A.; Koessler, T. Chemotherapy-induced Takotsubo cardiomyopathy, a case report and review of the literature. BMC Cancer 2017, 17, 394. [Google Scholar] [CrossRef]
- Shahzad, M.A.; Ishtiaq, R.; Zahid, U.; Anwer, F. Successful recovery and allogeneic stem cell transplant following chemotherapy-induced severe cardiomyopathy: Literature review of management and prognostic factors. BMJ Case Rep. 2016, 2016, bcr2016217210. [Google Scholar] [CrossRef]
- Balakrishnan, K.R.; Rao, K.G.S.; Subramaniam, G.; Sharma, D. Transplantation for chemotherapy-induced cardiomyopathy-case series and review of current practice. Indian J. Thorac Cardiovasc. Surg. 2020, 36, 287–293. [Google Scholar] [CrossRef]
- Inui, T.; Kohno, H.; Matsuura, K.; Ueda, H.; Tamura, Y.; Watanabe, M.; Inage, Y.; Yakita, Y.; Matsumiya, G. A case of left ventricular assist device application for chemotherapy-related cardiomyopathy caused by trastuzumab and anthracycline. J. Artif. Organs. 2020, 23, 270–274. [Google Scholar] [CrossRef]
- Gupta, D.; Chan, A.; Jordan, J.; Steingart, R.M. Chemotherapy-Induced Cardiomyopathy: Clinical Scenarios and Challenges. Oncology 2015, 29, 730–732, 786. [Google Scholar] [PubMed]
- Higgins, A.Y.; O’Halloran, T.D.; Chang, J.D. Chemotherapy-induced cardiomyopathy. Heart Fail. Rev. 2015, 20, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Piper, S.E.; McDonagh, T.A. Chemotherapy-related Cardiomyopathy. Eur. Cardiol. 2015, 10, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Adams, M.J.; Ganatra, S.; Colan, S.D.; Aggarwal, S.; Steiner, R.; Amdani, S.; Lipshultz, E.R.; Lipshultz, S.E. Strategies to prevent anthracycline-induced cardiotoxicity in cancer survivors. Cardiooncology 2019, 5, 18. [Google Scholar] [CrossRef] [PubMed]
- Payne, D.L.; Nohria, A. Prevention of Chemotherapy Induced Cardiomyopathy. Curr. Heart Fail. Rep. 2017, 14, 398–403. [Google Scholar] [CrossRef]
- Heck, S.L.; Mecinaj, A.; Ree, A.H.; Hoffmann, P.; Schulz-Menger, J.E.; Fagerland, M.W.; Gravdehaug, B.; Røsjø, H.; Steine, K.; Geisler, J.; et al. Prevention of Cardiac Dysfunction During Adjuvant Breast Cancer Therapy (PRADA) Extended Follow-Up of a 2 × 2 Factorial, Randomized, Placebo-Controlled, Double-Blind Clinical Trial of Candesartan and Metoprolol. Circulation 2021, 143, 2431–2440. [Google Scholar] [CrossRef]
- Abdel-Qadir, H.; Bobrowski, D.; Zhou, L.; Austin, P.C.; Calvillo-Argüelles, O.; Amir, E.; Lee, D.S.; Thavendiranathan, P. Statin Exposure and Risk of Heart Failure After Anthracycline- or Trastuzumab-Based Chemotherapy for Early Breast Cancer: A Propensity ScoreMatched Cohort Study. J. Am. Heart Assoc. 2021, 10, e018393. [Google Scholar] [CrossRef]
- Acar, Z.; Kale, A.; Turgut, M.; Demircan, S.; Durna, K.; Demir, S.; Meriç, M.; Ağaç, M.T. Efficiency of Atorvastatin in the Protection of Anthracycline-Induced Cardiomyopathy. J. Am. Coll. Cardiol. 2011, 58, 988–989. [Google Scholar] [CrossRef]
- Calvillo-Argüelles, O.; Abdel-Qadir, H.; Michalowska, M.; Billia, F.; Suntheralingam, S.; Amir, E.; Thavendiranathan, P. Cardioprotective Effect of Statins in Patients with HER2-Positive Breast Cancer Receiving Trastuzumab Therapy. Can. J. Cardiol. 2019, 35, 153–159. [Google Scholar] [CrossRef]
- Chotenimitkhun, R.; D’Agostino, R.; Lawrence, J.A.; Hamilton, C.A.; Jordan, J.H.; Vasu, S.; Lash, T.L.; Yeboah, J.; Herrington, D.M.; Hundley, W.G. Chronic Statin Administration May Attenuate Early Anthracycline-Associated Declines in Left V1ntricular Ejection Function. Can. J. Cardiol. 2015, 31, 302–307. [Google Scholar] [CrossRef]
- Nabati, M.; Janbabai, G.; Esmailian, J.; Yazdani, J. Effect of Rosuvastatin in Preventing Chemotherapy-Induced Cardiotoxicity in Women With Breast Cancer: A Randomized, Single-Blind, Placebo-Controlled Trial. J. Cardiovasc. Pharmacol. Ther. 2019, 24, 233–241. [Google Scholar] [CrossRef]
- Seicean, S.; Seicean, A.; Plana, J.C.; Budd, G.T.; Marwick, T.H. Effect of statin therapy on the risk for incident heart failure in patients with breast cancer receiving anthracycline chemotherapy: An observational clinical cohort study. J. Am. Coll. Cardiol. 2012, 60, 2384–2390. [Google Scholar] [CrossRef]
- Tase, A.; Titus Ovidiu, T.; Tase, A.; Savoiu, G.; Iorga-Siman, I.; Mihaila, M. Add-On therapy with hmg-coa-reductase inhibitors may lower the risk for incident left ventricular dysfunction +/− heart failure in epirubicin recipients with gastric cancer. J. Am. Coll. Cardiol. 2014, 63, A932. [Google Scholar] [CrossRef][Green Version]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Harbord, M. Funnel plots in meta-analysis. Stata J. 2004, 4, 127–141. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple graphical test. Br. Med. J. 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.J.; Ekert, H.; Waters, K.; Matthews, R.N. High incidence of cardiomyopathy in children treated with adriamycin and DTIC in combination chemotherapy. Cancer Treat. Rep. 1977, 61, 1736–1738. [Google Scholar]
- Granger, C.B. Prediction and prevention of chemotherapy-induced cardiomyopathy: Can it be done? Circulation 2006, 114, 2432–2433. [Google Scholar] [CrossRef] [PubMed]
- Saidi, A.; Alharethi, R. Management of chemotherapy induced cardiomyopathy. Curr. Cardiol. Rev. 2011, 7, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, Z.; Davaro, E.; Batanian, J.; Verma, N. First-dose idarubicin cardiomyopathy: A case of new heart failure after induction chemotherapy for acute myeloid leukaemia. BMJ Case Rep. 2019, 12, e228149. [Google Scholar] [CrossRef]
- Caner, M.; Sonmez, B.; Kurnaz, O.; Aldemir, C.; Salar, S.; Altug, T.; Bilir, A.; Altinoz, M.A. Atorvastatin has cardiac safety at intensive cholesterol-reducing protocols for long term, yet its cancer-treatment doses with chemotherapy may cause cardiomyopathy even under coenzyme-Q10 protection. Cell Biochem. Funct. 2007, 25, 463–472. [Google Scholar] [CrossRef]
- Cai, A.W.; Taylor, M.H.; Ramu, B. Treatment of chemotherapy-associated cardiomyopathy. Curr. Opin. Cardiol. 2019, 34, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.P.; Solomon, S.D.; Fradley, M.G.; Barac, A.; Kremer, K.A.; Beck, C.A.; Brown, M.W.; McNitt, S.; Schleede, S.; Zareba, W.; et al. Association of Cardiac Resynchronization Therapy with Change in Left Ventricular Ejection Fraction in Patients With Chemotherapy-Induced Cardiomyopathy. JAMA 2019, 322, 1799–1805. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.M.; Westerman, S.; Mandawat, A. Cardiac Resynchronization Therapy for Chemotherapy-Induced Cardiomyopathy. JAMA 2020, 323, 1316. [Google Scholar] [CrossRef] [PubMed]
- Ezzeddine, F.M.; Saliba, A.N.; Jain, V.; Villarraga, H.R.; Herrmann, J.; Asirvatham, S.J.; Cha, Y.M. Outcomes of cardiac resynchronization therapy in patients with chemotherapy-induced cardiomyopathy. Pacing Clin. Electrophysiol. 2021, 44, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Preventing Anthracycline Cardiovascular Toxicity with Statins (PREVENT) (ClinicalTrials.gov Website). Available online: https://clinicaltrials.gov/ct2/show/NCT01988571 (accessed on 20 May 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country | Published Year | Study Type | Number of Participants (n = 3042) | Mean or Median Age (Years) | Mean Follow-Up Durations (Months) | Cancer | Chemotherapy | Statin, n (n = 1382) |
|---|---|---|---|---|---|---|---|---|---|
| Acar | Turkey | 2011 | RCT | 40 | 53.0 ± 15.0 | 6 | NHL MM Leukemia | Anthracycline | Atorvastatin, 20 |
| Calvillo- Argüelles | Canada | 2018 | Case control | 129 | 62.0 ± 9.0 | 11 | Breast | Trastuzumab | Atorvastatin, 24 Rosuvastatin, 11 Simvastatin, 5 Pravastatin, 3 |
| Chotenimtkhun | U.S. | 2013 | Cohort | 51 | 48.0 ± 2.0 | 6 | Breast Leukemia Lymphoma | Anthracycline | Atorvastatin, 5 Simvastatin, 9 |
| Nabati | Iran | 2018 | RCT | 77 | 49.3 ± 11.2 | 6 | Breast | Anthracycline Trastuzumab | Rosuvastatin, 38 |
| Seicean | U.S. | 2012 | Cohort | 201 | 51.5 ± 10.8 | 31.2 | Breast | Anthracycline | N/A, 67 |
| Tase | Romania | 2014 | Cohort | 432 | 57.5 ± 11.2 | 30.6 | Gastric | Anthracycline | Rosuvastatin, 77 Atorvastatin, 52 Other, 15 |
| Abdel-Qadir | Canada | 2021 | Cohort | 2112 | 69.0 (IQR 67–72) * | 60 | Breast | Anthracycline Trastuzumab | Rosuvastatin, 491 Atorvastatin, 433 Simvastatin, 82 Pravastatin, 27 Other, 23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Nishimura, Y.; Kewcharoen, J.; Yess, J. Statin Use Can Attenuate the Decline in Left Ventricular Ejection Fraction and the Incidence of Cardiomyopathy in Cardiotoxic Chemotherapy Recipients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3731. https://doi.org/10.3390/jcm10163731
Kim J, Nishimura Y, Kewcharoen J, Yess J. Statin Use Can Attenuate the Decline in Left Ventricular Ejection Fraction and the Incidence of Cardiomyopathy in Cardiotoxic Chemotherapy Recipients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(16):3731. https://doi.org/10.3390/jcm10163731
Chicago/Turabian StyleKim, Jean, Yoshito Nishimura, Jakrin Kewcharoen, and James Yess. 2021. "Statin Use Can Attenuate the Decline in Left Ventricular Ejection Fraction and the Incidence of Cardiomyopathy in Cardiotoxic Chemotherapy Recipients: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 16: 3731. https://doi.org/10.3390/jcm10163731
APA StyleKim, J., Nishimura, Y., Kewcharoen, J., & Yess, J. (2021). Statin Use Can Attenuate the Decline in Left Ventricular Ejection Fraction and the Incidence of Cardiomyopathy in Cardiotoxic Chemotherapy Recipients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 10(16), 3731. https://doi.org/10.3390/jcm10163731