
Cytomegalovirus-Associated Autoantibody against TAF9 Protein in Patients with Systemic Lupus Erythematosus


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Antibody Purification
2.3. ELISA Assay
2.4. CMV IgG Avidity Testing
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berman, N.; Belmont, H.M. Disseminated cytomegalovirus infection complicating active treatment of systemic lupus erythematosus: An emerging problem. Lupus 2017, 26, 431–434. [Google Scholar] [CrossRef]
- Dioverti, M.V.; Razonable, R.R. Cytomegalovirus. Microbiol. Spectr. 2016, 4, 1–26. [Google Scholar] [CrossRef]
- Rozenblyum, E.V.; Levy, D.M.; Allen, U.; Harvey, E.; Hebert, D.; Silverman, E.D. Cytomegalovirus in pediatric systemic lupus erythematosus: Prevalence and clinical manifestations. Lupus 2015, 24, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Reis, A.D.; Mudinutti, C.; de Freitas Peigo, M.; Leon, L.L.; Bonon, S.H.A. Active human herpesvirus infections in adults with systemic lupus erythematosus and correlation with the SLEDAI score. Adv. Rheumatol. 2020, 60, 42. [Google Scholar] [CrossRef] [PubMed]
- Baboonian, C.; Venables, P.J.; Booth, J.; Williams, D.G.; Roffe, L.M.; Maini, R.N. Virus infection induces redistribution and membrane localization of the nuclear antigen La (SS-B): A possible mechanism for autoimmunity. Clin. Exp. Immunol. 1989, 78, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J. Cytomegalovirus infection induces expression of 60 KD/Ro antigen on human keratinocytes. Lupus 1995, 4, 396–406. [Google Scholar] [CrossRef] [PubMed]
- Newkirk, M.M.; van Venrooij, W.J.; Marshall, G.S. Autoimmune response to U1 small nuclear ribonucleoprotein (U1 snRNP) associated with cytomegalovirus infection. Arthritis Res. 2001, 3, 253–258. [Google Scholar] [CrossRef]
- Abate, D.A.; Watanabe, S.; Mocarski, E.S. Major human cytomegalovirus structural protein pp65 (ppUL83) prevents interferon response factor 3 activation in the interferon response. J. Virol. 2004, 78, 10995–11006. [Google Scholar] [CrossRef]
- Li, T.; Chen, J.; Cristea, I.M. Human cytomegalovirus tegument protein pUL83 inhibits IFI16-mediated DNA sensing for immune evasion. Cell Host Microbe 2013, 14, 591–599. [Google Scholar] [CrossRef]
- Chang, M.; Pan, M.R.; Chen, D.Y.; Lan, J.L. Human cytomegalovirus pp65 lower matrix protein: A humoral immunogen for systemic lupus erythematosus patients and autoantibody accelerator for NZB/W F1 mice. Clin. Exp. Immunol. 2006, 143, 167–179. [Google Scholar] [CrossRef]
- Hsieh, A.H.; Wang, C.M.; Wu, Y.J.; Chen, A.; Chang, M.I.; Chen, J.Y. B cell epitope of human cytomegalovirus phosphoprotein 65 (HCMV pp65) induced anti-dsDNA antibody in BALB/c mice. Arthritis Res. Ther. 2017, 19, 65. [Google Scholar] [CrossRef]
- Hsieh, A.H.; Jhou, Y.J.; Liang, C.T.; Chang, M.; Wang, S.L. Fragment of tegument protein pp65 of human cytomegalovirus induces autoantibodies in BALB/c mice. Arthritis Res. Ther. 2011, 13, R162. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, A.H.; Kuo, C.F.; Chou, I.J.; Tseng, W.Y.; Chen, Y.F.; Yu, K.H.; Luo, S.F. Human cytomegalovirus pp65 peptide-induced autoantibodies cross-reacts with TAF9 protein and induces lupus-like autoimmunity in BALB/c mice. Sci. Rep. 2020, 10, 9662. [Google Scholar] [CrossRef] [PubMed]
- Prince, H.E.; Lape-Nixon, M. Role of cytomegalovirus (CMV) IgG avidity testing in diagnosing primary CMV infection during pregnancy. Clin. Vaccine Immunol. 2014, 21, 1377–1384. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.H.; Chen, P.C.; Jeng, S.F.; Hsieh, C.J.; Hsieh, W.S. High perinatal seroprevalence of cytomegalovirus in northern Taiwan. J. Paediatr. Child. Health 2008, 44, 166–169. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.C.; Chin, L.T.; Wu, F.M.; Hsieh, G.J. Seroprevalence of CMV antibodies in a blood donor population and premature neonates in the south-central Taiwan. Kaohsiung J. Med. Sci. 1999, 15, 603–610. [Google Scholar] [PubMed]
- Heieren, M.H.; van der Woude, F.J.; Balfour, H.H., Jr. Cytomegalovirus replicates efficiently in human kidney mesangial cells. Proc. Natl. Acad. Sci. USA 1988, 85, 1642–1646. [Google Scholar] [CrossRef]
- Popik, W.; Correa, H.; Khatua, A.; Aronoff, D.M.; Alcendor, D.J. Mesangial cells, specialized renal pericytes and cytomegalovirus infectivity: Implications for HCMV pathology in the glomerular vascular unit and post-transplant renal disease. J. Transl. Sci. 2019, 5, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, T.; Stewart, J.A. Immune-complex glomerulonephritis associated with cytomegalovirus infection. Am. J. Clin. Pathol. 1979, 72, 103–107. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mo, H.Y.; Wei, J.C.C.; Chen, X.H.; Chen, H.H. Increased risk of systemic lupus erythematosus in patients with autoimmune haemolytic anaemia: A nationwide population-based cohort study. Ann. Rheum. Dis. 2020, 80, 403–404. [Google Scholar] [CrossRef]
- Butler, L.M.; Dzabic, M.; Bakker, F.; Davoudi, B.; Jeffery, H.; Religa, P.; Bojakowski, K.; Yaiw, K.C.; Rahbar, A.; Soderberg-Naucler, C. Human cytomegalovirus inhibits erythropoietin production. J. Am. Soc. Nephrol. 2014, 25, 1669–1678. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | SLE (n = 193) | SS (n = 70) | RA (n = 84) | Gout (n = 92) | AS (n = 68) | p Value |
|---|---|---|---|---|---|---|
| Mean age, y (SD) | 41.5 (12.7) | 52.8 (11.1) | 54.1 (12.6) | 51.7 (14.1) | 44.0 (12.8) | <0.0001 a |
| Gender | <0.0001 b | |||||
| Male, n (%) | 17 (8.8) | 8 (11.4) | 9 (10.7) | 86 (93.5) | 32 (47.1) | |
| Female, n (%) | 176 (91.2) | 62 (88.6) | 75 (89.3) | 6 (6.5) | 36 (52.9) | |
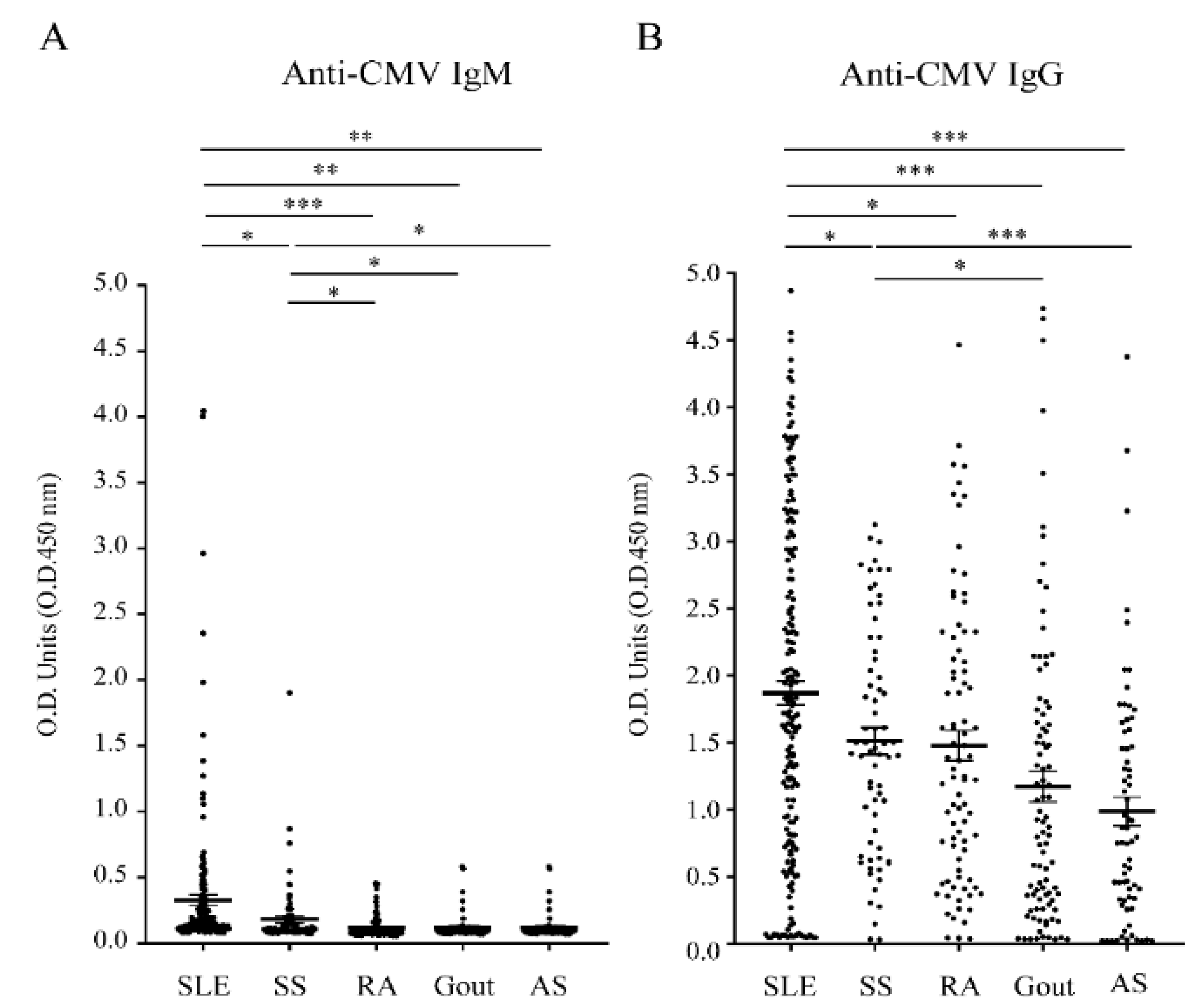
| Anti-CMV IgG (+) | 163 (84.5) | 64 (91.4) | 76 (90.5) | 70 (76.1) | 52 (76.5) | 0.0063 b |
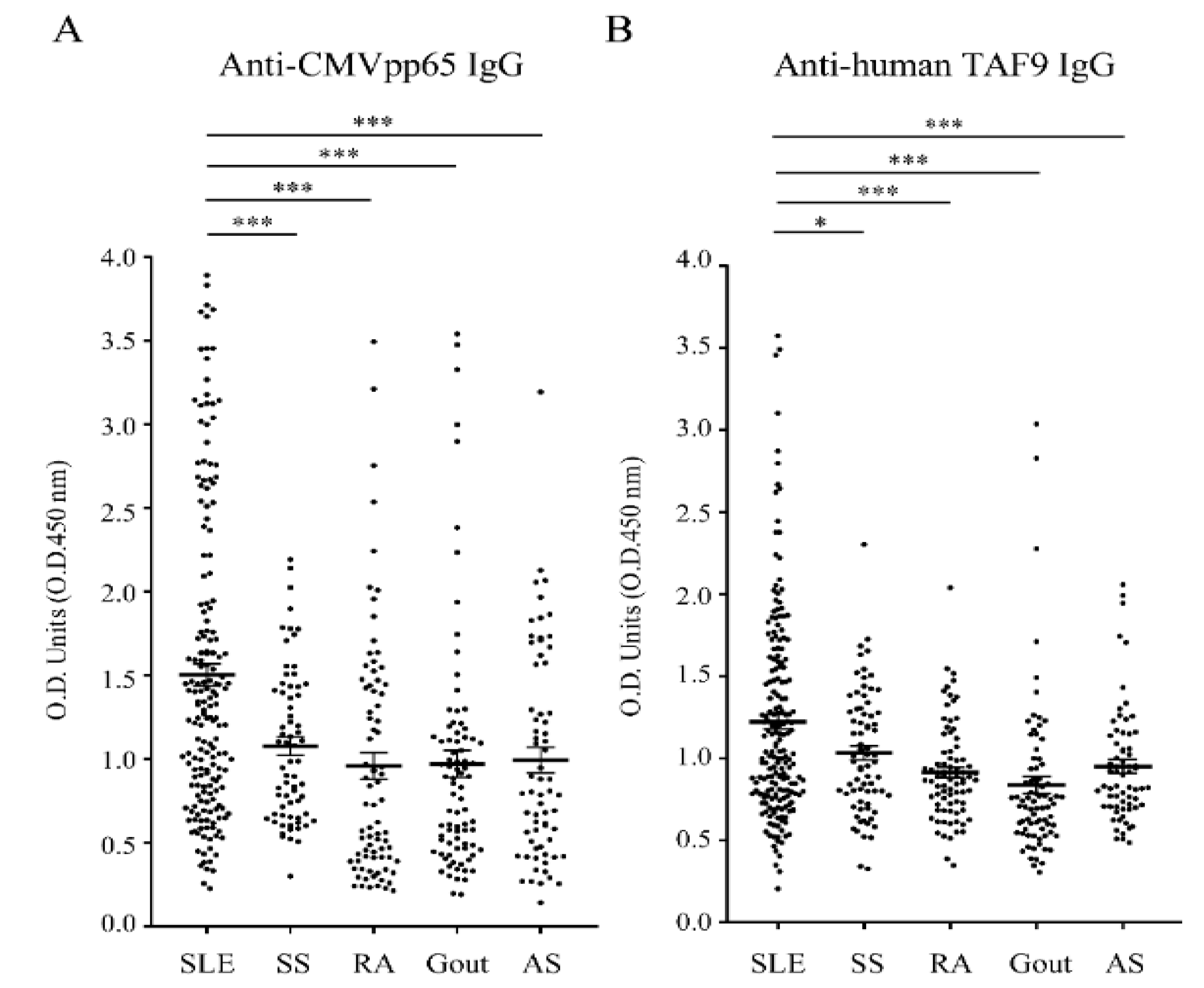
| Anti-CMVpp65 IgG c, n (%) | 61 (37.4) | 12 (18.8) | 10 (13.2) | 13 (18.6) | 17 (32.7) | 0.0004 b |
| Anti-TAF9 IgG c, n (%) | 50 (30.7) | 13 (20.3) | 6 (7.9) | 8 (11.4) | 6 (11.5) | 0.0001 b |
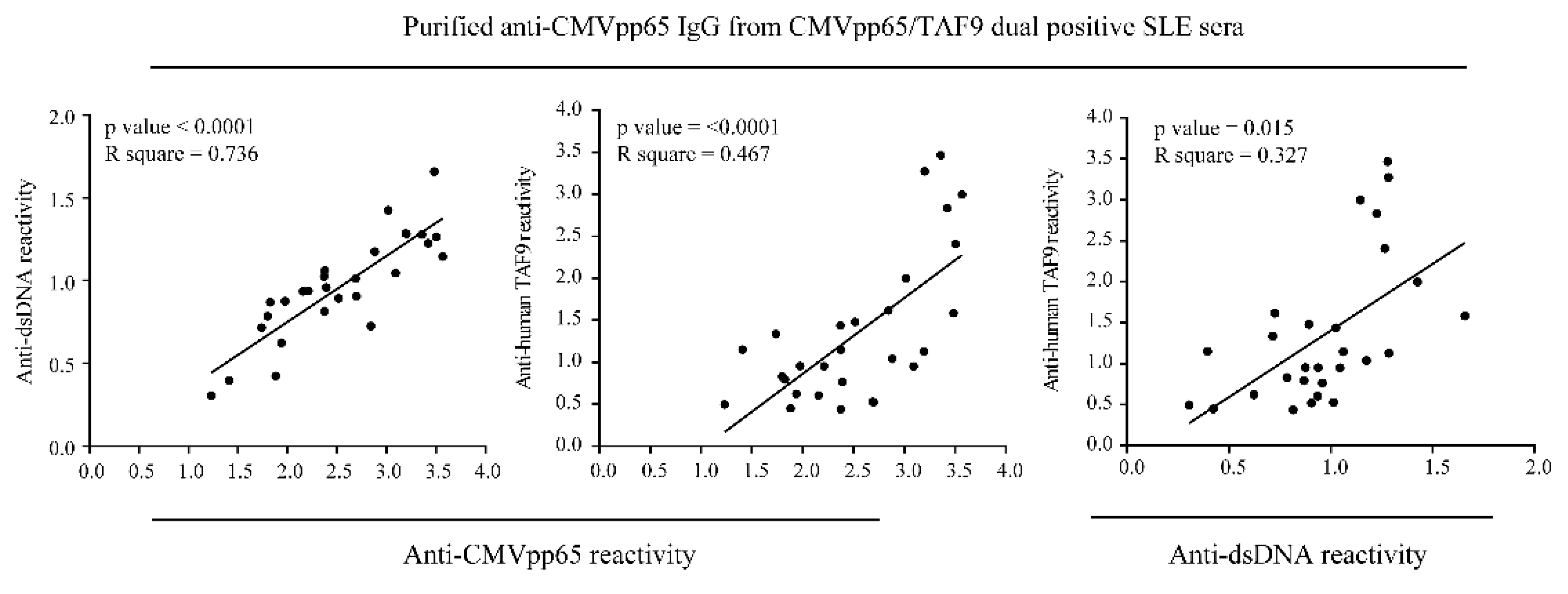
| Dual positives c, n (%) | 28 (17.2) | 8 (12.5) | 3 (3.9) | 4 (5.7) | 5 (9.6) | 0.0219 b |
| Anti-CMV IgM | 21 (10.9) | 5 (7.1) | 2 (2.4) | 3 (3.3) | 2 (2.9) | 0.0217 b |
| Anti-CMV IgM and IgG | 21 (10.9) | 5 (7.1) | 2 (2.4) | 3 (3.3) | 2 (2.9) | 0.0217 b |
| Characteristics | CMV IgG Negative (n = 30) | CMV IgG Positive (n = 163) | p Value | CMVpp65 IgG Negative (n = 102) | CMVpp65 IgG Positive (n = 61) | p Value |
|---|---|---|---|---|---|---|
| Mean age, y (SD) | 43.4 (12.7) | 42.9 (12.1) | 0.837 a | 42.9 (12.3) | 42.8 (12.9) | 0.961 a |
| Female, n (%) | 26 (86.7) | 150 (92.0) | 0.309 b | 94 (92.2) | 56 (91.8) | 1.000 b |
| Cre, n (%) | 3 (10.0) | 25 (15.3) | 0.580 b | 16 (15.7) | 9 (14.8) | 0.873 c |
| Urine protein, n (%) | 3 (10.0) | 48 (29.4) | 0.026 c | 21 (20.6) | 27 (44.3) | 0.002 c |
| WBC, n (%) | 7 (23.3) | 24 (14.7) | 0.278 b | 14 (13.7) | 10 (16.4) | 0.642 c |
| RBC, n (%) | 8 (26.7) | 52 (31.9) | 0.569 c | 29 (28.4) | 23 (37.7) | 0.219 c |
| Hb, n (%) | 9 (30.0) | 89 (54.6) | 0.013 c | 42 (41.2) | 47 (77.1) | <0.0001 c |
| Hct, n (%) | 10 (33.3) | 127 (77.9) | <0.001 c | 78 (76.5) | 49 (80.3) | 0.566 c |
| MCV, n (%) | 4 (13.3) | 29 (17.8) | 0.551 c | 18 (17.6) | 11 (18.0) | 0.950 c |
| MCH, n (%) | 3 (10.0) | 34 (20.9) | 0.165 c | 19 (18.6) | 15 (24.6) | 0.365 c |
| MCHC, n (%) | 2 (6.7) | 14 (8.6) | 1.000 b | 5 (4.9) | 9 (14.8) | 0.029 c |
| Platelets, n (%) | 2 (6.7) | 26 (16) | 0.262 b | 13 (12.7) | 13 (21.3) | 0.148 c |
| Low C3, n (%) | 11 (36.7) | 73 (44.8) | 0.410 c | 40 (39.2) | 33 (54.1) | 0.064 c |
| Low C4, n (%) | 8 (26.7) | 69 (42.3) | 0.107 c | 42 (41.2) | 27 (44.3) | 0.699 c |
| Autoantibodies | ||||||
| Anti-dsDNA, n (%) | 12 (40.0) | 104 (63.8) | 0.014 b | 63 (61.8) | 41 (67.2) | 0.484 c |
| Anti-SSA, n (%) | 4 (13.3) | 59 (36.2) | 0.014 c | 36 (35.3) | 23 (37.7) | 0.757 c |
| Anti-SSB, n (%) | 6 (20.0) | 17 (10.4) | 0.214 b | 11 (10.8) | 6 (9.8) | 0.848 c |
| Anti-Sm, n (%) | 6 (20.0) | 31 (19) | 0.900 c | 19 (18.6) | 12 (19.7) | 0.869 c |
| Anti-RNP, n (%) | 3 (10.0) | 34 (20.9) | 0.165 c | 20 (19.6) | 14 (23.0) | 0.611 c |
| Anti-Scl70, n (%) | 0 (0) | 1 (0.6) | 1.000 b | 0 (0) | 1 (1.6) | 0.374 b |
| Anti-Jo1, n (%) | 0 (0) | 2 (1.2) | 1.000 b | 1 (1) | 1 (1.6) | 1.000 b |
| Anti-CentB, n (%) | 1 (3.3) | 4 (2.5) | 0.575 b | 3 (2.9) | 1 (1.6) | 1.000 b |
| Anti-Histone, n (%) | 4 (13.3) | 22 (13.5) | 1.000 b | 14 (13.7) | 8 (13.1) | 0.912 c |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-F.; Hsieh, A.-H.; Wang, L.-C.; Yu, K.-H.; Kuo, C.-F. Cytomegalovirus-Associated Autoantibody against TAF9 Protein in Patients with Systemic Lupus Erythematosus. J. Clin. Med. 2021, 10, 3722. https://doi.org/10.3390/jcm10163722
Chen Y-F, Hsieh A-H, Wang L-C, Yu K-H, Kuo C-F. Cytomegalovirus-Associated Autoantibody against TAF9 Protein in Patients with Systemic Lupus Erythematosus. Journal of Clinical Medicine. 2021; 10(16):3722. https://doi.org/10.3390/jcm10163722
Chicago/Turabian StyleChen, Yen-Fu, Ao-Ho Hsieh, Lian-Chin Wang, Kuang-Hui Yu, and Chang-Fu Kuo. 2021. "Cytomegalovirus-Associated Autoantibody against TAF9 Protein in Patients with Systemic Lupus Erythematosus" Journal of Clinical Medicine 10, no. 16: 3722. https://doi.org/10.3390/jcm10163722
APA StyleChen, Y.-F., Hsieh, A.-H., Wang, L.-C., Yu, K.-H., & Kuo, C.-F. (2021). Cytomegalovirus-Associated Autoantibody against TAF9 Protein in Patients with Systemic Lupus Erythematosus. Journal of Clinical Medicine, 10(16), 3722. https://doi.org/10.3390/jcm10163722