
The Relative Merits of Posterior Surgical Treatments for Multi-Level Degenerative Cervical Myelopathy Remain Uncertain: Findings from a Systematic Review

 ,
,  , , , , , , ,
, , , , , , ,  , and add
Show full author list
, and add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
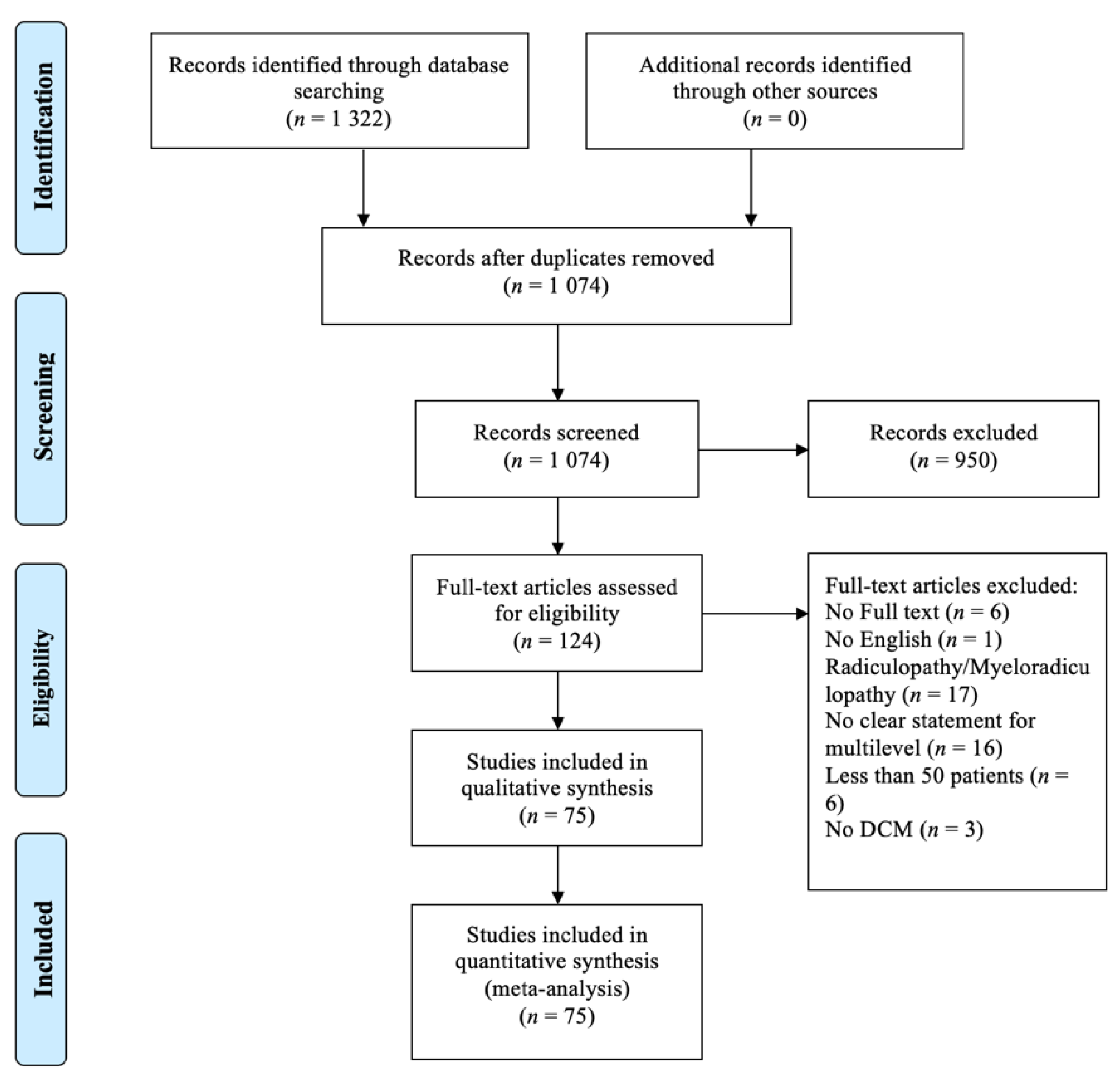
2.1. Literature Search and Selection
- Prospective study with more than 10 patients or retrospective study with more than 50 patients;
- Including multi-level DCM, defined as 2 or more levels;
- Including posterior surgical treatment;
- English, full text;
- Articles published since 1st January 1995.
2.2. Data Extraction
2.3. Quality Assessment
3. Results
3.1. Characteristics of Studies
3.2. Data Quality
3.3. Study Design, Patient Selection and Reporting Differences
3.4. Comparison between Laminoplasty and Laminectomy with Fusion
3.5. Comparison between Laminoplasty and Laminectomy without Fusion
3.6. Comparison between Laminoplasty, Laminectomy with and without Fusion
4. Discussion
4.1. Summary of Findings
4.2. Comparison between Posterior Approaches
4.3. Designing a Future Comparative Study
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Davies, B.M.; Mowforth, O.D.; Smith, E.K.; Kotter, M.R. Degenerative cervical myelopathy. BMJ 2018, 360, k186. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.S.; Stewart, M.E.; Davies, B.M.; Kotter, M.R.N. The Prevalence of Asymptomatic and Symptomatic Spinal Cord Compression on Magnetic Resonance Imaging: A Systematic Review and Meta-analysis. Glob. Spine J. 2021, 11, 597–607. [Google Scholar] [CrossRef]
- Fehlings, M.G.; Tetreault, L.A.; Riew, K.D.; Middleton, J.W.; Aarabi, B.; Arnold, P.M.; Brodke, D.S.; Burns, A.S.; Carette, S.; Chen, R.; et al. A Clinical Practice Guideline for the Management of Patients with Degenerative Cervical Myelopathy: Recommendations for Patients with Mild, Moderate, and Severe Disease and Nonmyelopathic Patients with Evidence of Cord Compression. Glob. Spine J. 2017, 7, 70s–83s. [Google Scholar] [CrossRef] [PubMed]
- Bajamal, A.H.; Kim, S.H.; Arifianto, M.R.; Faris, M.; Subagio, E.A.; Roitberg, B.; Udo-Inyang, I.; Belding, J.; Zileli, M.; Parthiban, J. Posterior Surgical Techniques for Cervical Spondylotic Myelopathy: WFNS Spine Committee Recommendations. Neurospine 2019, 16, 421–434. [Google Scholar] [CrossRef] [PubMed]
- Davies, B.M.; Khan, D.Z.; Mowforth, O.D.; McNair, A.G.K.; Gronlund, T.; Kolias, A.G.; Tetreault, L.; Starkey, M.L.; Sadler, I.; Sarewitz, E.; et al. RE-CODE DCM (REsearch Objectives and Common Data Elements for Degenerative Cervical Myelopathy): A Consensus Process to Improve Research Efficiency in DCM, Through Establishment of a Standardized Dataset for Clinical Research and the Definition of the Research Priorities. Glob. Spine J. 2019, 9, 65s–76s. [Google Scholar] [CrossRef]
- Ghogawala, Z.; Benzel, E.C.; Heary, R.F.; Riew, K.D.; Albert, T.J.; Butler, W.E.; Barker, F.G., 2nd; Heller, J.G.; McCormick, P.C.; Whitmore, R.G.; et al. Cervical spondylotic myelopathy surgical trial: Randomized, controlled trial design and rationale. Neurosurgery 2014, 75, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Davies, B.M.; Francis, J.J.; Butler, M.B.; Mowforth, O.; Goacher, E.; Starkey, M.; Kolias, A.; Wynne-Jones, G.; Hutton, M.; Selvanathan, S.; et al. Current surgical practice for multi-level degenerative cervical myelopathy: Findings from an international survey of spinal surgeons. J. Clin. Neurosci. 2021, 87, 84–88. [Google Scholar] [CrossRef]
- Ryken, T.C.; Heary, R.F.; Matz, P.G.; Anderson, P.A.; Groff, M.W.; Holly, L.T.; Kaiser, M.G.; Mummaneni, P.V.; Choudhri, T.F.; Vresilovic, E.J.; et al. Cervical laminectomy for the treatment of cervical degenerative myelopathy. J. Neurosurg. Spine 2009, 11, 142–149. [Google Scholar] [CrossRef]
- Hale, J.J.; Gruson, K.I.; Spivak, J.M. Laminoplasty: A review of its role in compressive cervical myelopathy. Spine J. 2006, 6, 289s–298s. [Google Scholar] [CrossRef]
- Kaptain, G.J.; Simmons, N.E.; Replogle, R.E.; Pobereskin, L. Incidence and outcome of kyphotic deformity following laminectomy for cervical spondylotic myelopathy. J. Neurosurg. 2000, 93, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Hansen-Schwartz, J.; Kruse-Larsen, C.; Nielsen, C.J. Follow-up after cervical laminectomy, with special reference to instability and deformity. Br. J. Neurosurg. 2003, 17, 301–305. [Google Scholar] [CrossRef]
- Hyun, S.J.; Rhim, S.C.; Roh, S.W.; Kang, S.H.; Riew, K.D. The time course of range of motion loss after cervical laminoplasty: A prospective study with minimum two-year follow-up. Spine (Phila PA 1976) 2009, 34, 1134–1139. [Google Scholar] [CrossRef]
- Houten, J.K.; Cooper, P.R. Laminectomy and posterior cervical plating for multilevel cervical spondylotic myelopathy and ossification of the posterior longitudinal ligament: Effects on cervical alignment, spinal cord compression, and neurological outcome. Neurosurgery 2003, 52, 1081–1088, discussion 1087–1088. [Google Scholar] [PubMed]
- Anderson, P.A.; Matz, P.G.; Groff, M.W.; Heary, R.F.; Holly, L.T.; Kaiser, M.G.; Mummaneni, P.V.; Ryken, T.C.; Choudhri, T.F.; Vresilovic, E.J.; et al. Laminectomy and fusion for the treatment of cervical degenerative myelopathy. J. Neurosurg. Spine 2009, 11, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Rhee, J.M.; Basra, S. Posterior surgery for cervical myelopathy: Laminectomy, laminectomy with fusion, and laminoplasty. Asian Spine J. 2008, 2, 114–126. [Google Scholar] [CrossRef] [PubMed]
- Hamanishi, C.; Tanaka, S. Bilateral multilevel laminectomy with or without posterolateral fusion for cervical spondylotic myelopathy: Relationship to type of onset and time until operation. J. Neurosurg. 1996, 85, 447–451. [Google Scholar] [CrossRef]
- Guigui, P.; Benoist, M.; Deburge, A. Spinal deformity and instability after multilevel cervical laminectomy for spondylotic myelopathy. Spine (Phila PA 1976) 1998, 23, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.S.; Dhillon, R.S. Cervical Laminectomy with or Without Lateral Mass Instrumentation: A Comparison of Outcomes. Clin. Spine Surg. 2019, 32, 226–232. [Google Scholar] [CrossRef]
- McAllister, B.D.; Rebholz, B.J.; Wang, J.C. Is posterior fusion necessary with laminectomy in the cervical spine? Surg. Neurol. Int. 2012, 3, S225–S231. [Google Scholar] [CrossRef]
- Abduljabbar, F.H.; Teles, A.R.; Bokhari, R.; Weber, M.; Santaguida, C. Laminectomy with or without Fusion to Manage Degenerative Cervical Myelopathy. Neurosurg. Clin. N. Am. 2018, 29, 91–105. [Google Scholar] [CrossRef]
- Komotar, R.J.; Mocco, J.; Kaiser, M.G. Surgical management of cervical myelopathy: Indications and techniques for laminectomy and fusion. Spine J. 2006, 6, 252s–267s. [Google Scholar] [CrossRef]
- Fehlings, M.G.; Ibrahim, A.; Tetreault, L.; Albanese, V.; Alvarado, M.; Arnold, P.; Barbagallo, G.; Bartels, R.; Bolger, C.; Defino, H.; et al. A global perspective on the outcomes of surgical decompression in patients with cervical spondylotic myelopathy: Results from the prospective multicenter AOSpine international study on 479 patients. Spine (Phila PA 1976) 2015, 40, 1322–1328. [Google Scholar] [CrossRef] [PubMed]
- Nouri, A.; Martin, A.R.; Nater, A.; Witiw, C.D.; Kato, S.; Tetreault, L.; Reihani-Kermani, H.; Santaguida, C.; Fehlings, M.G. Influence of Magnetic Resonance Imaging Features on Surgical Decision-Making in Degenerative Cervical Myelopathy: Results from a Global Survey of AOSpine International Members. World Neurosurg. 2017, 105, 864–874. [Google Scholar] [CrossRef] [PubMed]
- Davies, B.M.; McHugh, M.; Elgheriani, A.; Kolias, A.G.; Tetreault, L.A.; Hutchinson, P.J.A.; Fehlings, M.G.; Kotter, M.R.N. Reported Outcome Measures in Degenerative Cervical Myelopathy: A Systematic Review. PLoS ONE 2016, 11, e0157263. [Google Scholar] [CrossRef]
- Mowforth, O.D.; Davies, B.M.; Goh, S.; O’Neill, C.P.; Kotter, M.R.N. Research Inefficiency in Degenerative Cervical Myelopathy: Findings of a Systematic Review on Research Activity Over the Past 20 Years. Glob. Spine J. 2020, 10, 476–485. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [PubMed]
- Ajiboye, R.M.; Zoller, S.D.; Ashana, A.A.; Sharma, A.; Sheppard, W.; Holly, L.T. Regression of Disc-Osteophyte Complexes Following Laminoplasty Versus Laminectomy with Fusion for Cervical Spondylotic Myelopathy. Int. J. Spine Surg. 2017, 11, 17. [Google Scholar] [CrossRef]
- Ha, Y.; Shin, J.J. Comparison of clinical and radiological outcomes in cervical laminoplasty versus laminectomy with fusion in patients with ossification of the posterior longitudinal ligament. Neurosurg. Rev. 2019, 43, 1409–1421. [Google Scholar] [CrossRef]
- Highsmith, J.M.; Dhall, S.S.; Haid, R.W., Jr.; Rodts, G.E., Jr.; Mummaneni, P.V. Treatment of cervical stenotic myelopathy: A cost and outcome comparison of laminoplasty versus laminectomy and lateral mass fusion. J. Neurosurg. Spine 2011, 14, 619–625. [Google Scholar] [CrossRef]
- Lee, J.J.; Shin, D.A.; Yi, S.; Kim, K.N.; Yoon, D.H.; Shin, H.C.; Ha, Y. Effect of posterior instrumented fusion on three-dimensional volumetric growth of cervical ossification of the posterior longitudinal ligament: A multiple regression analysis. Spine J. 2018, 18, 1779–1786. [Google Scholar] [CrossRef] [PubMed]
- Stephens, B.F.; Rhee, J.M.; Neustein, T.M.; Arceo, R. Laminoplasty Does not Lead to Worsening Axial Neck Pain in the Properly Selected Patient with Cervical Myelopathy: A Comparison with Laminectomy and Fusion. Spine (Phila PA 1976) 2017, 42, 1844–1850. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Gu, Y.; Shi, J.; Gao, R.; Liu, Y.; Li, J.; Yuan, W. Modified plate-only open-door laminoplasty versus laminectomy and fusion for the treatment of cervical stenotic myelopathy. Orthopedics 2013, 36, e79–e87. [Google Scholar] [CrossRef]
- Chang, H.; Kim, C.; Choi, B.W. Selective laminectomy for cervical spondylotic myelopathy: A comparative analysis with laminoplasty technique. Arch. Orthop. Trauma Surg. 2017, 137, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Han, X.; Wang, R.; Zhang, Y.; Liu, P.; Dong, Q. Clinical recovery after 5 level of posterior decompression spine surgeries in patients with cervical spondylotic myelopathy: A retrospective cohort study. Asian J. Surg. 2020, 43, 613–624. [Google Scholar] [CrossRef]
- Yoo, S.; Ryu, D.; Choi, H.J.; Kuh, S.U.; Chin, D.K.; Kim, K.S.; Cho, Y.E. Ossification foci act as stabilizers in continuous-type ossification of the posterior longitudinal ligament: A comparative study between laminectomy and laminoplasty. Acta Neurochir. (Wien.) 2017, 159, 1783–1790. [Google Scholar] [CrossRef]
- Du, W.; Wang, L.; Shen, Y.; Zhang, Y.; Ding, W.; Ren, L. Long-term impacts of different posterior operations on curvature, neurological recovery and axial symptoms for multilevel cervical degenerative myelopathy. Eur. Spine J. 2013, 22, 1594–1602. [Google Scholar] [CrossRef]
- Lee, C.H.; Jahng, T.A.; Hyun, S.J.; Kim, K.J.; Kim, H.J. Expansive Laminoplasty Versus Laminectomy Alone Versus Laminectomy and Fusion for Cervical Ossification of the Posterior Longitudinal Ligament: Is There a Difference in the Clinical Outcome and Sagittal Alignment? Clin. Spine Surg. 2016, 29, E9–E15. [Google Scholar] [CrossRef]
- Sjöström, L.; Jacobsson, O.; Karlström, G.; Pech, P.; Rauschning, W. Spinal canal remodelling after stabilization of thoracolumbar burst fractures. Eur. Spine J. 1994, 3, 312–317. [Google Scholar] [CrossRef]
- Mumford, J.; Weinstein, J.N.; Spratt, K.F.; Goel, V.K. Thoracolumbar burst fractures. The clinical efficacy and outcome of nonoperative management. Spine (Phila PA 1976) 1993, 18, 955–970. [Google Scholar] [CrossRef]
- Ota, M.; Furuya, T.; Maki, S.; Inada, T.; Kamiya, K.; Ijima, Y.; Saito, J.; Takahashi, K.; Yamazaki, M.; Aramomi, M.; et al. Addition of instrumented fusion after posterior decompression surgery suppresses thickening of ossification of the posterior longitudinal ligament of the cervical spine. J. Clin. Neurosci. 2016, 34, 162–165. [Google Scholar] [CrossRef]
- Hirabayashi, K.; Satomi, K. Operative procedure and results of expansive open-door laminoplasty. Spine (Phila PA 1976) 1988, 13, 870–876. [Google Scholar] [CrossRef]
- Kato, Y.; Iwasaki, M.; Fuji, T.; Yonenobu, K.; Ochi, T. Long-term follow-up results of laminectomy for cervical myelopathy caused by ossification of the posterior longitudinal ligament. J. Neurosurg. 1998, 89, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Bartels, R.H.; van Tulder, M.W.; Moojen, W.A.; Arts, M.P.; Peul, W.C. Laminoplasty and laminectomy for cervical sponydylotic myelopathy: A systematic review. Eur. Spine J. 2015, 24 (Suppl. 2), 160–167. [Google Scholar] [CrossRef] [PubMed]
- Lao, L.; Zhong, G.; Li, X.; Qian, L.; Liu, Z. Laminoplasty versus laminectomy for multi-level cervical spondylotic myelopathy: A systematic review of the literature. J. Orthop. Surg. Res. 2013, 8, 45. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wo, J.; Wen, J.; Zhang, L.; Xu, W.; Wang, X. Laminoplasty versus laminectomy with fusion for treatment of multilevel cervical compressive myelopathy: An updated meta-analysis. Postgrad. Med. J. 2021. [Google Scholar] [CrossRef]
- Deyo, R.A.; Mirza, S.K. Trends and variations in the use of spine surgery. Clin. Orthop. Relat. Res. 2006, 443, 139–146. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, P.; Altman, D.G.; Campbell, W.B.; Flum, D.R.; Glasziou, P.; Marshall, J.C.; Nicholl, J.; Aronson, J.K.; Barkun, J.S.; Blazeby, J.M.; et al. No surgical innovation without evaluation: The IDEAL recommendations. Lancet 2009, 374, 1105–1112. [Google Scholar] [CrossRef]
- Ghogawala, Z.; Terrin, N.; Dunbar, M.R.; Breeze, J.L.; Freund, K.M.; Kanter, A.S.; Mummaneni, P.V.; Bisson, E.F.; Barker, F.G., 2nd; Schwartz, J.S.; et al. Effect of Ventral vs Dorsal Spinal Surgery on Patient-Reported Physical Functioning in Patients with Cervical Spondylotic Myelopathy: A Randomized Clinical Trial. JAMA 2021, 325, 942–951. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Article | Years of Publication | Selection | Comparability | Outcome | Total Score | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Exposed Cohort | Non-Exposed Cohort | Ascertainment of Exposure | Outcome of Interest | Assessment of Outcome | Length of Follow-Up | Adequacy of Follow-Up | ||||
| Ajiboye et al. | 2017 | - | - | * | - | * | - | - | - | 3 * |
| Chang et al. | 2017 | - | - | * | - | * | - | * | * | 5 * |
| Du et al. | 2013 | - | - | * | - | * | * | * | * | 5 * |
| Ha et al. | 2019 | * | * | * | - | * | - | * | * | 6 * |
| Highsmith et al. | 2011 | - | - | * | - | * | - | * | * | 4 * |
| Lee et al. | 2016 | - | - | * | - | * | - | * | * | 4 * |
| Lee et al. | 2018 | - | - | * | - | * | - | * | * | 4 * |
| Li et al. | 2019 | - | - | * | - | * | - | * | * | 5 * |
| Stephens et al. | 2017 | * | * | * | - | * | - | * | * | 5 * |
| Yang et al. | 2013 | - | - | * | - | ** | * | * | * | 6 * |
| Yoo et al. | 2017 | - | - | * | - | ** | - | * | * | 5 * |
| Article | Years of Publication | Sample Size | Study Design | Allocation Basis | Cause of Myelopathy | Function Outcome | Time Point | Radiographic Outcome | Time Point |
|---|---|---|---|---|---|---|---|---|---|
| Ajiboye et al. | 2007 | 70 | Retro | NA | CSM | mJOA | Pre- and post- operation | Disc-osteophyte complex size | Baseline and 10 months |
| Cobb angle | Pre-operation | ||||||||
| Ha et al. | 2019 | 91 | Retro | Radiological factors and age | OPLL | NDI JOA | Pre- and 2 years post-operation | C2–7 SVA C0–2 Cobb angle C2–7 Cobb angle T1 slope Total ROM | Pre-operation and 6,12,24 months |
| Occupying ratio of the spinal canal | Pre-operation | ||||||||
| The thickness of the OPLL Progression of the thickness of the OPLL | Pre-operation and 24 months | ||||||||
| Signal intensity changes | Pre-operation | ||||||||
| Highsmith et al. | 2011 | 56 | Retro | Surgeon-based | Cervical stenotic myelopathy | mJOA Nurick Odom | 42 months | Cervical lordosis ROM | Pre-operation and 42 months |
| Lee et al. | 2018 | 83 | Retro | Cervical lordosis Neck pain Surgeon’s preference | OPLL | NA | - | Cervical curvature ROM | Pre-operation and 2 years |
| OPLL volume | Pre-operation | ||||||||
| Stephens et al. | 2017 | 137 | Retro | Neck pain C2–7 sagittal angle | Cervical myelopathy | NDI mJOA | Pre-operation 6 weeks, 6 and 12 months | C2–7 Cobb angle T1 slope C2–7 SVA Forward pitch Axial canal diameter Miyazaki Spondylosis score | Pre-operation and 12 months |
| Yang et al. | 2013 | 141 | Retro | Surgeon-based | Cervical stenotic myelopathy | mJOA Nurick NDI | Pre- and 24 months | ROM Cervical curvature | Pre- and 24 months |
| Osseous fusion | 6 months postoperatively | ||||||||
| Area of dural sac, increase in area, spinal cord drift | Pre-operation, 6 and 24 months |
| Article | Years of Publication | Sample Size | Study Design | Allocation Basis | Cause of Myelopathy | Function Outcome | Time Point | Radiographic Outcome | Time Point |
|---|---|---|---|---|---|---|---|---|---|
| Chang et al. | 2017 | 67 | Retro | NA | CSM | JOA NDI | Pre-operation, and 12 months | C2–7 Cobb angle ROM | Pre-operation, post-operation, and 12 months |
| Maximal cord compression | Pre-operation | ||||||||
| Spinal canal expansion | Pre-operation and 6 weeks | ||||||||
| Li et al. | 2019 | 330 | Retro | Surgeon-based | CSM | Nurick | 12 months | Cervical lordosis ROM | Pre-operation and 12 months |
| Bony fusion | 6 and 12 months | ||||||||
| Spinal cord volume | 1 week | ||||||||
| Yoo et al. | 2017 | 73 | Retro | NA | OPLL | JOA NDI | Pre-operation and >2 years | C2–7 Cobb angle SVA T1 slope | Pre-operation and >2 years |
| Article | Years of Publication | Sample Size | Study Design | Allocation Basis | Cause of Myelopathy | Function Outcome | Time Point | Radiographic Outcome | Time Point |
|---|---|---|---|---|---|---|---|---|---|
| Du et al. | 2013 | 98 | Retro | NA | DCM and OPLL | JOA NDI | Pre-operation and 7 to 12 years | Curvature index | Pre-operation and 7 to 12 years |
| Lee et al. | 2016 | 57 | Retro | NA | CSM and OPLL | NDI | Pre-operation and 2 years | Curvature index C2–C7 SVA C2–C7 Cobb angle | Pre-operation and 2 years |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, X.; Gharooni, A.-A.; Dhillon, R.S.; Goacher, E.; Dyson, E.W.; Mowforth, O.; Budu, A.; Wynne-Jones, G.; Francis, J.; Trivedi, R.; et al. The Relative Merits of Posterior Surgical Treatments for Multi-Level Degenerative Cervical Myelopathy Remain Uncertain: Findings from a Systematic Review. J. Clin. Med. 2021, 10, 3653. https://doi.org/10.3390/jcm10163653
Yang X, Gharooni A-A, Dhillon RS, Goacher E, Dyson EW, Mowforth O, Budu A, Wynne-Jones G, Francis J, Trivedi R, et al. The Relative Merits of Posterior Surgical Treatments for Multi-Level Degenerative Cervical Myelopathy Remain Uncertain: Findings from a Systematic Review. Journal of Clinical Medicine. 2021; 10(16):3653. https://doi.org/10.3390/jcm10163653
Chicago/Turabian StyleYang, Xiaoyu, Aref-Ali Gharooni, Rana S. Dhillon, Edward Goacher, Edward W. Dyson, Oliver Mowforth, Alexandru Budu, Guy Wynne-Jones, Jibin Francis, Rikin Trivedi, and et al. 2021. "The Relative Merits of Posterior Surgical Treatments for Multi-Level Degenerative Cervical Myelopathy Remain Uncertain: Findings from a Systematic Review" Journal of Clinical Medicine 10, no. 16: 3653. https://doi.org/10.3390/jcm10163653
APA StyleYang, X., Gharooni, A.-A., Dhillon, R. S., Goacher, E., Dyson, E. W., Mowforth, O., Budu, A., Wynne-Jones, G., Francis, J., Trivedi, R., Ivanov, M., Ahuja, S., Rezajooi, K., Demetriades, A. K., Choi, D., Bateman, A. H., Quraishi, N., Kumar, V., Tripathi, M., ... Kotter, M. R. N. (2021). The Relative Merits of Posterior Surgical Treatments for Multi-Level Degenerative Cervical Myelopathy Remain Uncertain: Findings from a Systematic Review. Journal of Clinical Medicine, 10(16), 3653. https://doi.org/10.3390/jcm10163653