
Failure of High-Flow Nasal Cannula Therapy in Pneumonia and Non-Pneumonia Sepsis Patients: A Prospective Cohort Study


 , , and
, , and
Abstract
:1. Introduction
2. Methods
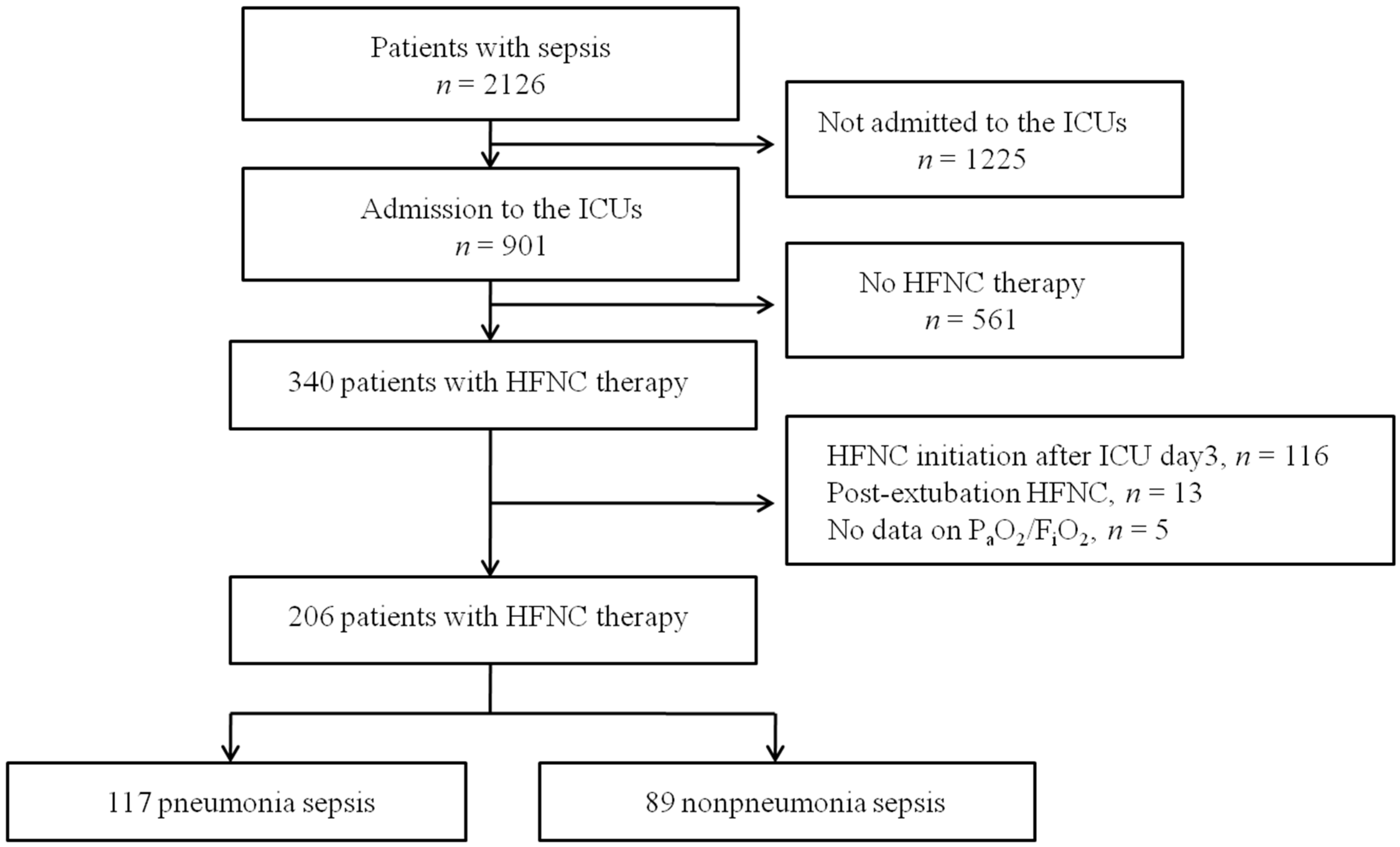
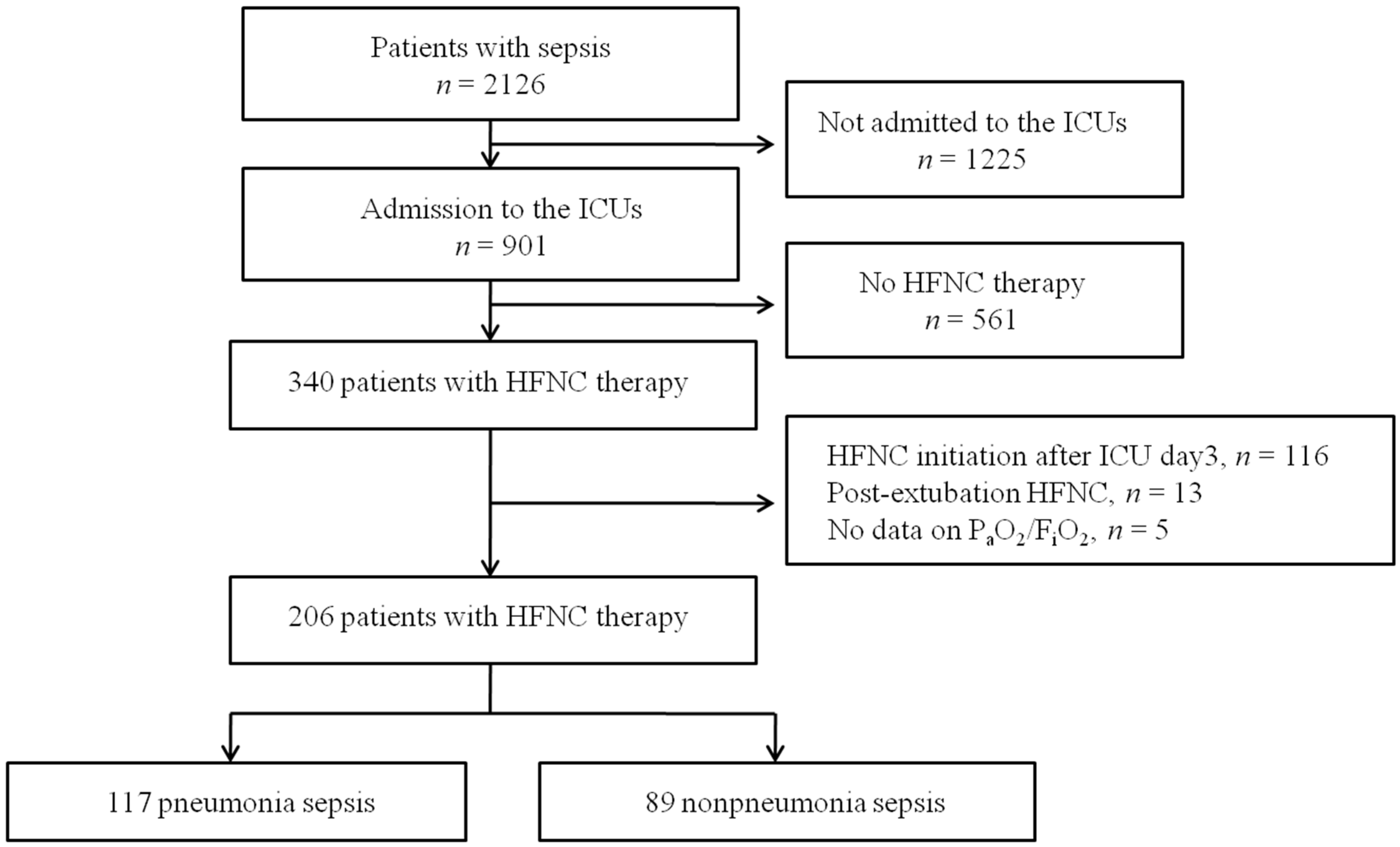
2.1. Study Population
2.2. Data Collection
2.3. Diagnosis of Sepsis and Septic Shock
2.4. Data Analyses
3. Results
3.1. Study Population
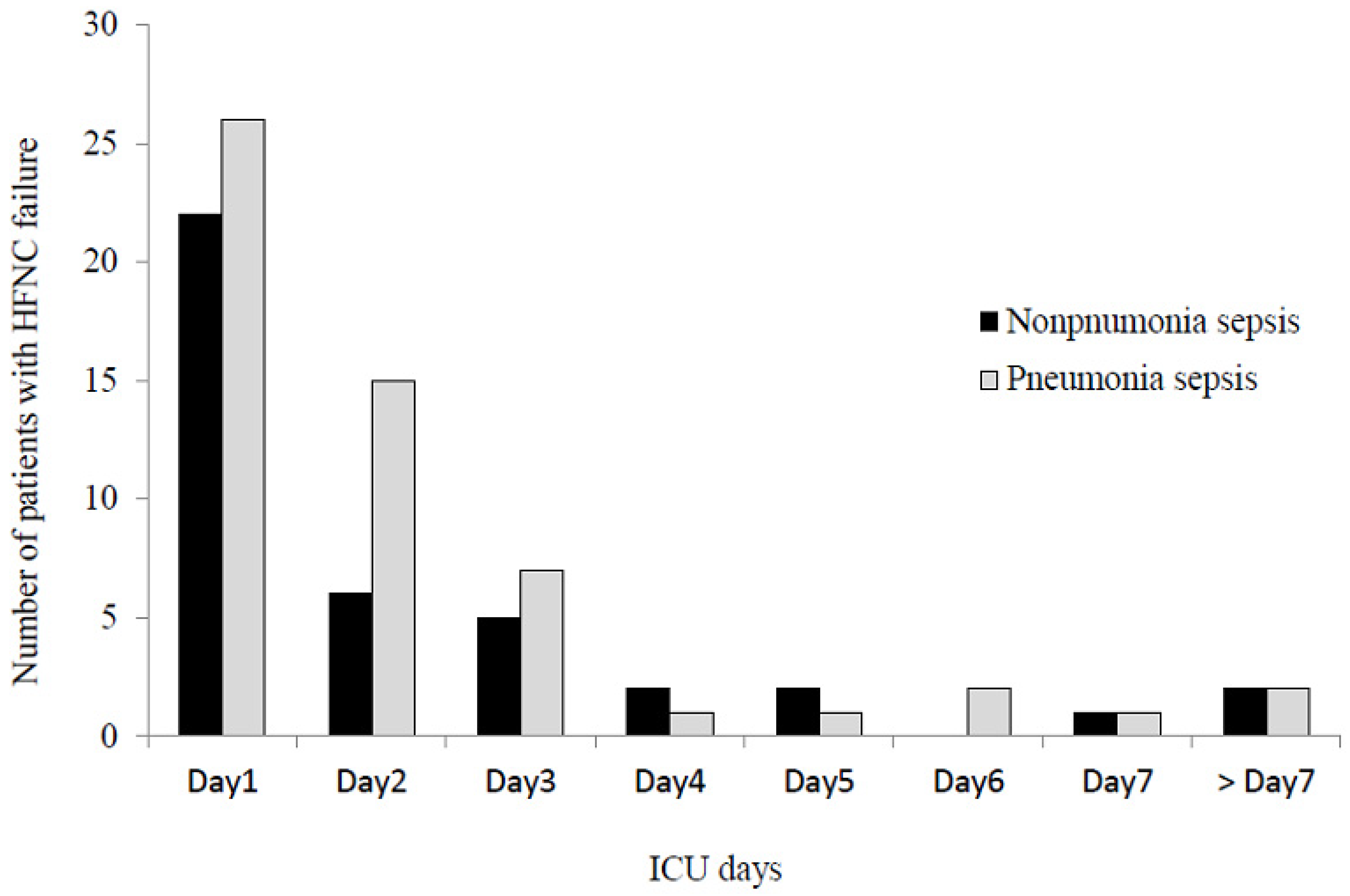
3.2. Treatments and Outcomes
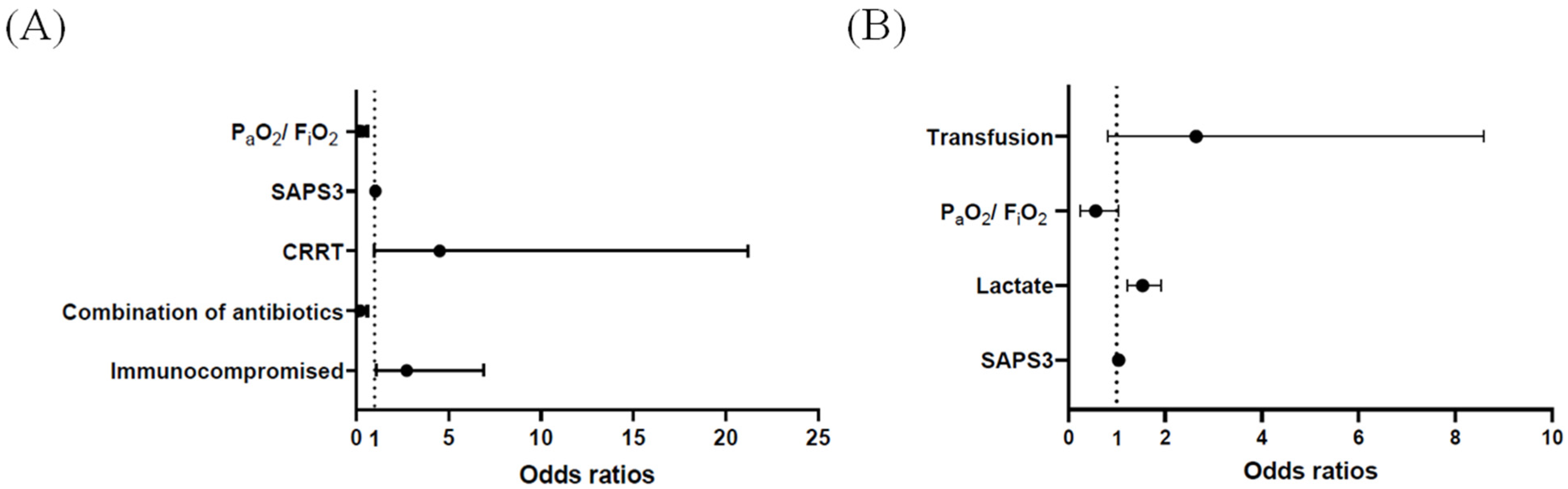
3.3. Risk Factors for Early HFNC Failure
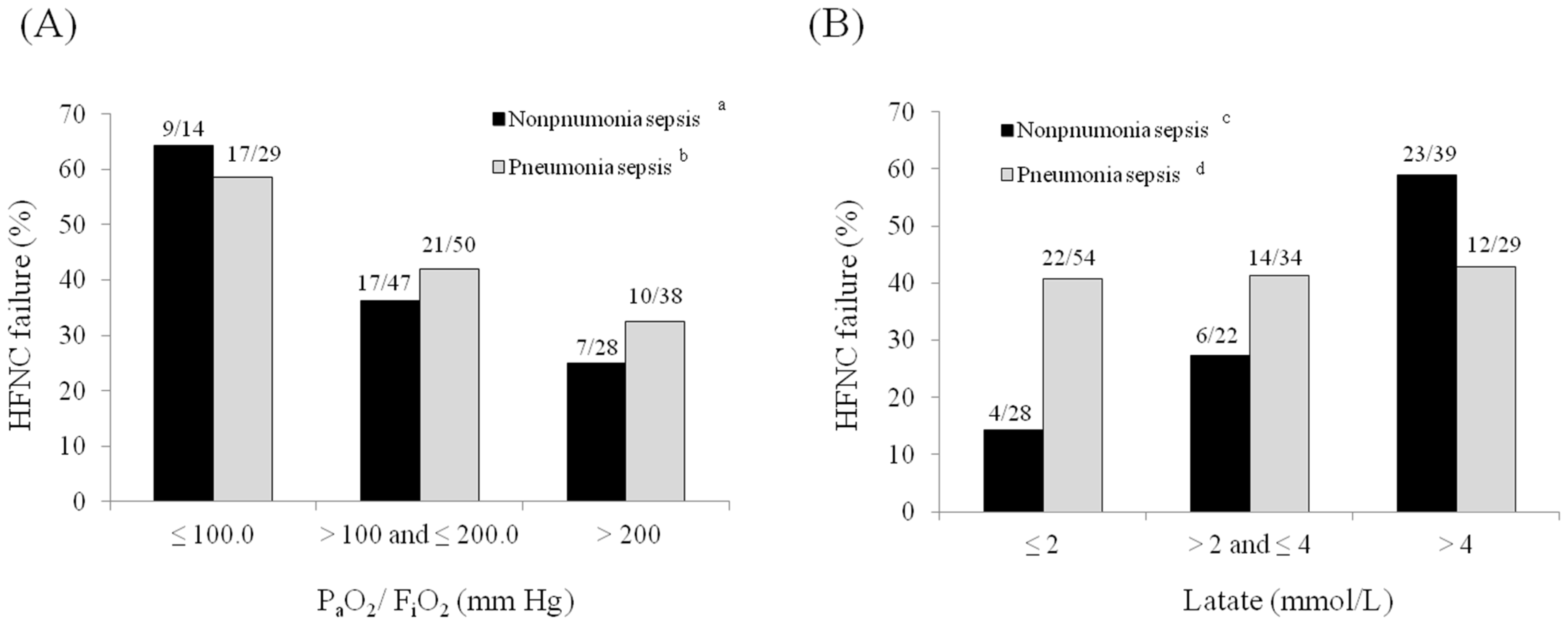
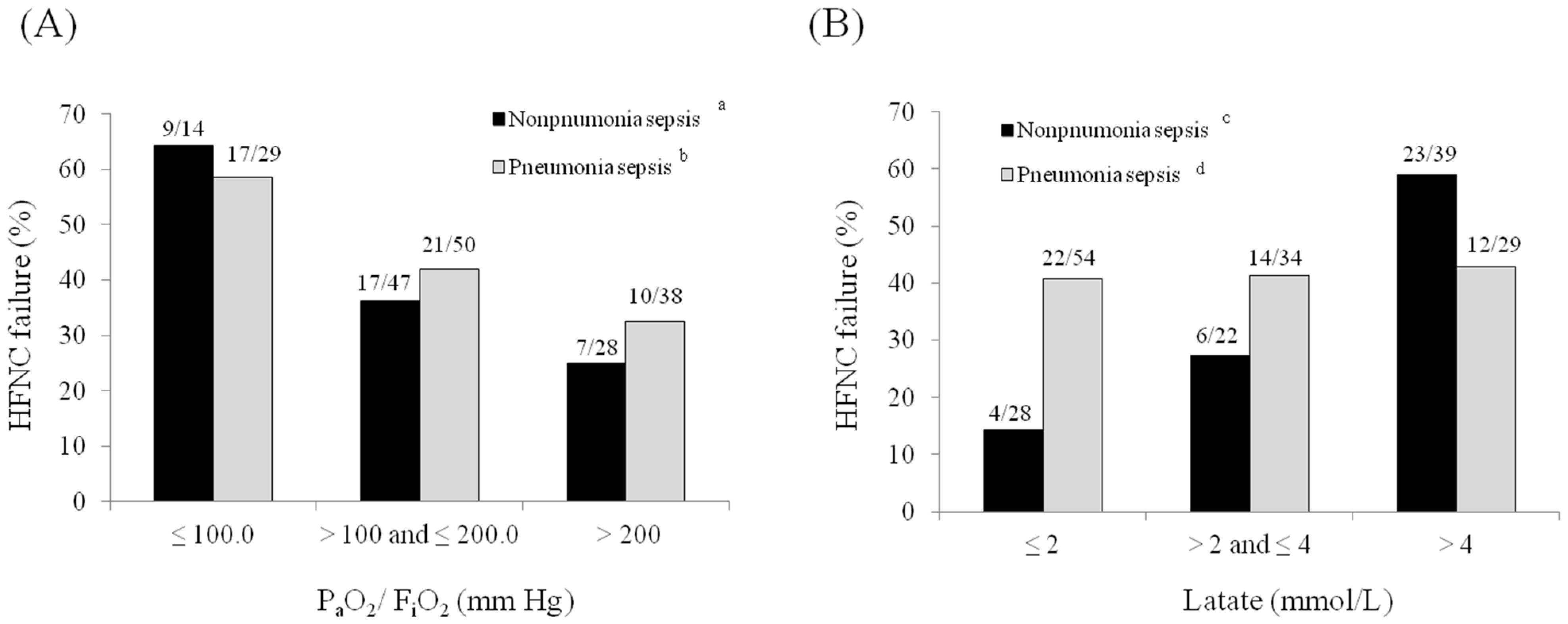
3.4. Rates of Early HFNC Failure According to PaO2/FiO2 Ratios and Lactate Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Angus, D.C.; Linde-Zwirble, W.T.; Lidicker, J.; Clermont, G.; Carcillo, J.; Pinsky, M.R. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001, 29, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Kaukonen, K.M.; Bailey, M.; Suzuki, S.; Pilcher, D.; Bellomo, R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000–2012. JAMA 2014, 311, 1308–1316. [Google Scholar] [CrossRef]
- Horak, J.; Martinkova, V.; Radej, J.; Matejovič, M. Back to Basics: Recognition of Sepsis with New Definition. J. Clin. Med. 2019, 8, 1838. [Google Scholar] [CrossRef] [Green Version]
- Frat, J.P.; Ragot, S.; Girault, C.; Perbet, S.; Prat, G.; Boulain, T.; Demoule, A.; Ricard, J.D.; Coudroy, R.; Robert, R.; et al. Effect of non-invasive oxygenation strategies in immunocompromised patients with severe acute respiratory failure: A post-hoc analysis of a randomised trial. Lancet Respir. Med. 2016, 4, 646–652. [Google Scholar] [CrossRef]
- Frat, J.P.; Thille, A.W.; Mercat, A.; Girault, C.; Ragot, S.; Perbet, S.; Prat, G.; Boulain, T.; Morawiec, E.; Cottereau, A.; et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N. Engl. J. Med. 2015, 372, 2185–2196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauri, T.; Turrini, C.; Eronia, N.; Grasselli, G.; Volta, C.A.; Bellani, G.; Pesenti, A. Physiologic Effects of High-Flow Nasal Cannula in Acute Hypoxemic Respiratory Failure. Am. J. Respir. Crit. Care Med. 2017, 195, 1207–1215. [Google Scholar] [CrossRef] [PubMed]
- Roca, O.; Riera, J.; Torres, F.; Masclans, J.R. High-flow oxygen therapy in acute respiratory failure. Respir. Care 2010, 55, 408–413. [Google Scholar]
- Sztrymf, B.; Messika, J.; Bertrand, F.; Hurel, D.; Leon, R.; Dreyfuss, D.; Ricard, J.D. Beneficial effects of humidified high flow nasal oxygen in critical care patients: A prospective pilot study. Intensive Care Med. 2011, 37, 1780–1786. [Google Scholar] [CrossRef]
- Roca, O.; Caralt, B.; Messika, J.; Samper, M.; Sztrymf, B.; Hernandez, G.; Garcia-de-Acilu, M.; Frat, J.P.; Masclans, J.R.; Ricard, J.D. An Index Combining Respiratory Rate and Oxygenation to Predict Outcome of Nasal High-Flow Therapy. Am. J. Respir. Crit. Care Med. 2019, 199, 1368–1376. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Moreno, R.P.; Metnitz, P.G.; Almeida, E.; Jordan, B.; Bauer, P.; Campos, R.A.; Iapichino, G.; Edbrooke, D.; Capuzzo, M.; Le Gall, J.R. SAPS 3—From evaluation of the patient to evaluation of the intensive care unit. Part 2: Development of a prognostic model for hospital mortality at ICU admission. Intensive Care Med. 2005, 31, 1345–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Melot, C.; Vincent, J.L. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA 2001, 286, 1754–1758. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratala, J.; et al. Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M., Jr.; Musher, D.M.; Niederman, M.S.; et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2007, 44 (Suppl. 2), S27–S72. [Google Scholar] [CrossRef]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The Surviving Sepsis Campaign Bundle: 2018 update. Intensive Care Med. 2018, 44, 925–928. [Google Scholar] [CrossRef] [Green Version]
- Rochwerg, B.; Granton, D.; Wang, D.X.; Helviz, Y.; Einav, S.; Frat, J.P.; Mekontso-Dessap, A.; Schreiber, A.; Azoulay, E.; Mercat, A.; et al. High flow nasal cannula compared with conventional oxygen therapy for acute hypoxemic respiratory failure: A systematic review and meta-analysis. Intensive Care Med. 2019, 45, 563–572. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Jeon, K.; Oh, D.K.; Choi, E.Y.; Seong, G.M.; Heo, J.; Chang, Y.; Kwack, W.G.; Kang, B.J.; Choi, W.I.; et al. Normothermia in Patients with Sepsis Who Present to Emergency Departments Is Associated with Low Compliance with Sepsis Bundles and Increased In-Hospital Mortality Rate. Crit. Care Med. 2020, 48, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Corley, A.; Caruana, L.R.; Barnett, A.G.; Tronstad, O.; Fraser, J.F. Oxygen delivery through high-flow nasal cannulae increase end-expiratory lung volume and reduce respiratory rate in post-cardiac surgical patients. Br. J. Anaesth. 2011, 107, 998–1004. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.H.; Kim, E.Y.; Seo, G.J.; Suh, H.J.; Huh, J.W.; Hong, S.B.; Koh, Y.; Lim, C.M. Global and Regional Ventilation during High Flow Nasal Cannula in Patients with Hypoxia. Acute Crit. Care 2018, 33, 7–15. [Google Scholar] [CrossRef]
- Epstein, A.S.; Hartridge-Lambert, S.K.; Ramaker, J.S.; Voigt, L.P.; Portlock, C.S. Humidified high-flow nasal oxygen utilization in patients with cancer at Memorial Sloan-Kettering Cancer Center. J. Palliat. Med. 2011, 14, 835–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, S.G.; Holets, S.R.; Gay, P.C. High-flow nasal cannula therapy in do-not-intubate patients with hypoxemic respiratory distress. Respir. Care 2013, 58, 597–600. [Google Scholar]
- Makdee, O.; Monsomboon, A.; Surabenjawong, U.; Praphruetkit, N.; Chaisirin, W.; Chakorn, T.; Permpikul, C.; Thiravit, P.; Nakornchai, T. High-Flow Nasal Cannula versus Conventional Oxygen Therapy in Emergency Department Patients with Cardiogenic Pulmonary Edema: A Randomized Controlled Trial. Ann. Emerg. Med. 2017, 70, 465–472.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thille, A.W.; Muller, G.; Gacouin, A.; Coudroy, R.; Decavele, M.; Sonneville, R.; Beloncle, F.; Girault, C.; Dangers, L.; Lautrette, A.; et al. Effect of Postextubation High-Flow Nasal Oxygen with Noninvasive Ventilation vs. High-Flow Nasal Oxygen Alone on Reintubation Among Patients at High Risk of Extubation Failure: A Randomized Clinical Trial. JAMA 2019, 322, 1465–1475. [Google Scholar] [CrossRef]
- Bae, S.; Han, M.; Kim, C.; Lee, H.; Ahn, J.J.; Kim, J.H.; Kang, B.J. High-Flow Nasal Cannula Oxygen Therapy Can Be Effective for Patients in Acute Hypoxemic Respiratory Failure with Hypercapnia: A Retrospective, Propensity Score-Matched Cohort Study. J. Korean Med. Sci. 2020, 35, e67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rello, J.; Perez, M.; Roca, O.; Poulakou, G.; Souto, J.; Laborda, C.; Balcells, J.; Serra, J.; Masclans, J.R.; CRIPS Investigators. High-flow nasal therapy in adults with severe acute respiratory infection: A cohort study in patients with 2009 influenza A/H1N1v. J. Crit. Care 2012, 27, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Koga, Y.; Kaneda, K.; Mizuguchi, I.; Nakahara, T.; Miyauchi, T.; Fujita, M.; Kawamura, Y.; Oda, Y.; Tsuruta, R. Extent of pleural effusion on chest radiograph is associated with failure of high-flow nasal cannula oxygen therapy. J. Crit. Care 2016, 32, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.Y.; Sung, H.; Hong, S.B.; Lim, C.M.; Koh, Y.; Huh, J.W. Predictors of high flow nasal cannula failure in immunocompromised patients with acute respiratory failure due to non-HIV pneumocystis pneumonia. J. Thorac. Dis. 2017, 9, 3013–3022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messika, J.; Ben Ahmed, K.; Gaudry, S.; Miguel-Montanes, R.; Rafat, C.; Sztrymf, B.; Dreyfuss, D.; Ricard, J.D. Use of High-Flow Nasal Cannula Oxygen Therapy in Subjects with ARDS: A 1-Year Observational Study. Respir. Care 2015, 60, 162–169. [Google Scholar] [CrossRef] [Green Version]
- Roca, O.; de Acilu, M.G.; Caralt, B.; Sacanell, J.; Masclans, J.R. Humidified high flow nasal cannula supportive therapy improves outcomes in lung transplant recipients readmitted to the intensive care unit because of acute respiratory failure. Transplantation 2015, 99, 1092–1098. [Google Scholar] [CrossRef]
- Liu, L.; Xie, J.; Wu, W.; Chen, H.; Li, S.; He, H.; Yu, Y.; Hu, M.; Li, J.; Zheng, R.; et al. A simple nomogram for predicting failure of non-invasive respiratory strategies in adults with COVID-19: A retrospective multicentre study. Lancet. Digit. Health 2021, 3, e166–e74. [Google Scholar] [CrossRef]
- Kang, B.J.; Koh, Y.; Lim, C.M.; Huh, J.W.; Baek, S.; Han, M.; Seo, H.S.; Suh, H.J.; Seo, G.J.; Kim, E.Y.; et al. Failure of high-flow nasal cannula therapy may delay intubation and increase mortality. Intensive Care Med. 2015, 41, 623–632. [Google Scholar] [CrossRef]
- Peake, S.L.; Delaney, A.; Bailey, M.; Bellomo, R.; Cameron, P.A.; Cooper, D.J.; Higgins, A.M.; Holdgate, A.; Howe, B.D.; Webb, S.A.; et al. Goal-directed resuscitation for patients with early septic shock. N. Engl. J. Med. 2014, 371, 1496–1506. [Google Scholar]
- Yealy, D.M.; Kellum, J.A.; Huang, D.T.; Barnato, A.E.; Weissfeld, L.A.; Pike, F.; Terndrup, T.; Wang, H.E.; Hou, P.C.; LoVecchio, F.; et al. A randomized trial of protocol-based care for early septic shock. N. Engl. J. Med. 2014, 370, 1683–1693. [Google Scholar] [PubMed] [Green Version]
- Mouncey, P.R.; Osborn, T.M.; Power, G.S.; Harrison, D.A.; Sadique, M.Z.; Grieve, R.D.; Jahan, R.; Harvey, S.E.; Bell, D.; Bion, J.F.; et al. Trial of early, goal-directed resuscitation for septic shock. N. Engl. J. Med. 2015, 372, 1301–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.I.; Park, S. Sepsis: Early Recognition and Optimized Treatment. Tuberc. Respir. Dis. 2019, 82, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Frat, J.P.; Ragot, S.; Coudroy, R.; Constantin, J.M.; Girault, C.; Prat, G.; Boulain, T.; Demoule, A.; Ricard, J.D.; Razazi, K.; et al. Predictors of Intubation in Patients with Acute Hypoxemic Respiratory Failure Treated with a Noninvasive Oxygenation Strategy. Crit. Care Med. 2018, 46, 208–215. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Pneumonia Sepsis (n = 117) | Non-Pneumonia Sepsis (n = 89) | p Value |
|---|---|---|---|
| Age, years | 71.0 (63.0–78.0) | 71.0 (60.5–80.0) | 0.956 |
| Gender, M/F | 87/30 | 55/34 | 0.054 |
| Underlying disease | |||
| Cardiovascular disease | 23 (19.7%) | 17 (19.1%) | 0.920 |
| Cerebrovascular disease | 25 (21.4%) | 16 (18.0%) | 0.546 |
| Chronic liver disease | 7 (6.0%) | 11(12.4%) | 0.108 |
| Connective tissue disease | 3 (2.6%) | 1 (1.1%) | 0.635 |
| Chronic lung disease | 27 (23.1%) | 8 (9.0%) | 0.008 |
| Chronic kidney disease | 16 (13.7%) | 16 (18.0%) | 0.398 |
| Diabetes | 46 (39.3%) | 27 (30.3%) | 0.182 |
| Immunocompromised a | 40 (34.2%) | 31 (34.8%) | 0.932 |
| Charlson comorbidity index | 5.0 (3.0–6.5) | 5.0 (3.0–6.0) | 0.583 |
| ECOG | 2.0 (1.0–3.0) | 2.0 (1.0–3.0) | 0.907 |
| Septic shock | 27 (23.1%) | 54 (60.7%) | <0.001 |
| Sepsis origin | |||
| Lung | 117 (100.0%) | 0 (0.0%) | <0.001 |
| Abdomen | 0 (0.0%) | 36 (40.4%) | |
| Urinary | 0 (0.0%) | 28 (31.5%) | |
| Skin and soft tissue | 0 (0.0%) | 7 (7.9%) | |
| CLABSI | 0 (0.0%) | 4 (4.5%) | |
| Other systemic infections | 0 (0.0%) | 14 (15.7%) | |
| SAPS3 at ICU admission | 65.0 (55.0–74.0) | 69.0 (67.0–81.0) | 0.005 |
| SOFA on the day of HFNC start | 7.0 (5.0–9.5) | 10.0 (7.0–12.0) | <0.001 |
| At the initiation of HFNC | |||
| pH | 7.41 (7.35–7.46) | 7.38 (7.31–7.45) | 0.049 |
| PaCO2, mm Hg | 32.1 (27.8–38.5) | 30.1 (25.9–36.0) | 0.102 |
| PaO2/FiO2 | 150.0 (100.5–224.2) | 164.0 (117.8–230.2) | 0.218 |
| Lactate, mmol/L | 2.1 (1.2–4.0) | 3.2 (1.8–6.2) | <0.001 |
| Bacteremia | 15 (12.8%) | 36 (40.0%) | <0.001 |
| Infection by MDR pathogens | 21 (17.9%) | 19 (21.3%) | 0.541 |
| CAI/HAI | 83/34 | 47/42 | 0.008 |
| 3-h sepsis bundle b | 28 (23.9%) | 25 (28.1%) | 0.499 |
| Adequate antibiotics | 101 (86.3%) | 82 (92.1%) | 0.190 |
| Combination of antibiotics | 87 (74.4%) | 44 (49.4%) | <0.001 |
| Steroid treatments | 36 (30.8%) | 27 (30.3%) | 0.947 |
| Transfusions | 27 (23.1%) | 47 (52.8%) | <0.001 |
| Noninvasive ventilation | 2 (1.7%) | 2 (2.2%) | 0.782 |
| CRRT | 11 (9.4%) | 27 (30.3%) | <0.001 |
| Pre-ICU fluid balance, mL | 749.0 (200.0–1763.8) | 972.0 (305.0–2238.0) | 0.389 |
| Day1 fluid balance, mL | 366.4 (−34.3–901.8) | 721.0 (78.5–1680.9) | 0.029 |
| Outcomes | Pneumonia Sepsis (n = 117) | Non-Pneumonia Sepsis (n = 89) | p Value |
|---|---|---|---|
| Mechanical ventilation | 44 (37.6%) | 28 (31.5%) | 0.359 |
| ICU death | 26 (22.0%) | 25 (28.1%) | 0.334 |
| Hospital death | 40 (34.2%) | 30 (33.7%) | 0.943 |
| HFNC failure at ICU day3 | 48 (41.0%) | 33 (37.1%) | 0.566 |
| HFNC failure at ICU day7 | 53 (45.3%) | 38 (42.7%) | 0.709 |
| HFNC failure during ICU stay | 55 (47.0%) | 40 (44.9%) | 0.768 |
| Length of ICU stay, days | 6.0 (3.0–11.0) | 4.0 (3.0–10.0) | 0.248 |
| Length of hospital stay, days | 20.0 (10.0–30.0) | 19.0 (10.0–31.5) | 0.803 |
| Variables | Univariable Analysis | Multivariable Analysis d | ||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Immunocompromised b | 2.397 | 1.097–5.239 | 2.730 | 1.082–6.889 |
| Combination of antibiotics | 0.351 | 0.149–0.824 | 0.219 | 0.079–0.605 |
| CRRT | 4.400 | 1.013–17.556 | 4.520 | 0.963–21.215 |
| SAPS3 at ICU admission | 1.001 | 1.000–1.001 | 1.038 | 0.997–1.081 |
| PaO2/FiO2 ratio c | 0.502 | 0.300–0.841 | 0.308 | 0.158–0.601 |
| Variables | Univariable Analysis | Multivariable Analysis c | ||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| SAPS3 at ICU admission | 1.074 | 1.033–1.117 | 1.040 | 0.990–1.092 |
| Lactate | 1.618 | 1.302–2.012 | 1.532 | 1.218–1.926 |
| PaO2/FiO2 ratio b | 0.447 | 0.225–0.889 | 0.564 | 0.244–1.030 |
| Transfusion | 3.826 | 1.505–9.725 | 2.643 | 0.813–8.590 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, E.; Jeon, K.; Oh, D.K.; Cho, Y.-J.; Hong, S.-B.; Lee, Y.J.; Lee, S.-M.; Suh, G.Y.; Park, M.-H.; Lim, C.-M.; et al. Failure of High-Flow Nasal Cannula Therapy in Pneumonia and Non-Pneumonia Sepsis Patients: A Prospective Cohort Study. J. Clin. Med. 2021, 10, 3587. https://doi.org/10.3390/jcm10163587
Kim E, Jeon K, Oh DK, Cho Y-J, Hong S-B, Lee YJ, Lee S-M, Suh GY, Park M-H, Lim C-M, et al. Failure of High-Flow Nasal Cannula Therapy in Pneumonia and Non-Pneumonia Sepsis Patients: A Prospective Cohort Study. Journal of Clinical Medicine. 2021; 10(16):3587. https://doi.org/10.3390/jcm10163587
Chicago/Turabian StyleKim, Eunhye, Kyeongman Jeon, Dong Kyu Oh, Young-Jae Cho, Sang-Bum Hong, Yeon Joo Lee, Sang-Min Lee, Gee Young Suh, Mi-Hyeon Park, Chae-Man Lim, and et al. 2021. "Failure of High-Flow Nasal Cannula Therapy in Pneumonia and Non-Pneumonia Sepsis Patients: A Prospective Cohort Study" Journal of Clinical Medicine 10, no. 16: 3587. https://doi.org/10.3390/jcm10163587
APA StyleKim, E., Jeon, K., Oh, D. K., Cho, Y.-J., Hong, S.-B., Lee, Y. J., Lee, S.-M., Suh, G. Y., Park, M.-H., Lim, C.-M., Park, S., & on behalf of the Korean Sepsis Alliance (KSA) Investigators. (2021). Failure of High-Flow Nasal Cannula Therapy in Pneumonia and Non-Pneumonia Sepsis Patients: A Prospective Cohort Study. Journal of Clinical Medicine, 10(16), 3587. https://doi.org/10.3390/jcm10163587