
3D-Printed Titanium Custom-Made Prostheses in Reconstruction after Pelvic Tumor Resection: Indications and Results in a Series of 14 Patients at 42 Months of Average Follow-Up

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Epidemiology
3.2. Histologies and Localizations
3.3. Symptoms
3.4. Surgeries
3.5. Chemotherapy
3.6. Radiotherapy
3.7. Complications
3.8. Local Recurrence
3.9. Metastases
3.10. Survival
3.11. Functional Results
4. Discussion
4.1. Indications
- The patient’s age: 3DPTCMPs could be unsuitable in young ages because the pelvis still has to reach its ultimate size, whereas reconstruction in very old patients could give fixation and mobilization problems due to low bone quality.
- The diagnosis: the time needed to produce the 3DPTCMP has to be taken into account. At present, fabrication requires an average of four weeks, so patients affected by low-grade malignant tumors are more suitable than those with high-grade tumors. Obviously, the prosthesis can be produced during neoadjuvant chemotherapy in the case of high-grade tumors. Indeed, chondrosarcoma is the main histology treated, both because it is the most frequent malignant bone tumor in the pelvis and because its grade of aggressiveness is usually compatible with prosthesis making. In the present series, two cases of Ewing’s sarcoma also underwent reconstruction with 3DPTCMP. In these cases, chemotherapy was entirely performed in a neoadjuvant setting, considering that possible surgical infection could have played against chemotherapy prosecution. Indeed, one of the two cases had sepsis caused by urinary catheter infection; this caused a hardware contamination and removal was necessary to resolve the septic shock. The patient is due to have cemented spacer removal and new reconstruction, 12 months after rib metastasis extirpation and 40 months from index surgery (case 7).
- The site: the aim of reconstruction after pelvic resection is to restore hip stability by giving the articulation a pivot. Acetabulum sparing is the keystone. Reconstruction can be performed with a hip prosthesis that includes a cup with an iliac stem when part of the anterior or posterior column is spared. When resection includes the acetabular roof (Figure 3A), an acetabulum with an iliac stem does not have sufficient bone support, so 3DPTCMP is a possible solution (Figure 3C right side); the 3DPTCMP should be linked to a spine stabilization to neutralize vertical cutting forces when resection includes the sacrum-iliac joint (Figure 5A,B).
4.2. Reconstruction
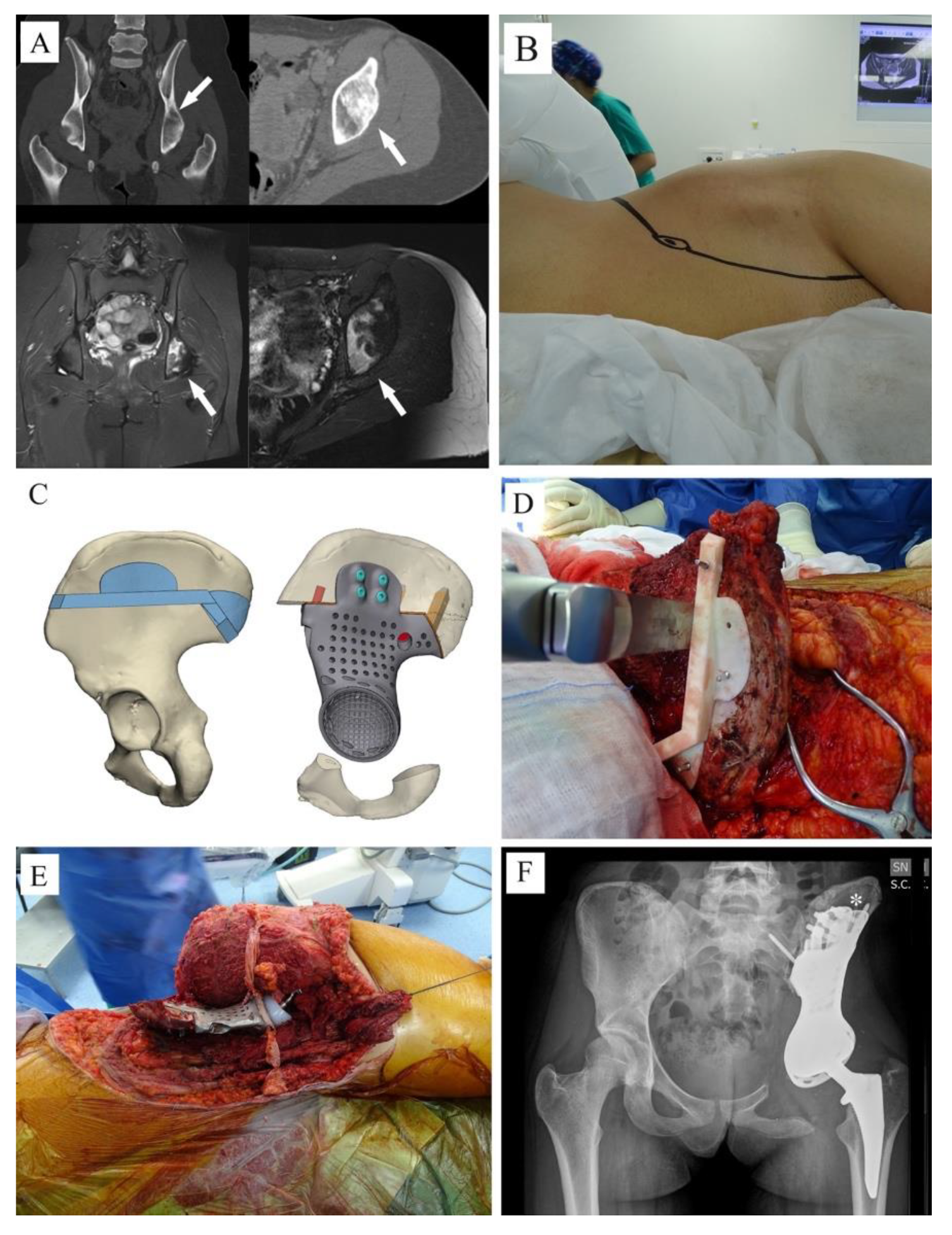
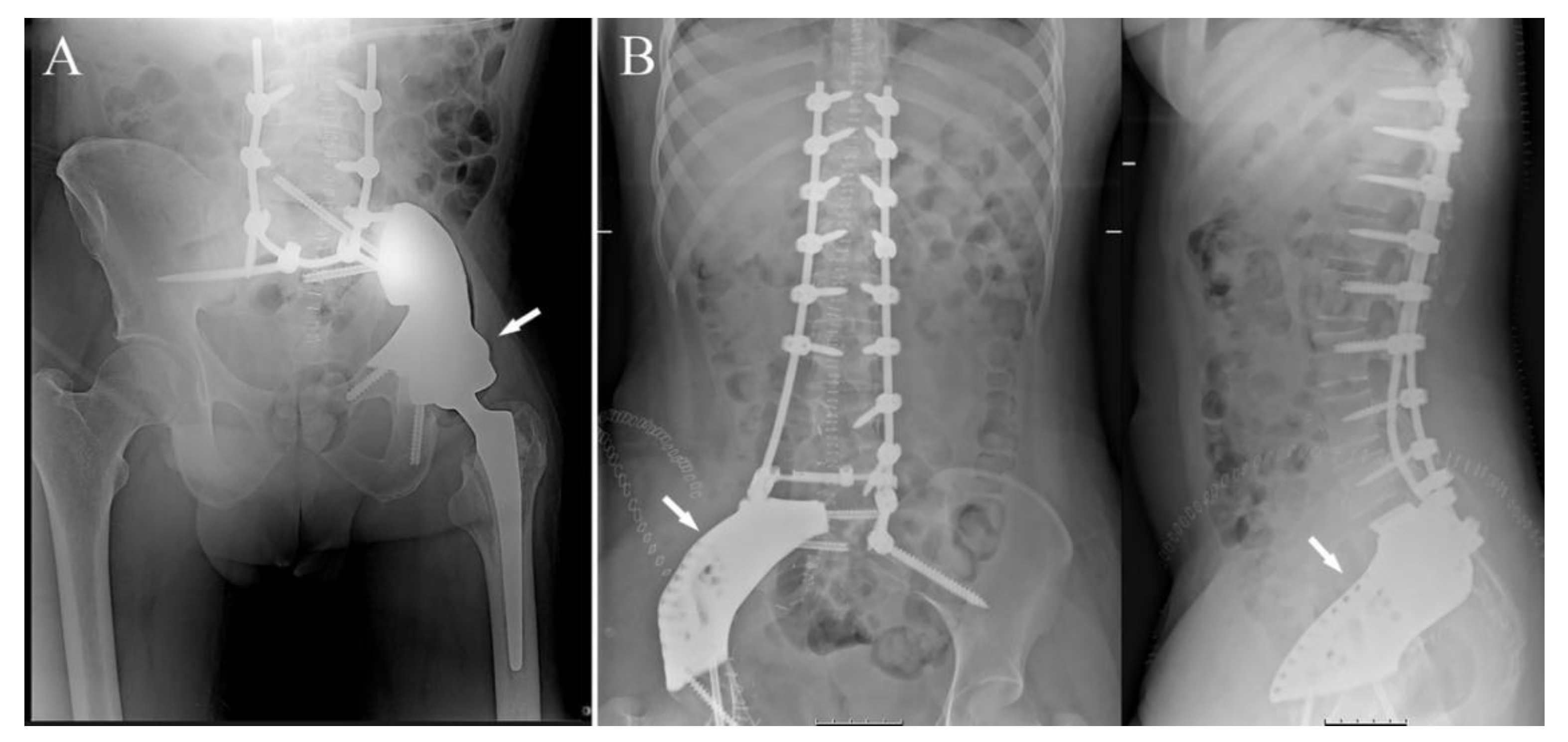
- Prosthesis shape: most prostheses were constructed trying to reproduce normal bone anatomy (Figure 4A–C). Actually, this tactic could cause problems as wound dehiscence due to skin decubitus on the prosthesis; taking this into consideration, the option of designing a low-profile prosthesis has to be taken into account (Figure 5A,B): when the tumor involves the iliac wing, the prosthesis could simply connect the sacrum-iliac joint to the hip without reproducing the iliac wing’s shape (Figure 5A,B). Currently, several prosthesis designs are proposed in the literature.
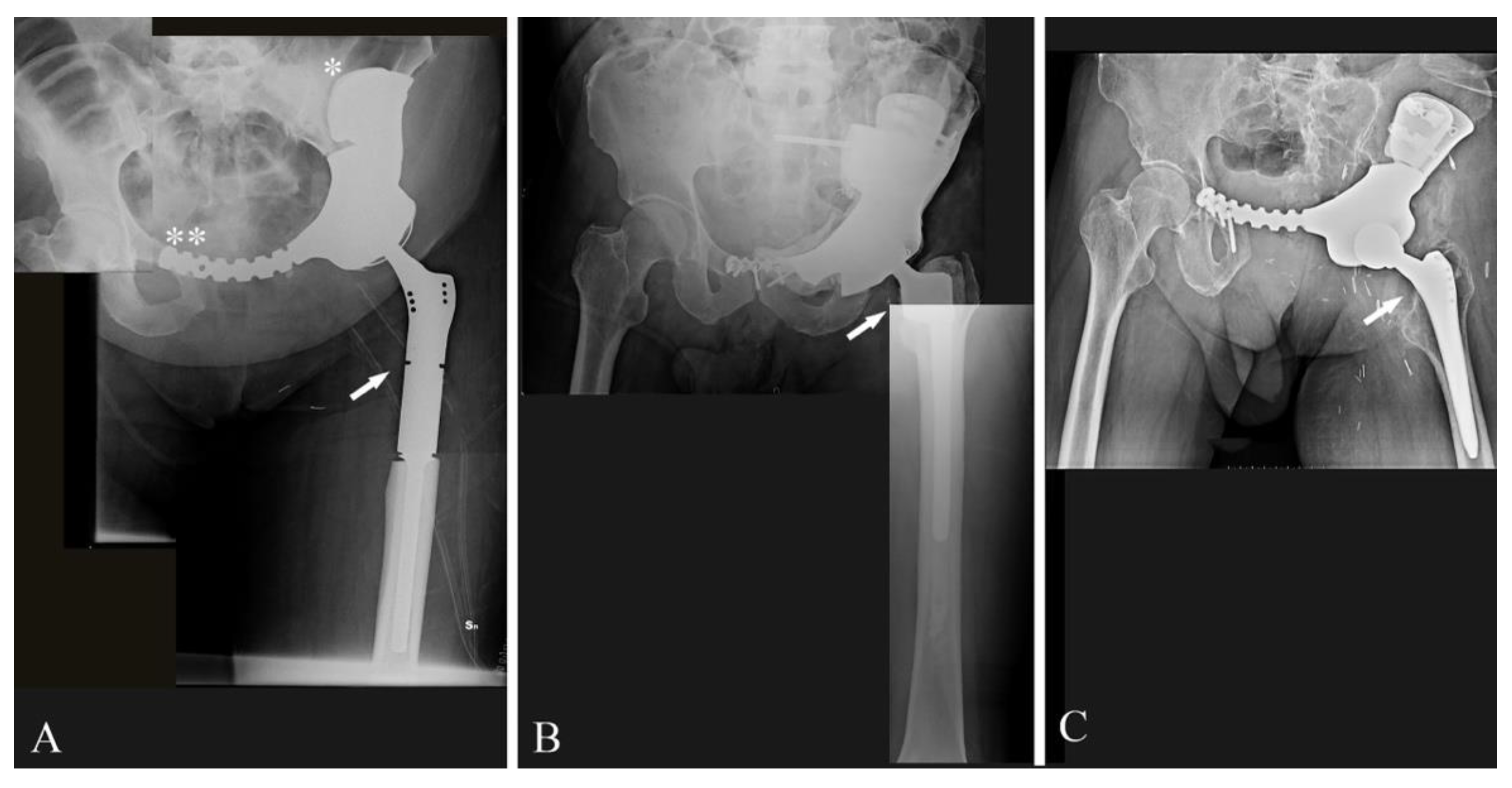
- The fixation: several solutions are possible; the first prostheses had a voluminous plate as an extension, which was fixed with screws to another independent plate on the other side of the iliac wing (“wafer fixation”) (Figure 4C); this technique could cause necrosis of the bone included between the plates, so, at present, an iliac stem is preferred to obtain primary stability, decreasing the size of the wafer fixation. In the last cases of the present series, the prostheses were produced with one or two stems which were inserted press-fit in the residual wing, obtaining a good primary stability with a probable lower damage of the bone’s vascular supply and a better osteointegration (Figure 7A). Park et al. in 2019, using a finite element analysis, showed how the shape of the plates of fixation play an important role in stress distribution. Further studies are advocated to find the best solutions [24].
- The pelvic ring restoration: several authors sustain the importance of restoring the connection between the sacrum-iliac area, the acetabulum and the symphysis [25,26]; other authors sustain a non-anatomical reconstruction [26,27]. Connection to the symphysis could be a more stable fixation at first (Figure 7B), but in the long term, this technique could increase the risk of osteolysis in the symphysis (Figure 7C) (case 3) and prosthesis loosening. Indeed, a connection with the symphysis can transfer the stress forces to the bone–prosthesis interface at the acetabular level every time that weight-bearing is on the contralateral side; contrariwise, when weight-bearing is on the side of the prosthesis, the stress forces are transmitted to the prosthesis–bone symphysis interface with hypothetical easier mobilization. Based on these concepts, connection to the symphysis has to be well evaluated; actually, a fascia lata allograft can be used to reconstruct the inguinal ligament and support the abdominal viscera when necessary (Figure 7C). The fascia lata also decreases the friction between the vessels and the prosthesis and therefore the risk of their damage, as happened in one case of our series, in which the patient died from iliac vein rupture (case 5). Instead, reconstruction of the ileo-pubic ramus has an important biomechanical value; indeed, it represents a fulcrum with the iliopsoas muscle, allowing it to act as a hip flexor; when the ileo-pubic ramus is not reconstructed, the iliopsoas collapses inside the pelvis, acting more as an adductor muscle, with a consequent loss of flexion activity. Based on these considerations, while symphysis fixation presents a rationale, ischium fixation is not recommended because it would transmit cutting forces to the bone–prosthesis interface every time the patient sits down.When the tumor also involves the Enneking and Dunham T1 and 4 areas, spine stabilization is suggested to neutralize the cutting forces that act on the prosthesis (Figure 4A,B); in these cases, a median incision is completed to perform a bilateral stabilization; bone fusion is suggested to decrease the risk of pedicle screw loosening. This surgical step can be performed during tumor removal surgery or in a second moment to decrease the impact of a massive surgery on the patient. Actually, spine stabilization could become unnecessary in the future if osteointegration improves. A possible solution to improve osteointegration could be the use of a composite prosthesis composed by a 3DPTCMP as a scaffold for a vascularized autologous bone graft as a fibular flap; in that case, the 3DPTCMP should assure primary stability, whereas the fibular flap should give osteointegration and stability without the need of spine stabilization. Recently, Lu et al. proposed a similar composite structure for diaphyseal reconstruction after bone tumor removal with good results; actually, that technique could also be suggested for reconstruction in the Enneking and Dunham T 1 and 4 areas when the acetabular roof is spared [28].
- Hip reconstruction: a prosthetic cup is cemented inside the prosthetic acetabulum. In the first cases, a constrained system was used to reduce the risk of femoral prosthesis dislocation (Figure 4A,B); later on, a dual mobility system was adopted. Indeed, constrained hip prostheses transfer traction stress forces caused by the weight of the inferior limb directly on the bone–prosthesis interface while the dual mobility system is a less rigid strategy which should guarantee a better cushioning and may be at lower risk of prosthesis failure (Figure 3E,F). Both strategies are probably effective in preventing femoral head dislocation.
4.3. Complications
4.4. Cost Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zoccali, C.; Baldi, J.; Attala, D.; Rossi, B.; Anelli, V.; Annovazzi, A.; Ferraresi, V. Intralesional vs. extralesional procedures for low-grade central chondrosarcoma: A systematic review of the literature. Arch. Orthop. Trauma Surg. 2018, 138, 929–937. [Google Scholar] [CrossRef]
- He, F.; Zhang, W.; Shen, Y.; Yu, P.; Bao, Q.; Wen, J.; Hu, C.; Qiu, S. Effects of resection margins on local recurrence of osteosarcoma in extremity and pelvis: Systematic review and meta-analysis. Int. J. Surg. 2016, 36 Pt A, 283–292. [Google Scholar] [CrossRef]
- Ozturk, A.K.; Gokaslan, Z.L.; Wolinsky, J.P. Surgical treatment of sarcomas of the spine. Curr. Treat. Options Oncol. 2014, 15, 482–492. [Google Scholar] [CrossRef]
- Rath, B.; Tingart, M.; Migliorini, F.; Eschweiler, J.; Zureik, R.; Hardes, J. Differenzierte Therapiestrategien bei Knochenmetastasen der Extremitäten [Differentiated treatment strategies for bone metastases of the extremities]. Orthopade 2019, 48, 752–759. [Google Scholar] [CrossRef]
- Grünwald, V.; Eberhardt, B.; Bex, A.; Flörcken, A.; Gauler, T.; Derlin, T.; Panzica, M.; Dürr, H.R.; Grötz, K.A.; Giles, R.H.; et al. An interdisciplinary consensus on the management of bone metastases from renal cell carcinoma. Nat. Rev. Urol. 2018, 15, 511–521. [Google Scholar] [CrossRef]
- Zeegen, E.N.; Aponte-Tinao, L.A.; Hornicek, F.J.; Gebhardt, M.C.; Mankin, H.J. Survivorship analysis of 141 modular metallic endoprostheses at early followup. Clin. Orthop. Relat. Res. 2004, 420, 239–250. [Google Scholar] [CrossRef]
- Ji, T.; Yang, Y.; Tang, X.; Liang, H.; Yan, T.; Yang, R.; Guo, W. 3D-Printed Modular Hemipelvic Endoprosthetic Reconstruction Following Periacetabular Tumor Resection: Early Results of 80 Consecutive Cases. J. Bone Jt. Surg. Am. 2020, 102, 1530–1541. [Google Scholar] [CrossRef]
- Ayvaz, M.; Bekmez, S.; Mermerkaya, M.U.; Caglar, O.; Acaroglu, E.; Tokgozoglu, A.M. Long-term results of reconstruction with pelvic allografts after wide resection of pelvic sarcomas. Sci. World J. 2014, 2014, 605019. [Google Scholar] [CrossRef] [PubMed]
- Wafa, H.; Grimer, R.J.; Jeys, L.; Abudu, A.T.; Carter, S.R.; Tillman, R.M. The use of extracorporeally irradiated autografts in pelvic reconstruction following tumour resection. Bone Jt. J. 2014, 96-B, 1404–1410. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, B.; O’Connor, M.I.; Kaufman, K.R.; Padgett, D.J.; Sim, F.H. Iliofemoral arthrodesis and pseudarthrosis: A long-term functional outcome evaluation. Clin. Orthop. Relat. Res. 2002, 397, 29–35. [Google Scholar] [CrossRef]
- Puri, A.; Gulia, A.; Jambhekar, N.; Laskar, S. The outcome of the treatment of diaphyseal primary bone sarcoma by resection; irradiation and re-implantation of the host bone: Extracorporeal irradiation as an option for reconstruction in diaphyseal bone sarcomas. J. Bone Jt. Surg. Br. 2012, 94, 982–988. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Li, J.; Li, Q.; Li, G.; Cai, Z. Clinical effectiveness of hemipelvic reconstruction using computer-aided custom-made prostheses after resection of malignant pelvic tumors. J. Arthroplast. 2011, 26, 1508–1513. [Google Scholar] [CrossRef]
- Enneking, W.F.; Dunham, W.K. Resection and reconstruction for primary neoplasms involving the innominate bone. J. Bone Jt. Surg. Am. 1978, 60, 731–746. [Google Scholar] [CrossRef]
- Enneking, W.F. A system of staging musculoskeletal neoplasm. Clin. Ortop. 1996, 204, 1383–1390. [Google Scholar] [CrossRef]
- Park, J.W.; Kang, H.G.; Kim, J.H.; Kim, H.S. New 3-dimensional implant application as an alternative to allograft in limb salvage surgery: A technical note on 10 cases. Acta Orthop. 2020, 91, 489–496. [Google Scholar] [CrossRef]
- Leaper, D.; Whitaker, I. Postoperative Complications, 2nd ed.; Oxford University Press Inc.: Oxford, UK, 2010. [Google Scholar]
- Enneking, W.F.; Dunham, W.; Gebhardt, M.C.; Malawar, M.; Pritchard, D.J. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin. Orthop. Relat. Res. 1993, 286, 241–246. [Google Scholar] [CrossRef]
- Balke, M.; Ahrens, H.; Streitbürger, A.; Gosheger, G.; Hardes, J. Modular endoprosthetic reconstruction in malignant bone tumors: Indications and limits. Recent Results Cancer Res. 2009, 179, 39–50. [Google Scholar] [CrossRef]
- Qu, H.; Li, D.; Tang, S.; Zang, J.; Wang, Y.; Guo, W. Pelvic reconstruction following resection of tumour involving the whole ilium and acetabulum. J. Bone Oncol. 2019, 16, 100234. [Google Scholar] [CrossRef]
- Ji, T.; Guo, W.; Yang, R.L.; Tang, X.D.; Wang, Y.F. Modular hemipelvic endoprosthesis reconstruction—Experience in 100 patients with mid-term follow-up results. Eur. J. Surg. Oncol. 2013, 39, 53–60. [Google Scholar] [CrossRef]
- Langlais, F.; Lambotte, J.C.; Thomazeau, H. Long-term results of hemipelvis reconstruction with allografts. Clin. Orthop. Relat. Res. 2001, 388, 178–186. [Google Scholar] [CrossRef]
- Yoshida, Y.; Osaka, S.; Mankin, H.J. Hemipelvic allograft reconstruction after periacetabular bone tumor resection. J. Orthop. Sci. 2000, 5, 198–204. [Google Scholar] [CrossRef]
- Bell, R.S.; Davis, A.M.; Wunder, J.S.; Buconjic, T.; McGoveran, B.; Gross, A.E. Allograft reconstruction of the acetabulum after resection of stage-IIB sarcoma. Intermediate-term results. J. Bone Jt. Surg. Am. 1997, 79, 1663–1674. [Google Scholar] [CrossRef]
- Liang, H.; Ji, T.; Zhang, Y.; Wang, Y.; Guo, W. Reconstruction with 3D-printed pelvic endoprostheses after resection of a pelvic tumour. Bone Jt. J. 2017, 99-B, 267–275. [Google Scholar] [CrossRef]
- Park, D.W.; Lim, A.; Park, J.W.; Lim, K.M.; Kang, H.G. Biomechanical Evaluation of a New Fixation Type in 3D-Printed Periacetabular Implants using a Finite Element Simulation. Appl. Sci. 2019, 9, 820. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Hao, Y.; Pu, F.; Jiang, W.; Shao, Z. Computer-aided designed; three dimensional-printed hemipelvic prosthesis for peri-acetabular malignant bone tumour. Int. Orthop. 2018, 42, 687–694. [Google Scholar] [CrossRef]
- Angelini, A.; Trovarelli, G.; Berizzi, A.; Pala, E.; Breda, A.; Ruggieri, P. Three-dimension-printed custom-made prosthetic reconstructions: From revision surgery to oncologic reconstructions. Int. Orthop. 2019, 43, 123–132. [Google Scholar] [CrossRef] [Green Version]
- Parrett, B.M.; Winograd, J.M.; Garfein, E.S.; Lee, W.P.A.; Hornicek, F.J.; Austen, W.G., Jr. The vertical and extended rectus abdominis myocutaneous flap for irradiated thigh and groin defects. Plast. Reconstr. Surg. 2008, 122, 171–177. [Google Scholar] [CrossRef]
- Knox, K.; Bitzos, I.; Granick, M.; Datiashvili, R.; Benevenia, J.; Patterson, F. Immediate reconstruction of oncologic hemipelvectomy defects. Ann. Plast. Surg. 2006, 57, 184–189. [Google Scholar] [CrossRef]
- Lu, Y.; Chen, G.; Long, Z.; Li, M.; Ji, C.; Wang, F.; Li, H.; Lu, J.; Wang, Z.; Li, J. Novel 3D-printed prosthetic composite for reconstruction of massive bone defects in lower extremities after malignant tumor resection. J. Bone Oncol. 2019, 16, 100220. [Google Scholar] [CrossRef]
- Lannon, D.A.; Ross, G.L.; Addison, P.D.; Novak, C.B.; Lipa, J.E.; Neligan, P.C. Versatility of the proximally pedicled anterolateral thigh flap and its use in complex abdominal and pelvic reconstruction. Plast. Reconstr. Surg. 2011, 127, 677–688. [Google Scholar] [CrossRef]
- Kallala, R.; Harris, W.E.; Ibrahim, M.; Dipane, M.; McPherson, E. Use of Stimulan absorbable calcium sulphate beads in revision lower limb arthroplasty: Safety profile and complication rates. Bone Jt. Res. 2018, 7, 570–579. [Google Scholar] [CrossRef]
- Zoccali, C.; Scoccianti, G.; Biagini, R.; Daolio, P.A.; Giardina, F.L.; Campanacci, D.A. Antibacterial hydrogel coating in joint mega-prosthesis: Results of a comparative series. Eur. J. Orthop. Surg. Traumatol. 2021, 1–9. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N° | PT | Age | Dia | G | Enn C | D&E C | SITE | M | 3DP | Loos | SS | Loos | Cup | Disl | Stem | Type | Loos | Sym Conn | Loos | Is Conn | Loos | FU | R | M | Status |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | MS,F | 58 | CS | G1 | IB | T2-T3 | pf, ace | w | yes | no | no | . | con | no | cem | 13 cm-mp | no | yes | no | res | . | 65 | no | no | NED |
| 2 | FA,F | 74 | CS | G2 | IB | T1-T4 | SIJ | w | yes | no | yes | no | . | . | . | . | . | . | . | . | . | 12 | no | no | d (heart attack with NED) |
| 3 | CC,M | 53 | CS | G3 | IIB | T2-T3 | ace, is, il-p-r | w | yes | no | no | . | con | no | cem | minimal mp | no | yes | yes | res | . | 55 | 36 | 7m (lung) | alive with lung metastasis |
| 4 | BM,M | 65 | CS | G3 | IIB | T1-T2 | ace | w | yes | no | no | . | con | no | cem | minimal mp | no | yes | no | yes | no | 11 | no | no | d (Erisipela with NED |
| 5 | CG,M | 72 | CS | G2 | IB | T2-T3 | ace, il-p-r | w | yes | no | no | . | con | no | cem | minimal mp | . | yes | no | failed | . | 2 | no | no | d (iliac vein rupture) |
| 6 | LA,F | 57 | MEH | LG | III | T2-T3 | ace, il-p-r | w | yes | no | no | . | con | no | cem | minimal mp | no | yes | no | yes | no | 50 | no | already present | d (for lung progressionw/o local disease |
| 7 | PP,M | 48 | ES | HG | IIB | T1-T2-T4 | ace, SIJ | w | yes | r | yes | r | dm | no | cem | standard | . | . | . | . | . | 40 | no | 12 (rib) | NED He is due for temporary spacer exchange with new prosthesis |
| 8 | LA,F | 50 | CS | G3 | IB | T2-T3 | ace, il-p-r | w | yes | no | no | . | dm | no | pf | standard | no | yes | yes | yes | yes | 15 | no | no | NED |
| 9 | BG,F | 15 | ES | HG | IIB | T1-T2-T3 | ace, Il, is, Il-p-r | w | yes | no | no | . | dm | no | pf | mini | no | no | . | no | . | 21 | no | no | NED |
| 10 | IM,M | 38 | CS | G3 | IIA | T2-T3 | ace, il-p-r | m | yes | no | no | . | con | no | pf | standard | no | failed | res | . | 67 | no | no | NED | |
| 11 | CAM,F | 53 | CS | G2 | IIB | T2-T3 | ace, il-p-r, is | i | yes | no | no | . | dm | no | pf | standard | no | yes | no | res | . | 49 | no | no | NED |
| 12 | FL,M | 68 | CS | G3 | IIB | T2-T3 | ace, il-p-r | w | yes | no | no | . | con | no | pf | standard | no | yes | no | res | . | 61 | no | no | NED |
| 13 | CP,F | 58 | CS | G2 | IIA | T2-T3 | ace, is | w | yes | no | no | . | dm | no | pf | standard | no | no | no | 29 | no | no | NED | ||
| 14 | KK,F | 20 | CS | MHG | IIB | T1-T4 | il, SIJ | w | yes | no | yes | no | . | . | . | . | . | . | . | . | 15 | no | no | NED |
| Epidemiology | 14 Patients (6 Males, 8 Females) |
|---|---|
| Histologies |
|
| Enneking and Dunham classification |
|
| Enneking staging | IB: 4, IIA: 2, IIB: 7; III: 1 |
| Symptoms |
|
| Surgeries |
|
| Margin | Wide: 12, Marginal: 1, Intralesional: 1 |
| Early complications: | 8 patients
|
| Late complications |
|
| Local recurrence | 1 case |
| Distant Metastasis | 3 (one already metastatic at index surgery) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zoccali, C.; Baldi, J.; Attala, D.; Scotto di Uccio, A.; Cannavò, L.; Scotto, G.; Luzzati, A. 3D-Printed Titanium Custom-Made Prostheses in Reconstruction after Pelvic Tumor Resection: Indications and Results in a Series of 14 Patients at 42 Months of Average Follow-Up. J. Clin. Med. 2021, 10, 3539. https://doi.org/10.3390/jcm10163539
Zoccali C, Baldi J, Attala D, Scotto di Uccio A, Cannavò L, Scotto G, Luzzati A. 3D-Printed Titanium Custom-Made Prostheses in Reconstruction after Pelvic Tumor Resection: Indications and Results in a Series of 14 Patients at 42 Months of Average Follow-Up. Journal of Clinical Medicine. 2021; 10(16):3539. https://doi.org/10.3390/jcm10163539
Chicago/Turabian StyleZoccali, Carmine, Jacopo Baldi, Dario Attala, Alessandra Scotto di Uccio, Luca Cannavò, Gennaro Scotto, and Alessandro Luzzati. 2021. "3D-Printed Titanium Custom-Made Prostheses in Reconstruction after Pelvic Tumor Resection: Indications and Results in a Series of 14 Patients at 42 Months of Average Follow-Up" Journal of Clinical Medicine 10, no. 16: 3539. https://doi.org/10.3390/jcm10163539
APA StyleZoccali, C., Baldi, J., Attala, D., Scotto di Uccio, A., Cannavò, L., Scotto, G., & Luzzati, A. (2021). 3D-Printed Titanium Custom-Made Prostheses in Reconstruction after Pelvic Tumor Resection: Indications and Results in a Series of 14 Patients at 42 Months of Average Follow-Up. Journal of Clinical Medicine, 10(16), 3539. https://doi.org/10.3390/jcm10163539