
High Post-Procedural Transvalvular Gradient or Delayed Mean Gradient Increase after Transcatheter Aortic Valve Implantation: Incidence, Prognosis and Associated Variables. The FRANCE-2 Registry

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
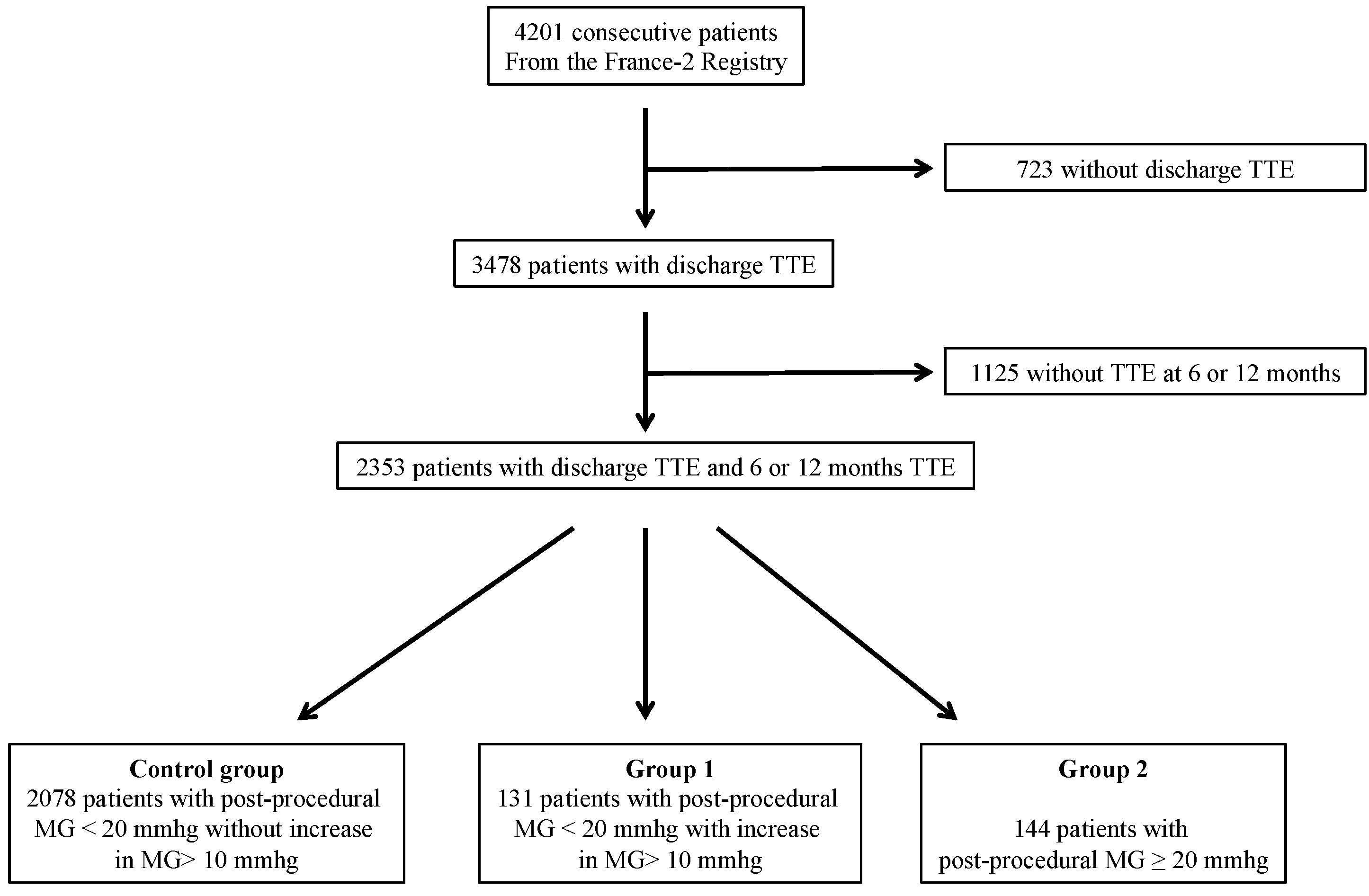
2.1. Population
2.2. Transthoracic Echocardiography (TTE) Evaluation
2.3. Follow-Up and Data Management
2.4. Statistical Analysis
3. Results
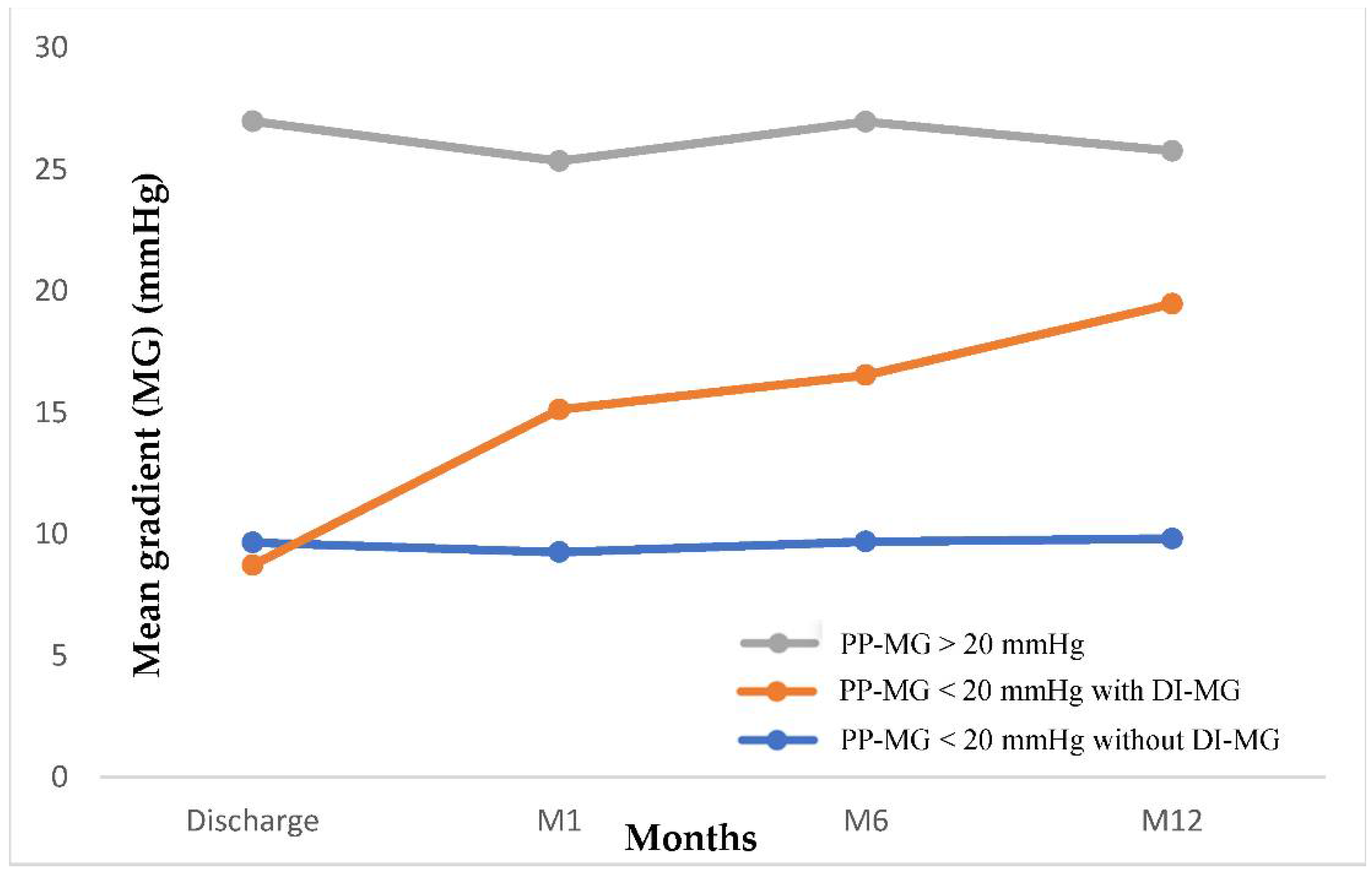
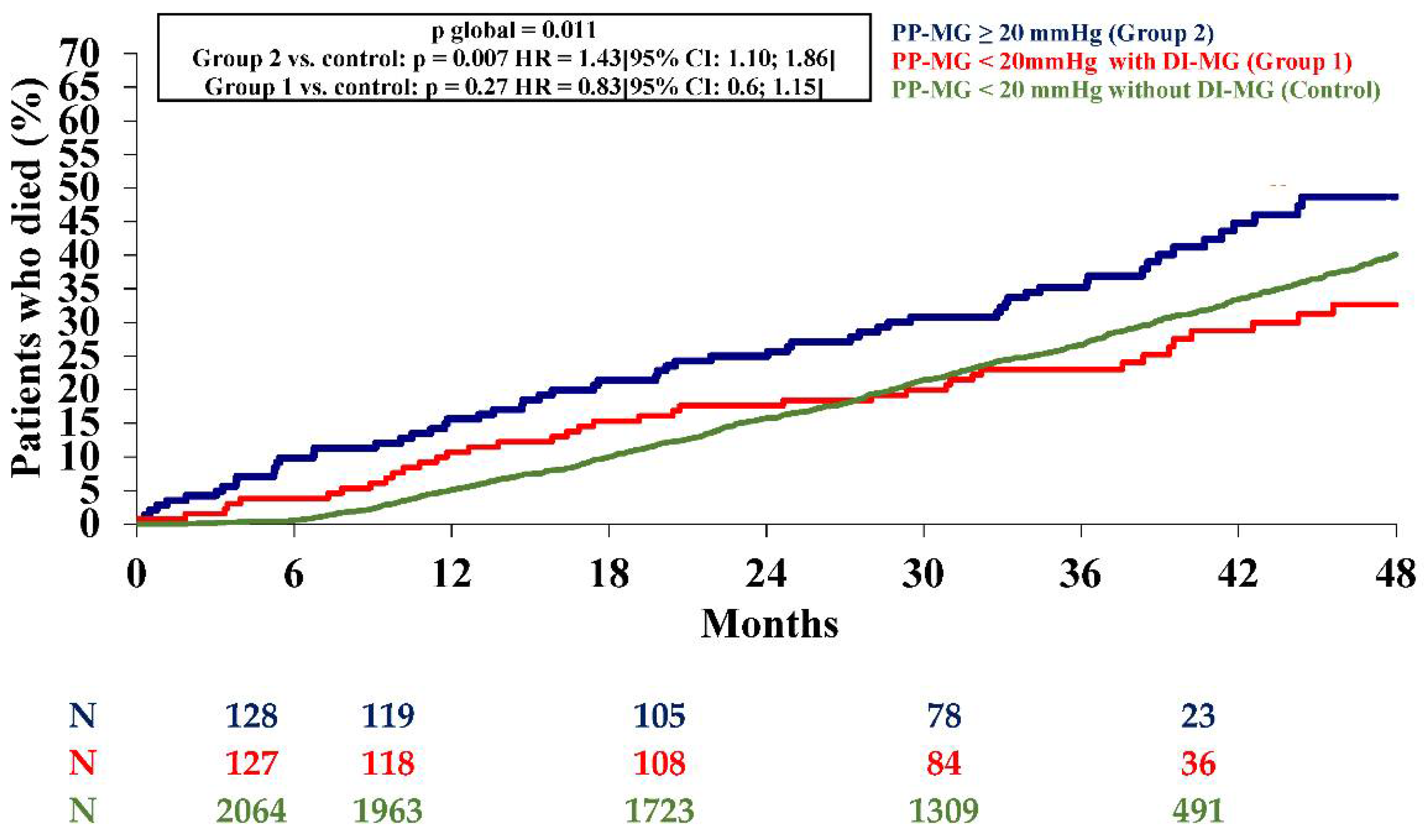
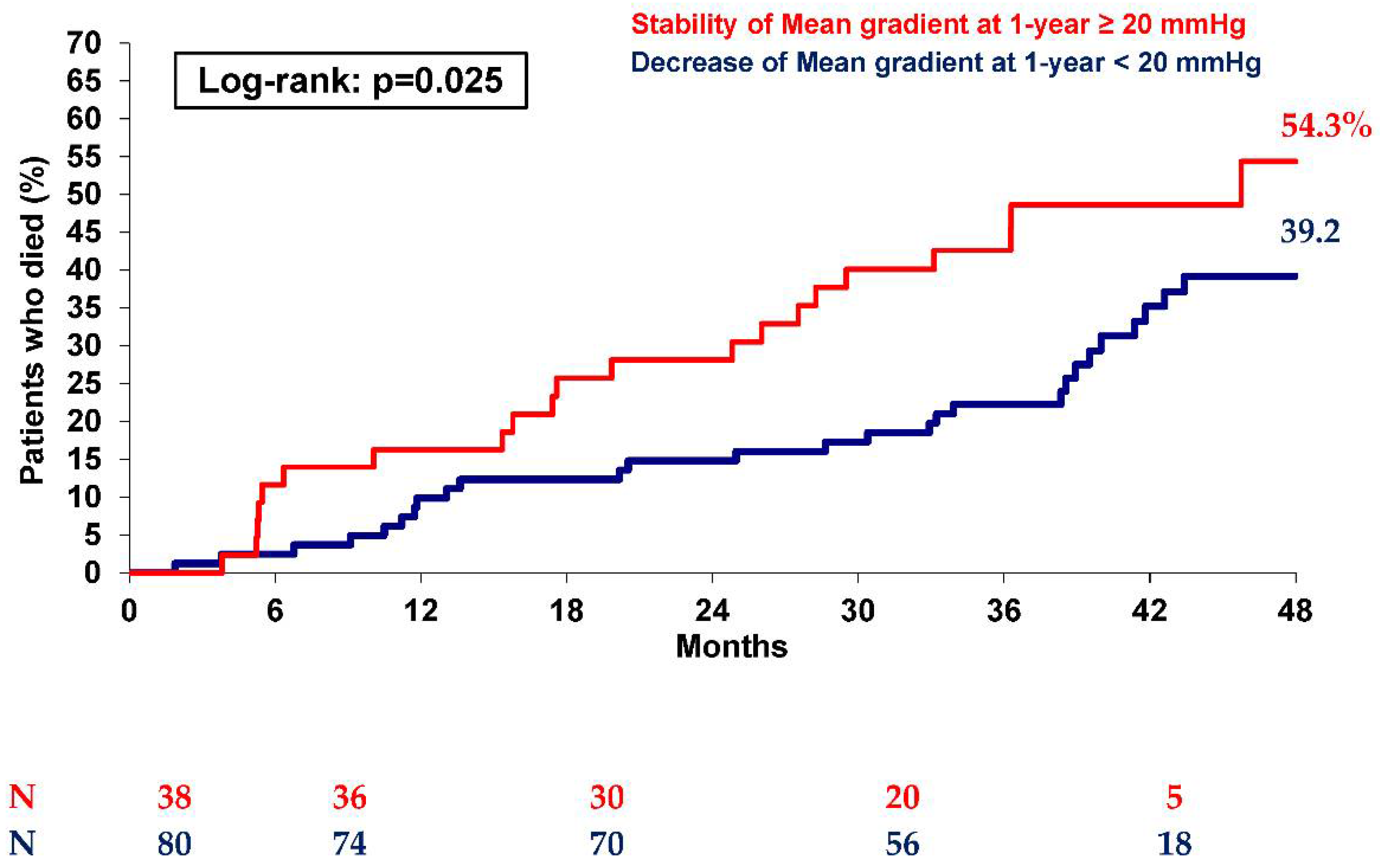
3.1. DMGI in Patients with PPMG < 20 mmHg (Group 1 versus Control Group)
3.2. Patients with PPMG ≥ 20 mmHg (Group 2 versus Control Group)
4. Discussion
4.1. DMGI in Patients with PPMG < 20 mmHg
4.2. Patients with PPMG ≥ 20 mmHg
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mack, M.J.; Leon, M.B.; Smith, C.R.; Miller, D.C.; Moses, J.W.; Tuzcu, E.M.; Webb, J.G.; Douglas, P.S.; Anderson, W.N.; Blackstone, E.H.; et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve re-placement for high surgical risk patients with aortic stenosis (PARTNER 1): A randomised controlled trial. Lancet 2015, 385, 2477–2484. [Google Scholar] [CrossRef]
- Deeb, G.M.; Reardon, M.J.; Chetcuti, S.; Patel, H.J.; Grossman, P.M.; Yakubov, S.J.; Kleiman, N.S.; Coselli, J.S.; Gleason, T.G.; Lee, J.S.; et al. 3-Year Outcomes in High-Risk Patients Who Underwent Surgical or Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2016, 67, 2565–2574. [Google Scholar] [CrossRef]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef]
- Adams, D.H.; Popma, J.J.; Reardon, M.J.; Yakubov, S.J.; Coselli, J.S.; Deeb, G.M.; Gleason, T.G.; Buchbinder, M.; Hermiller, J., Jr.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Prosthesis. N. Engl. J. Med. 2014, 370, 1790–1798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Muñoz, D.R.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J. Am. Coll. Cardiol. 2017, 136, e137–e161. [Google Scholar] [CrossRef]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef] [PubMed]
- Capodanno, D.; Petronio, A.S.; Prendergast, B.; Eltchaninoff, H.; Vahanian, A.; Modine, T.; Lancellotti, P.; Sondergaard, L.; Ludman, P.F.; Tamburino, C.; et al. Standardized definitions of structural deterioration and valve failure in assessing long-term durability of transcatheter and surgical aortic bioprosthetic valves: A consensus statement from the Euro-pean Association of Percutaneous Cardiovascular Interventions (EAPCI) endorsed by the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2017, 38, 3382–3390. [Google Scholar] [PubMed] [Green Version]
- Del Trigo, M.; Muñoz-Garcia, A.J.; Wijeysundera, H.C.; Nombela-Franco, L.; Cheema, A.N.; Gutierrez, E.; Serra, V.; Kefer, J.; Amat-Santos, I.J.; Benitez, L.M.; et al. Incidence, Timing, and Predictors of Valve Hemodynamic Deterio-ration After Transcatheter Aortic Valve Replacement: Multicenter Registry. J. Am. Coll. Cardiol. 2016, 67, 644–655. [Google Scholar] [CrossRef] [PubMed]
- Vemulapalli, S.; Holmes, D.R.; Dai, D.; Matsouaka, R.; Mack, M.J.; Grover, F.L.; Makkar, R.R.; Thourani, V.H.; Douglas, P.S. Valve hemodynamic deterioration and cardiovascular outcomes in TAVR: A report from the STS/ACC TVT Registry. Am. Heart J. 2018, 195, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Didier, R.; Eltchaninoff, H.; Donzeau-Gouge, P.; Chevreul, K.; Fajadet, J.; Leprince, P.; Leguerrier, A.; Lièvre, M.; Prat, A.; Teiger, E.; et al. Five-Year Clinical Outcome and Valve Durability after Transcatheter Aortic Valve Replacement in High-Risk Patients. Circulation 2018, 138, 2597–2607. [Google Scholar] [CrossRef] [PubMed]
- Blackman, D.J.; Saraf, S.; MacCarthy, P.A.; Myat, A.; Anderson, S.G.; Malkin, C.J.; Cunnington, M.S.; Somers, K.; Brennan, P.; Manoharan, G.; et al. Long-Term Durability of Transcatheter Aortic Valve Prostheses. J. Am. Coll. Cardiol. 2019, 73, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Gilard, M.; Eltchaninoff, H.; Iung, B.; Donzeau-Gouge, P.; Chevreul, K.; Fajadet, J.; Leprince, P.; Leguerrier, A.; Lievre, M.; Prat, A.; et al. Registry of Transcatheter Aortic-Valve Implantation in High-Risk Patients. N. Engl. J. Med. 2012, 366, 1705–1715. [Google Scholar] [CrossRef] [PubMed]
- Gilard, M.; Eltchaninoff, H.; Donzeau-Gouge, P.; Chevreul, K.; Fajadet, J.; Leprince, P.; Leguerrier, A.; Lievre, M.; Prat, A.; Teiger, E.; et al. Late Outcomes of Transcatheter Aortic Valve Replacement in High-Risk Patients: The FRANCE-2 Registry. J. Am. Coll. Cardiol. 2016, 68, 1637–1647. [Google Scholar] [CrossRef] [PubMed]
- Mooney, J.; Sellers, S.L.; Blanke, P.; Pibarot, P.; Hahn, R.T.; Dvir, D.; Douglas, P.S.; Weissman, N.J.; Kodali, S.K.; Thourani, V.H.; et al. CT-Defined Prosthesis–Patient Mismatch Downgrades Frequency and Severity, and Demonstrates No Association With Adverse Outcomes After Transcatheter Aortic Valve Replacement. JACC: Cardiovasc. Interv. 2017, 10, 1578–1587. [Google Scholar] [CrossRef] [PubMed]
- Pibarot, P.; Weissman, N.J.; Stewart, W.J.; Hahn, R.T.; Lindman, B.R.; McAndrew, T.; Kodali, S.K.; Mack, M.J.; Thourani, V.H.; Craig Miller, D.; et al. Incidence and sequelae of prosthesis-patient mismatch in transcatheter versus surgical valve replacement in high-risk patients with severe aortic stenosis: A PARTNER trial cohort—A analysis. J. Am. Coll. Cardiol. 2014, 64, 1323–1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pibarot, P.; Simonato, M.; Barbanti, M.; Linke, A.; Kornowski, R.; Rudolph, T.; Spence, M.; Moat, N.; Aldea, G.; Mennuni, M.; et al. Impact of Pre-Existing Prosthesis-Patient Mismatch on Survival Following Aor-tic Valve-in-Valve Procedures. JACC Cardiovasc. Interv. 2018, 11, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Durand, E.; Sokoloff, A.; Urena-Alcazar, M.; Chevalier, B.; Chassaing, S.; Didier, R.; Tron, C.; Litzler, P.-Y.; Bouleti, C.; Himbert, D.; et al. Assessment of Long-Term Structural Deterioration of Transcatheter Aortic Bioprosthetic Valves Using the New European Definition. Circ. Cardiovasc. Interv. 2019, 12, e007597. [Google Scholar] [CrossRef] [PubMed]
- Lindman, B.R.; Stewart, W.J.; Pibarot, P.; Hahn, R.T.; Otto, C.M.; Xu, K.; Devereux, R.B.; Weissman, N.J.; Enriquez-Sarano, M.; Szeto, W.Y.; et al. Early Regression of Severe Left Ventricular Hypertrophy After Transcatheter Aortic Valve Replacement Is Associated with Decreased Hospitalizations. JACC Cardiovasc. Interv. 2014, 7, 662–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PP-MG < 20 mmHg without DIMG (Control) n = 2078 | PP-MG < 20 mmHg with DIMG (Group 1) n = 131 | PP-MG ≥ 20 mmHg (Group 2) n = 144 | p-Value | |
|---|---|---|---|---|
| Age (year) | 82.6 ± 7.2 | 82.2 ± 6.9 | 80.5 ± 9.3 | 0.038 |
| Male sex | 1033/2078 (49.7%) | 66/131 (50.4%) | 69/144 (47.9%) | 0.903 |
| Body mass index (kg/m2) | 26.21 ± 5.00 | 26.44 ± 4.93 | 26.66 ± 5.72 | 0.752 |
| NYHA, III or IV | 1559/2078 (75.0%) | 84/131 (64.1%) | 104/144 (72.2%) | |
| Syncope | 141/2071 (6.8%) | 8/131 (6.1%) | 10/142 (7.0%) | 0.946 |
| Angina | 347/2071 (16.8%) | 14/131 (10.7%) | 21/142 (14.8%) | 0.167 |
| Hypertension | 1439/2071 (69.5%) | 78/131 (59.9%) | 113/142 (79.6%) | 0.020 |
| Diabetes | 533/2071 (25.7%) | 29/131 (22.1%) | 29/142 (20.4%) | 0.261 |
| Dyslipidaemia | 1023/2071 (49.4%) | 55/131 (42%) | 83/142 (58.5%) | 0.023 |
| Active smoking | 67/2071 (3.2%) | 1/131 (0.8%) | 7/142 (4.9%) | 0.126 |
| Coronary artery disease | 958/2029 (47.2%) | 56/129 (43.4%) | 55/138 (39.9%) | 0.187 |
| Previous CABG | 386/2071 (18.6%) | 26/131 (19.8%) | 24/142 (16.9%) | 0.816 |
| COPB | 497/2071 (24.0%) | 32/131 (24.4%) | 33/142 (23.2%) | 0.972 |
| Peripheral vascular disease | 393/2071 (19.0%) | 16/131 (12.2%) | 27/142 (19.0%) | 0.154 |
| Cerebrovascular disease | 205/2071 (9.9%) | 13/131 (9.9%) | 8/142 (5.6%) | 0.248 |
| Renal dialysis | 40/2071 (1.9%) | 2/131 (1.5%) | 4/142 (2.8%) | 0.679 |
| Logistic EuroSCORE (%) | 20.77 ± 13.28 | 20.48 ± 13.26 | 17.37 ± 11.34 | 0.017 |
| STS score (%) | 13.25 ± 10.98 | 15.52 ± 13.62 | 9.99 ± 9.77 | <0.001 |
| Atrial fibrillation | 478/2047 (23.2%) | 35/131 (26.9%) | 30/144 (21%) | 0.499 |
| Permanent pacemaker | 274/2075 (13.2%) | 21/131 (16%) | 13/143 (9.1%) | 0.220 |
| Echocardiographic findings | ||||
| LVEF (%) | 53.6 ± 13.9 | 56.3 ± 14.8 | 57.0 ± 11.9 | 0.003 |
| Mean AVG (mmHg) | 48.57 ± 15.92 | 50.64 ± 17.11 | 55.64 ± 18.62 | <0.001 |
| Indexed AVA (cm2/m2) | 0.396 ± 0.160 | 0.418 ± 0.219 | 0.380 ± 0.109 | 0.208 |
| PH (sPAP > 60 mmHg) | 295/1626 (18.1%) | 18/95 (18.9%) | 19/115 (16.5%) | 0.886 |
| Aortic regurgitation ≥ 2 | 363/1969 (18.4%) | 29/123 (23.6%) | 39/138 (28.3%) | 0.009 |
| Approach site | NA | |||
| Transfemoral | 1595/2067 (77.2%) | 95/130 (73.1%) | 112/143 (78.3%) | |
| Transapical | 316/2067 (15.3%) | 26/130 (20.0%) | 20/143 (14.0%) | |
| Transaortic or subclavian | 119/2067 (5.8%) | 6/130 (4.6%) | 9/143 (6.3%) | |
| Type of prosthesis | ||||
| Edwards | 1424/2077 (68.6%) | 97/131 (74.0%) | 94/143 (65.7%) | 0.310 |
| CoreValve | 653/2077 (31.4%) | 34/131 (26.0%) | 49/143 (34.3%) | |
| Prosthesis size | ||||
| ≤23 mm | 613/2077 (29.5%) | 48/131 (36.6%) | 65/143 (45.5%) | <0.001 |
| >23 mm | 1464/2077 (70.5%) | 83/131 (63.4%) | 78/143 (54.5%) | |
| Previous AVR surgery | 20/2071 (1.0%) | 9/131 (6.9%) | 15/142 (10.6%) | <0.001 |
| Preoperative treatment | ||||
| Aspirin | 1224/2071 (59.1%) | 67/131 (51.1%) | 83/142 (58.5%) | 0.200 |
| Clopidogrel | 634/2071 (30.6%) | 32/131 (24.4%) | 42/144 (29.6%) | 0.322 |
| VKA | 493/2071 (23.8%) | 24/131 (18.3%) | 29/144 (20.4%) | 0.250 |
| Discharge echocardiographic findings | ||||
| LEVF (%) | 56.0 ± 12.3 | 57.1 ± 12.3 | 58.9 ± 11.6 | |
| Mean AVG (mmHg) | 10.0 ± 3.4 | 8.7 ± 3.2 | 24.7 ± 7.3 | <0.001 |
| Indexed AVA (cm2/m2) | 1.054 ± 0.299 | 1.076 ± 0.256 | 0.824 ± 0.286 | |
| Post-procedural AR ≥ 2 | 293/2017 (14.5%) | 15/124 (12.1%) | 25/139 (18.0%) | 0.385 |
| PP-MG < 20 mmHg without DIMG (Control) n = 2078 | PP-MG < 20 mmHg with DIMG (Group 1) n = 131 | Univariable Analysis OR [95% CI] | p-Value | Multivariable Analysis OR [95% CI] | p-Value | |
|---|---|---|---|---|---|---|
| Age (year) | 86.2 ± 7.2 | 82.2 ± 6.9 | 0.99 [0.97; 1.02] | 0.552 | ||
| Male sex | 49.7 | 50.4 | 0.97 [0.68; 1.39] | 0.882 | ||
| Body mass index (kg/m2) | 26.2 ± 5.0 | 26.4 ± 4.9 | 1.01 [0.98; 1.04] | 0.612 | ||
| NYHA, III or IV | 75.0 | 64.1 | 0.59 [0.41; 0.86] | 0.006 | 0.56 [0.38; 0.82] | 0.0029 |
| Syncope | 7.2 | 7.0 | 0.98 [0.51; 1.88] | 0.946 | ||
| Angina | 16.8 | 10.7 | 0.59 [0.34; 1.05] | 0.072 | ||
| Hypertension | 69.5 | 59.9 | 0.65 [0.45; 0.93] | 0.018 | 0.66 [0.45; 0.96] | 0.0289 |
| Diabetes | 25.7 | 22.1 | 0.82 [0.54; 1.25] | 0.360 | ||
| Dyslipidaemia | 49.4 | 42.0 | 0.74 [0.52; 1.06] | 0.101 | ||
| Active smoking | 3.2 | 0.8 | 0.23 [0.03; 1.67] | 0.146 | ||
| Coronary artery disease | 47.2 | 43.4 | 0.86 [0.60; 1.23] | 0.402 | ||
| Logistic EuroSCORE ≥ 25 | 29.9 | 30.5 | 1.03 [0.70; 1.51] | 0.886 | ||
| Echocardiographic findings | ||||||
| LVEF (%) | 53.6 ± 13.9 | 56.3 ± 14.8 | 1.02 [1.00; 1.03] | 0.032 | ||
| Mean AVG (mmHg) | 48.57 ± 15.92 | 50.64 ± 17.11 | 1.01 [1.00; 1.02] | 0.158 | ||
| Indexed AVA (cm2/m2) | 0.40 ± 0.16 | 0.42 ± 0.22 | 1.799 [0.80; 4.06] | 0.158 | ||
| PH (sPAP > 60 mmHg) | 18.1 | 18.9 | 1.05 [0.62; 1.79] | 0.843 | ||
| Aortic regurgitation ≥ 2 | 18.4 | 23.6 | 1.37 [0.89; 2.10] | 0.157 | ||
| Procedural characteristics | ||||||
| Edwards | 68.6 | 74.0 | 1.31 [0.88; 1.95] | 0.190 | ||
| Prosthesis size > 23 mm | 70.5 | 63.4 | 0.72 [0.50; 1.05] | 0.085 | 0.54 [0.37; 0.80] | 0.0019 |
| Previous AVR surgery | 1.0 | 6.9 | 7.57 [3.37; 16.97] | <0.001 | 11.40 [4.78; 27.14] | <0.0001 |
| Preoperative treatment | ||||||
| Aspirin | 59.1 | 51.1 | 0.72 [0.51; 1.03] | 0.074 | 0.67 [0.45; 0.98] | 0.040 |
| Clopidogrel | 30.6 | 24.4 | 0.73 [0.49; 1.10] | 0.137 | 0.74 [0.47; 1.14] | 0.17 |
| VKA | 23.8 | 18.3 | 0.72 [0.46; 1.13] | 0.153 | 0.65 [0.40; 1.05] | 0.080 |
| Discharge echocardiographic findings | ||||||
| LEVF (%) | 56.0 ± 12.3 | 57.1 ± 12.3 | 1.01 [0.99; 1.02] | 0.3341 | ||
| Mean AVG (mmHg) | 10.0 ± 3.4 | 8.7 ± 3.2 | 0.89 [0.84; 0.94] | <0.0001 | 0.87 [0.81; 0.92] | <0.0001 |
| Indexed AVA (cm2/m2) | 1.05 ± 0.90 | 1.08 ± 0.26 | 1.26 [0.60; 2.65] | 0.536 | ||
| Post-procedural AR ≥ 2 | 14.5 | 12.1 | 0.81 [0.47; 1.41] | 0.455 |
| PP-MG < 20 mmHg n = 3334 | PP-MG ≥ 20 mmHg n = 144 | Univariable Analysis OR [95% CI] | p-Value | Multivariable Analysis OR [95% CI] | p-Value | |
|---|---|---|---|---|---|---|
| Age (year) | 82.9 ± 7.1 | 80.5 ± 9.3 | 0.96 [0.95; 0.98] | 0.004 | 1.73 [1.16; 2.58] | 0.007 |
| Male sex | 49.2 | 52.1 | 1.12 [0.80; 1.57] | 0.497 | ||
| Body mass index (kg/m2) | 4.9 | 10.5 | 2.29 [1.31; 4.00] | 0.004 | 2.75 [1.17; 4.03] | 0.01 |
| NYHA, III or IV | 75.1 | 72.7 | 0.89 [0.61; 1.29] | 0.526 | ||
| Syncope | 7.2 | 7.0 | 0.98 [0.51; 1.88] | 0.946 | ||
| Angina | 16.3 | 14.8 | 0.89 [0.55; 1.43] | 0.624 | ||
| Hypertension | 68.3 | 74.6 | 1.36 [0.93; 2.00] | 0.114 | ||
| Diabetes | 25.7 | 20.4 | 0.74 [0.49; 1.13] | 0.162 | ||
| Dyslipidaemia | 47.8 | 58.5 | 1.54 [1.09; 2.16] | 0.013 | 1.65 [1.12; 2.44] | 0.011 |
| Active smoking | 3.1 | 4.9 | 1.60 [0.73; 3.52] | 0.237 | ||
| Coronary artery disease | 47.0 | 39.9 | 0.75 [0.53; 1.06] | 0.100 | ||
| Logistic EuroSCORE ≥ 25 | 31.2 | 18.2 | 0.49 [0.32; 0.76] | <0.001 | 0.40 [0.24; 0.68] | 0.0007 |
| Echocardiographic findings | ||||||
| LVEF (%) | 53.1 ± 14.2 | 57.0 ± 11.9 | 1.01 [1.01; 1.03] | 0.0012 | ||
| Mean AVG (mmHg) | 48.05 ± 16.11 | 55.64 ± 18.62 | 1.03 [1.01; 1.03] | <0.0001 | 1.03 [1.02; 1.04] | 0.0003 |
| Indexed AVA (cm2/m2) | 0.398 ± 0.169 | 0.380 ± 0.109 | 0.359 [0.08; 1.73] | 0.202 | ||
| PH (sPAP > 60 mmHg) | 18.6 | 16.5 | 0.87 [0.53; 1.43] | 0.582 | ||
| Aortic regurgitation ≥ 2 | 17.7 | 28.3 | 1.84 [1.25; 2.69] | 0.002 | ||
| Procedural characteristics | ||||||
| Edwards | 66.3 | 65.7 | 0.97 [0.68; 1.39] | 0.883 | ||
| Prosthesis size > 23 mm | 72.0 | 54.5 | 0.47 [0.33; 0.66] | <0.001 | 0.43 [0.30; 0.64] | <0.0001 |
| Previous AVR surgery | 1.5 | 10.6 | 8.60 [4.67; 15.84] | <0.001 | 21.38 [9.94; 45.99] | <0.0001 |
| Preoperative treatment | ||||||
| Aspirin | 57.7 | 58.5 | 1.07 [0.73; 1.45] | 0.869 | 1.08 [0.72; 1.60] | 0.74 |
| Clopidogrel | 29.2 | 29.6 | 1.02 [0.71; 1.47] | 0.914 | ||
| VKA | 23.8 | 20.4 | 0.82 [0.54; 1.25] | 0.354 | 0.87 [0.53; 1.42] | 0.57 |
| Discharge echocardiographic findings | ||||||
| LEVF (%) | 55.4 ± 12.6 | 58.9 ± 11.6 | 1.02 [1.01; 1.04] | 0.0019 | ||
| Mean AVG (mmHg) | 9.8 ± 3.4 | 24.7 ± 7.3 | 26.70 [9.26; 76.97] | <0.0001 | ||
| Indexed AVA (cm2/m2) | 1.054 ± 0.288 | 0.824 ± 0.286 | 0.024 [0.01; 0.06] | <0.0001 | ||
| Post-procedural AR ≥ 2 | 14.8 | 18.0 | 1.26 [0.81; 1.97] | 0.302 |
| Decrease of the MG over Year < 20 mmHg n = 83 | Stability of the MG over Year ≥ 20 mmHg n = 43 | p-Value | |
|---|---|---|---|
| Age (year) | 80.8 ± 9.0 | 78.7 ± 10.4 | 0.260 |
| Male sex | 36/83 (43.4%) | 25/43 (58.1%) | 0.116 |
| Body mass index (kg/m2) | 26.03 ± 5.62 | 27.97 ± 6.09 | 0.042 |
| NYHA, III or IV | 56/83 (67.5%) | 36/43 (83.7%) | 0.051 |
| Syncope | 8/83 (9.6%) | 0/43 (0%) | 0.050 |
| Hypertension | 62/83 (74.7%) | 32/43 (74.4%) | 0.973 |
| Diabetes | 11/83 (13.3%) | 15/43 (34.9%) | 0.004 |
| Dyslipidaemia | 46/83 (55.4%) | 29/43 (67.4%) | 0.192 |
| Active smoking | 4/83 (4.8%) | 3/43 (7.0%) | 0.689 |
| Coronary artery disease | 32/83 (38.6%) | 16/43 (37.2%) | 0.883 |
| Previous CABG | 10/83 (12.0%) | 14/43 (32.6%) | 0.005 |
| COPB | 16/83 (19.8%) | 14/43 (32.6%) | 0.097 |
| Peripheral vascular disease | 18/83 (21.7%) | 7/43 (16.3%) | 0.470 |
| Cerebrovascular disease | 7/83 (8.4%) | 0/43 (0%) | 0.094 |
| Renal dialysis | 2/83 (2.4%) | 1/43 (2.3%) | 1 |
| Logistic EuroSCORE (%) | 15.72 ± 9.86 | 20.37 ± 11.97 | 0.033 |
| STS score (%) | 9.37 ± 8.8 | 9.69 ± 9.78 | 0.895 |
| Atrial fibrillation | 18/83 (21.7%) | 7/43 (16.3%) | 0.470 |
| Permanent pacemaker | 5/83 (6.0%) | 6/43 (14.0%) | 0.135 |
| Echocardiographic findings | |||
| LVEF (%) | 56.1 ± 11.7 | 57.5 ± 11.3 | 0.621 |
| Mean AVG (mmHg) | 56.80 ± 19.65 | 54.07 ± 17.01 | 0.442 |
| Indexed AVA (cm2/m2) | 0.384 ± 0.107 | 0.370 ± 0.098 | 0.681 |
| PH (sPAP > 60 mmHg) | 11/67 (16.4%) | 7/37 (18.9%) | 0.747 |
| Aortic regurgitation ≥ 2 | 25/79 (31.6%) | 11/42 (26.2%) | 0.532 |
| Approach site | NA | ||
| Transfemoral | 63/83 (75.9%) | 36/43 (83.7%) | |
| Transapical | 13/83 (15.7%) | 4/43 (9.3%) | |
| Transaortic or subclavian | 7/83 (8.4%) | 3/43 (7.0%) | |
| Type of prosthesis | |||
| Edwards | 56/83 (67.5%) | 26/43 (60.5%) | 0.434 |
| CoreValve | 27/83 (32.5%) | 17/43 (39.5%) | |
| Prosthesis size | |||
| ≤23 mm | 39/83 (47.0%) | 21/43 (48.8%) | 0.844 |
| >23 mm | 44/83 (53%) | 22/43 (51.2%) | |
| Previous AVR surgery | 1/83 (1.2%) | 13/43 (30.2%) | <0.001 |
| Preoperative treatment | |||
| Aspirin | 47/83 (56.6%) | 26/43 (60.5%) | 0.679 |
| Clopidogrel | 23/83 (31.3%) | 9/43 (20.9%) | 0.217 |
| VKA | 15/83 (18.1%) | 9/43 (20.9%) | 0.698 |
| Discharge echocardiographic findings | |||
| LEVF (%) | 59.2 ± 10.7 | 59.3 ± 12.2 | 0.816 |
| Mean AVG (mmHg) | 22.8 ± 3.1 | 27.0 ± 6.4 | <0.001 |
| Indexed AVA (cm2/m2) | 0.901 ± 0.276 | 0.665 ± 0.216 | <0.001 |
| Post-procedural AR ≥ 2 | 19/81 (23.5%) | 4/40 (10.0%) | 0.089 |
| 6-month echocardiographic findings | |||
| LEVF (%) | 56.6 ± 13.2 | 62.3 ± 11.5 | 0.035 |
| Mean AVG (mmHg) | 12.6 ± 4.6 | 26.9 ± 15.1 | <0.001 |
| Indexed AVA (cm2/m2) | 1.003 ± 0.297 | 0.923 ± 0.418 | 0.297 |
| Post-procedural AR ≥ 2 | 15/65 (24.2%) | 4/26 (16.7%) | 0.569 |
| 1 year echocardiographic findings | |||
| LEVF (%) | 56.2 ± 11.2 | 60.9 ± 9.3 | 0.066 |
| Mean AVG (mmHg) | 13.0 ± 4.1 | 25.7 ± 9.7 | <0.001 |
| Indexed AVA (cm2/m2) | 0.917 ± 0.264 | 0.802 ± 0.228 | 0.195 |
| Post-procedural AR ≥ 2 | 10/62 (16.7%) | 3/26 (12.0%) | 0.747 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Didier, R.; Benic, C.; Nasr, B.; Le Ven, F.; Hannachi, S.; Eltchaninoff, H.; Koifman, E.; Donzeau-Gouge, P.; Fajadet, J.; Leprince, P.; et al. High Post-Procedural Transvalvular Gradient or Delayed Mean Gradient Increase after Transcatheter Aortic Valve Implantation: Incidence, Prognosis and Associated Variables. The FRANCE-2 Registry. J. Clin. Med. 2021, 10, 3221. https://doi.org/10.3390/jcm10153221
Didier R, Benic C, Nasr B, Le Ven F, Hannachi S, Eltchaninoff H, Koifman E, Donzeau-Gouge P, Fajadet J, Leprince P, et al. High Post-Procedural Transvalvular Gradient or Delayed Mean Gradient Increase after Transcatheter Aortic Valve Implantation: Incidence, Prognosis and Associated Variables. The FRANCE-2 Registry. Journal of Clinical Medicine. 2021; 10(15):3221. https://doi.org/10.3390/jcm10153221
Chicago/Turabian StyleDidier, Romain, Clément Benic, Bahaa Nasr, Florent Le Ven, Sinda Hannachi, Hélène Eltchaninoff, Edward Koifman, Patrick Donzeau-Gouge, Jean Fajadet, Pascal Leprince, and et al. 2021. "High Post-Procedural Transvalvular Gradient or Delayed Mean Gradient Increase after Transcatheter Aortic Valve Implantation: Incidence, Prognosis and Associated Variables. The FRANCE-2 Registry" Journal of Clinical Medicine 10, no. 15: 3221. https://doi.org/10.3390/jcm10153221
APA StyleDidier, R., Benic, C., Nasr, B., Le Ven, F., Hannachi, S., Eltchaninoff, H., Koifman, E., Donzeau-Gouge, P., Fajadet, J., Leprince, P., Leguerrier, A., Lièvre, M., Prat, A., Teiger, E., Lefevre, T., Cuisset, T., Le Breton, H., Auffret, V., Iung, B., & Gilard, M. (2021). High Post-Procedural Transvalvular Gradient or Delayed Mean Gradient Increase after Transcatheter Aortic Valve Implantation: Incidence, Prognosis and Associated Variables. The FRANCE-2 Registry. Journal of Clinical Medicine, 10(15), 3221. https://doi.org/10.3390/jcm10153221