
Efficacy of Modified Treat-and-Extend Regimen of Aflibercept for Macular Edema from Branch Retinal Vein Occlusion: 2-Year Prospective Study Outcomes

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Patients and Ophthalmological Examination
2.3. mTAE Regimen
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
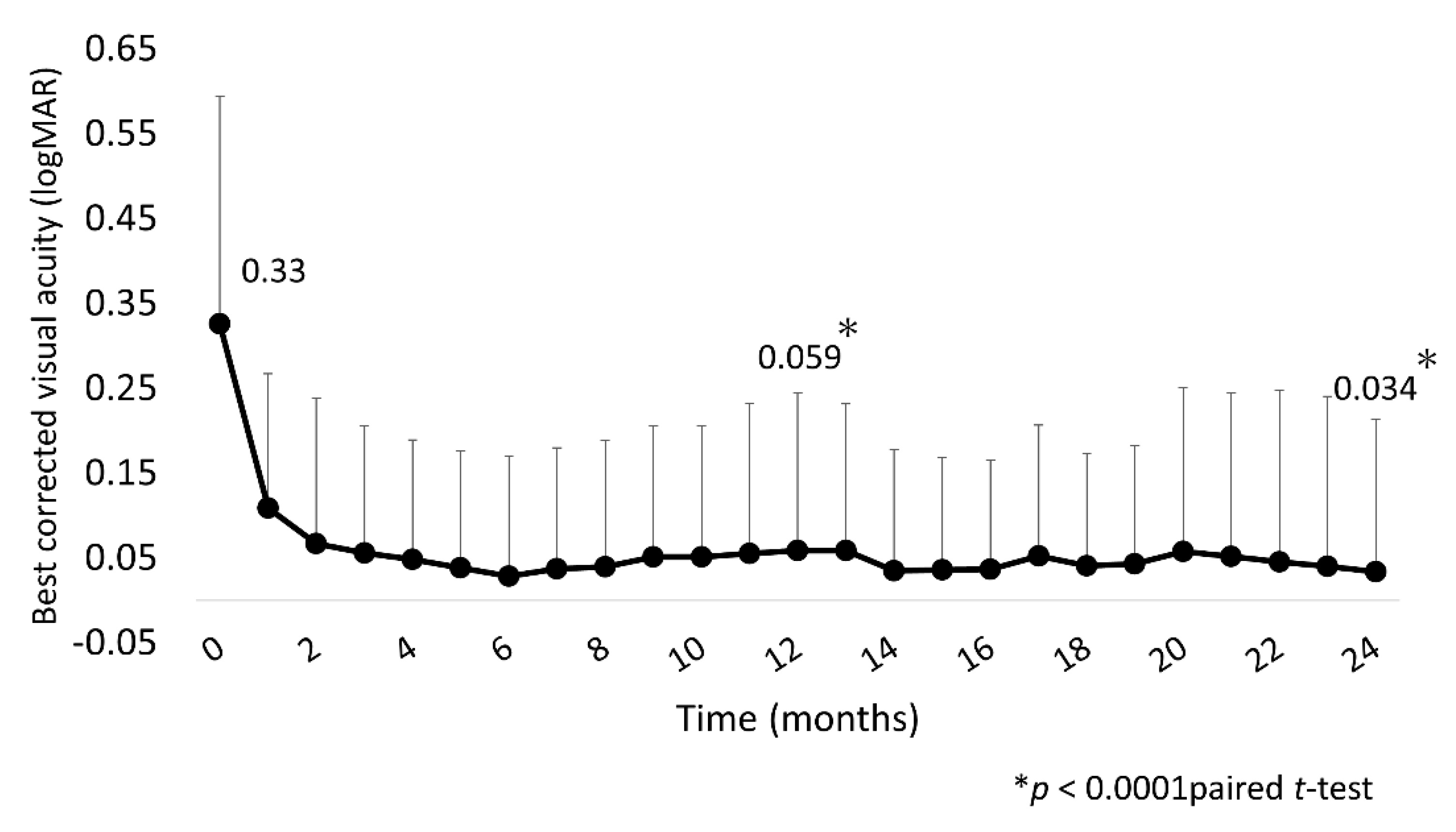
3.2. BCVA and CST Outcomes
3.3. IVA Injections and Clinic Visits
3.4. Time to First Recurrence from First Injection
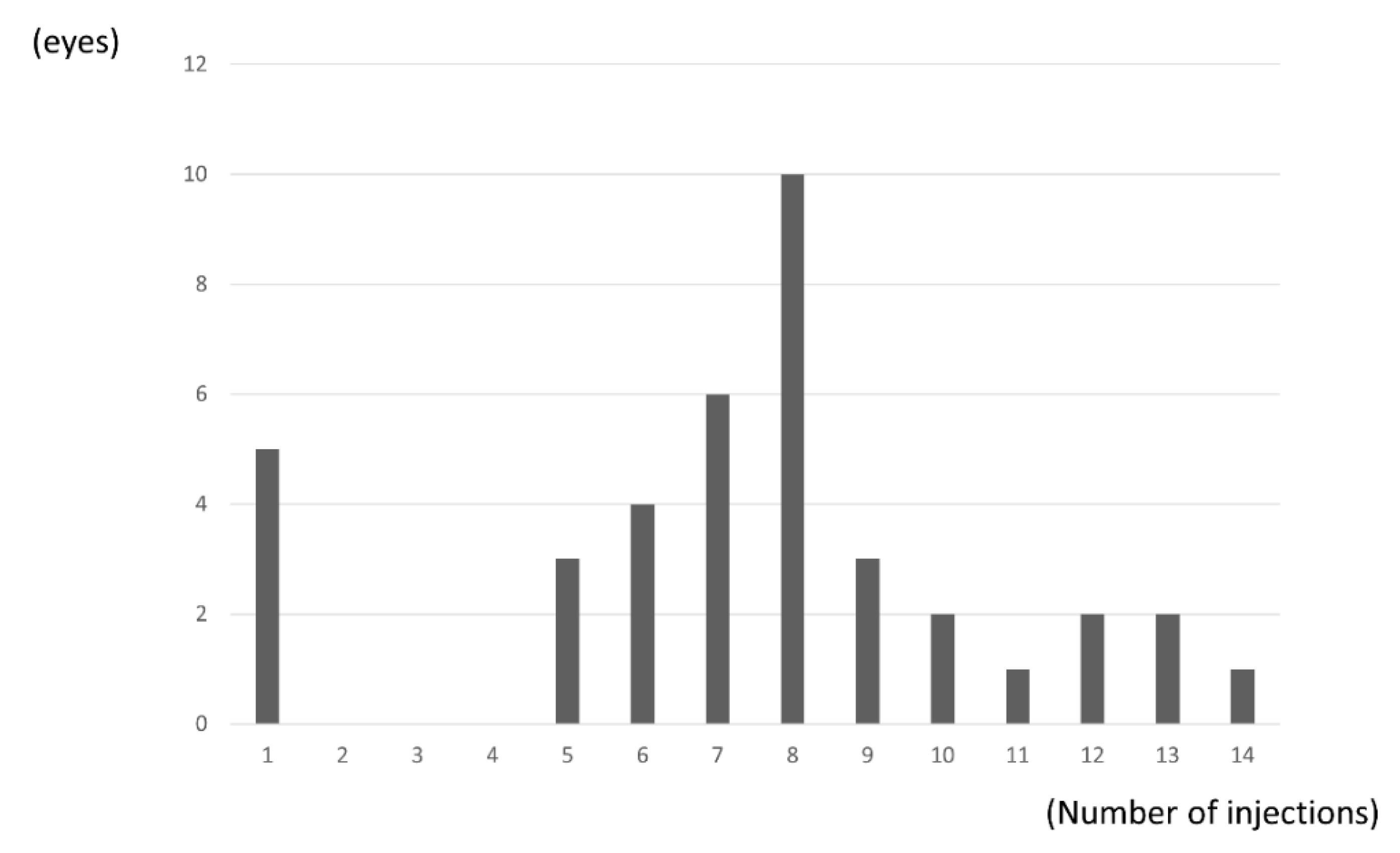
3.5. Injection Frequency
3.6. Major and Macular BRVO
3.7. Safety over the 24 Months
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rogers, S.; McIntosh, R.L.; Cheung, N.; Lim, L.; Wang, J.J.; Mitchell, P.; Kowalski, J.W.; Nguyen, H.; Wong, T.Y. International Eye Disease Consortium. The prevalence of retinal vein occlusion: Pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology 2010, 117, 313–319. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, M.; Kiyohara, Y.; Arakawa, S.; Hata, Y.; Yonemoto, K.; Doi, Y.; Iida, M.; Ishibashi, T. Prevalence and systemic risk factors for retinal vein occlusion in a general Japanese population: The Hisayama study. Investig. Ophthalmol. Vis. Sci. 2010, 51, 3205–3209. [Google Scholar] [CrossRef] [Green Version]
- Mitry, D.; Bunce, C.; Charteris, D. Anti-vascular endothelial growth factor for macular oedema secondary to branch retinal vein occlusion. Cochrane Database Syst. Rev. 2013, 2013, 009510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuppermann, B.D.; Blumenkranz, M.S.; Haller, J.A.; Williams, G.A.; Weinberg, C.C.; Whitcup, S.M.; Dexamethasone, D.D.S. Phase II Study Group. Randomized controlled study of an intravitreous dexamethasone drug delivery system in patients with persistent macular edema. Arch. Ophthalmol. 2007, 125, 309–317. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Hafiz, G.; Shah, S.M.; Nguyen, Q.D.; Ying, H.; Do, D.V.; Quinlan, E.; Zimmer-Galler, I.; Haller, J.A.; Solomon, S.D.; et al. Ranibizumab for macular edema due to retinal vein occlusions: Implication of VEGF as a critical stimulator. Mol. Ther. 2008, 16, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Campochiaro, P.A.; Brown, D.M.; Awh, C.C.; Lee, S.Y.; Gray, S.; Saroj, N.; Murahashi, W.Y.; Rubio, R.G. Sustained benefits from ranibizumab for macular edema following branch retinal vein occlusion: 12-month outcomes of a phase III study. Ophthalmology 2011, 118, 1594–1602. [Google Scholar] [CrossRef]
- Tadayoni, R.; Waldstein, S.M.; Boscia, F.; Gerding, H.; Pearce, I.; Priglinger, S.; Wenzel, A.; Barnes, E.; Gekkieva, M.; Pilz, S.; et al. Individualized stabilization criteria-driven ranibizumab versus laser in branch retinal vein occlusion: Six-month results of BRIGHTER. Ophthalmology 2016, 123, 1332–1344. [Google Scholar] [CrossRef] [Green Version]
- Miwa, Y.; Muraoka, Y.; Osaka, R.; Ooto, S.; Murakami, T.; Suzuma, K.; Takahashi, A.; Iida, Y.; Yoshimura, N.; Tsujikawa, A. Ranibizumab for macular edema after branch retinal vein occlusion. Retina 2017, 37, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Campochiro, P.A.; Sophie, R.; Pearlman, J.; Brown, D.M.; Boyer, D.S.; Heier, J.S.; Marcus, D.M.; Feiner, L.; Patel, A.; RETAIN Study Group. Long-term outcomes inpatients with retinal vein occlusion treated with ranibizumab. The RETAIN study. Ophthalmology 2014, 121, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Ang, J.L.; Moye, S.A.; Kim, L.N.; Nguyen, V.; Hunt, A.; Barthelmes, D.; Gillies, M.C.; Mehta, H. A systematic review of real-world evidence of the management of macular oedema secondary to branch retinal vein occlusion. Eye (Lond.) 2020, 34, 1770–1796. [Google Scholar] [CrossRef]
- Arai, Y.; Takahashi, H.; Inoda, S.; Sakamoto, S.; Tan, X.; Inlue, Y.; Tominaga, S.; Kawashima, H.; Yanagi, Y. Efficacy of modified treat-and-extend aflibercept regimen for macular edema due to branch retinal vein occlusion: 1-year prospective study. J. Clin. Med. 2020, 239, 2360. [Google Scholar] [CrossRef] [PubMed]
- Hayreh, S.S.; Zimmerman, M.B. Fundus changes in branch retinal vein occlusion. Retina 2015, 35, 1016–1027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, W.L.; Boyer, D.S.; Heier, J.S.; Brown, D.M.; Haller, J.A.; Vitti, R.; Kazmi, H.; Berliner, A.J.; Erickson, K.; Chu, K.W.; et al. Intravitreal aflibercept for macular edema following branch retinal vein occlusion: 52-week results of the VIBRANT study. Ophthalmology 2016, 123, 330–336. [Google Scholar] [CrossRef]
- Tadayoni, R.; Waldstein, S.M.; Boscia, F.; Gerding, H.; Gekkieva, M.; Barnes, E.; Gupta, A.D.; Wenzel, A.; Pearce, I.; BRIGHTER Study Group. Sustained benefits of ranibizumab with or without laser in branch retinal vein occlusion. 24-month results of the BRIGHTER study. Ophthalmology 2017, 124, 1778–1787. [Google Scholar] [CrossRef] [Green Version]
- Chatziralli, I.; Theodossiadis, G.; Chatzirallis, A.; Parikakis, E.; Mitropoulos, P.; Theodossiadis, P. Ranibizumab for retinal vein occulusion: Predictive factors and long-term outcomes in real-life data. Retina 2018, 38, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.H.; Downey, L.; Devonport, H.; Gale, R.P.; Kotagiri, A.; Mahmood, S.; Mehta, H.; Narendran, N.; Patel, P.J.; Parmar, N.; et al. Recommendation by a UK expert panel on an aflibercept treat-and-extend pathway for the treatment of neovascular age-related macular degeneration. Eye (Lond.). 2020, 34, 1825–1834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogura, Y.; Kondo, M.; Kadonosono, K.; Shimura, M.; Kamei, M.; Tshujikawa, A. Current practice in the management of branch retinal vein occlusion in Japan: Survey results of retina specialists in Japan. Jpn. J. Ophthalmol. 2016, 63, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Haller, J.A.; Bandello, F.; Belfort, R., Jr.; Blumenkranz, M.S.; Gillies, M.; Heier, J.; Loewenstein, A.; Yoon, Y.H.; Jacques, M.L.; Jiao, J.; et al. Randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology 2010, 117, 1134–1146. [Google Scholar] [CrossRef]
- Sakimoto, S.; Kamei, M.; Sakaguchi, H.; Suzuki, M.; Matsumura, N.; Nishida, K.; Nishida, K. Direct photocoagulation to leakage points to treat chronic macular edema associated with branch retinal vein occlusion: A pilot study. Clin. Ophthalmol. 2014, 7, 2055–2060. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Li, Y.; Fang, S.F.; Wang, H. Efficacy of intravitreal lucentis injection on major and macular branch retinal vein occlusion. BMC Ophthalmol. 2020, 20, 274. [Google Scholar] [CrossRef]
- Tao, Y.; Huang, C.; Liu, M.; Sun, L.; Li, L.; Wei, Y.; Yu, X.; Wang, H. Short-term effect of intravitreal conbercept injection on major and macular branch retinal vein occlusion. J. Int. Med. Res. 2019, 47, 1202–1209. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cases | 50 |
|---|---|
| Age (years; mean ± SD) | 66 ± 12 |
| Sex (male/female) | 24/26 |
| BCVA (logMAR; mean ± SD) | 0.33 ± 0.27 |
| CMT (µm; mean ± SD) | 488 ± 171 |
| Major BRVO (n = 25) | Macular BRVO (n = 14) | p-Value * | |
|---|---|---|---|
| Baseline BCVA (logMAR; mean ± SD ) | 0.33 ± 0.26 | 0.30 ± 0.30 | 0.68 |
| Baseline CRT (µm; mean ± SD) | 509 ± 161 | 477 ± 191 | 0.28 |
| BCVA at month 24 (logMAR; mean ± SD) | 0.0017 ± 0.14 | −0.026 ± 0.074 | 0.15 |
| CRT at month 24 (µm; mean ± SD) | 257 ± 52 | 259 ± 70 | 0.94 |
| Mean number of injections (times; mean ± SD) | 7.52 ± 3.57 | 7.07 ± 2.97 | 0.69 |
| Mean number of visits (times; mean ± SD) | 11.32 ± 2.19 | 10.64 ± 1.55 | 0.31 |
| Duration between symptoms and initial therapy (month; mean ± SD) | 1.46 ± 1.55 | 3.26 ± 3.76 | 0.041 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arai, Y.; Takahashi, H.; Inoda, S.; Sakamoto, S.; Tan, X.; Inoue, Y.; Tominaga, S.; Kawashima, H.; Yanagi, Y. Efficacy of Modified Treat-and-Extend Regimen of Aflibercept for Macular Edema from Branch Retinal Vein Occlusion: 2-Year Prospective Study Outcomes. J. Clin. Med. 2021, 10, 3162. https://doi.org/10.3390/jcm10143162
Arai Y, Takahashi H, Inoda S, Sakamoto S, Tan X, Inoue Y, Tominaga S, Kawashima H, Yanagi Y. Efficacy of Modified Treat-and-Extend Regimen of Aflibercept for Macular Edema from Branch Retinal Vein Occlusion: 2-Year Prospective Study Outcomes. Journal of Clinical Medicine. 2021; 10(14):3162. https://doi.org/10.3390/jcm10143162
Chicago/Turabian StyleArai, Yusuke, Hidenori Takahashi, Satoru Inoda, Shinichi Sakamoto, Xue Tan, Yuji Inoue, Satoko Tominaga, Hidetoshi Kawashima, and Yasuo Yanagi. 2021. "Efficacy of Modified Treat-and-Extend Regimen of Aflibercept for Macular Edema from Branch Retinal Vein Occlusion: 2-Year Prospective Study Outcomes" Journal of Clinical Medicine 10, no. 14: 3162. https://doi.org/10.3390/jcm10143162
APA StyleArai, Y., Takahashi, H., Inoda, S., Sakamoto, S., Tan, X., Inoue, Y., Tominaga, S., Kawashima, H., & Yanagi, Y. (2021). Efficacy of Modified Treat-and-Extend Regimen of Aflibercept for Macular Edema from Branch Retinal Vein Occlusion: 2-Year Prospective Study Outcomes. Journal of Clinical Medicine, 10(14), 3162. https://doi.org/10.3390/jcm10143162