
Grip Strength Correlates with Mental Health and Quality of Life after Critical Care: A Retrospective Study in a Post-Intensive Care Syndrome Clinic

 , ,
, ,
Abstract
:1. Introduction
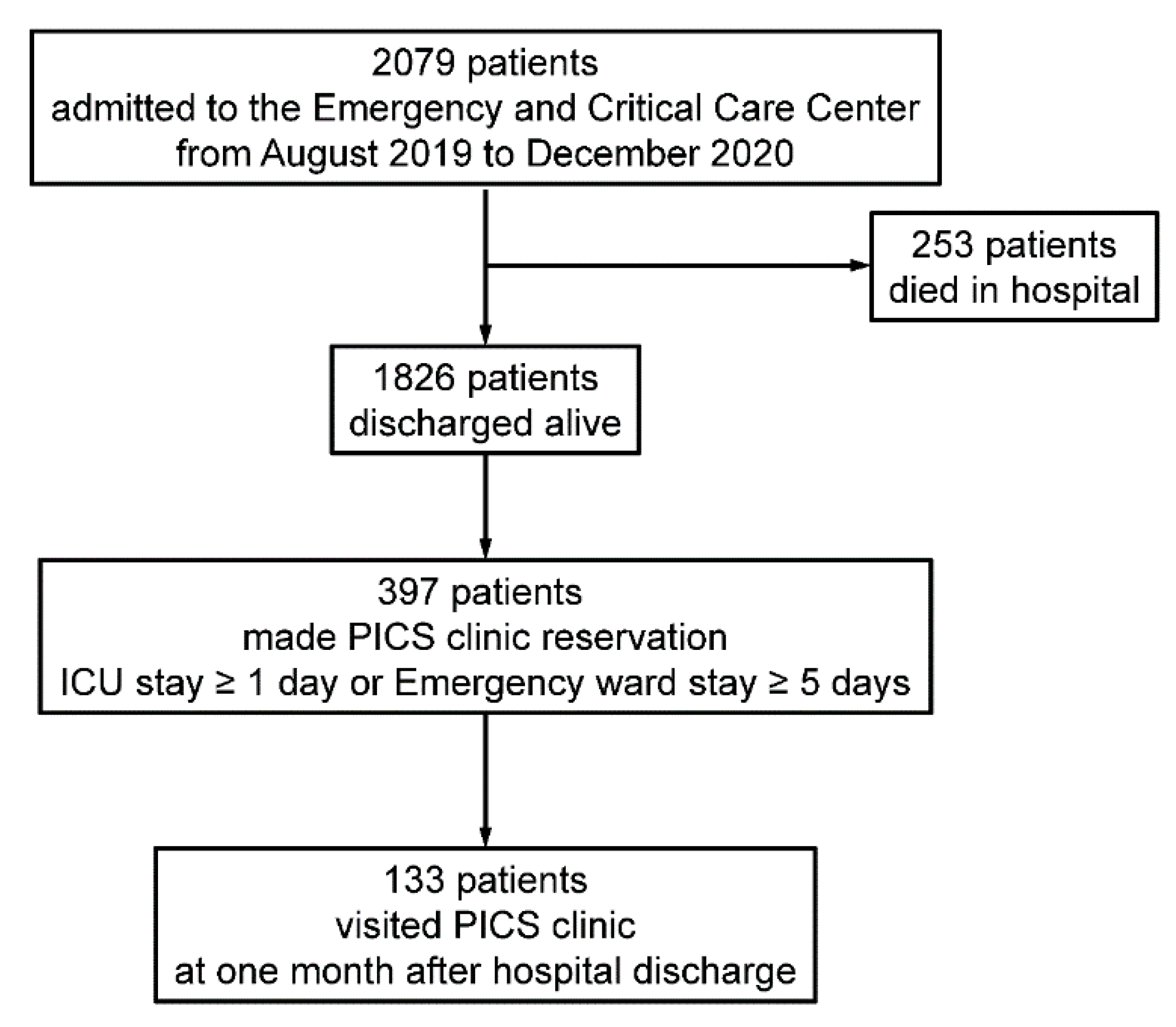
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Needham, D.M.; Davidson, J.; Cohen, H.; Hopkins, R.O.; Weinert, C.; Wunsch, H.; Zawistowski, C.; Bemis-Dougherty, A.; Berney, S.C.; Bienvenu, O.J.; et al. Improving long-term outcomes after discharge from intensive care unit: Report from a stakeholders’ conference. Crit. Care. Med. 2012, 40, 502–509. [Google Scholar] [CrossRef]
- Kress, J.P.; Hall, J.B. ICU-acquired weakness and recovery from critical illness. N. Engl. J. Med. 2014, 370, 1626–1635. [Google Scholar] [CrossRef] [Green Version]
- Hatch, R.; Young, D.; Barber, V.S.; Griffiths, J.; Harrison, D.A.; Watkinson, P.J. Anxiety, depression and post-traumatic stress disorder management after critical illness: A UK multi-centre prospective cohort study. Crit. Care 2020, 24, 633. [Google Scholar] [CrossRef] [PubMed]
- Hatch, R.; Young, D.; Barber, V.; Griffiths, J.; Harrison, D.A.; Watkinson, P. Anxiety, Depression and Post Traumatic Stress Disorder after critical illness: A UK-wide prospective cohort study. Crit. Care 2018, 22, 310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davydow, D.S.; Zatzick, D.; Hough, C.L.; Katon, W.J. A longitudinal investigation of posttraumatic stress and depressive symptoms over the course of the year following medical-surgical intensive care unit admission. Gen. Hosp. Psychiatry 2013, 35, 226–232. [Google Scholar] [CrossRef] [Green Version]
- Wade, D.M.; Howell, D.C.; Weinman, J.A.; Hardy, R.J.; Mythen, M.G.; Brewin, C.R.; Borja-Boluda, S.; Matejowsky, C.F.; Raine, R.A. Investigating risk factors for psychological morbidity three months after intensive care: A prospective cohort study. Crit. Care 2012, 16, R192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parsons, E.C.; Hough, C.L.; Vitiello, M.V.; Zatzick, D.; Davydow, D.S. Insomnia is associated with quality of life impairment in medical-surgical intensive care unit survivors. Heart Lung. 2015, 44, 89–94. [Google Scholar] [CrossRef]
- Elliott, D.; Davidson, J.E.; Harvey, M.A.; Bemis-Dougherty, A.; Hopkins, R.O.; Iwashyna, T.J.; Wagner, J.; Weinert, C.; Wunsch, H.; Bienvenu, O.J.; et al. Exploring the scope of post-intensive care syndrome therapy and care: Engagement of non-critical care providers and survivors in a second stakeholders meeting. Crit. Care Med. 2014, 42, 2518–2526. [Google Scholar] [CrossRef] [PubMed]
- Angus, D.C.; Carlet, J.; Participants, B.R. Surviving intensive care: A report from the 2002 Brussels Roundtable. Intensive Care Med. 2003, 29, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Modrykamien, A.M. The ICU follow-up clinic: A new paradigm for intensivists. Respir. Care 2012, 57, 764–772. [Google Scholar] [CrossRef]
- Griffiths, J.A.; Barber, V.S.; Cuthbertson, B.H.; Young, J.D. A national survey of intensive care follow-up clinics. Anaesth 2006, 61, 950–955. [Google Scholar] [CrossRef]
- Van Der Schaaf, M.; Bakhshi-Raiez, F.; Van Der Steen, M.; Dongelmans, D.A.; De Keizer, N.F. Recommendations for intensive care follow-up clinics; report from a survey and conference of Dutch intensive cares. Minerva Anestesiol. 2015, 81, 135–144. [Google Scholar] [PubMed]
- Kjer, C.K.W.; Estrup, S.; Poulsen, L.M.; Mathiesen, O. Follow-up after intensive care treatment: A questionnaire survey of intensive care aftercare in Denmark. Acta Anaesthesiol. Scand. 2017, 61, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, M.E.; Still, M.; Anderson, B.J.; Bienvenu, O.J.; Brodsky, M.B.; Brummel, N.; Butcher, B.; Clay, A.S.; Felt, H.; Ferrante, L.E.; et al. Society of Critical Care Medicine’s International Consensus Conference on Prediction and Identification of Long-Term Impairments After Critical Illness. Crit. Care Med. 2020, 48, 1670–1679. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.C.; Pandharipande, P.P.; Girard, T.D.; Brummel, N.E.; Thompson, J.L.; Hughes, C.G.; Pun, B.T.; Vasilevskis, E.E.; Morandi, A.; Shintani, A.K.; et al. Depression, post-traumatic stress disorder, and functional disability in survivors of critical illness in the BRAIN-ICU study: A longitudinal cohort study. Lancet Respir. Med. 2014, 2, 369–379. [Google Scholar] [CrossRef] [Green Version]
- Marques, A.; Gaspar de Matos, M.; Henriques-Neto, D.; Peralta, M.; Gouveia, É.; Tesler, R.; Martins, J.; Gomez-Baya, D. Grip Strength and Depression Symptoms Among Middle-Age and Older Adults. Mayo Clin. Proc. 2020, 95, 2134–2143. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The barthel index. Md. State. Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Thrush, A.; Rozek, M.; Dekerlegand, J.L. The clinical utility of the functional status score for the intensive care unit (FSS-ICU) at a long-term acute care hospital: A prospective cohort study. Phys. Ther. 2012, 92, 1536–1545. [Google Scholar] [CrossRef]
- Turan, Z.; Topaloglu, M.; Ozyemisci Taskiran, O. Medical Research Council-sumscore: A tool for evaluating muscle weakness in patients with post-intensive care syndrome. Crit. Care 2020, 24, 562. [Google Scholar] [CrossRef]
- Annunziata, M.A.; Muzzatti, B.; Bidoli, E.; Flaiban, C.; Bomben, F.; Piccinin, M.; Gipponi, K.M.; Mariutti, G.; Busato, S.; Mella, S. Hospital Anxiety and Depression Scale (HADS) accuracy in cancer patients. Support Care Cancer 2020, 28, 3921–3926. [Google Scholar] [CrossRef]
- Hosey, M.M.; Bienvenu, O.J.; Dinglas, V.D.; Turnbull, A.E.; Parker, A.M.; Hopkins, R.O.; Neufeld, K.J.; Needham, D.M. The IES-R remains a core outcome measure for PTSD in critical illness survivorship research. Crit. Care 2019, 23, 362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Shiroiwa, T.; Ikeda, S.; Noto, S.; Igarashi, A.; Fukuda, T.; Saito, S.; Shimozuma, K. Comparison of Value Set Based on DCE and/or TTO Data: Scoring for EQ-5D-5L Health States in Japan. Value Health 2016, 19, 648–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciesielska, N.; Sokołowski, R.; Mazur, E.; Podhorecka, M.; Polak-Szabela, A.; Kędziora-Kornatowska, K. Is the Montreal Cognitive Assessment (MoCA) test better suited than the Mini-Mental State Examination (MMSE) in mild cognitive impairment (MCI) detection among people aged over 60? Meta-analysis. Psychiatr. Pol. 2016, 50, 1039–1052. [Google Scholar] [CrossRef]
- Maki, N.; Ikeda, M.; Hokoishi, K.; Nebu, A.; Komori, K.; Shigenobu, K.; Fukuhara, R.; Hirono, N.; Nakata, H.; Tanabe, H. Validity of the Short-Memory Questionnaire in vascular dementia. Int. J. Geriatr. Psychiatry 2000, 15, 1143–1146. [Google Scholar] [CrossRef]
- Herridge, M.S.; Cheung, A.M.; Tansey, C.M.; Matte-Martyn, A.; Diaz-Granados, N.; Al-Saidi, F.; Cooper, A.B.; Guest, C.B.; Mazer, C.D.; Mehta, S.; et al. One-year outcomes in survivors of the acute respiratory distress syndrome. N. Engl. J. Med. 2003, 348, 683–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, A.M.; Sricharoenchai, T.; Raparla, S.; Schneck, K.W.; Bienvenu, O.J.; Needham, D.M. Posttraumatic stress disorder in critical illness survivors: A metaanalysis. Crit. Care Med. 2015, 43, 1121–1129. [Google Scholar] [CrossRef]
- Kume, M.; Kanoya, Y.; Sato, C. A Study on Patient’s Anxiety and Stress in ICU. JJNS. 2004, 27, 93–99. [Google Scholar]
- Clavet, H.; Hébert, P.C.; Fergusson, D.; Doucette, S.; Trudel, G. Joint contracture following prolonged stay in the intensive care unit. CMAJ 2008, 178, 691–697. [Google Scholar] [CrossRef] [Green Version]
- Gordon, B.R.; McDowell, C.P.; Lyons, M.; Herring, M.P. Associations between grip strength and generalized anxiety disorder in older adults: Results from the Irish longitudinal study on ageing. J. Affect. Disord. 2019, 255, 136–141. [Google Scholar] [CrossRef]
- Marconcin, P.; Peralta, M.; Ferrari, G.; Gaspar de Matos, M.; Espanha, M.; Murawska-Ciałowicz, E.; Marques, A. The Association of Grip Strength with Depressive Symptoms among Middle-Aged and Older Adults with Different Chronic Diseases. Int. J. Environ. Res. Public Health 2020, 17, 6942. [Google Scholar] [CrossRef]
- Gustafson, O.D.; Rowland, M.J.; Watkinson, P.J.; McKechnie, S.; Igo, S. Shoulder Impairment Following Critical Illness: A Prospective Cohort Study. Crit. Care Med. 2018, 46, 1769–1774. [Google Scholar] [CrossRef]
- Jensen, J.F.; Thomsen, T.; Overgaard, D.; Bestle, M.H.; Christensen, D.; Egerod, I. Impact of follow-up consultations for ICU survivors on post-ICU syndrome: A systematic review and meta-analysis. Intensive Care Med. 2015, 41, 763–775. [Google Scholar] [CrossRef] [PubMed]
- Bienvenu, O.J.; Colantuoni, E.; Mendez-Tellez, P.A.; Shanholtz, C.; Dennison-Himmelfarb, C.R.; Pronovost, P.J.; Needham, D.M. Cooccurrence of and remission from general anxiety, depression, and posttraumatic stress disorder symptoms after acute lung injury: A 2-year longitudinal study. Crit. Care Med. 2015, 43, 642–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brück, E.; Larsson, J.W.; Lasselin, J.; Bottai, M.; Hirvikoski, T.; Sundman, E.; Eberhardson, M.; Sackey, P.; Olofsson, P.S. Lack of clinically relevant correlation between subjective and objective cognitive function in ICU survivors: A prospective 12-month follow-up study. Crit. Care 2019, 23, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| N | 133 |
|---|---|
| age, years | 69.8 ± 14.2 |
| sex (male) | 90 (67.6%) |
| SOFA | 5 (4, 8) |
| APACHEII | 15 (9, 18.75) |
| length of hospital stay | 10 (4, 14) |
| length of ICU stay | 7 (3, 12) |
| acute surgery | 46 (34.6%) |
| sepsis | 58 (43.6%) |
| mechanical ventilation, days | 64 (48.1%), 2 (1, 7) |
| renal replacement therapy, days | 25 (18.8%), 3 (1, 7) |
| N | 133 | |
|---|---|---|
| At hospital discharge | ||
| Physical status | Barthel index (n = 57) | 85 (60, 95) |
| FSS-ICU (n = 57) | 34 (25, 35) | |
| MRC score (n = 57) | 56 (48, 60) | |
| grip strength (kg) (n = 57) | 19.5 (12, 25) | |
| grip strength ≥ age/gender matched control (n = 57) | 0 (0%) | |
| In the PICS clinic | ||
| Physician assessment | At least one of the following symptoms | 109 (82%) |
| walking disability | 80 (60.2%) | |
| muscle volume loss | 70 (52.6%) | |
| respiratory dysfunction | 29 (21.8%) | |
| Depression | 17 (12.8%) | |
| Anxiety | 20 (15%) | |
| sleep disorder | 23 (17.3%) | |
| memory impairment | 43 (32.3%) | |
| executive function disorders | 27 (20.3%) | |
| Physical status | Barthel index | 100 (90, 100) |
| FSS-ICU | 35 (35, 35) | |
| MRC score | 58 (54, 60) | |
| grip strength (kg) | 20.75 (15.75, 28.25) | |
| grip strength ≥ age/gender matched control | 6 (4.5%) | |
| Mental status | total HADS | 8 (5, 15) |
| HADS (depression) | 5 (3, 10) | |
| HADS (anxiety) | 3 (1, 6) | |
| total IES-R | 4 (1, 9) | |
| IES-R (Intrusion) | 1 (0, 3) | |
| IES-R (Avoidance) | 0 (0, 3) | |
| IES-R (Hyperarousal) | 1 (0, 4) | |
| Cognitive status | MMSE (n = 40) | 27.5 (23, 30) |
| SMQ (n = 24) | 36 (26.5, 41) | |
| Quality of life | EQ5D | 0.84 (0.68, 0.96) |
| No Walking Disability | Walking Disability | p-Value | ||
| n | 53 | 80 | value | |
| Admission data | age | 72.2 ± 11.9 | 68.2 ± 15.7 | 0.14 |
| sex (male) | 39 (73.5%) | 52 (65%) | 0.30 | |
| SOFA | 5 (4, 8) | 5 (4, 9) | 0.94 | |
| APACHEII | 16 (11.5, 19.5) | 15 (9, 18.5) | 0.40 | |
| length of hospital stay | 7 (3, 13) | 7 (3, 14) | 0.94 | |
| length of ICU stay | 6 (3, 11) | 7 (3, 13) | 0.59 | |
| At discharge | n (%) | 19 (35.8%) | 38 (47.5%) | 0.50 |
| Physical status | Barthel index at discharge | 90 (70, 100) | 80 (48.75, 95) | 0.0056 * |
| FSS-ICU at discharge | 35 (28, 35) | 34 (25, 35) | 0.086 | |
| MRC score at discharge | 58 (56, 60) | 55 (48, 58.25) | 0.0010 * | |
| grip strength (kg) at discharge | 19.5 (15.5, 31) | 19.0 (11.65, 23.65) | 0.17 | |
| grip strength ≥ age/gender matched control | 0 (0%) | 0 (0%) | 1 | |
| At PICS clinic | ||||
| Physical status | Barthel index | 100 (100, 100) | 100 (80, 100) | 0.012 * |
| FSS-ICU | 35 (35, 35) | 35 (34, 35) | 0.0025 * | |
| MRC score | 60 (58, 60) | 58 (53, 60) | 0.0010 * | |
| grip strength (kg) | 24.75 (18.20, 31.30) | 20.10 (13.10, 26.35) | 0.0021 * | |
| grip strength ≥ age/gender matched control | 5 (10.9%) | 1 (1.3%) | 0.015 * | |
| Mental status | total HADS | 7 (4, 13) | 10 (6, 16) | 0.029 * |
| HADS (depression) | 4 (1, 7) | 7 (4, 10) | 0.013 * | |
| HADS (anxiety) | 2 (1, 4) | 4 (1, 7) | 0.046 * | |
| total IES-R | 3 (1, 8) | 4.5 (1, 10) | 0.25 | |
| IES-R (Intrusion) | 1 (1, 2.75) | 2 (0, 4) | 0.43 | |
| IES-R (Avoidance) | 0 (0, 2) | 0 (0, 3) | 0.49 | |
| IES-R (Hyperarousal) | 1 (0, 3) | 1 (0, 5) | 0.26 | |
| Quality of life | EQ5D | 0.96 (0.84, 1) | 0.77 (0.62, 0.89) | <0.0001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, K.; Kawasaki, A.; Suzuki, N.; Hosoi, S.; Fujita, T.; Hachisu, S.; Nakano, H.; Naraba, H.; Mochizuki, M.; Takahashi, Y. Grip Strength Correlates with Mental Health and Quality of Life after Critical Care: A Retrospective Study in a Post-Intensive Care Syndrome Clinic. J. Clin. Med. 2021, 10, 3044. https://doi.org/10.3390/jcm10143044
Nakamura K, Kawasaki A, Suzuki N, Hosoi S, Fujita T, Hachisu S, Nakano H, Naraba H, Mochizuki M, Takahashi Y. Grip Strength Correlates with Mental Health and Quality of Life after Critical Care: A Retrospective Study in a Post-Intensive Care Syndrome Clinic. Journal of Clinical Medicine. 2021; 10(14):3044. https://doi.org/10.3390/jcm10143044
Chicago/Turabian StyleNakamura, Kensuke, Ayako Kawasaki, Noriyo Suzuki, Sayaka Hosoi, Takahiro Fujita, Syohei Hachisu, Hidehiko Nakano, Hiromu Naraba, Masaki Mochizuki, and Yuji Takahashi. 2021. "Grip Strength Correlates with Mental Health and Quality of Life after Critical Care: A Retrospective Study in a Post-Intensive Care Syndrome Clinic" Journal of Clinical Medicine 10, no. 14: 3044. https://doi.org/10.3390/jcm10143044
APA StyleNakamura, K., Kawasaki, A., Suzuki, N., Hosoi, S., Fujita, T., Hachisu, S., Nakano, H., Naraba, H., Mochizuki, M., & Takahashi, Y. (2021). Grip Strength Correlates with Mental Health and Quality of Life after Critical Care: A Retrospective Study in a Post-Intensive Care Syndrome Clinic. Journal of Clinical Medicine, 10(14), 3044. https://doi.org/10.3390/jcm10143044