
Efficacy and Safety of Postmenopausal Osteoporosis Treatments: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Selection Criteria
2.1.1. Search Strategy
2.1.2. Selection Criteria
2.1.3. Population
2.1.4. Interventions
2.1.5. Comparisons
2.1.6. Outcomes
2.2. Data Abstraction and Quality Assessment
2.3. Statistical Methods
3. Results
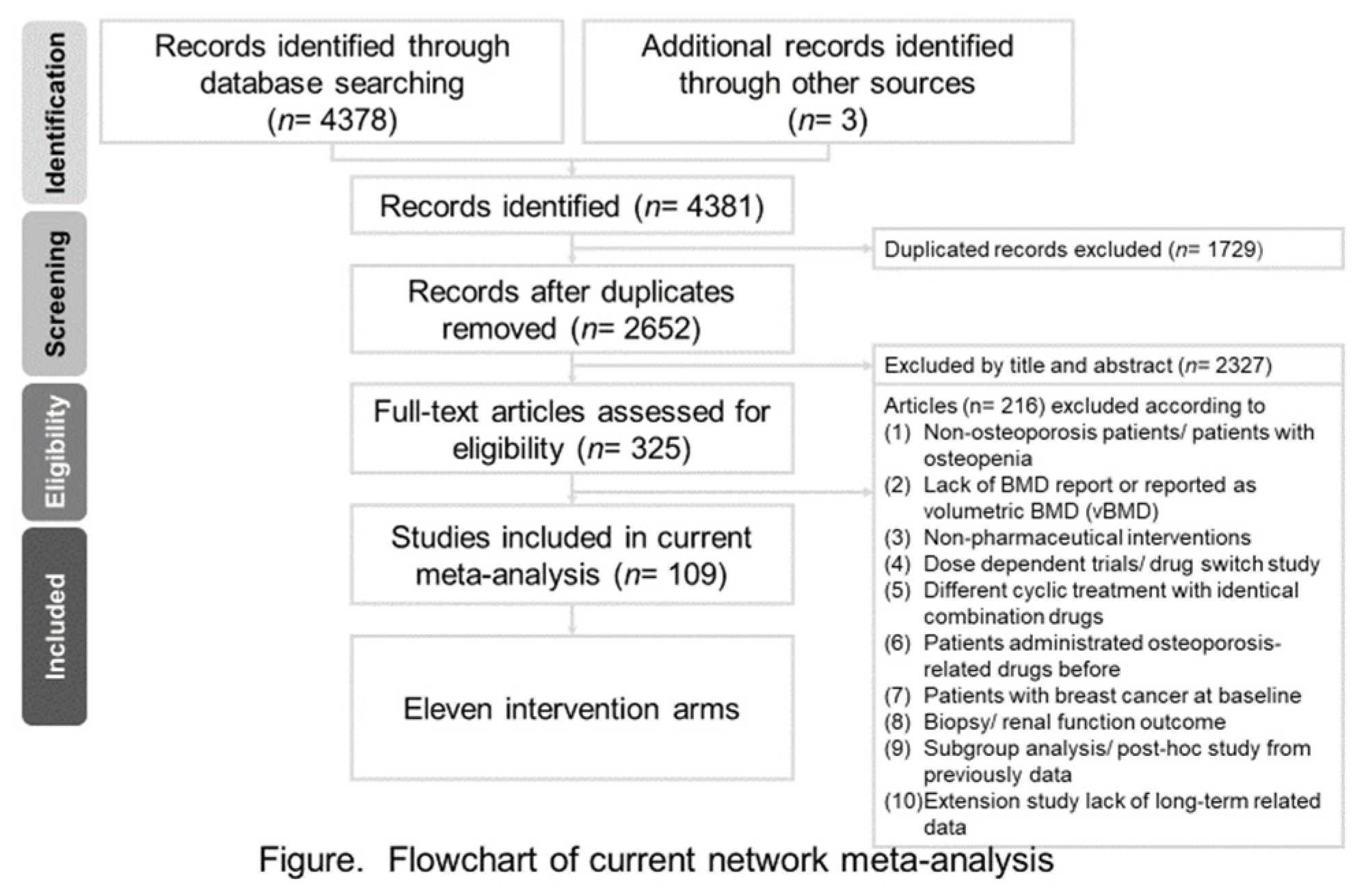
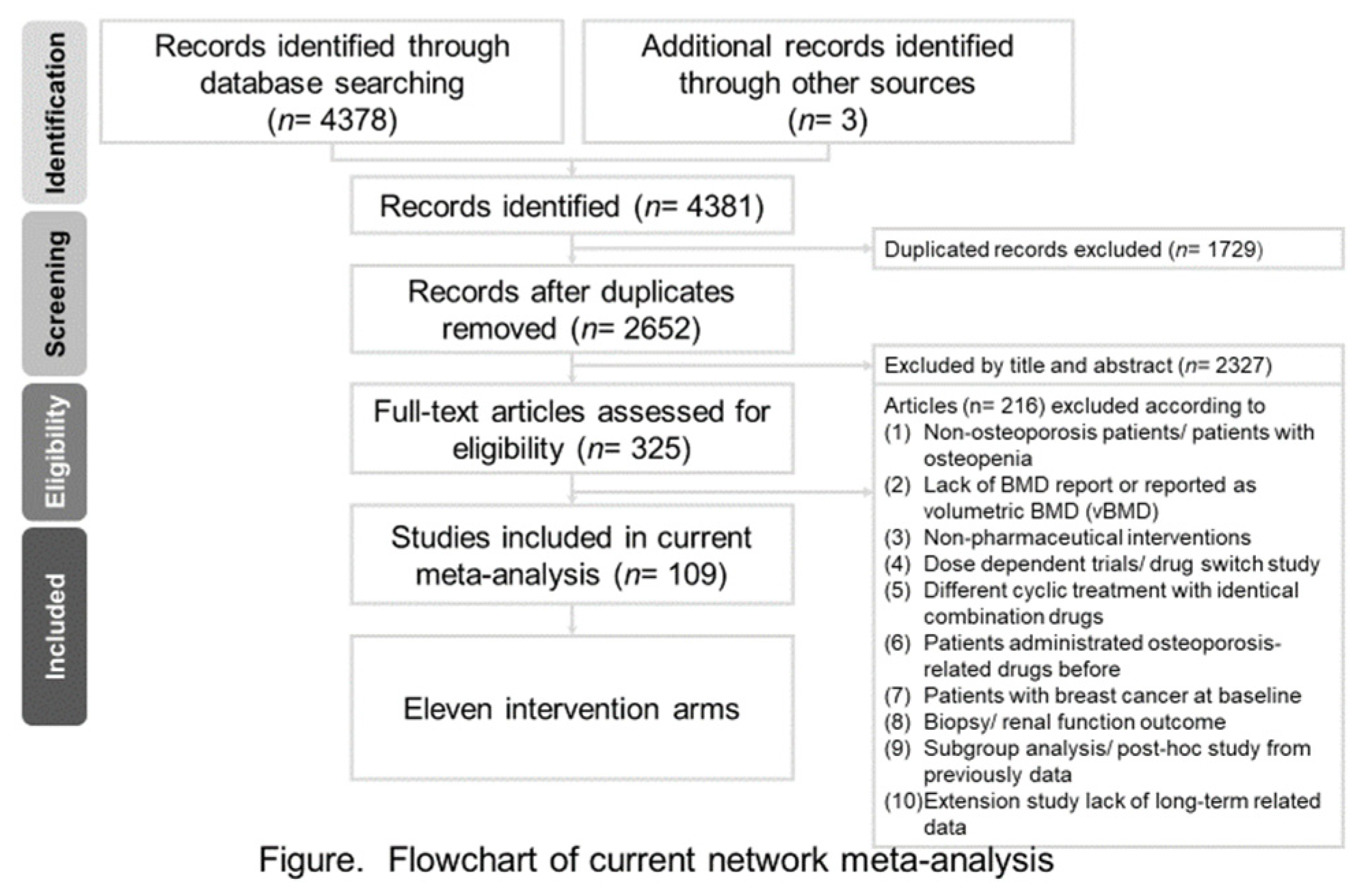
3.1. Search Results
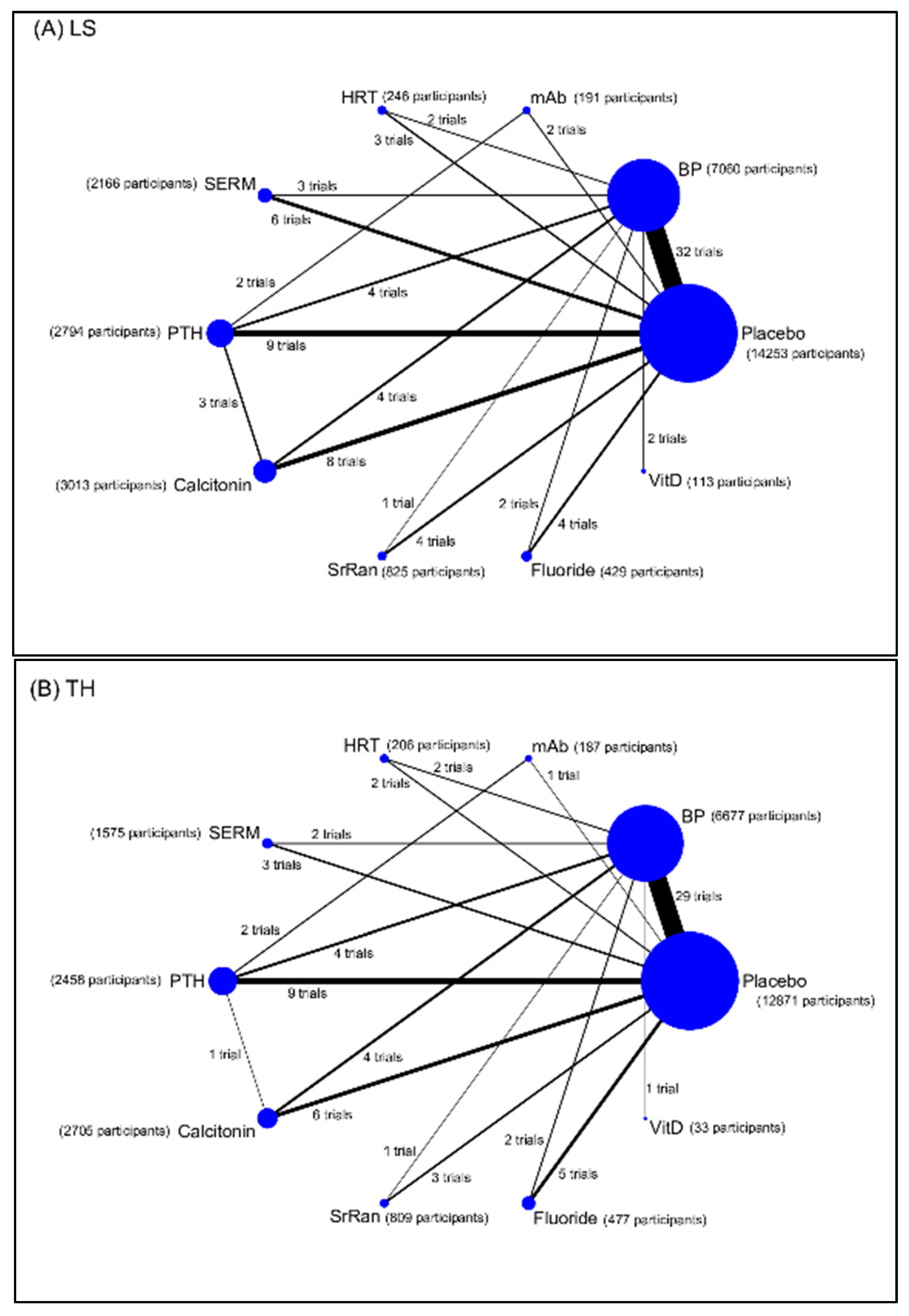
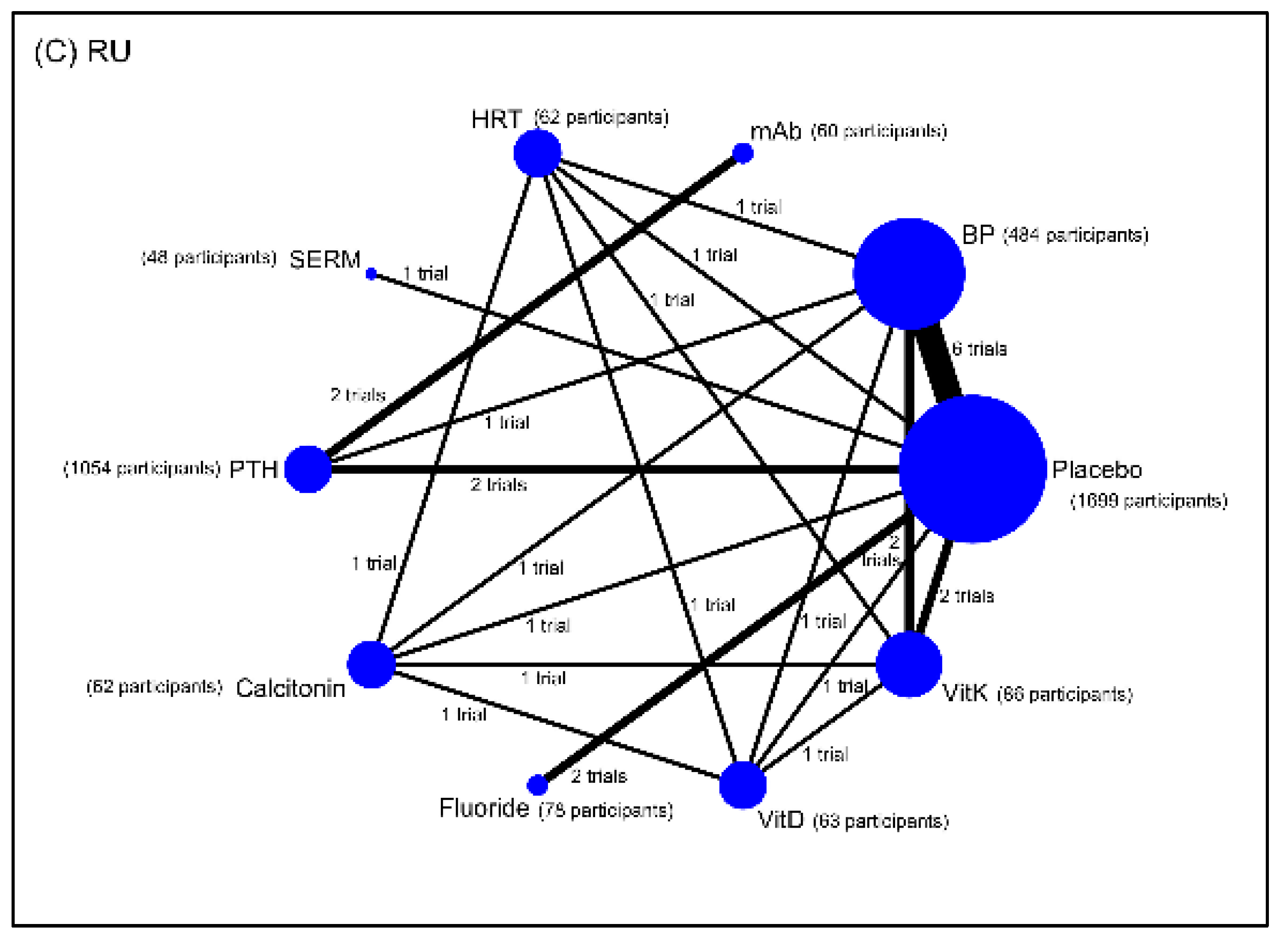
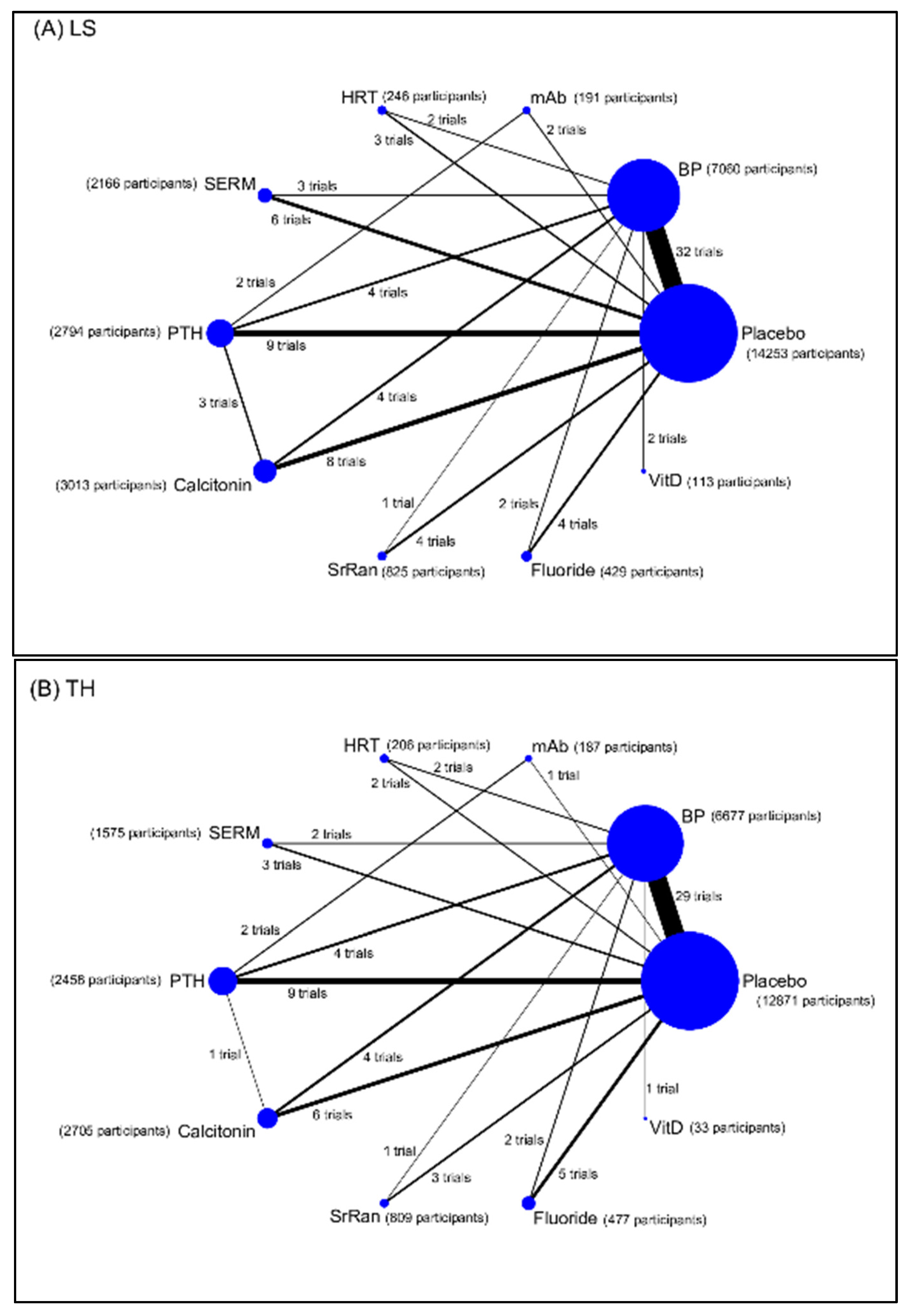
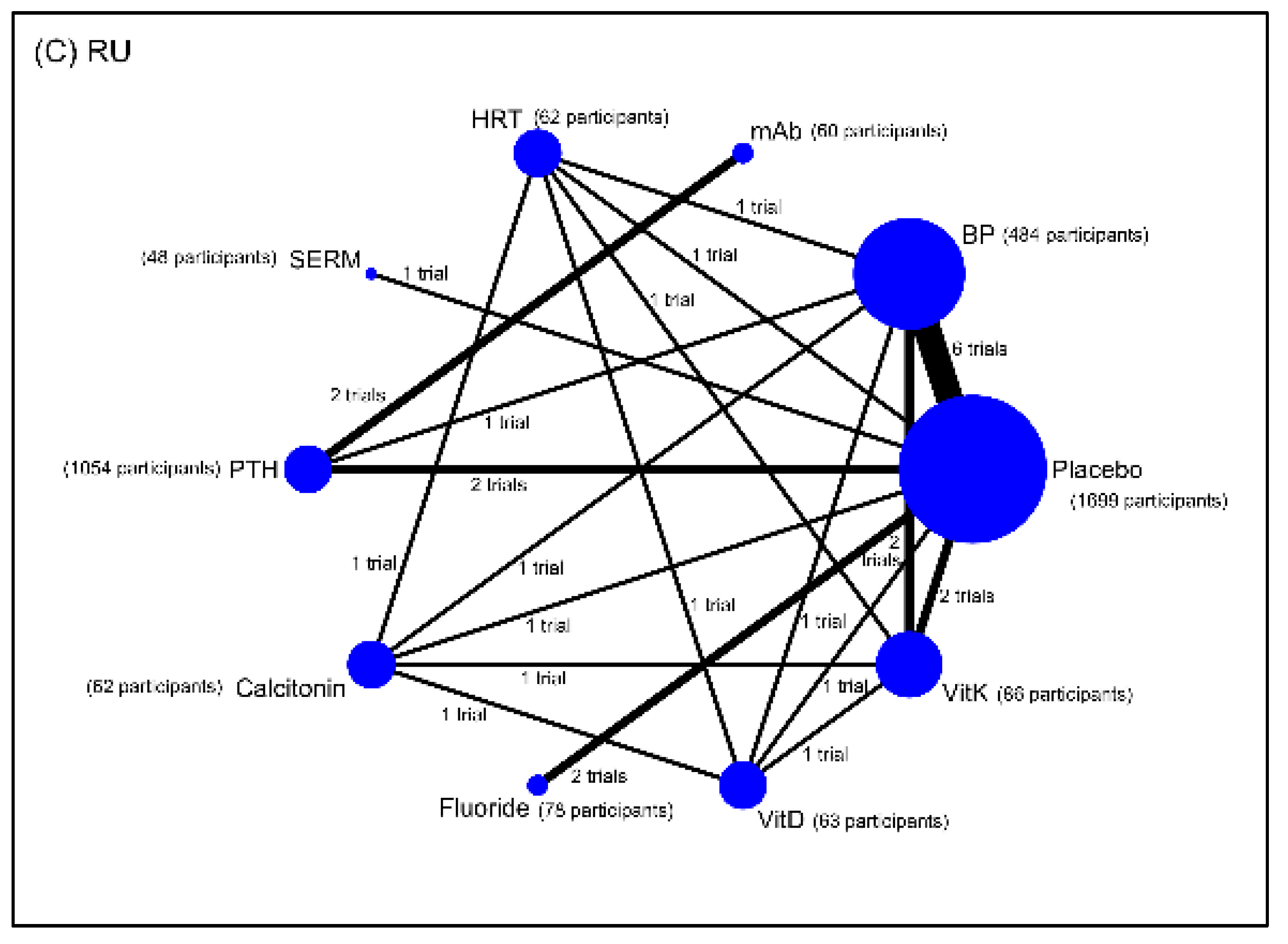
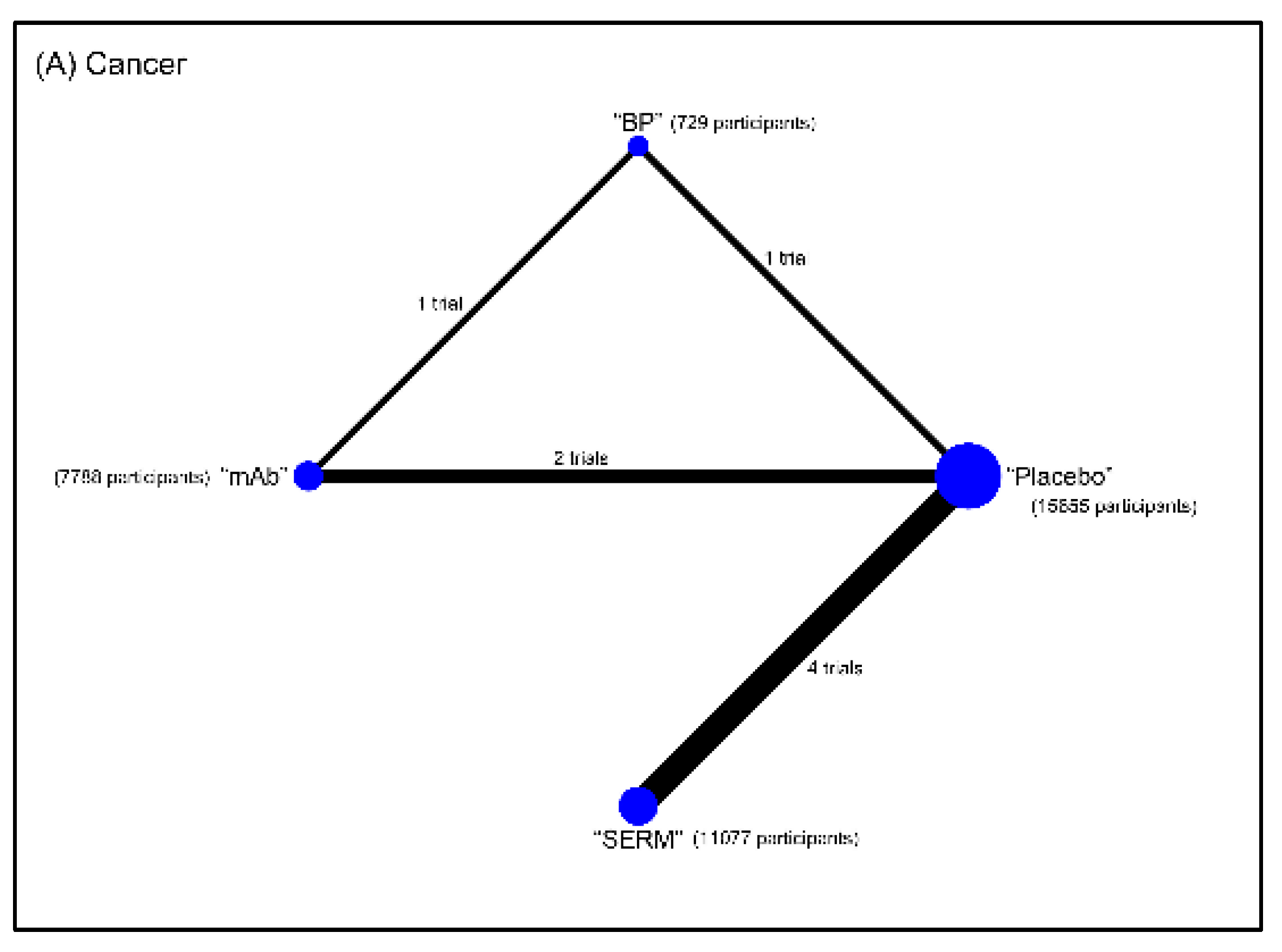
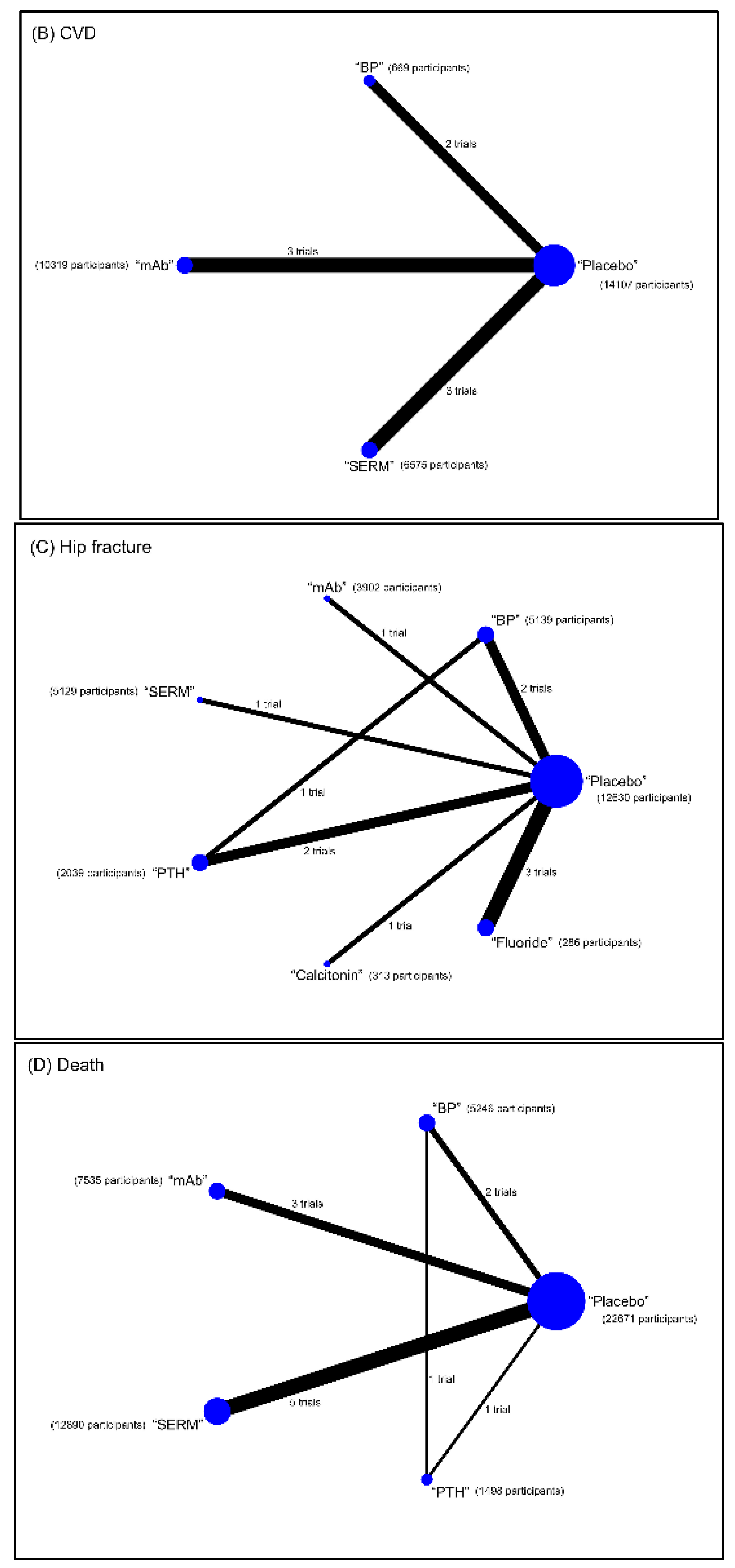
3.2. Results of the Network Meta-Analysis
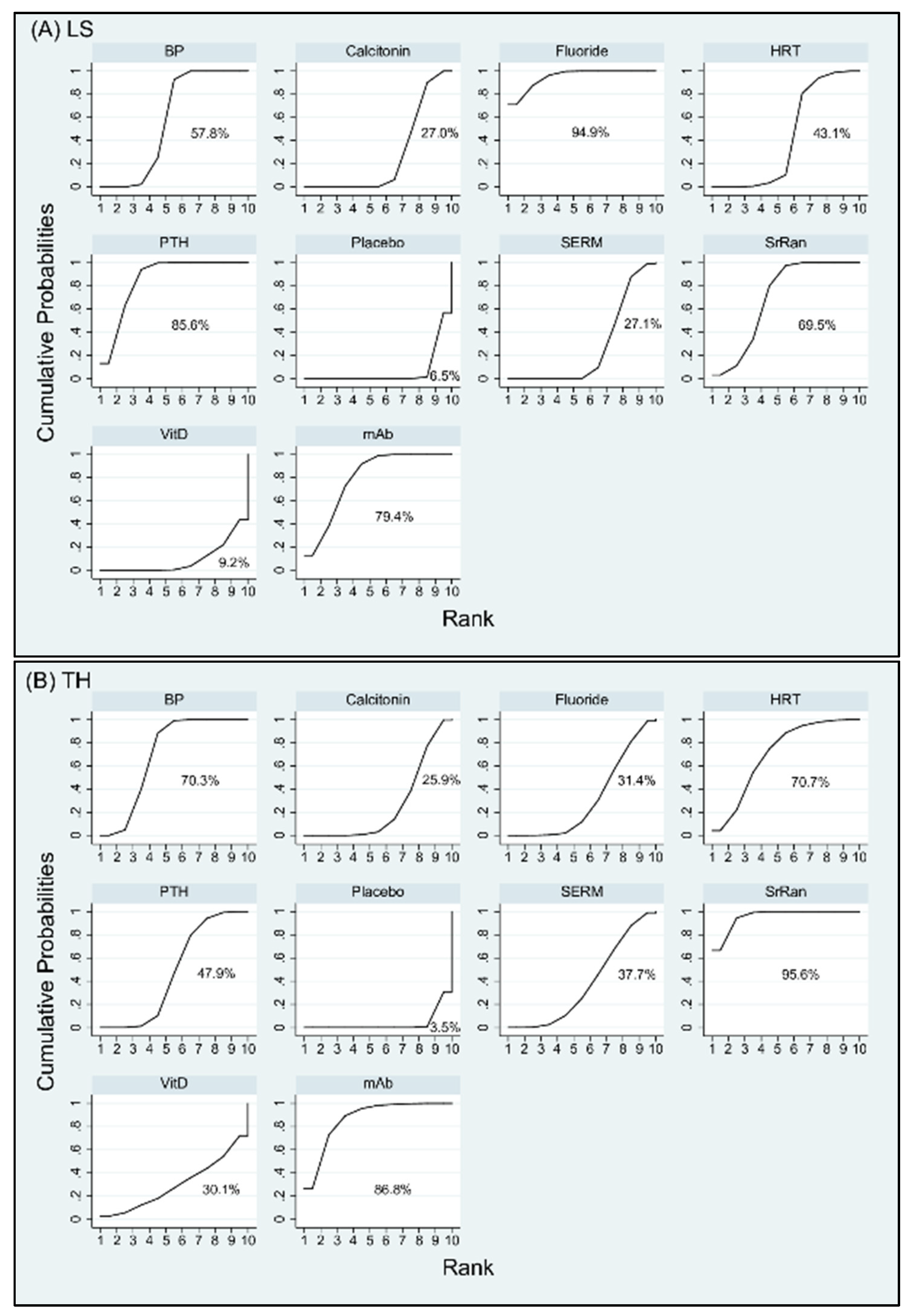
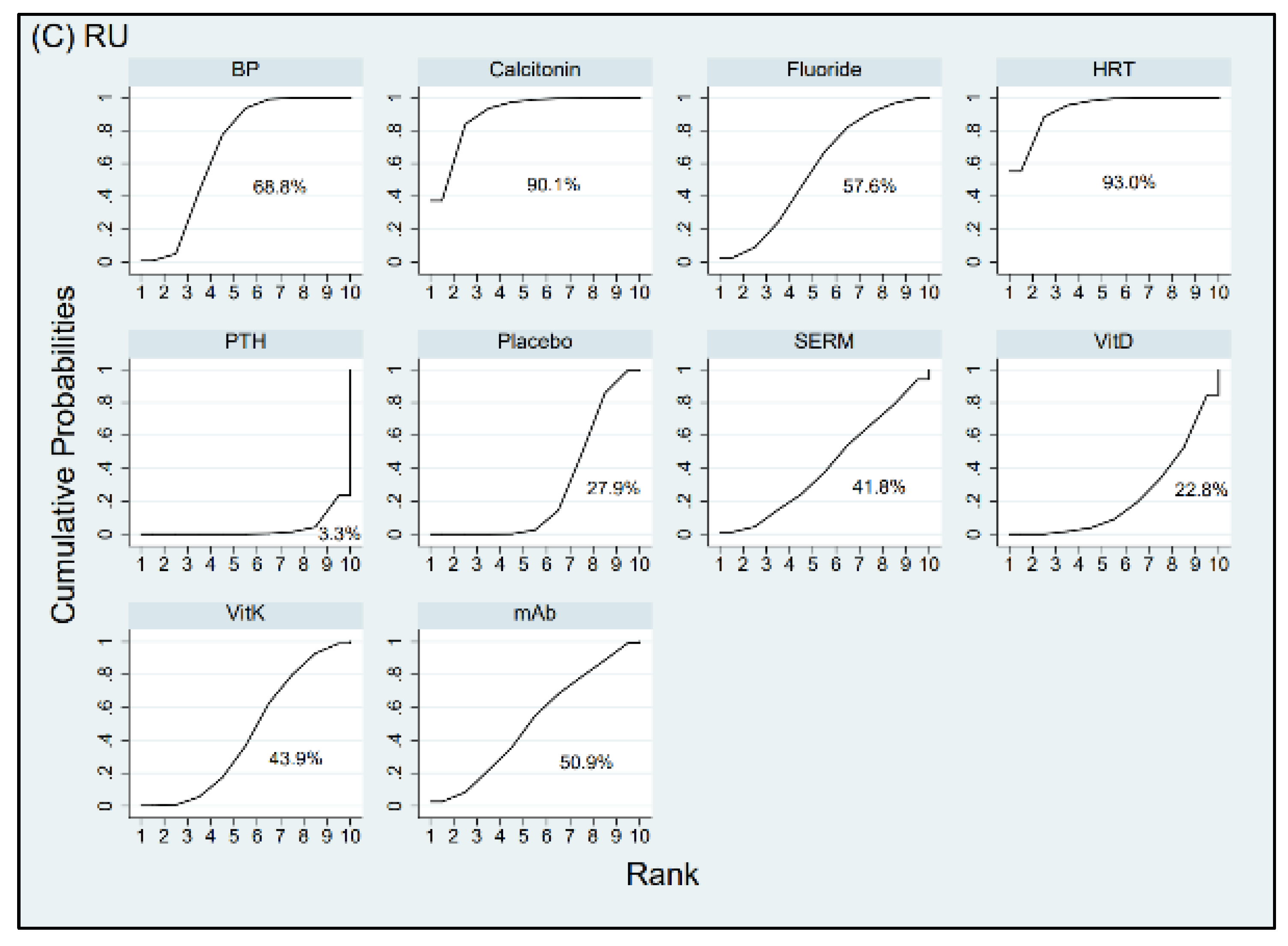
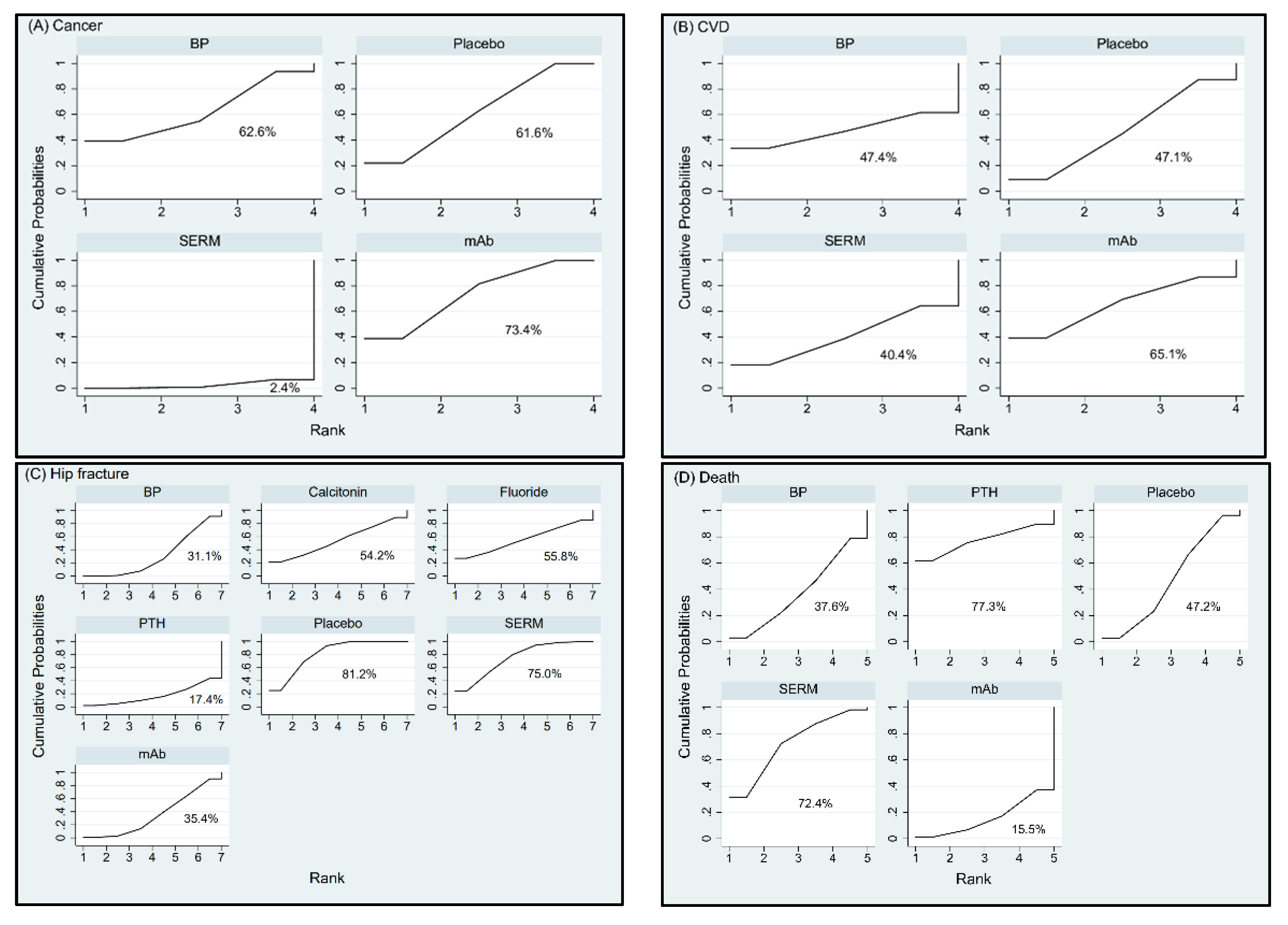
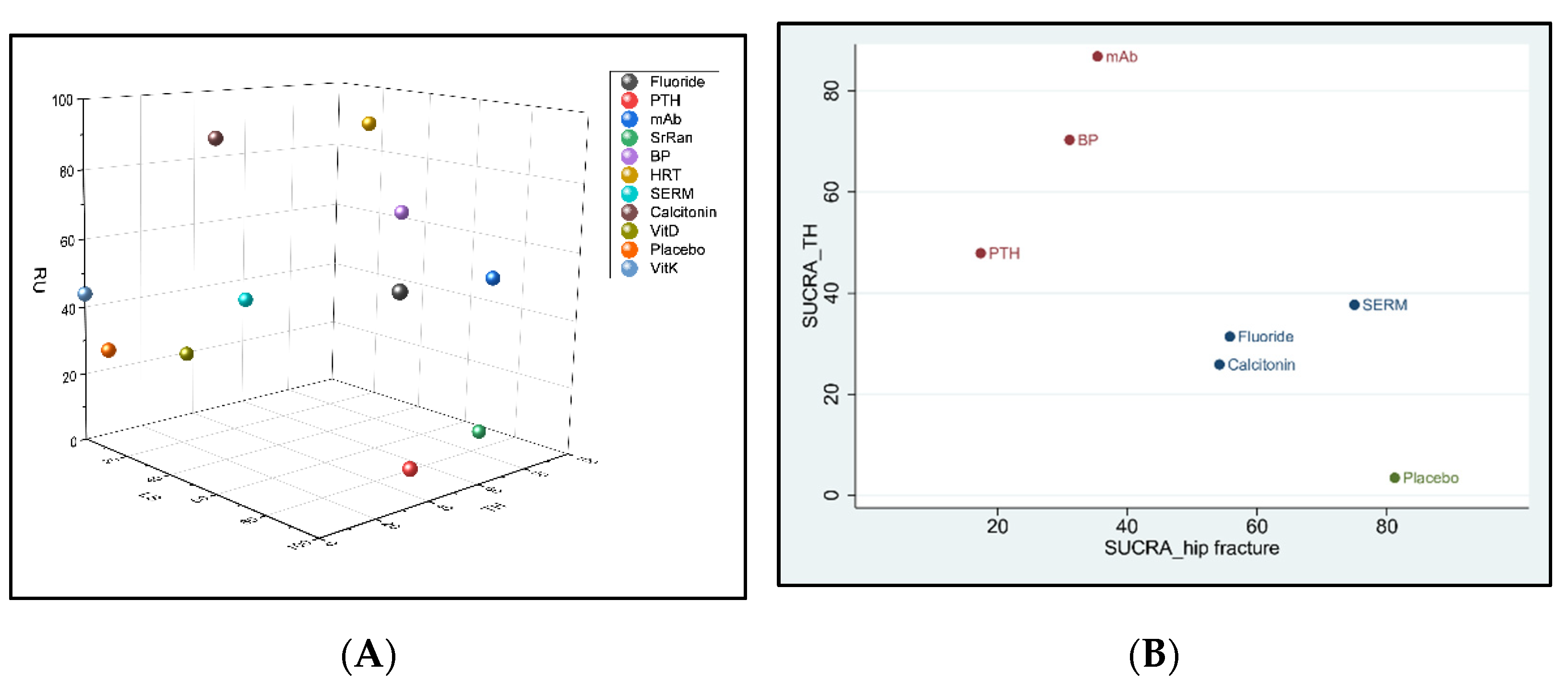
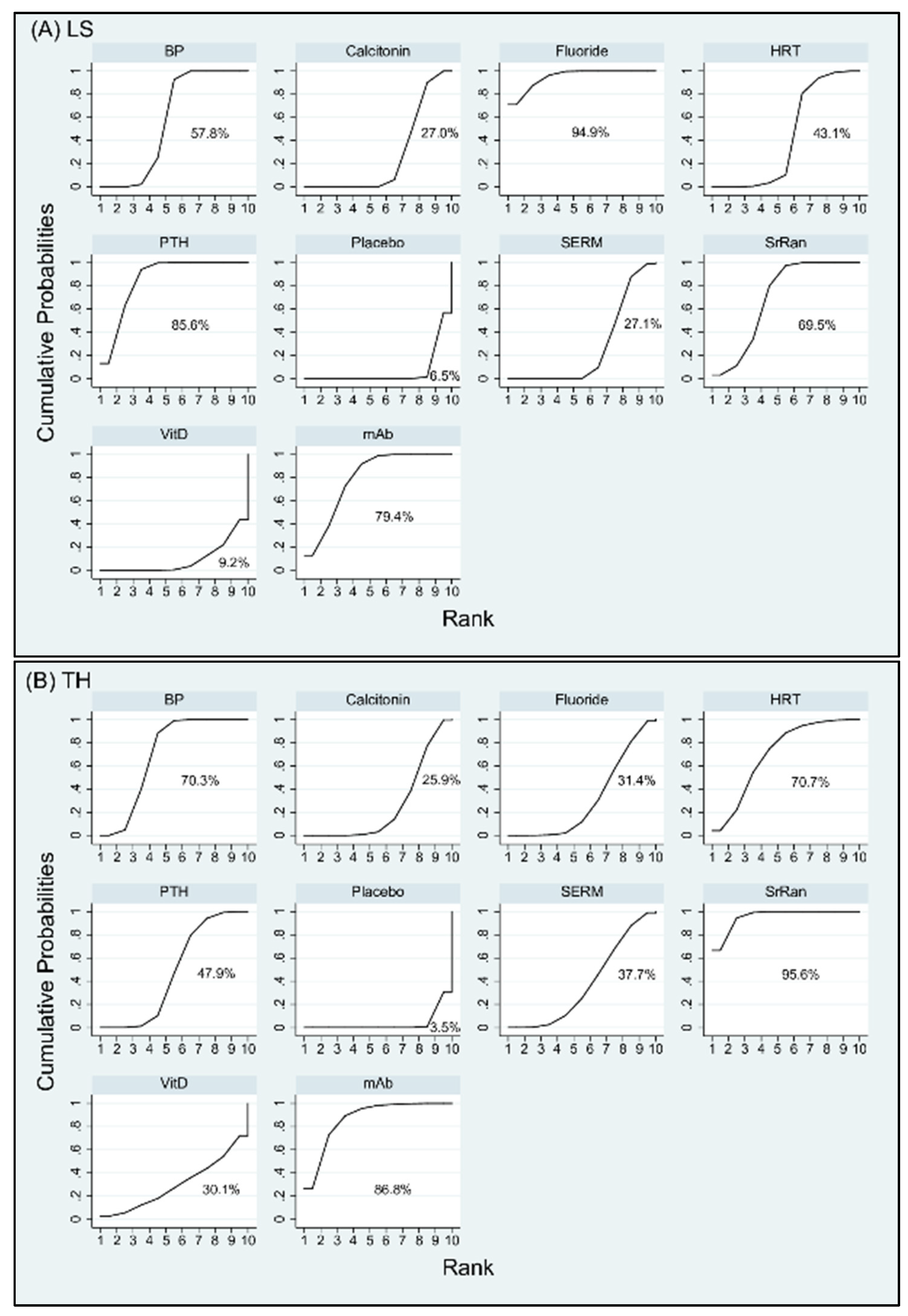
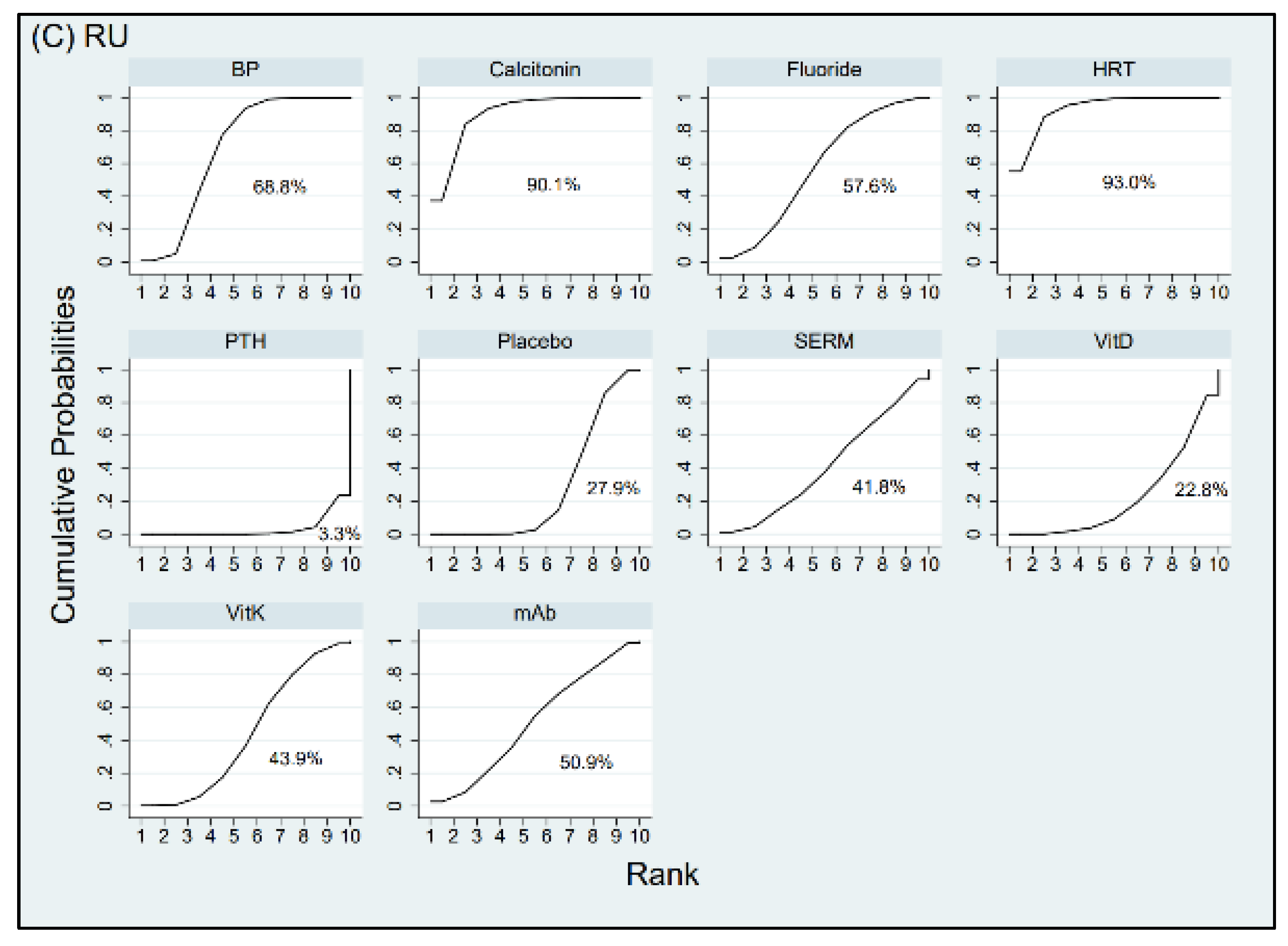
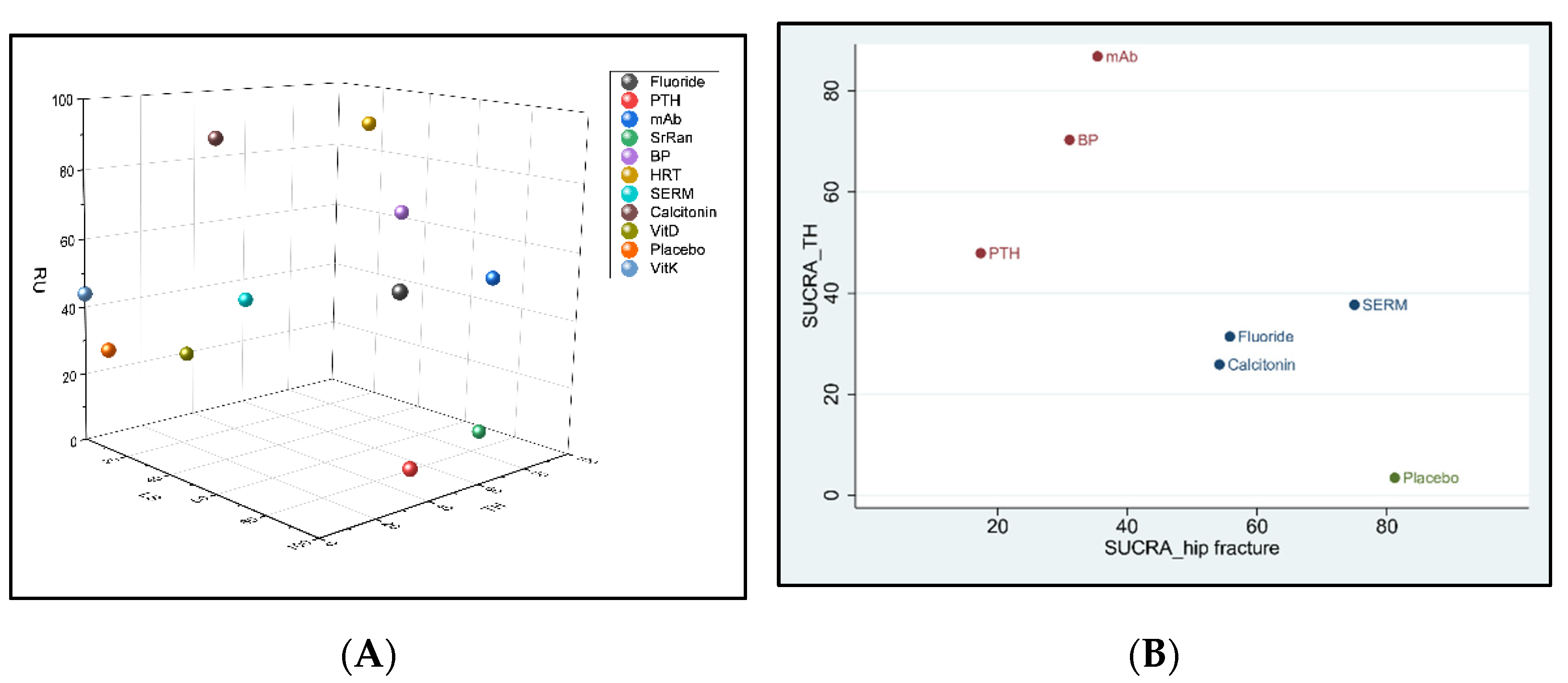
3.3. Ranking of Interventions
3.4. Evaluating the Inconsistency between Direct and Indirect Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheng, L.; Zhang, K.; Zhang, Z. Effectiveness of thiazides on serum and urinary calcium levels and bone mineral density in patients with osteoporosis: A systematic review and meta-analysis. Drug Des. Dev. Ther. 2018, 12, 3929–3935. [Google Scholar] [CrossRef] [Green Version]
- Cummings, S.R.; Melton, L.J. Epidemiology and outcomes of osteoporotic fractures. Lancet 2002, 359, 1761–1767. [Google Scholar] [CrossRef]
- Vidal, M.; Thibodaux, R.J.; Neira, L.F.V.; Messina, O.D. Osteoporosis: A clinical and pharmacological update. Clin. Rheumatol. 2019, 38, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Sattui, S.E.; Saag, K.G. Fracture mortality: Associations with epidemiology and osteoporosis treatment. Nat. Rev. Endocrinol. 2014, 10, 592–602. [Google Scholar] [CrossRef] [PubMed]
- Daruwalla, Z.J.; Huq, S.S.; Wong, K.L.; Nee, P.Y.; Leong, K.M.; Pillay, K.R.; Murphy, D.P. Hip fractures, preceding distal radius fractures and screening for osteoporosis: Should we be screening earlier? A minimum 10-year retrospective cohort study at a single centre. Osteoporos. Int. 2016, 27, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Willson, T.; Nelson, S.D.; Newbold, J.; Nelson, R.E.; LaFleur, J. The clinical epidemiology of male osteoporosis: A review of the recent literature. Clin. Epidemiol. 2015, 7, 65–76. [Google Scholar]
- Silverman, S.L.; Kupperman, E.S.; Bukata, S.V. Fracture healing: A consensus report from the International Osteoporosis Foundation Fracture Working Group. Osteoporos. Int. 2016, 27, 2197–2206. [Google Scholar] [CrossRef]
- Unni, S.; Yao, Y.; Milne, N.; Gunning, K.; Curtis, J.R.; LaFleur, J. An evaluation of clinical risk factors for estimating fracture risk in postmenopausal osteoporosis using an electronic medical record database. Osteoporos. Int. 2015, 26, 581–587. [Google Scholar] [CrossRef]
- Anagnostis, P.; Siolos, P.; Gkekas, N.K.; Kosmidou, N.; Artzouchaltzi, A.M.; Christou, K.; Goulis, D.G. Association between age at menopause and fracture risk: A systematic review and meta-analysis. Endocrine 2019, 63, 213–224. [Google Scholar] [CrossRef]
- Zhu, H.; Jiang, J.; Wang, Q.; Zong, J.; Zhang, L.; Ma, T.; Zhang, L. Associations between ERalpha/beta gene polymorphisms and osteoporosis susceptibility and bone mineral density in postmenopausal women: A systematic review and meta-analysis. BMC Endocr. Disord. 2018, 18, 11. [Google Scholar] [CrossRef] [Green Version]
- Jimenez-Mola, S.; Calvo-Lobo, C.; Idoate-Gil, J.; Seco-Calvo, J. Functionality, comorbidity, complication surgery of hip fracture in older adults by age distribution. Rev. Assoc. Med. Bras. 2018, 64, 420–427. [Google Scholar] [CrossRef]
- Briot, K. Fracture Liaison Services. Curr. Opin. Rheumatol. 2017, 29, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Mugnier, B.; Daumas, A.; Couderc, A.L.; Mizzi, B.; Gonzalez, T.; Amrani, A.; Villani, P. Clinical effectiveness of osteoporosis treatment in older patients: A fracture liaison service-based prospective study. J. Women Aging 2019, 31, 553–565. [Google Scholar] [CrossRef] [PubMed]
- Brozek, W.; Reichardt, B.; Zwerina, J.; Dimai, H.P.; Klaushofer, K.; Zwettler, E. Antiresorptive therapy and risk of mortality and refracture in osteoporosis-related hip fracture: A nationwide study. Osteoporos. Int. 2016, 27, 387–396. [Google Scholar] [CrossRef]
- Davidson, E.; Seal, A.; Doyle, Z.; Fielding, K.; McGirr, J. Prevention of osteoporotic refractures in regional Australia. Aust. J. Rural Health 2017, 25, 362–368. [Google Scholar] [CrossRef] [Green Version]
- Lyu, H.; Jundi, B.; Xu, C.; Tedeschi, S.K.; Yoshida, K.; Zhao, S.; Solomon, D.H. Comparison of Denosumab and Bisphosphonates in Patients With Osteoporosis: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Endocrinol. Metab. 2019, 104, 1753–1765. [Google Scholar] [CrossRef] [PubMed]
- Pispati, A.; Pandey, V.; Patel, R. Oral Bisphosphonate Induced Recurrent Osteonecrosis of Jaw with Atypical Femoral Fracture and Subsequent Mandible Fracture in the Same Patient: A Case Report. J. Orthop. Case Rep. 2018, 8, 85–88. [Google Scholar]
- Black, D.M.; Abrahamsen, B.; Bouxsein, M.L.; Einhorn, T.; Napoli, N. Atypical Femur Fractures—Review of epidemiology, relationship to bisphosphonates, prevention and clinical management. Endocr. Rev. 2019, 40, 333–368. [Google Scholar] [CrossRef] [Green Version]
- Knopp-Sihota, J.A.; Cummings, G.G.; Homik, J.; Voaklander, D. The association between serious upper gastrointestinal bleeding and incident bisphosphonate use: A population-based nested cohort study. BMC Geriatr. 2013, 13, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palacios, S.; Silverman, S.L.; de Villiers, T.J.; Levine, A.B.; Goemaere, S.; Brown, J.P.; Chines, A.A. A 7-year randomized, placebo-controlled trial assessing the long-term efficacy and safety of bazedoxifene in postmenopausal women with osteoporosis: Effects on bone density and fracture. Menopause 2015, 22, 806–813. [Google Scholar] [CrossRef]
- Weaver, C.M.; Alexander, D.D.; Boushey, C.J.; Dawson-Hughes, B.; Lappe, J.M.; LeBoff, M.S.; Wang, D.D. Calcium plus vitamin D supplementation and risk of fractures: An updated meta-analysis from the National Osteoporosis Foundation. Osteoporos. Int. 2016, 27, 367–376. [Google Scholar] [CrossRef] [Green Version]
- Peng, L.; Luo, Q.; Lu, H. Efficacy and safety of bazedoxifene in postmenopausal women with osteoporosis: A systematic review and meta-analysis. Medicine 2017, 96, e8659. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Sui, L.; Gai, P.; Li, G.; Qi, X.; Jiang, X. The efficacy and safety of vertebral fracture prevention therapies in post-menopausal osteoporosis treatment: Which therapies work best? a network meta-analysis. Bone Jt. Res. 2017, 6, 452–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, X.; Wen, F.; Yang, W.; Xie, J.Y.; Ding, L.L.; Mo, Y.X. Comparative efficacy and safety of pharmacological interventions for osteoporosis in postmenopausal women: A network meta-analysis (Chongqing, China). Menopause 2019, 26, 929–939. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.F.; Wang, Z.Q.; Liu, L.; Zhang, B.T.; Miao, Y.Y.; Yu, S.N. A network meta-analysis on the short-term efficacy and adverse events of different anti-osteoporosis drugs for the treatment of postmenopausal osteoporosis. J. Cell Biochem. 2018, 119, 4469–4481. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Kang, N.; Yang, J.C.; Su, Q.J.; Liu, Y.Z.; Guan, L.; Hai, Y. Drug efficacies on bone mineral density and fracture rate for the treatment of postmenopausal osteoporosis: A network meta-analysis. Eur. Rev. Med. Pharm. Sci. 2019, 23, 2640–2668. [Google Scholar]
- Yang, X.C.; Deng, Z.H.; Wen, T.; Luo, W.; Xiao, W.F.; Zhao, R.B.; Li, Y.S. Network Meta-Analysis of Pharmacological Agents for Osteoporosis Treatment and Fracture Prevention. Cell Physiol. Biochem. 2016, 40, 781–795. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Allon, R.; Levy, Y.; Lavi, I.; Kramer, A.; Barzilai, M.; Wollstein, R. How to Best Predict Fragility Fractures: An Update and Systematic Review. Isr. Med Assoc. J. IMAJ 2018, 20, 773–779. [Google Scholar]
- Gao, Y.N.; Wu, Y.C.; Lin, S.Y.; Chang, J.Z.; Tu, Y.K. Short-term efficacy of minimally invasive treatments for adult obstructive sleep apnea: A systematic review and network meta-analysis of randomized controlled trials. J. Med. Assoc. 2019, 118, 750–765. [Google Scholar] [CrossRef]
- Kendler, D.L.; Marin, F.; Zerbini, C.A.F.; Russo, L.A.; Greenspan, S.L.; Zikan, V.; Lopez-Romero, P. Effects of teriparatide and risedronate on new fractures in post-menopausal women with severe osteoporosis (VERO): A multicentre, double-blind, double-dummy, randomised controlled trial. Lancet 2018, 391, 230–240. [Google Scholar] [CrossRef]
- Saag, K.G.; Petersen, J.; Brandi, M.L.; Karaplis, A.C.; Lorentzon, M.; Thomas, T.; Grauer, A. Romosozumab or Alendronate for Fracture Prevention in Women with Osteoporosis. N. Engl. J. Med. 2017, 377, 1417–1427. [Google Scholar] [CrossRef] [Green Version]
- Cummings, S.R.; San Martin, J.; McClung, M.R.; Siris, E.S.; Eastell, R.; Reid, I.R.; Trial, F. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N. Engl. J. Med. 2009, 361, 756–765. [Google Scholar] [CrossRef] [Green Version]
- Cosman, F.; Crittenden, D.B.; Adachi, J.D.; Binkley, N.; Czerwinski, E.; Ferrari, S.; Grauer, A. Romosozumab Treatment in Postmenopausal Women with Osteoporosis. N. Engl. J. Med. 2016, 375, 1532–1543. [Google Scholar] [CrossRef]
- Watts, N.B.; Grbic, J.T.; Binkley, N.; Papapoulos, S.; Butler, P.W.; Yin, X.; McClung, M. Invasive Oral Procedures and Events in Postmenopausal Women With Osteoporosis Treated With Denosumab for Up to 10 Years. J. Clin. Endocrinol. Metab. 2019, 104, 2443–2452. [Google Scholar] [CrossRef]
- Wu, J.; Zhang, Q.; Yan, G.; Jin, X. Denosumab compared to bisphosphonates to treat postmenopausal osteoporosis: A meta-analysis. J. Orthop. Surg. Res. 2018, 13, 194. [Google Scholar] [CrossRef] [Green Version]
- Sanderson, J.; Martyn-St James, M.; Stevens, J.; Goka, E.; Wong, R.; Campbell, F.; Davis, S. Clinical effectiveness of bisphosphonates for the prevention of fragility fractures: A systematic review and network meta-analysis. Bone 2016, 89, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Marjoribanks, J.; Farquhar, C.; Roberts, H.; Lethaby, A.; Lee, J. Long-term hormone therapy for perimenopausal and postmenopausal women. Cochrane Database Syst. Rev. 2017, 1, CD004143. [Google Scholar] [CrossRef]
- Haguenauer, D.; Welch, V.; Shea, B.; Tugwell, P.; Wells, G. Fluoride for treating postmenopausal osteoporosis. Cochrane Database Syst. Rev. 2000, CD002825. [Google Scholar] [CrossRef]
- Gupta, M.; Gupta, N. Bisphosphonate Related Jaw Osteonecrosis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2018. [Google Scholar]
- Kilic, E.; Doganay, O. Current management concepts for bisphosphonate-related osteonecrosis of the jaw: A review. Gen. Dent. 2018, 66, e1–e5. [Google Scholar]
- Nicolatou-Galitis, O.; Schiødt, M.; Mendes, R.A.; Ripamonti, C.; Hope, S.; Drudge-Coates, L.; Van den Wyngaert, T. Medication-related osteonecrosis of the jaw: Definition and best practice for prevention, diagnosis, and treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 117–135. [Google Scholar] [CrossRef] [Green Version]
- Gallacher, S.J.; Dixon, T. Impact of treatments for postmenopausal osteoporosis (bisphosphonates, parathyroid hormone, strontium ranelate, and denosumab) on bone quality: A systematic review. Calcif. Tissue Int. 2010, 87, 469–484. [Google Scholar] [CrossRef]
- Finkelstein, J.S.; Wyland, J.J.; Lee, H.; Neer, R.M. Effects of teriparatide, alendronate, or both in women with postmenopausal osteoporosis. J. Clin. Endocrinol. Metab. 2010, 95, 1838–1845. [Google Scholar] [CrossRef] [Green Version]
- Lou, S.; Lv, H.; Li, Z.; Zhang, L.; Tang, P. Combination therapy of anabolic agents and bisphosphonates on bone mineral density in patients with osteoporosis: A meta-analysis of randomised controlled trials. BMJ Open 2018, 8, e015187. [Google Scholar] [CrossRef] [Green Version]
- Lou, S.; Wang, L.; Wang, Y.; Jiang, Y.; Liu, J.; Wang, Y. Combination therapy of anabolic and nonbisphosphonates antiresorptive agents for the treatment of osteoporosis: A meta-analysis. Medicine 2017, 96, e9534. [Google Scholar] [CrossRef]
- Lou, S.; Lv, H.; Yin, P.; Li, Z.; Tang, P.; Wang, Y. Combination therapy with parathyroid hormone analogs and antiresorptive agents for osteoporosis: A systematic review and meta-analysis of randomized controlled trials. Osteoporos. Int. 2019, 30, 59–70. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A. Lumbar Spine | |||||||||
| VitD | −6.17 (−10.10, −2.24) | ||||||||
| −9.83 (−14.87, −4.80) | Fluoride | 4.52 (0.89, 8.15) | 8.98 (7.01, 10.95) | ||||||
| −7.28 (−12.18, −2.37) | 2.55 (−0.86, 5.97) | SrRan | 0.90 (−1.53, 3.33) | 6.88 (−0.14, 13.89) | |||||
| −2.28 (−6.85, 2.29) | 7.55 (4.62, 10.49) | 5.00 (2.30, 7.69) | Calcitonin | −4.49 (−5.81, −3.16) | −1.90 (−2.75, −1.05) | 1.17 (0.46, 1.87) | |||
| −8.71 (−13.23, −4.18) | 1.13 (−1.74, 4.00) | −1.43 (−4.05, 1.20) | −6.43 (−8.21, −4.64) | PTH | 1.20 (−0.39, 2.79) | 5.42 (1.02, 9.83) | 7.45 (6.59, 8.31) | ||
| −2.31 (−6.99, 2.36) | 7.52 (4.41, 10.62) | 4.96 (2.08, 7.84) | −0.03 (−2.32, 2.25) | 6.39 (4.19, 8.59) | SERM | −3.86 (−6.87, −0.84) | 1.81 (1.04, 2.58) | ||
| −4.27 (−9.24, 0.71) | 5.56 (2.01, 9.11) | 3.01 (−0.34, 6.36) | −1.99 (−4.84, 0.86) | 4.44 (1.65, 7.23) | −1.96 (−4.98, 1.07) | HRT | −4.60 (−6.17, −3.02) | 4.77 (2.97, 6.57) | |
| −8.14 (−13.24, −3.04) | 1.69 (−1.99, 5.38) | −0.86 (−4.35, 2.63) | −5.86 (−8.84, −2.88) | 0.57 (−2.13, 3.26) | −5.82 (−9.01, −2.63) | −3.87 (−7.49, −0.25) | mAb | 8.25 (−1.65, 18.15) | |
| −6.20 (−10.49, −1.91) | 3.63 (0.10, 6.27) | 1.08 (−1.29, 3.45) | −3.92 (−5.48, −2.36) | 2.51 (1.07, 3.95) | −3.88 (−5.74, −2.03) | −1.93 (−4.44, 0.58) | 1.94 (−0.81, 4.69) | BP | 6.06 (5.69, 6.44) |
| −0.38 (−4.75, 3.99) | 9.45 (6.89, 12.01) | 6.90 (4.62, 9.17) | 1.90 (0.43, 3.36) | 8.32 (6.99, 9.66) | 1.93 (0.15, 3.72) | 3.89 (1.41, 6.37) | 7.76 (5.10, 10.41) | 5.82 (5.00, 6.63) | Placebo |
| B. Total Hip | |||||||||
| VitD | −2.20 (−4.20, −0.20) | ||||||||
| −0.40 (−4.78, 4.00) | Fluoride | −2.03 (−8.01, 3.94) | 1.57 (0.92, 2.21) | ||||||
| −4.39 (−8.91, 0.12) | −4.00 (−6.33, −1.67) | SrRan | 1.40 (−0.47, 3.27) | 5.76 (0.87, 10.66) | |||||
| −0.17 (−4.46, 4.12) | 0.22 (−1.66, 2.11) | 4.22 (2.05, 6.39) | Calcitonin | 0.10 (−0.24, 0.44) | −1.10 (−1.82, −0.38) | 1.24 (0.71, 1.77) | |||
| −1.16 (−5.41, 3.08) | −0.77 (−2.53, 0.99) | 3.23 (1.17, 5.28) | −0.99 (−2.45, 0.47) | PTH | −1.20 (−1.80, −0.60) | 1.23 (−0.96, 3.43) | 1.59 (0.97, 2.21) | ||
| −0.70 (−5.17, 3.76) | −0.31 (−2.57, 1.95) | 3.69 (1.19, 6.19) | −0.53 (−2.62, 1.56) | 0.46 (−1.51, 2.44) | SERM | −1.00 (−1.72, −0.28) | 1.73 (1.45, 2.01) | ||
| −2.42 (−6.98, 2.14) | −2.03 (−4.47, 0.42) | 1.97 (−0.70, 4.64) | −2.25 (−4.53, 0.04) | −1.26 (−3.44, 0.93) | −1.72 (−4.32, 0.88) | HRT | 0.19 (−1.03, 1.41) | 3.92 (2.46, 5.38) | |
| −3.50 (−8.15, 1.16) | −3.10 (−5.70, −0.50) | 0.90 (−1.91, 3.70) | −3.32 (−5.74, −0.90) | −2.33 (−4.41, −0.25) | −2.79 (−5.54, −0.04) | −1.07 (−3.98, 1.83) | mAb | 6.80 (6.56, 7.04) | |
| −2.20 (−6.30, 1.90) | −1.80 (−3.35, −0.26) | 2.19 (0.31, 4.07) | −2.03 (−3.28, −0.78) | −1.04 (−2.10, 0.03) | −1.50 (−3.26, 0.26) | 0.22 (−1.76, 2.20) | 1.29 (−0.91, 3.50) | BP | 3.72 (2.83, 4.61) |
| 1.26 (−2.90, 5.41) | 1.65 (0.18, 3.12) | 5.65 (3.83, 7.46) | 1.43 (0.22, 2.64) | 2.42 (1.43, 3.41) | 1.96 (0.22, 3.70) | 3.68 (1.70, 5.65) | 4.75 (2.61, 6.90) | 3.46 (2.83, 4.08) | Placebo |
| C. Distal Radius | |||||||||
| VitK | 1.70 (1.05, 2.35) | −3.50 (−4.16, −2.84) | −3.90 (−4.63, −3.17) | −1.49 (−2.14, −0.84) | 1.29 (0.67, 1.92) | ||||
| 1.47 (−1.83, 4.76) | VitD | −5.20 (−5.72, −4.68) | −5.60 (−6.22, −4.98) | −3.10 (−3.67, −2.53) | −0.30 (−0.84, 0.24) | ||||
| −0.91 (−4.58, 2.75) | −2.38 (−6.50, 1.74) | Fluoride | 2.01 (−2.46, 6.47) | ||||||
| −3.73 (−7.03, −0.44) | −5.20 (−8.74, −1.66) | −2.82 (−6.94, 1.30) | Calcitonin | −0.40 (−1.02, 0.22) | 2.10 (1.53, 2.67) | 4.90 (4.36, 5.44) | |||
| 3.31 (0.08, 6.53) | 1.84 (−1.90, 5.57) | 4.22 (0.68, 7.76) | 7.04 (3.30, 10.77) | PTH | −3.62 (−4.75, −2.48) | −7.80 (−9.70, −5.90) | −1.03 (−5.89, 3.83) | ||
| 0.21 (−4.16, 4.57) | −1.26 (−6.01, 3.49) | 1.12 (−3.42, 5.66) | 3.94 (−0.82, 8.69) | −3.10 (−7.36, 1.16) | SERM | 0.70 (−0.13, 1.53) | |||
| −4.13 (−7.45, −0.81) | −5.60 (−9.16, −2.04) | −3.21 (−7.35, 0.92) | −0.40 (−3.96, 3.16) | −7.44 (−11.19, −3.68) | −4.34 (−9.11, 0.43) | HRT | 2.50 (1.84, 3.16) | 5.30 (4.66, 5.94) | |
| −0.34 (−4.61, 3.94) | −1.81 (−6.48, 2.87) | 0.58 (−3.94, 5.09) | 3.39 (−1.28, 8.07) | −3.64 (−6.45, −0.84) | −0.54 (−5.65, 4.56) | 3.79 (−0.89, 8.48) | mAb | ||
| −1.59 (−4.04, 0.86) | −3.06 (−6.15, 0.02) | −0.68 (−3.77, 2.41) | 2.14 (−0.95, 5.22) | −4.90 (−7.34, −2.46) | −1.80 (−5.70, 2.10) | 2.54 (−0.57, 5.65) | −1.26 (−4.97, 2.46) | BP | 2.22 (1.72, 2.72) |
| 0.91 (−1.53, 3.34) | −0.56 (−3.64, 2.52) | 1.82 (−0.91, 4.55) | 4.64 (1.56, 7.72) | −2.40 (−4.65, −0.15) | 0.70 (−2.92, 4.32) | 5.04 (1.93, 8.14) | 1.24 (−2.35, 4.84) | 2.50 (1.06, 3.94) | Placebo |
| A. Cancer | ||||||
| SERM | 0.65 (0.40, 0.90) | |||||
| 0.62 (0.43, 0.91) | mAb | 1.09 (0.58, 1.61) | 1.03 (0.76, 1.29) | |||
| 0.64 (0.37, 1.10) | 1.03 (0.66, 1.59) | BP | 1.12 (0.45, 1.79) | |||
| 0.65 (0.48, 0.88) | 1.04 (0.83, 1.31) | 1.01 (0.65, 1.58) | Placebo | |||
| B. Cardiovascular Disease | ||||||
| SERM | 1.03 (0.79, 1.26) | |||||
| 0.92 (0.63, 1.35) | mAb | 1.05 (0.86, 1.24) | ||||
| 0.97 (0.56, 1.68) | 1.06 (0.62, 1.79) | BP | 1.00 (0.56, 1.43) | |||
| 0.97 (0.73, 1.29) | 1.05 (0.82, 1.35) | 1.00 (0.63, 1.59) | Placebo | |||
| C. Hip Fracture | ||||||
| Fluoride | 1.04 (−0.34, 2.41) | |||||
| 0.99 (0.20, 4.99) | Calcitonin | 0.75 (−0.25, 1.75) | ||||
| 1.86 (0.36, 9.63) | 1.87 (0.44, 7.98) | PTH | 0.40 (−1.25, 2.04) | 0.75 (−0.75, 2.25) | ||
| 0.78 (0.20, 3.01) | 0.79 (0.26, 2.37) | 0.42 (0.13, 1.33) | SERM | 0.95 (0.50, 1.40) | ||
| 1.24 (0.32, 4.82) | 1.25 (0.41, 3.80) | 0.67 (0.21, 2.13) | 1.58 (0.81, 3.08) | mAb | 0.60 (0.11, 1.09) | |
| 1.28 (0.34, 4.74) | 1.29 (0.45, 3.70) | 0.69 (0.24, 1.99) | 1.63 (0.93, 2.86) | 1.03 (0.57, 1.87) | BP | 0.58 (0.23, 0.92) |
| 0.75 (0.21, 2.65) | 0.75 (0.28, 2.05) | 0.40 (0.14, 1.15) | 0.95 (0.61, 1.50) | 0.60 (0.37, 0.98) | 0.58 (0.42, 0.82) | Placebo |
| D. Death | ||||||
| PTH | 2.17 (1.27, 3.07) | 0.60 (−0.83, 2.03) | ||||
| 1.18 (0.46, 3.05) | SERM | 1.23 (0.79, 1.67) | ||||
| 1.75 (0.65, 4.71) | 1.49 (0.86, 2.58) | mAb | 0.78 (0.50, 1.05) | |||
| 1.49 (0.64, 3.45) | 1.26 (0.74, 2.14) | 0.85 (0.47, 1.53) | BP | 1.02 (0.65, 1.38) | ||
| 1.40 (0.58, 3.39) | 1.19 (0.83, 1.69) | 0.80 (0.52, 1.21) | 0.94 (0.63, 1.40) | Placebo | ||
| A. Medication-Related Osteonecrosis of the Jaw (ONJ) | |||
|---|---|---|---|
| Study | Treatment | Total Number (Incidence) | Follow Up |
| Watts, N. B. 2019 (7-Year FREEDOM extension) | Denosumab (3 + 7 yrs) a Placebo (3 yrs)/Denosumab (7 yrs) | 2343 (7) b 2207 (6) | 10 years 10 years |
| Kendler, D.L. 2018 | Teriparatide Risedronate (BP) | 680 (0) 680 (0) | 24 months 24 months |
| Saag, K.G. 2017 | Romosozumab (mAb) Alendronate (BP) | 2040 (0) 2014 (0) | 1 year 1 year |
| Cosman, F. 2016 | Romosozumab (mAb) Placebo Romosozumab to Denosumab c Placebo to Denosumab | 3581 (1) 3576 (0) 3581 (2) 3576 (1) | 12 months 12 months 24 months 24 months |
| Cummings, S.R. 2009 (FREEDOM study) | Denosumab (mAb) Placebo | 3902 (0) 3906 (0) | 36 months 36 months |
| B. Cancer | |||
| Study | Intervention | Type of Cancers | Number of Events (Percentage of Events, %) |
| (Saag, K. G. et al. 2017) | SC 210mg Romosozumab QM for 12 M Oral 70 mg Alendronate QW for 12 M | All cancers | Romosozumab group: 31 (1.5) Alendronate group: 28 (1.4) |
| (Cosman, F. et al. 2016) | SC 210 mg Romosozumab QM for 12 M Placebo | All cancers | Romosozumab group: 59 (1.6) Placebo group: 69 (1.9) |
| (Palacios, S. et al. 2015) | Oral 20 mg Bazedoxifene daily for 7 yrs Placebo | Breast cancer | Bazedoxifene group: 23 (0.6) Placebo group: 11 (0.6) |
| (LaCroix, A. Z. et al. 2010) | Oral 0.5 mg Lasofoxifene daily for 5 yrs Placebo | Breast cancer | Lasofoxifene group: 5 (0.41) Placebo group: 24 (1.97) |
| (Christiansen, C. et al. 2010) | Oral 20 mg Bazedoxifene daily for 3 yrs Oral 60 mg Raloxifene daily for 3 yrs Placebo | Breast cancer | Bazedoxifene group: 6 (0.3) Raloxifene group: 7 (0.4) Placebo group: 8 (0.4) |
| (Cummings, S. R. et al. 2009) | SC 60 mg Denosumab Q6 M for 36 M Placebo | All cancers | Denosumab group: 187 (4.8) Placebo group: 166 (4.3) |
| (Martino, S. et al. 2005) | Oral 60 mg Raloxifene daily for 8 yrs Placebo | All cancers (excluding non-melanoma skin cancer) | Raloxifene group: 156 (5.7) Placebo group: 110 (8.6) |
| (Barrett-Connor, E. et al. 2004) | Oral 60 or 120 mg Raloxifene daily for 4 yrs Placebo | Invasive breast cancer, endometrial cancer | Invasive breast cancer Raloxifene group: 17 (0.1) Placebo group: 35 (0.4) Endometrial cancer Raloxifene group: 7 (0.04) Placebo group: 5 (0.06) |
| (Martino, S. et al. 2004) | Oral 60 mg Raloxifene daily for 8 yrs Placebo | Breast cancers | Raloxifene group: 31 (0.9) Placebo group: 30 (1.8) |
| (Reginster, J. Y. et al. 2000) | Oral 5 mg Risedronate daily for 1 yr Placebo | All cancers | Risedronate group: 19 (4.7) Placebo group: 17 (4.2) |
| C. Death | |||
| Study | Intervention | Reasons of Death | Number of Events (Percentage of Events, %) |
| (Kendler, D. L. et al. 2018) | SC 20 ug Teriparatide daily for 24 M Oral 35 mg Risedronate weekly for 24 M | N/A (1) | Teriparatide group: 15 (2.2) Risedronate group: 7 (1.0) |
| (Koh, J. M. et al. 2016) | SC 60 mg Denosumab Q6 M for 6 M Placebo | Traumatic subdural hemorrhage due to motorcycle accident | Denosumab group: 1 (1) Placebo group: 0 (0) |
| (Cosman, F. et al. 2016) | SC 210 mg Romosozumab QM for 12 M Placebo | Romosozumab: 17 from Cardiovascular causes Placebo: 15 from Cardiovascular causes | Romosozumab group: 23 (0.6) Placebo group: 29 (0.8) |
| (Miller, P. D. et al. 2016) | SC 80 ug Abaloparatide daily for 1 yr SC 20 ug Teriparatide daily for 1 yr Placebo | Abaloparatide: sepsis, bronchiectasis, ischemic heart disease Teriparatide: pancreatic cancer, general health deterioration, cardiorespiratory arrest Placebo: bowel cancer, intestinal obstruction, myocardial infarction, dissecting aneurysm of the aorta, sudden death | Abaloparatide group: 3 (0.4) Teriparatide group: 3 (0.4) Placebo group: 5 (0.6) |
| (Palacios, S. et al. 2015) | Oral 20 mg Bazedoxifene daily for 7 yrs Placebo | N/A (2) | Bazedoxifene group: 52 (1.4) Placebo group: 18 (1.0) |
| (Cummings, S. R. et al. 2010) | Oral 0.25 mg Lasofoxifene daily for 5 yrs Placebo | Lasofoxifene: 34 from cancers Placebo: 20 from cancers | Lasofoxifene group: 90 (3.2) Placebo group: 65 (2.3) |
| (Cummings, S. R. et al. 2009) | SC 60 mg Denosumab Q6 M for 36 M Placebo | N/A | Denosumab group: 70 (1.8) Placebo group: 90 (2.3) |
| (Black, D. M. et al. 2007) | IV (15 min) 5 mg Zoldronic acid yearly for 3 yrs Placebo | Zoldronic acid: 20 from stroke; 39 from cardiovascular causes Placebo: 11 from stroke; 33 from cardiovascular causes | Zoldronic acid group: 130 (3.4) Placebo group: 112 (2.9) |
| (Martino, S. et al. 2005) | Oral 60 mg Raloxifene daily for 8 yrs Placebo | N/A | Raloxifene group: 47 (1.7) Placebo group: 29 (2.3) |
| (Boonen, S. et al. 2004) | Oral 5 mg Risedronate daily for 3 yrs Placebo | N/A | Risedronate group: 40 (5.7) Placebo group: 49 (7.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, S.-Y.; Hung, M.-C.; Chang, S.-F.; Tsuang, F.-Y.; Chang, J.Z.-C.; Sun, J.-S. Efficacy and Safety of Postmenopausal Osteoporosis Treatments: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 3043. https://doi.org/10.3390/jcm10143043
Lin S-Y, Hung M-C, Chang S-F, Tsuang F-Y, Chang JZ-C, Sun J-S. Efficacy and Safety of Postmenopausal Osteoporosis Treatments: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2021; 10(14):3043. https://doi.org/10.3390/jcm10143043
Chicago/Turabian StyleLin, Shih-Yin, Min-Chih Hung, Shih-Fu Chang, Fon-Yih Tsuang, Jenny Zwei-Chieng Chang, and Jui-Sheng Sun. 2021. "Efficacy and Safety of Postmenopausal Osteoporosis Treatments: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 10, no. 14: 3043. https://doi.org/10.3390/jcm10143043
APA StyleLin, S.-Y., Hung, M.-C., Chang, S.-F., Tsuang, F.-Y., Chang, J. Z.-C., & Sun, J.-S. (2021). Efficacy and Safety of Postmenopausal Osteoporosis Treatments: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine, 10(14), 3043. https://doi.org/10.3390/jcm10143043