
Uric Acid as a Predictor for Early Allograft Dysfunction after Living Donor Liver Transplantation: A Prospective Observational Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives
2.2. Data Collection and Variable Definition
2.3. Statistical Analysis
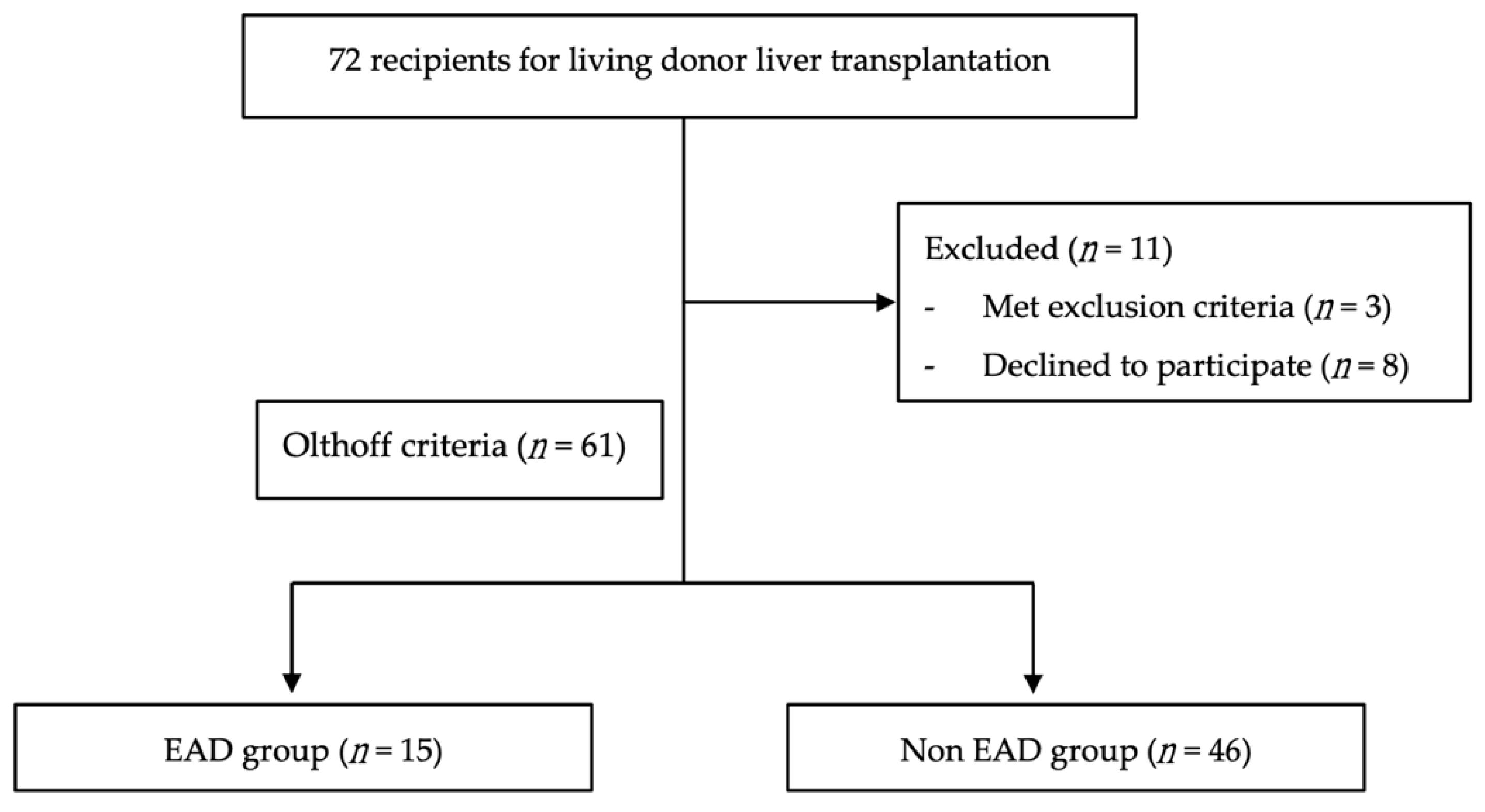
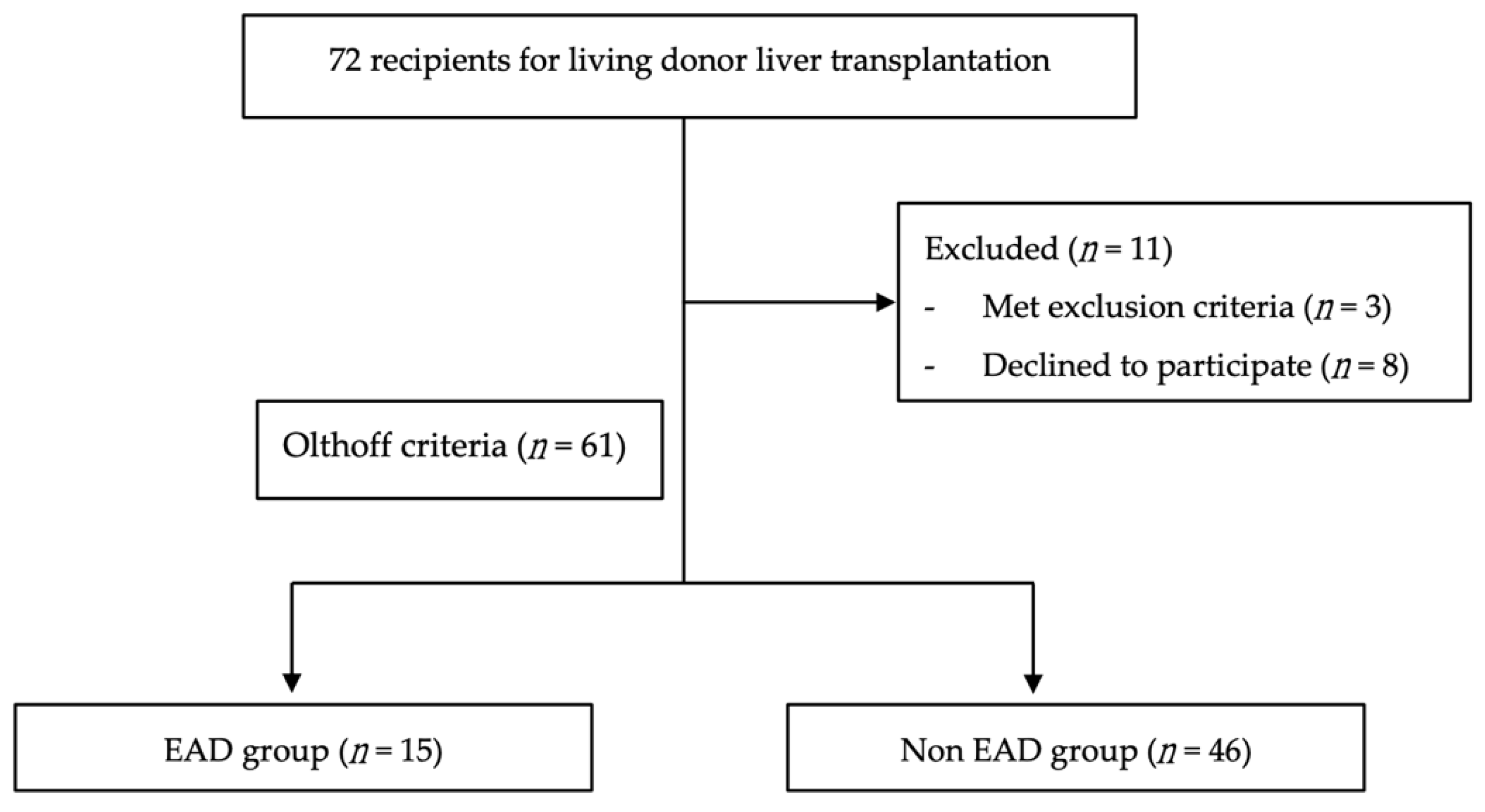
3. Results
3.1. Baseline Characteristics
3.2. SUA Level in Different Subgroups
3.3. Risk Factors for Early Allograft Dysfunction
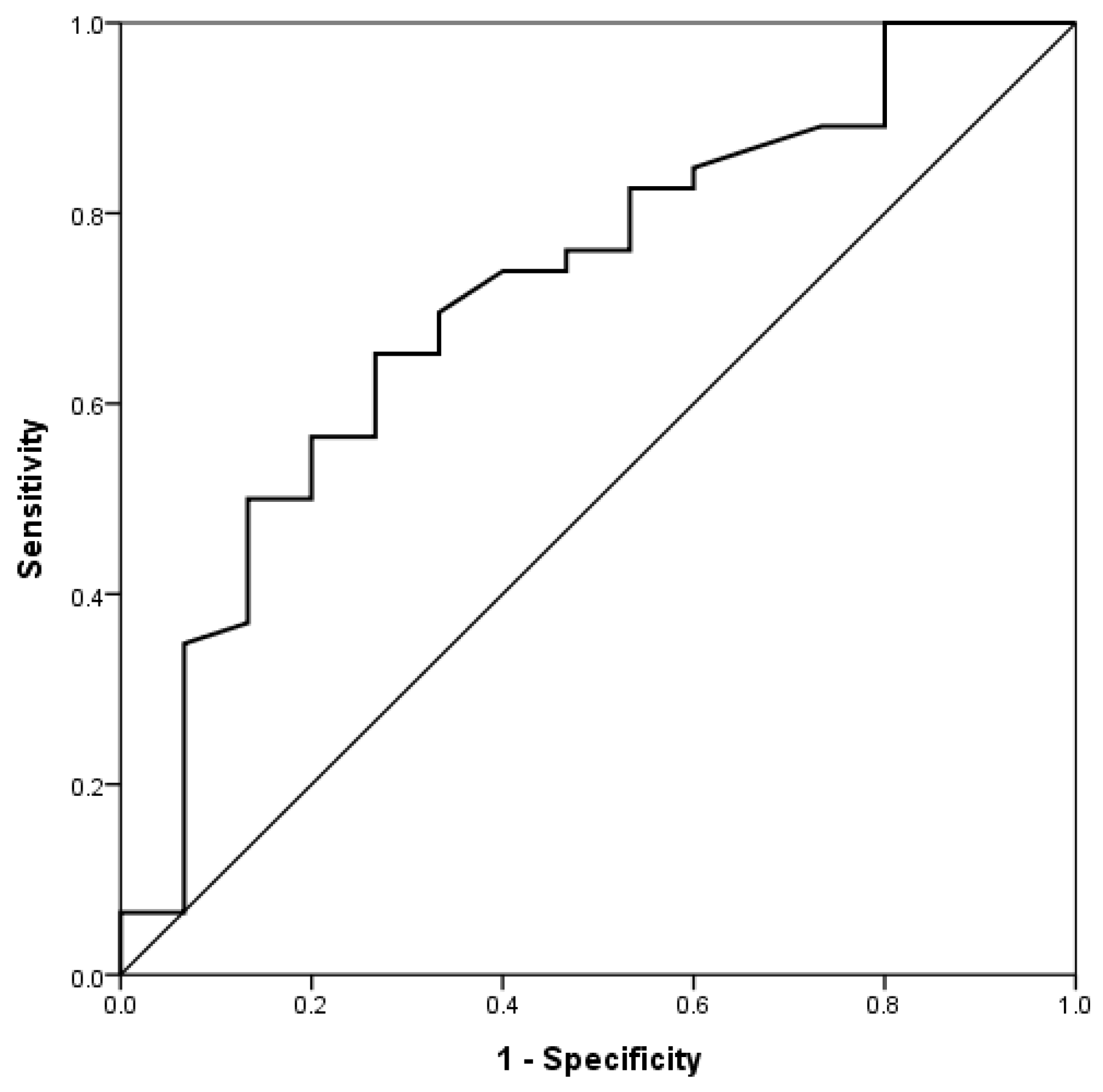
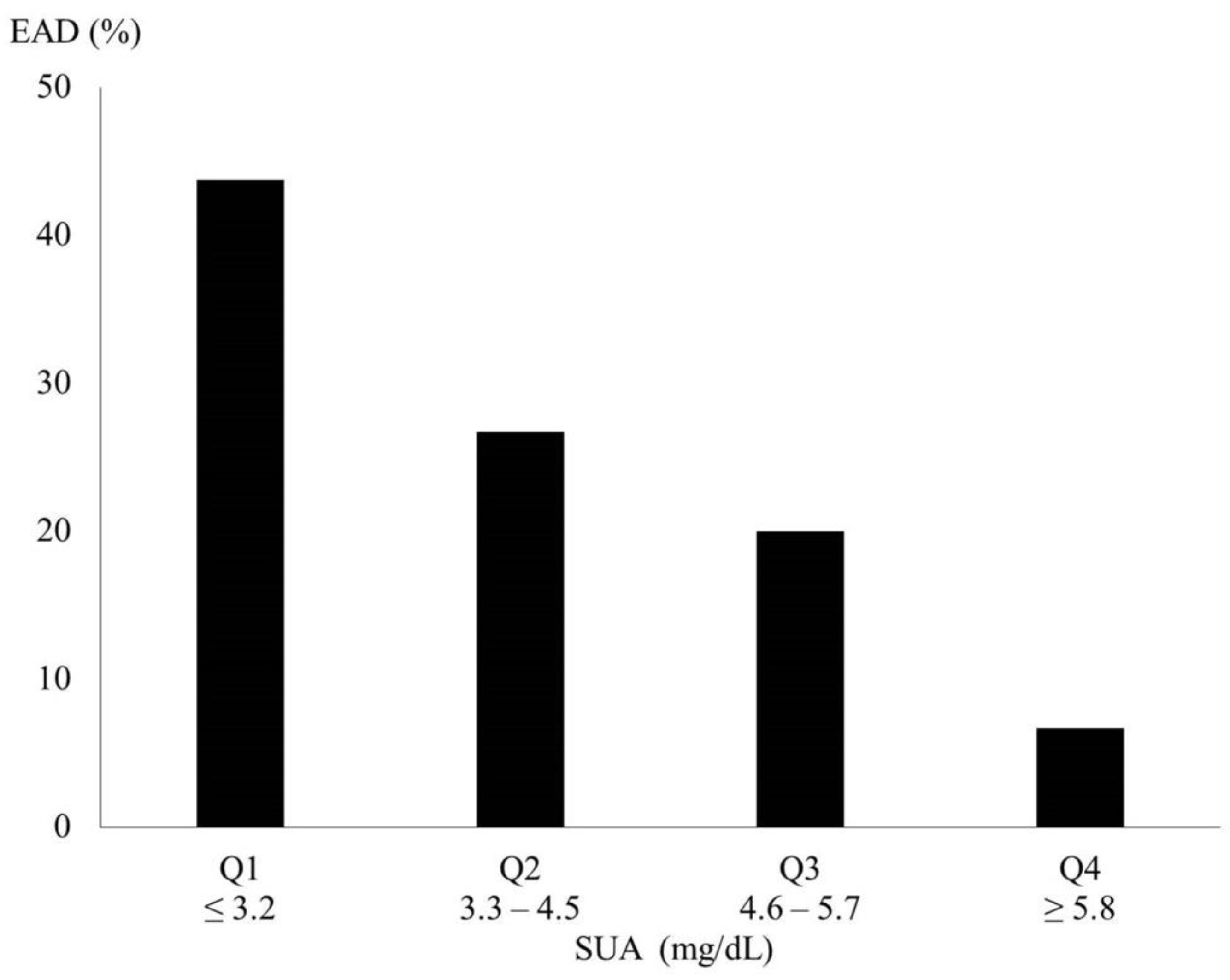
3.4. SUA and the Association with Early Allograft Dysfunction
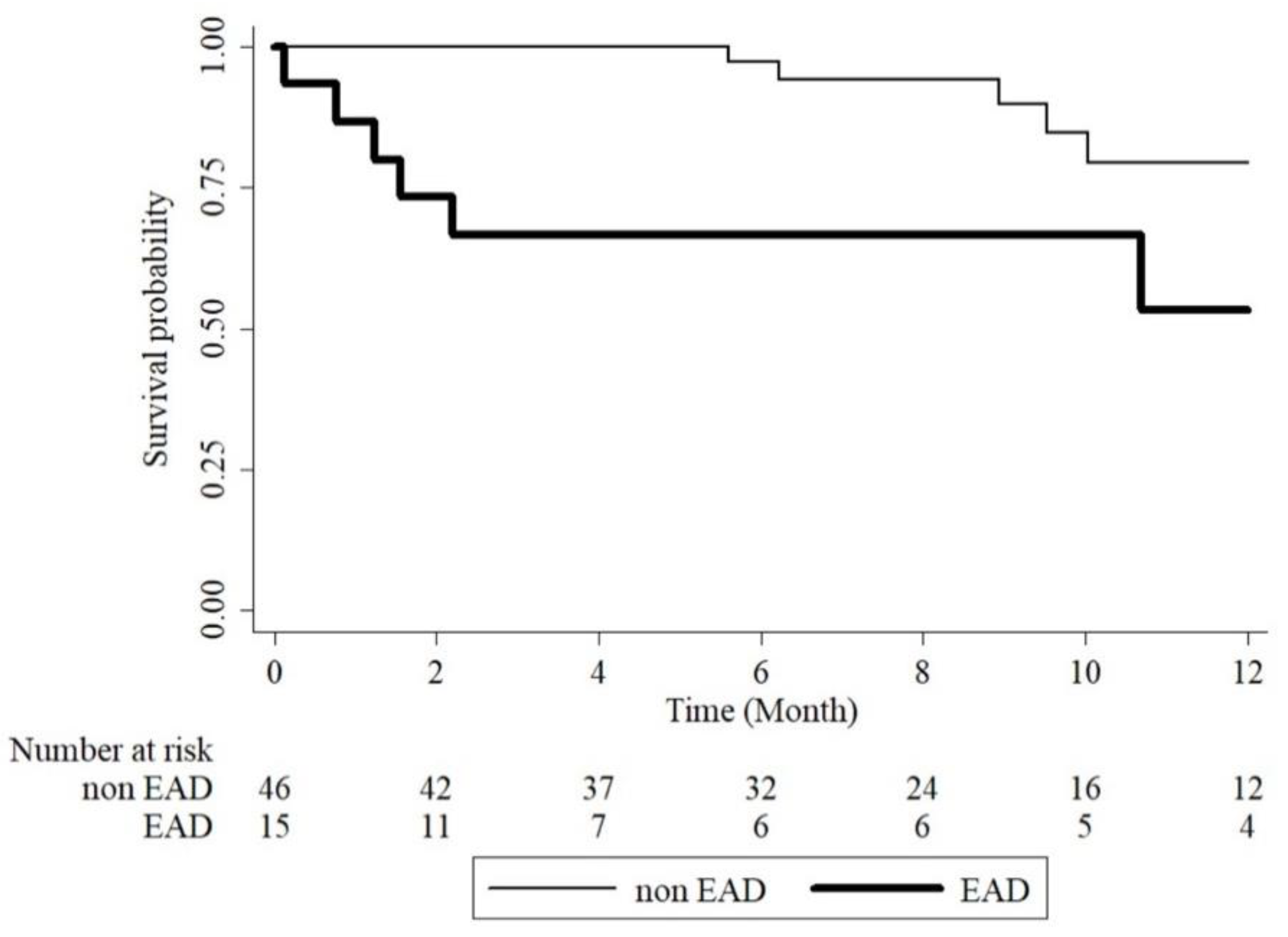
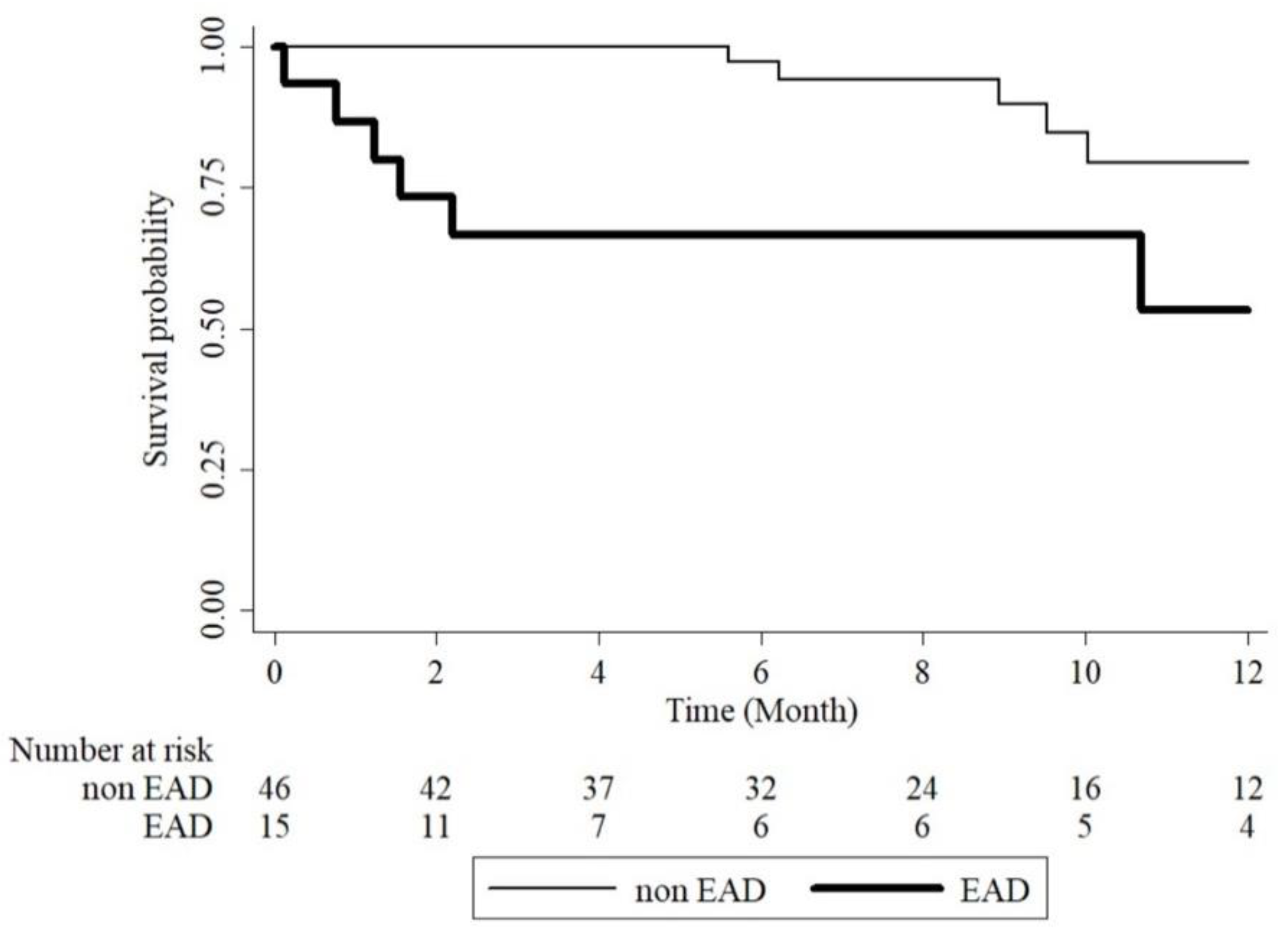
3.5. Early Allograft Dysfunction and One Year Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lo, C.-M.; Fan, S.-T.; Liu, C.-L.; Lo, R.J.W.; Lai, C.-L.; Chan, J.K.F.; Ng, L.; Fung, I.A.; Wong, J. Adult-to-Adult Living Donor Liver Transplantation Using Extended Right Lobe Grafts. Ann. Surg. 1997, 226, 261–270. [Google Scholar] [CrossRef]
- Brea-Gómez, E.; Villar-Quintana, R.; Plata-Illescas, C.; Zambudio-Carroll, N.; Lopez-Garrido, M.A.; Nogueras-Lopez, F.; Muffak-Granero, K.; Becerra-Massare, A.; Villegas-Herrera, M.T.; Segura Jiménez, I.; et al. Analysis of the Predictive Ability for Graft Loss and Mortality of Two Criteria for Early Allograft Dysfunction After Liver Transplantation. Transplant. Proc. 2018, 50, 605–609. [Google Scholar] [CrossRef]
- Wadei, H.M.; Lee, D.D.; Croome, K.P.; Mai, M.L.; Golan, E.; Brotman, R.; Keaveny, A.P.; Taner, C.B. Early Allograft Dysfunction after Liver Transplantation Is Associated with Short- and Long-Term Kidney Function Impairment. Am. J. Transplant. 2016, 16, 850–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deschenes, M. Early Allograft Dysfunction: Causes, Recognition, and Management. Liver Transplant. 2013, 19, S6–S8. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.D.; Croome, K.P.; Shalev, J.A.; Musto, K.R.; Sharma, M.; Keaveny, A.P.; Taner, C.B. Early Allograft Dysfunction after Liver Transplantation: An Intermediate Outcome Measure for Targeted Improvements. Ann. Hepatol. 2016, 15, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Pomposelli, J.J.; Goodrich, N.P.; Emond, J.C.; Humar, A.; Baker, T.B.; Grant, D.R.; Fisher, R.A.; Roberts, J.P.; Olthoff, K.M.; Gillespie, B.W.; et al. Patterns of Early Allograft Dysfunction in Adult Live Donor Liver Transplantation: The A2ALL Experience. Transplantation 2016, 100, 1490–1499. [Google Scholar] [CrossRef]
- Álvarez-Lario, B.; MacArrón-Vicente, J. Is There Anything Good in Uric Acid? QJM Int. J. Med. 2011, 104, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Ndrepepa, G. Uric Acid and Cardiovascular Disease. Clin. Chim. Acta 2018, 484, 150–163. [Google Scholar] [CrossRef]
- Maiuolo, J.; Oppedisano, F.; Gratteri, S.; Muscoli, C.; Mollace, V. Regulation of Uric Acid Metabolism and Excretion. Int. J. Cardiol. 2016, 213, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Wen, M.; Zhou, B.; Chen, Y.-H.; Ma, Z.-L.; Gou, Y.; Zhang, C.-L.; Yu, W.-F.; Jiao, L. Serum Uric Acid Levels in Patients with Parkinson’s Disease: A Meta-Analysis. PLoS ONE 2017, 12, e0173731. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Gajardo, R.; Matamala, J.M.; Gutiérrez, R.; Lozano, P.; Cortés-Fuentes, I.A.; Sotomayor, C.G.; Bustamante, G.; Pasten, J.A.; Vargas, G.; Guerrero, R.; et al. Relationship between Infarct Size and Serum Uric Acid Levels during the Acute Phase of Stroke. PLoS ONE 2019, 14, e0219402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boccardi, V.; Carino, S.; Marinelli, E.; Lapenna, M.; Caironi, G.; Bianco, A.R.; Cecchetti, R.; Ruggiero, C.; Mecocci, P.; Defanti, C.A.; et al. Uric Acid and Late-Onset Alzheimer’s Disease: Results from the ReGAl 2.0 Project. Aging Clin. Exp. Res. 2020, 33, 361–366. [Google Scholar] [CrossRef]
- Mikami, T.; Sorimachi, M. Uric Acid Contributes Greatly to Hepatic Antioxidant Capacity besides Protein. Physiol. Res. 2017, 66, 1001–1007. [Google Scholar] [CrossRef]
- Olthoff, K.M.; Kulik, L.; Samstein, B.; Kaminski, M.; Abecassis, M.; Emond, J.; Shaked, A.; Christie, J.D. Validation of a Current Definition of Early Allograft Dysfunction in Liver Transplant Recipients and Analysis of Risk Factors. Liver Transplant. 2010, 16, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Xin, E.Y.; Liao, B.; Lai, L.J.; Han, M.; Wang, X.P.; Ju, W.Q.; Wang, D.P.; Guo, Z.Y.; He, X.S. Development and Validation of a Nomogram for Predicting Incidence of Early Allograft Dysfunction Following Liver Transplantation. Transplant. Proc. 2017, 49, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Ko, Y.C.; Tsai, H.I.; Lee, C.W.; Lin, J.R.; Lee, W.C.; Yu, H.P. A Nomogram for Prediction of Early Allograft Dysfunction in Living Donor Liver Transplantation. Medicine 2020, 99, e22749. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wang, H.; Yang, J.; Jiang, L.; Yang, J.; Wang, W.; Yan, L.; Wen, T.; Li, B.; Xu, M. Immediate Postoperative Low Platelet Counts after Living Donor Liver Transplantation Predict Early Allograft Dysfunction. Medicine 2015, 94, e1373. [Google Scholar] [CrossRef]
- Michelis, M.F.; Warms, P.C.; Fusco, R.D.; Davis, B.B. Hypouricemia and Hyperuricosuria in Laennec cirrhosis. Arch. Intern. Med. 1974, 134, 681–683. [Google Scholar] [CrossRef]
- de Oliveira, E.P.; Burini, R.C. High Plasma Uric Acid Concentration: Causes and Consequences. Diabetol. Metab. Syndr. 2012, 4, 12. [Google Scholar] [CrossRef] [Green Version]
- Mrug, S.; Mrug, M. Uric Acid Excretion Predicts Increased Aggression in Urban Adolescents. Physiol. Behav. 2016, 163, 144–148. [Google Scholar] [CrossRef]
- Dar, W.A.; Sullivan, E.; Bynon, J.S.; Eltzschig, H.; Ju, C. Ischaemia Reperfusion Injury in Liver Transplantation: Cellular and Molecular Mechanisms. Liver Int. 2019, 39, 788–801. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Yang, N.; Lin, S.; Zhang, F. Suitable Concentrations of Uric Acid Can Reduce Cell Death in Models of OGD and Cerebral Ischemia–Reperfusion Injury. Cell. Mol. Neurobiol. 2017, 37, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Cheng, G.; Wang, R.; Zhang, B.; Deng, X. The Protective Effect of Uric Acid in Reducing TLR4/NF-ΚB Activation through the Inhibition of HMGB1 Acetylation in a Model of Ischemia–Reperfusion Injury in Vitro. Mol. Biol. Rep. 2020, 47, 3233–3240. [Google Scholar] [CrossRef]
- Ya, B.; Liu, Q.; Li, H.; Cheng, H.; Yu, T.; Chen, L.; Wang, Y.; Yuan, L.; Li, W.; Liu, W.; et al. Uric Acid Protects against Focal Cerebral Ischemia/Reperfusion-Induced Oxidative Stress via Activating Nrf2 and Regulating Neurotrophic Factor Expression. Oxidative Med. Cell. Longev. 2018, 2018, 6069150. [Google Scholar] [CrossRef] [PubMed]
- Vukovic, J.; Modun, D.; Budimir, D.; Sutlovic, D.; Salamunic, I.; Zaja, I.; Boban, M. Acute, Food-Induced Moderate Elevation of Plasma Uric Acid Protects against Hyperoxia-Induced Oxidative Stress and Increase in Arterial Stiffness in Healthy Humans. Atherosclerosis 2009, 207, 255–260. [Google Scholar] [CrossRef]
- Kikuchi, K.; Setoyama, K.; Tanaka, E.; Otsuka, S.; Terashi, T.; Nakanishi, K.; Takada, S.; Sakakima, H.; Ampawong, S.; Kawahara, K.; et al. Uric Acid Enhances Alteplase-Mediated Thrombolysis as an Antioxidant. Sci. Rep. 2018, 8, 15844. [Google Scholar] [CrossRef] [Green Version]
- Chamorro, Á.; Amaro, S.; Castellanos, M.; Segura, T.; Arenillas, J.; Martí-Fábregas, J.; Gállego, J.; Krupinski, J.; Gomis, M.; Cánovas, D.; et al. Safety and Efficacy of Uric Acid in Patients with Acute Stroke (URICO-ICTUS): A Randomised, Double-Blind Phase 2b/3 Trial. Lancet Neurol. 2014, 13, 453–460. [Google Scholar] [CrossRef]
- Ekpenyong, C.E.; Daniel, N. Roles of Diets and Dietary Factors in the Pathogenesis, Management and Prevention of Abnormal Serum Uric Acid Levels. Pharma Nutr. 2015, 3, 29–45. [Google Scholar] [CrossRef]
- Kanbay, M.; Jensen, T.; Solak, Y.; Le, M.; Roncal-Jimenez, C.; Rivard, C.; Lanaspa, M.A.; Nakagawa, T.; Johnson, R.J. Uric Acid in Metabolic Syndrome: From an Innocent Bystander to a Central Player. Eur. J. Intern. Med. 2016, 29, 3–8. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Recipient (N = 61) | Donor (N = 61) |
|---|---|---|
| Age (years) | 55.13 ± 10.43 | 32.34 ± 9.21 |
| MELD | 16.67 ± 8.09 | |
| BMI (kg/m2) | 25.28 ± 4.27 | 23.00 ± 2.64 |
| Preoperative ALT (U/L) | 69.31 ± 149.85 | |
| Preoperative SUA (mg/dL) | 4.83 ± 2.58 | |
| Preoperative UUA (mg/dL) | 54.40 ± 59.65 | |
| Preoperative BUN (mg/dL) | 18.01 ± 11.78 | |
| Preoperative Cre (mg/dL) | 0.87 ± 0.49 | |
| Preoperative eGFR (mL/min/1.73 m2) | 113.69 ± 50.12 | |
| Gender | ||
| Male | 44 (72.13) | 33 (54.10) |
| Female | 17 (27.87) | 28 (45.90) |
| Blood type | ||
| A | 20 (32.79) | 17 (27.87) |
| B | 15 (24.59) | 11 (18.03) |
| O | 24 (39.34) | 33 (54.10) |
| AB | 2 (3.28) | 0 (0) |
| ABO incompatibility | 5 (8.20) | |
| Comorbidity | ||
| HBV | 32 (52.46) | |
| HCV | 11 (18.03) | |
| Alcoholism | 20 (32.79) | |
| HCC | 27 (44.26) | |
| CKD | 8 (13.11) | |
| DM | 15 (24.59) | |
| HTN | 21 (34.43) | |
| Gout | 3 (4.92) | |
| Medication (Diuretics/ACEi/ARB) | 42 (68.85) | |
| Intraoperative Parameters | ||
| Graft size (g) | 640.41 ± 131.43 | |
| Blood loss (mL) | 1977.38 ± 2181.03 | |
| GRWR (%) | 0.98 ± 0.21 | |
| Cold ischemia time (min) | 39.77 ± 25.97 | |
| Warm ischemia time (min) | 16.41 ± 4.19 | |
| Outcomes | ||
| EAD | 15 (24.59) | |
| 1 year mortality | 11 (18.03) | |
| Characteristics | Non-EAD (N = 46) | EAD (N = 15) | p-Value |
|---|---|---|---|
| Recipient | |||
| Age (years) | 56.37 ± 10.41 | 51.33 ± 9.88 | 0.105 |
| MELD | 15.20 ± 7.66 | 21.20 ± 7.92 | 0.011 |
| BMI (kg/m2) | 25.13 ± 4.10 | 25.71 ± 4.86 | 0.656 |
| Sex | |||
| Male | 33 (71.74) | 11 (73.33) | 1.000 |
| Female | 13 (28.26) | 4 (26.67) | |
| Blood type | |||
| A | 18 (39.13) | 2 (13.33) | 0.162 |
| B | 11 (23.91) | 4 (26.67) | |
| O | 15 (32.61) | 9 (60.00) | |
| AB | 2 (4.35) | 0 (0.00) | |
| ABO incompatible | 3 (6.52) | 2 (13.33) | 0.589 |
| Preoperative ALT (U/L) | 68.13 ± 169.1 | 72.93 ± 65.73) | 0.874 |
| Preoperative SUA (mg/dL) | 5.26 ± 2.57 | 3.51 ± 2.19 | 0.021 |
| Low UA (≤4.4 mg/dL) | 16 (34.78) | 11 (73.33) | 0.009 |
| High UA (>4.4 mg/dL) | 30 (65.22) | 4 (26.67) | |
| Preoperative UUA (mg/dL) | 59.45 ± 66.80 | 38.93 ± 23.79 | 0.082 |
| Preoperative BUN (mg/dL) | 17.89 ± 11.92 | 18.37 ± 11.74 | 0.891 |
| Preoperative Cre (mg/dL) | 0.83 ± 0.46 | 0.98 ± 0.58 | 0.309 |
| Preoperative eGFR (mL/min/1.73 m2) | 114.61 ± 44.77 | 110.88 ± 65.68 | 0.805 |
| Comorbidity | |||
| HBV | 25 (54.35) | 7 (46.67) | 0.605 |
| HCV | 7 (15.22) | 4 (26.67) | 0.439 |
| Alcoholism | 16 (34.78) | 4 (26.67) | 0.754 |
| HCC | 23 (50.00) | 4 (26.67) | 0.114 |
| CKD | 5 (10.87) | 5 (33.33) | 0.101 |
| DM | 10 (21.74) | 5 (33.33) | 0.491 |
| HTN | 16 (34.78) | 5 (33.33) | 0.918 |
| Gout | 3 (6.52) | 0 (0.00) | 0.569 |
| Medication (Diuretics/ACEi/ARB) | 32 (69.57) | 10 (66.67) | 0.833 |
| Donor | |||
| Age (years) | 31.61 ± 9.13 | 34.60 ± 9.38 | 0.278 |
| BMI (kg/m2) | 22.87 ± 2.85 | 23.38 ± 1.87 | 0.521 |
| Sex | |||
| Male | 25 (54.35) | 8 (53.33) | 0.945 |
| Female | 21 (45.65) | 7 (46.67) | |
| Blood type | |||
| A | 15 (32.61) | 2 (13.33) | 0.345 |
| B | 8 (17.39) | 3 (20.00) | |
| O | 23 (50.00) | 10 (66.67) | |
| AB | 0 (0.00) | 0 (0.00) | |
| Intraoperative Parameters | |||
| Graft size (g) | 635.50 ± 127.60 | 655.30 ± 146.20 | 0.617 |
| Blood loss (mL) | 1704.80 ± 2035.60 | 2813.30 ± 2464.80 | 0.087 |
| GRWR (%) | 0.97 ± 0.20 | 1.00 ± 0.27 | 0.588 |
| Cold ischemia (min) | 39.07 ± 25.4 | 41.93 ± 28.48 | 0.714 |
| Warm ischemia (min) | 16.07 ± 4.41 | 17.47 ± 3.31 | 0.264 |
| Outcomes | |||
| 1 year mortality | 5 (10.87) | 6 (40.00) | 0.019 |
| Sex | Female (N = 17) | Male (N = 44) | p-Value |
| SUA (mg/dL) | 4.81 ± 2.68 | 4.84 ± 2.57 | 0.960 |
| UUA (mg/dL) | 60.36 ± 108.11 | 52.10 ± 24.42 | 0.759 |
| Alcoholism | Non alcoholism (N = 41) | Alcoholism (N = 20) | p-Value |
| SUA (mg/dL) | 4.87 ± 2.73 | 4.77 ± 2.30 | 0.888 |
| UUA (mg/dL) | 56.62 ± 71.25 | 49.85 ± 22.74 | 0.582 |
| CKD | Non-CKD (N = 51) | CKD (N = 10) | p-Value |
| SUA (mg/dL) | 4.51 ± 2.13 | 6.48 ± 3.94 | 0.155 |
| UUA (mg/dL) | 58.02 ± 63.85 | 35.97 ± 24.94 | 0.073 |
| DM | Non-DM (N = 46) | DM (N = 15) | p-Value |
| SUA (mg/dL) | 4.56 ± 2.31 | 5.67 ± 3.21 | 0.151 |
| UUA (mg/dL) | 58.05 ± 66.91 | 43.323 ± 26.10 | 0.220 |
| HTN | Non-HTN (N = 40) | HTN (N = 21) | p-Value |
| SUA (mg/dL) | 5.01 ± 2.56 | 4.49 ± 2.65 | 0.458 |
| UUA (mg/dL) | 60.11 ± 71.65 | 43.54 ± 21.78 | 0.183 |
| Characteristics | Univariate Analysis | Multivariate Analysis (Stepwise Selection) | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Recipient | ||||
| Age | 0.96 (0.91–1.01) | 0.117 | ||
| MELD | 1.09 (1.02–1.18) | 0.018 | ||
| BMI | 1.03 (0.90–1.18) | 0.650 | ||
| Sex | ||||
| Male | 1.08 (0.29–4.02) | 0.905 | ||
| Female | Ref | |||
| Blood type | ||||
| A | Ref | |||
| B | 3.27 (0.51–20.93) | 0.215 | ||
| O | 5.40 (1.01–28.93) | 0.049 | ||
| AB | – | |||
| ABO incompatible | 2.21 (0.33–14.65) | 0.413 | ||
| Preoperative SUA | ||||
| Low UA (≤4.4 mg/dL) | 5.16 (1.41–18.83) | 0.013 | 5.39 (1.29–22.49) | 0.021 |
| High UA (>4.4 mg/dL) | Ref | |||
| ALT | 1.00 (1.00–1.00) | 0.914 | ||
| Comorbidity | ||||
| HBV | 0.74 (0.23–2.37) | 0.606 | ||
| HCV | 2.03 (0.50–8.21) | 0.323 | ||
| Alcoholism | 0.68 (0.19–2.49) | 0.562 | ||
| HCC | 0.36 (0.10–1.31) | 0.122 | ||
| CKD | 4.10 (0.99–16.95) | 0.051 | ||
| DM | 1.80 (0.50–6.49) | 0.369 | ||
| HTN | 0.94 (0.27–3.22) | 0.918 | ||
| Gout | – | – | ||
| Medication (Diuretics/ACEi/ARB) | 0.88 (0.25–3.04) | 0.833 | ||
| Donor | ||||
| Age | 1.04 (0.97–1.10) | 0.276 | ||
| BMI | 1.08 (0.86–1.35) | 0.514 | ||
| Sex | ||||
| Male | 0.96 (0.30–3.09) | 0.945 | ||
| Female | Ref | |||
| Blood type | ||||
| A | Ref | |||
| B | 2.81 (0.39–20.46) | 0.307 | ||
| O | 3.26 (0.63–17.01) | 0.161 | ||
| AB | – | – | ||
| Intraoperative Parameters | ||||
| Graft | 1.00 (1.00–1.01) | 0.610 | ||
| Blood loss | 1.00 (1.00–1.00) | 0.096 | ||
| GRWR | 2.12 (0.15–30.71) | 0.582 | ||
| Cold ischemia time | 1.00 (0.98–1.03) | 0.709 | ||
| Warm ischemia time | 1.08 (0.94–1.24) | 0.264 | ||
| Characteristics | Univariate Analysis | Multivariate Analysis (Stepwise Selection) | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Recipient | ||||
| Age | 1.05 (0.97–1.14) | 0.217 | ||
| MELD | 0.99 (0.92–1.08) | 0.879 | ||
| BMI | 0.88 (0.74–1.04) | 0.129 | ||
| Sex | ||||
| Male | 1.91 (0.41–8.86) | 0.409 | ||
| Female | Ref | |||
| Blood type | ||||
| A | Ref | |||
| B | 1.14 (0.16–8.14) | 0.893 | ||
| O | 3.78 (0.78–18.31) | 0.098 | ||
| AB | – | 0.995 | ||
| ABO incompatible | 1.18 (0.15–9.23) | 0.876 | ||
| Preoperative SUA | ||||
| Low UA (≤4.4 mg/dL) | 1.18 (0.36–2.87) | 0.785 | ||
| High UA (>4.4 mg/dL) | Ref | |||
| ALT | 0.99 (0.98–1.01) | 0.451 | ||
| Comorbidity | ||||
| HBV | 1.45 (0.42–4.96) | 0.555 | ||
| HCV | 0.62 (0.08–4.88) | 0.617 | ||
| Alcoholism | 0.49 (0.11–2.29) | 0.367 | ||
| HCC | 1.58 (0.48–5.51) | 0.450 | ||
| CKD | 1.56 (0.34–7.26) | 0.567 | ||
| DM | 1.33 (0.34–7.40) | 0.563 | ||
| HTN | 1.75 (0.53–5.74) | 0.357 | ||
| Gout | 2.91 (0.62–13.69) | 0.177 | ||
| Medication (Diuretics/ACEi/ARB) | 0.94 (0.28–3.22) | 0.923 | ||
| EAD | 4.4 (1.33–14.53) | 0.015 | 6.69 (1.66–26.92) | 0.008 |
| Donor | ||||
| Age | 1.00 (0.94–1.06) | 0.962 | ||
| BMI | 0.95 (0.76–1.20) | 0.662 | ||
| Sex | ||||
| Male | 1.84 (0.54–6.33) | 0.332 | ||
| Female | Ref | |||
| Blood type | ||||
| A | Ref | |||
| B | 1.07 (0.18–6.43) | 0.939 | ||
| O | 1.25 (0.31–5.01) | 0.754 | ||
| AB | – | – | ||
| Intraoperative Parameters | ||||
| Graft | 1.00 (0.99–1.00) | 0.253 | ||
| Blood loss | 1.00 (1.00–1.00) | 0.451 | ||
| GRWR | 0.78 (0.06–10.98) | 0.856 | ||
| Cold ischemia | 1.00 (0.98–1.02) | 0.961 | ||
| Warm ischemia | 0.93 (0.80–1.07) | 0.292 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, L.-M.; Tsai, H.-I.; Lee, C.-W.; Chen, H.-M.; Lee, W.-C.; Yu, H.-P. Uric Acid as a Predictor for Early Allograft Dysfunction after Living Donor Liver Transplantation: A Prospective Observational Study. J. Clin. Med. 2021, 10, 2729. https://doi.org/10.3390/jcm10122729
Hu L-M, Tsai H-I, Lee C-W, Chen H-M, Lee W-C, Yu H-P. Uric Acid as a Predictor for Early Allograft Dysfunction after Living Donor Liver Transplantation: A Prospective Observational Study. Journal of Clinical Medicine. 2021; 10(12):2729. https://doi.org/10.3390/jcm10122729
Chicago/Turabian StyleHu, Li-Min, Hsin-I Tsai, Chao-Wei Lee, Hui-Ming Chen, Wei-Chen Lee, and Huang-Ping Yu. 2021. "Uric Acid as a Predictor for Early Allograft Dysfunction after Living Donor Liver Transplantation: A Prospective Observational Study" Journal of Clinical Medicine 10, no. 12: 2729. https://doi.org/10.3390/jcm10122729
APA StyleHu, L.-M., Tsai, H.-I., Lee, C.-W., Chen, H.-M., Lee, W.-C., & Yu, H.-P. (2021). Uric Acid as a Predictor for Early Allograft Dysfunction after Living Donor Liver Transplantation: A Prospective Observational Study. Journal of Clinical Medicine, 10(12), 2729. https://doi.org/10.3390/jcm10122729