
Nutrition Assessment and Adverse Outcomes in Hospitalized Patients with Tuberculosis

 , and
, and
Abstract
1. Introduction
2. Methods
2.1. Study Design and Patients
2.2. Demography, Comorbidity, and Constitutional Symptoms
2.3. Diagnosis
2.4. Treatment, Adverse Drug Reactions, and Outcomes
2.5. Patient-Generated Subjective Global Assessment
2.6. Statistical Analysis
3. Results
3.1. Demography, Comorbidities, and Clinical Conditions
3.2. Well-Nourished and Malnourished Patients Compared
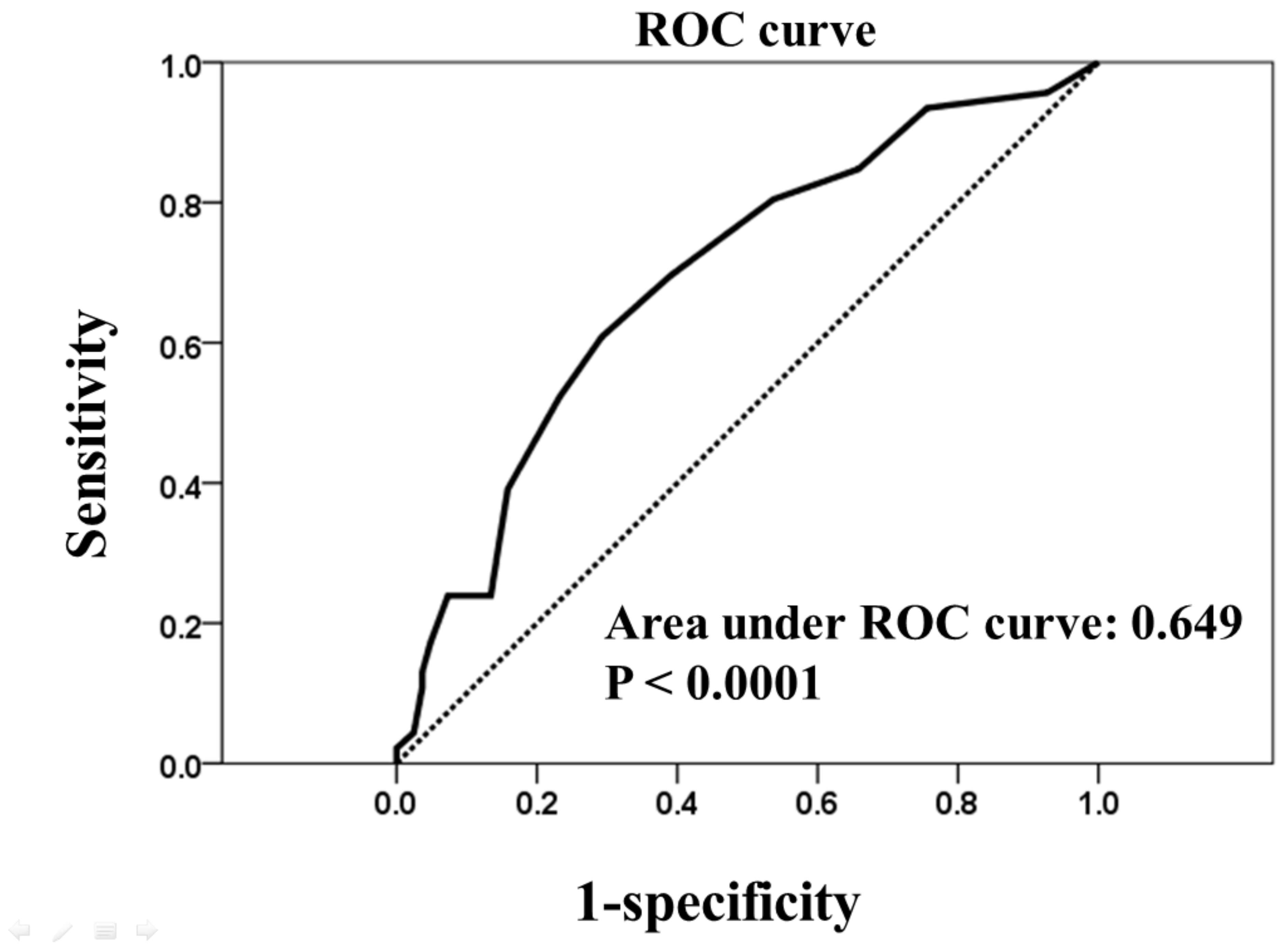
3.3. Factors Associated with Fatal Outcomes
4. Discussion
4.1. Nutrition, Diabetes, and Tuberculosis
4.2. Limitations of BMI Assessment for Elderly Patients
4.3. PG-SGA Scores, Hepatitis, and TB
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2020; World Health Organization: Geneva, Switzerland, 2020; p. 1. [Google Scholar]
- Gupta, K.B.; Gupta, R.; Atreja, A.; Verma, M.; Vishvkarma, S. Tuberculosis and nutrition. Lung India 2009, 26, 9–16. [Google Scholar] [CrossRef]
- Lönnroth, K.; Williams, B.G.; Cegielski, P.; Dye, C. A consistent log-linear relationship between tuberculosis incidence and body mass index. Int. J. Epidemiol. 2009, 39, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.J.; Sabina, E.P. Malnutrition and Associated Disorders in Tuberculosis and Its Therapy. J. Diet. Suppl. 2019, 16, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Podewils, L.J.; Holtz, T.; Riekstina, V.; Skripconoka, V.; Zarovska, E.; Kirvelaite, G.; Kreigere, E.; Leimane, V. Impact of malnutrition on clinical presentation, clinical course, and mortality in MDR-TB patients. Epidemiol. Infect. 2010, 139, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, A.; Chatterjee, M.; Jain, Y.; Chatterjee, B.; Kataria, A.; Bhargava, M.; Kataria, R.; D’Souza, R.; Jain, R.; Benedetti, A.; et al. Nutritional status of adult patients with pulmonary tuberculosis in rural central India and its association with mortality. PLoS ONE 2013, 8, e77979. [Google Scholar] [CrossRef] [PubMed]
- Miyata, S.; Tanaka, M.; Ihaku, D. Subjective Global Assessment in Patients with Pulmonary Tuberculosis. Nutr. Clin. Pract. 2011, 26, 55–60. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Nutritional Care and Support for Patients with Tuberculosis; World Health Organization: Geneva, Switzerland, 2013; p. 3. [Google Scholar]
- Detsky, A.S.; Baker, J.P.; Johnston, N.; Whittaker, S.; Mendelson, R.A.; Jeejeebhoy, K.N. What is subjective global assessment of nutritional status? Parenter Enter. Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef]
- Laky, B.; Janda, M.; Cleghorn, G.; Obermair, A. Comparison of different nutritional assessments and body-composition measurements in detecting malnutrition among gynecologic cancer patients. Am. J. Clin. Nutr. 2008, 87, 1678–1685. [Google Scholar] [CrossRef] [PubMed]
- Castillo-Martinez, L.; Castro-Eguiluz, A.D.; Copca-Mendoza, E.T.; Pérez-Camargo, D.A.; Reyes-Torres, C.A.; Damasco, E.; López-Córdova, G.; Fuentes-Hernández, M.R.; Cetina-Pérez, L.; Milke-García, M.D.P. Nutritional Assessment Tools for the Identification of Malnutrition and Nutritional Risk Associated with Cancer Treatment. Rev. Investig. Clin. 2018, 70, 121–125. [Google Scholar] [CrossRef]
- Thomas, J.M.; Isenring, E.; Kellett, E. Nutritional status and length of stay in patients admitted to an Acute Assessment Unit. J. Hum. Nutr. Diet. 2007, 20, 320–328. [Google Scholar] [CrossRef] [PubMed]
- ter Beek, L.; van der Vaart, H.; Wempe, J.B.; Krijnen, W.P.; Roodenburg, J.L.; van der Schans, C.P.; Jager-Wittenaar, H. Coexistence of Malnutri tion, Frailty, Physical Frailty and Disability in Patients With COPD Starting a Pulmonary Rehabilitation Program. Clin. Nutr. 2020, 39, 2557–2563. [Google Scholar] [CrossRef] [PubMed]
- Ottery, F. Patient-generated subjective global assessment. In The Clinical Guide to Oncology Nutrition; McCallum, P., Polisena, C., Eds.; American Dietetic Association: Chicago, IL, USA, 2000; pp. 11–23. [Google Scholar]
- Tellez-Navarrete, N.A.; Ramon-Luing, L.A.; Muñoz-Torrico, M.; Osuna-Padilla, I.A.; Chavez-Galan, L. Malnutrition and tuberculosis: The gap between basic research and clinical trials. J. Infect Dev. Ctries 2021, 15, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Lönnroth, K.; Roglic, G.; Harries, A.D. Improving tuberculosis prevention and care through addressing the global diabetes epidemic: From evidence to policy and practice. Lancet Diabetes Endocrinol. 2014, 2, 730–739. [Google Scholar] [CrossRef]
- Riza, A.L.; Pearson, F.; Ugarte-Gil, C.; Alisjahbana, B.; van de Vijver, S.; Panduru, N.M.; Hill, P.C.; Ruslami, R.; Moore, D.; Aarnoutse, R.; et al. Clinical management of concurrent diabetes and tuberculosis and the implications for patient services. Lancet Diabetes Endocrinol. 2014, 2, 740–753. [Google Scholar] [CrossRef]
- Huang, T.H.; Chi, C.C.; Liu, C.H.; Chang, C.C.; Kuo, L.M.; Hsieh, C.C. Nutritional status assessed by scored patient-generated subjective global assessment associated with length of hospital stay in adult patients receiving an appendectomy. Biomed. J. 2014, 37, 71–77. [Google Scholar]
- Zachariah, R.; Spielmann, M.; Harries, A.; Salaniponi, F. Moderate to severe malnutrition in patients with tuberculosis is a risk factor associated with early death. Trans. R. Soc. Trop. Med. Hyg. 2002, 96, 291–294. [Google Scholar] [CrossRef]
- Hirani, V.; Mindell, J. A comparison of measured height and demi-span equivalent height in the assessment of body mass index among people aged 65 years and over in England. Age Ageing 2008, 37, 311–317. [Google Scholar] [CrossRef]
- Gavriilidou, N.N.; Pihlsgård, M.; Elmståhl, S. High degree of BMI misclassification of malnutrition among Swedish elderly population: Age-adjusted height estimation using knee height and demispan. Eur. J. Clin. Nutr. 2015, 69, 565–571. [Google Scholar] [CrossRef]
- Hassen Ali, A.; Belachew, T.; Yami, A.; Ayen, W.Y. Anti-tuberculosis drug induced hepatotoxicity among TB/HIV co-infected patients at Jimma University Hospital, Ethiopia: Nested case-control study. PLoS ONE 2013, 8, e64622. [Google Scholar] [CrossRef]
- Tostmann, A.; Boeree, M.J.; Aarnoutse, R.E.; de Lange, W.C.; van der Ven, A.J.; Dekhuijzen, R. Antituberculosis drug-induced hepatotoxicity: Concise up-to-date review. J. Gastroenterol. Hepatol. 2008, 23, 192–202. [Google Scholar] [CrossRef]
- Singla, R.; Sharma, S.K.; Mohan, A.; Makharia, G.; Sreenivas, V.; Jha, B.; Kumar, S.; Sarda, P.; Singh, S. Evaluation of risk factors for antituberculosis treatment induced hepatotoxicity. Indian J. Med. Res. 2010, 132, 81–86. [Google Scholar]
- Saukkonen, J.J.; Cohn, D.L.; Jasmer, R.M.; Schenker, S.; Jereb, J.A.; Nolan, C.M.; Peloquin, C.A.; Gordin, F.M.; Nunes, D.; Strader, D.B.; et al. An Official ATS Statement: Hepatotoxicity of Antituberculosis Therapy. Am. J. Respir. Crit. Care Med. 2006, 174, 935–952. [Google Scholar] [CrossRef]
- Singh, J.; Arora, A.; Garg, P.K.; Thakur, V.S.; Pande, J.N.; Tandon, R.K. Antituberculosis treatment-induced hepatotoxicity: Role of predictive factors. Postgrad. Med. J. 1995, 71, 359–362. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All a | Well-Nourished a | Malnourished a | ||
|---|---|---|---|---|
| Characteristics | n = 128 | n = 65 | n = 63 | p |
| Female a, n (%) | 34 (26.6) | 18 (27.7) | 16 (25.4) | 0769 |
| Elderly b, n (%) | 92 (71.9) | 46 (70.8) | 46 (73.0) | 0.777 |
| Weight (kg) c | 55.3 ± 11.7 | 58.4 ± 11.2 | 52.1 ± 11.4 | 0.002 |
| Body mass index (kg/m2) c,d | 21.4 ± 4.2 | 22.5 ± 3.8 | 20.3 ± 4.3 | 0.002 |
| Body mass index (kg/m2) <18.5 d | 35 (27.7) | 11 (16.9) | 24 (38.4) | 0.007 |
| PG-SGA score c | 5.2 ± 3.7 | 2.6 ± 1.8 | 7.8 ± 3.2 | <0.001 |
| Hemoglobin (mg/dL) c | 11.6 ± 2.6 | 11.9 ± 2.7 | 11.4 ± 2.4 | 0.325 |
| Comorbidity, n (%) | ||||
| Diabetes mellitus | 30 (23.4) | 10 (15.4) | 20 (31.7) | 0.029 |
| Heart disease | 2 (1.6) | 0 (0.0) | 2 (3.2) | 0.240 |
| COPD | 13 (10.2) | 8 (12.3) | 5 (7.9) | 0.413 |
| CKD stage 5 | 6 (4.7) | 3 (4.6) | 3 (4.8) | 1.000 |
| DLC | 3 (2.3) | 2 (3.1) | 1 (1.6) | 1.000 |
| Solid tumor cancer | 23 (18.0) | 10 (15.4) | 13 (20.6) | 0.439 |
| Hematological malignancies | 5 (3.9) | 1 (1.5) | 4 (6.3) | 0.204 |
| Constitutional symptom, n (%) | ||||
| Fever | 34 (26.6) | 14 (21.5) | 20 (31.7) | 0.191 |
| Body weight loss | 10 (7.8) | 5 (9.2) | 5 (9.5) | 1.000 |
| Infectious source, n (%) | ||||
| Pulmonary | 117 (91.4) | 58 (89.2) | 59 (93.7) | 0.372 |
| Extrapulmonary | 19 (14.8) | 11 (16.9) | 8 (12.7) | 0.502 |
| Dissemination | 8 (6.3) | 4 (6.2) | 4 (6.3) | 1.000 |
| Smear positive | 55 (43.0) | 25 (38.5) | 30 (47.6) | 0.295 |
| Liver injury during therapy, n (%) | 26 (20.3) | 8 (12.3) | 18 (28.6) | 0.022 |
| Fatal outcome, n (%) | 26 (20.3) | 5 (7.7) | 21 (33.3) | <0.001 |
| Liver Injury a | Non-Liver Injury a | ||
|---|---|---|---|
| Variables | n = 26 | n = 102 | p |
| Female, n (%) | 5 (19.2) | 29 (28.4) | 0.343 |
| Elderly b, n (%) | 19 (73.1) | 73 (71.6) | 0.879 |
| Body mass index (kg/m2) c,d | 20.7 ± 3.0 | 21.6 ± 4.4 | 0.204 |
| Body mass index (kg/m2) < 18.5 d | 8 (30.8) | 27 (27.0) | 0.717 |
| PG-SGA score c | 7.3 ± 3.6 | 4.7 ± 3.5 | 0.002 |
| Hgb c | 12.3 ± 2.6 | 11.5 ± 2.6 | 0.166 |
| Comorbidity, n (%) | |||
| Diabetes mellitus | 5 (19.2) | 25 (24.5) | 0.571 |
| Heart disease | 2 (7.7) | 0 (0.0) | 0.004 |
| COPD | 4 (15.4) | 9 (8.8) | 0.299 |
| CKD stage 5 | 1 (3.8) | 5 (4.9) | 1.000 |
| DLC | 1 (3.8) | 2 (2.0) | 0.497 |
| Solid tumor cancer | 2 (7.7) | 21 (20.6) | 0.160 |
| Hematological malignancies | 0 (0) | 5 (4.9) | 0.582 |
| Constitutional symptom, n (%) | |||
| Fever | 7 (26.9) | 27 (26.7) | 0.963 |
| Body weight loss | 1 (3.8) | 9 (8.8) | 0.686 |
| Infectious source, n (%) | |||
| Pulmonary | 24 (92.3) | 93 (91.2) | 1.000 |
| Extrapulmonary | 3 (11.5) | 16 (15.7) | 0.762 |
| Dissemination | 1 (3.8) | 7 (6.9) | 1.000 |
| Smear positive, n (%) | 10 (38.5) | 45 (44.1) | 0.603 |
| Multivariate | |||||
|---|---|---|---|---|---|
| Fatal a | Favorable a | Univariate | Odds Ratio | ||
| Variables | n = 26 | n = 102 | p | 95% CI | p |
| Female a, n (%) | 5 (19.2) | 29 (28.4) | 0.343 | ||
| Elderly b, n (%) | 21 (80.8) | 71 (69.6) | 0.258 | ||
| BMI (kg/m2) c,d | 20.9 ± 4.4 | 21.6 ± 4.1 | 0.467 | ||
| BMI (kg/m2) < 18.5 d | 9 (34.6) | 26 (26.0) | 0.525 | ||
| PG-SGA score c | 6.7 ± 4.0 | 4.8 ± 3.5 | 0.028 | 1.142 (1.012–1.288) | 0.031 |
| Hgb c | 11.5 ± 2.5 | 11.7 ± 2.6 | 0.745 | ||
| Comorbidity, n (%) | |||||
| Diabetes mellitus | 10 (38.5) | 20 (19.6) | 0.043 | 1.993 (0.757–5.248) | 0.163 |
| Heart disease | 0 (0.0) | 2 (2.0) | 1.000 | ||
| COPD | 2 (7.8) | 11 (10.8) | 1.000 | ||
| CKD stage 5 | 2 (7.8) | 4 (3.9) | 0.601 | ||
| DLC | 1 (3.8) | 2 (2.0) | 0.497 | ||
| Solid tumor cancer | 8 (30.8) | 15 (14.7) | 0.083 | 2.251 (0.785–6.456) | 0.131 |
| Hematological malignancies | 2 (7.8) | 3 (2.9) | 0.268 | ||
| Constitutional symptom, n (%) | |||||
| Fever | 10 (38.5) | 24 (23.5) | 0.124 | ||
| Body weight loss | 2 (7.8) | 8 (7.8) | 1.000 | ||
| Infectious source, n (%) | |||||
| Pulmonary | 25 (96.2) | 92 (90.2) | 0.460 | ||
| Extrapulmonary | 2 (7.8) | 17 (16.7) | 0.360 | ||
| Dissemination | 1 (3.8) | 7 (6.9) | 1.000 | ||
| Smear positive, n (%) | 15 (57.7) | 40 (39.2) | 0.089 | 1.677 (0.664–4.238) | 0.274 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, H.-S.; Lin, M.-S.; Chi, C.-C.; Ye, J.-J.; Hsieh, C.-C. Nutrition Assessment and Adverse Outcomes in Hospitalized Patients with Tuberculosis. J. Clin. Med. 2021, 10, 2702. https://doi.org/10.3390/jcm10122702
Lin H-S, Lin M-S, Chi C-C, Ye J-J, Hsieh C-C. Nutrition Assessment and Adverse Outcomes in Hospitalized Patients with Tuberculosis. Journal of Clinical Medicine. 2021; 10(12):2702. https://doi.org/10.3390/jcm10122702
Chicago/Turabian StyleLin, Huang-Shen, Ming-Shyan Lin, Ching-Chi Chi, Jung-Jr Ye, and Ching-Chuan Hsieh. 2021. "Nutrition Assessment and Adverse Outcomes in Hospitalized Patients with Tuberculosis" Journal of Clinical Medicine 10, no. 12: 2702. https://doi.org/10.3390/jcm10122702
APA StyleLin, H.-S., Lin, M.-S., Chi, C.-C., Ye, J.-J., & Hsieh, C.-C. (2021). Nutrition Assessment and Adverse Outcomes in Hospitalized Patients with Tuberculosis. Journal of Clinical Medicine, 10(12), 2702. https://doi.org/10.3390/jcm10122702