
New Early Warning Score: EMS Off-Label Use in Out-of-Hospital Patients

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Materials and Training
2.4. Endpoint
2.5. Data Collection
2.6. Statistical Analysis
2.7. Ethics Statement
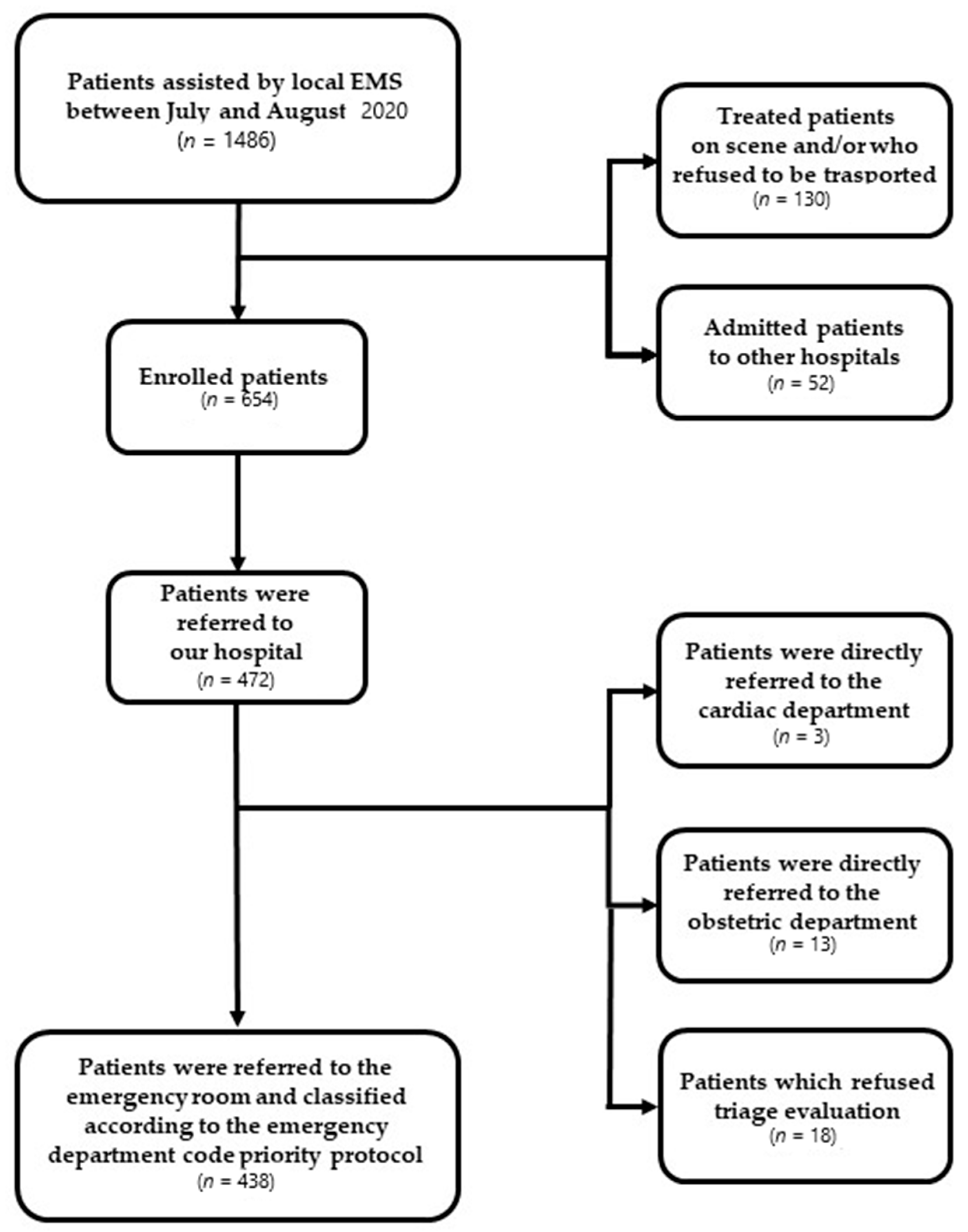
3. Results
3.1. Descriptive Statistics
3.2. On-Site NEWS Evaluation and Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

Appendix C

References
- Smith, G.B.; Prytherch, D.R.; Schmidt, P.E.; Featherstone, P.I. Review and performance evaluation of aggregate weighted ‘track and trigger’ systems. Resuscitation 2008, 77, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Yeung, J.; Scapigliati, A.; Hsieh, M.; Boulton, A.; Saviani, M.; Georgiou, M.; Schnaubelt, S.; Bray, J.; Bhanji, F.; Bigham, B.; et al. Rapid Response Systems in Adults Consensus on Science with Treatment Recommendations [Internet] Brussels, Belgium: International Liaison Committee on Resuscitation (ILCOR) Education, Implementation and Teams Task Force. Available online: https://costr.ilcor.org/document/rapid-response-systems-in-adults-systematic-review (accessed on 11 June 2021).
- Smith, G.B.; Prytherch, D.R.; Meredith, P.; Schmidt, P.E.; Featherstone, P.I. The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of early cardiac arrest, unanticipated intensive care unit admission, and death. Resuscitation 2013, 84, 465–470. [Google Scholar] [CrossRef] [PubMed]
- New National Early Warning Score Could Save 6000 Lives. Available online: https://www.rcplondon.ac.uk/news/new-national-early-warning-score-could-save-6000-lives (accessed on 11 June 2021).
- Semeraro, F.; Scquizzato, T.; Scapigliati, A.; Ristagno, G.; Gamberini, L.; Tartaglione, M.; Dell’Arciprete, O.; Mora, F.; Cordenons, F.; Del Giudice, D.; et al. New Early Warning Score: Off-label approach for Covid-19 outbreak patient deterioration in the community. Resuscitation 2020, 151, 24–25. [Google Scholar] [CrossRef] [PubMed]
- Schisterman, E.F.; Perkins, N.J.; Liu, A.; Bondell, H. Optimal Cut-point and Its Corresponding Youden Index to Discriminate Individuals Using Pooled Blood Samples. Epidemiology 2005, 16, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Uppanisakorn, S.; Bhurayanontachai, R.; Boonyarat, J.; Kaewpradit, J. National Early Warning Score (NEWS) at ICU discharge can predict early clinical deterioration after ICU transfer. J. Crit. Care 2018, 43, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Choi, J.W.; Park, Y.H.; Chung, C.; Park, D.I.; Lee, J.E.; Lee, H.S.; Moon, J.Y. Evaluation of the efficacy of the National Early Warning Score in predicting in-hospital mortality via the risk stratification. J. Crit. Care 2018, 47, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Silcock, D.J.; Corfield, A.R.; Gowens, P.A.; Rooney, K.D. Validation of the National Early Warning Score in the prehospital setting. Resuscitation 2015, 89, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Pirneskoski, J.; Kuisma, M.; Olkkola, K.T.; Nurmi, J. Prehospital National Early Warning Score predicts early mortality. Acta Anaesthesiol. Scand. 2019, 63, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Hoikka, M.; Silfvast, T.; Ala-Kokko, T.I. Does the prehospital National Early Warning Score predict the short-term mortality of unselected emergency patients? Scand. J. Trauma. Resusc. Emerg. Med. 2018, 26, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Silcock, D.J.; Corfield, A.R.; Staines, H.; Rooney, K.D. Superior performance of National Early Warning Score compared with quick Sepsis-related Organ Failure Assessment Score in predicting adverse outcomes: A retrospective observational study of patients in the prehospital setting. Eur. J. Emerg. Med. 2019, 26, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.; Fothergill, R.; Clark, S.; Moore, F. Can the prehospital National Early Warning Score identify patients most at risk from subsequent deterioration? Emerg. Med. J. 2017, 34, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Pullyblank, A.; Tavaré, A.; Little, H.; Redfern, E.; Le Roux, H.; Inada-Kim, M.; Cheema, K.; Cook, A. Implementation of the National Early Warning Score in patients with suspicion of sepsis: Evaluation of a system-wide quality improvement project. Br. J. Gen. Pr. 2020, 70, e381–e388. [Google Scholar] [CrossRef] [PubMed]
- Williams, T.A.; Tohira, H.; Finn, J.; Perkins, G.D.; Ho, K.M. The ability of early warning scores (EWS) to detect critical illness in the prehospital setting: A systematic review. Resuscitation 2016, 102, 35–43. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EMS Dispatch Priority Codes | Patients (%) | Emergency Department Triage Code | Patients (%) |
|---|---|---|---|
| White | 8 (1.2%) | White | 17 (3.9%) |
| Green | 237 (36.2%) | Green | 229 (52.3%) |
| Yellow | 295 (45.1%) | Yellow | 160 (36.5%) |
| Red | 114 (17.4%) | Red | 32 (7.3%) |
| Total | 654 | Total | 438 |
| Place of calls | Patients (%) | Emergency Department Outcome | Patients (%) |
| Residence | 477 (72.9%) | Discharged at home | 223 (50.9%) |
| Work/Office | 18 (2.8%) | Admitted to the hospital | 168 (38.4%) |
| Public building | 15 (2.3%) | Refused hospital admission | 43 (9.8%) |
| Street | 101 (15.4%) | Deceased in ED | 4 (0.9%) |
| Sport facilities | 2 (0.3%) | Total | 438 |
| Other | 41 (6.3%) | ||
| Total | 654 | ||
| Suspected pathology code | Patients (%) | Return code | Patients (%) |
| Traumatic | 165 (25.2%) | 0 | 130 (19.9%) |
| Cardiovascular | 105 (16.1%) | 1 | 459 (70.2%) |
| Respiratory | 58 (8.9%) | 2 | 63 (9.6%) |
| Neurologic | 51 (7.8%) | 3 | 2 (0.3%) |
| Psychiatric | 27 (4.1%) | ||
| Neoplastic | 7 (1.1%) | ||
| Intoxication | 17 (2.6%) | ||
| Metabolic | 6 (0.9%) | ||
| Gastroenteric | 48 (7.3%) | ||
| Urologic | 10 (3.7%) | ||
| Ophthalmic | 1 (0.2%) | ||
| ENT | 4 (0.6%) | ||
| Obstetric | 16 (2.4%) | ||
| Infectious | 7 (1.1%) | ||
| Other pathologies | 115 (17.6%) | ||
| Not identified | 3 (0.5%) | ||
| Total | 654 | ||
| Female | Male | p | <68 Years Old | ≥68 Years Old | p | |
|---|---|---|---|---|---|---|
| Respiratory rate | 0.29 ± 0.79 | 0.24 ± 0.72 | 0.413 | 0.26 ± 0.74 | 0.27 ± 0.77 | 0.775 |
| Oxygen saturation | 0.43 ± 0.86 | 0.34 ± 0.76 | 0.161 | 0.20 ± 0.61 | 0.57 ± 0.94 | 0.000 |
| Temperature | 0.23 ± 0.55 | 0.26 ± 0.56 | 0.501 | 0.23 ± 0.53 | 0.26 ± 0.58 | 0.551 |
| Systolic Pressure | 0.39 ± 0.74 | 0.52 ± 0.80 | 0.038 | 0.44 ± 0.71 | 0.48 ± 0.84 | 0.483 |
| Heart rate | 0.54 ± 0.75 | 0.53 ± 0.78 | 0.803 | 0.62 ± 0.79 | 0.45 ± 0.73 | 0.006 |
| Consciousness | 0.20 ± 0.75 | 0.20 ± 0.76 | 0.969 | 0.10 ± 0.54 | 0.30 ± 0.91 | 0.001 |
| Total score | 2.19 ± 2.51 | 2.21 ± 2.58 | 0.936 | 1.89 ± 2.05 | 2.51 ± 2.93 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Semeraro, F.; Corona, G.; Scquizzato, T.; Gamberini, L.; Valentini, A.; Tartaglione, M.; Scapigliati, A.; Ristagno, G.; Martella, C.; Descovich, C.; et al. New Early Warning Score: EMS Off-Label Use in Out-of-Hospital Patients. J. Clin. Med. 2021, 10, 2617. https://doi.org/10.3390/jcm10122617
Semeraro F, Corona G, Scquizzato T, Gamberini L, Valentini A, Tartaglione M, Scapigliati A, Ristagno G, Martella C, Descovich C, et al. New Early Warning Score: EMS Off-Label Use in Out-of-Hospital Patients. Journal of Clinical Medicine. 2021; 10(12):2617. https://doi.org/10.3390/jcm10122617
Chicago/Turabian StyleSemeraro, Federico, Giovanni Corona, Tommaso Scquizzato, Lorenzo Gamberini, Anna Valentini, Marco Tartaglione, Andrea Scapigliati, Giuseppe Ristagno, Carmela Martella, Carlo Descovich, and et al. 2021. "New Early Warning Score: EMS Off-Label Use in Out-of-Hospital Patients" Journal of Clinical Medicine 10, no. 12: 2617. https://doi.org/10.3390/jcm10122617
APA StyleSemeraro, F., Corona, G., Scquizzato, T., Gamberini, L., Valentini, A., Tartaglione, M., Scapigliati, A., Ristagno, G., Martella, C., Descovich, C., Picoco, C., & Gordini, G. (2021). New Early Warning Score: EMS Off-Label Use in Out-of-Hospital Patients. Journal of Clinical Medicine, 10(12), 2617. https://doi.org/10.3390/jcm10122617