
Prosthesis Position after TAVI with Balloon-Expandable SAPIEN 3 in Bicuspid Aortic Valves

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
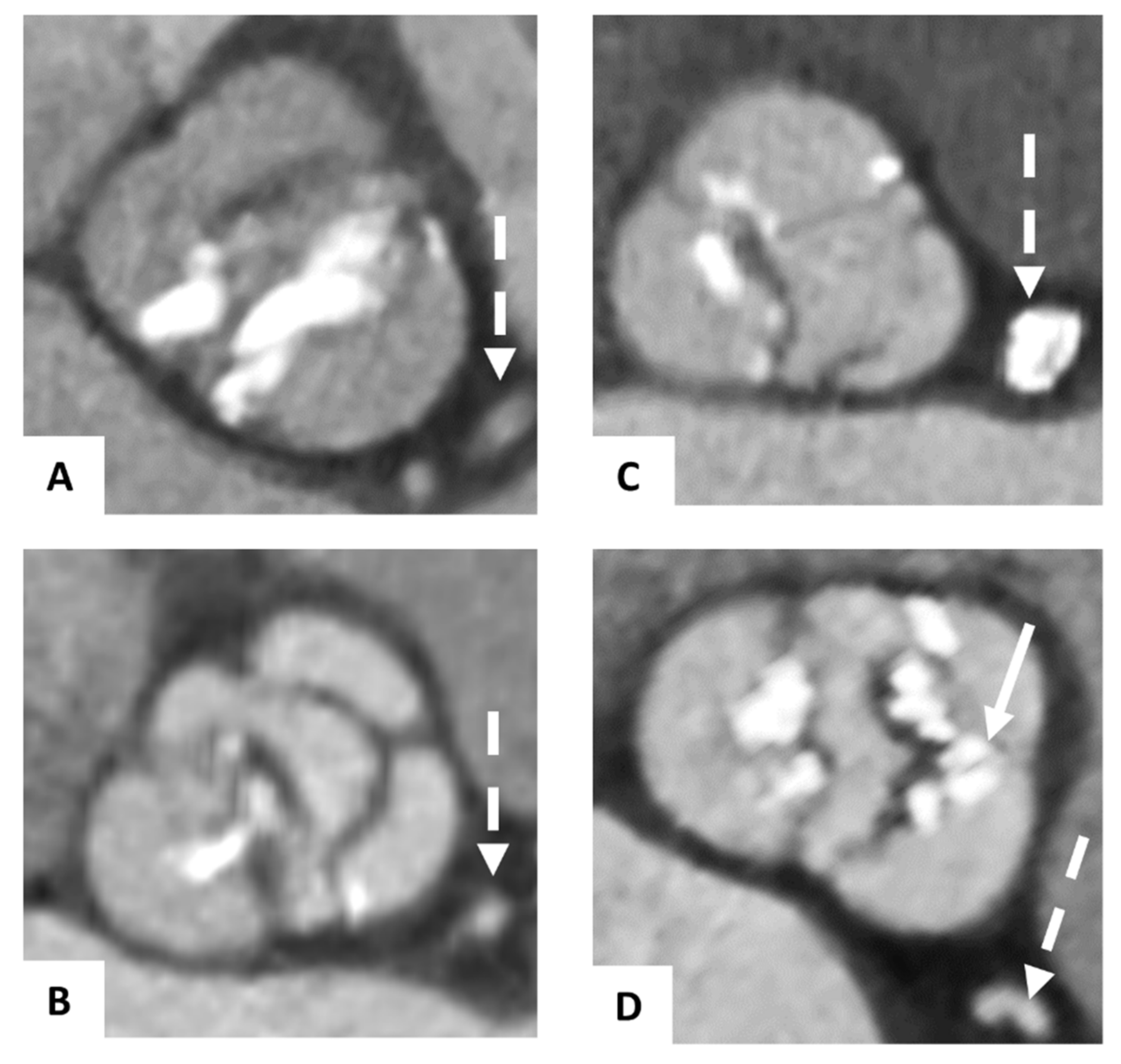
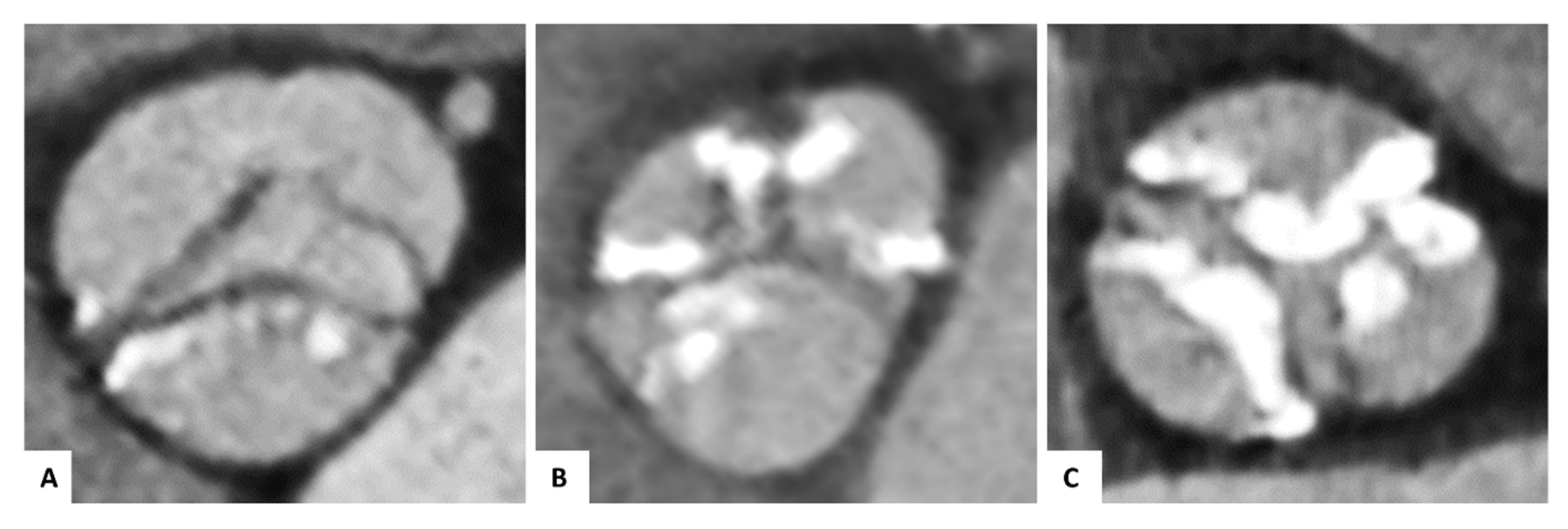
2.2. Morphology of the Bicuspid Aortic Valves
2.3. Image Acquisition
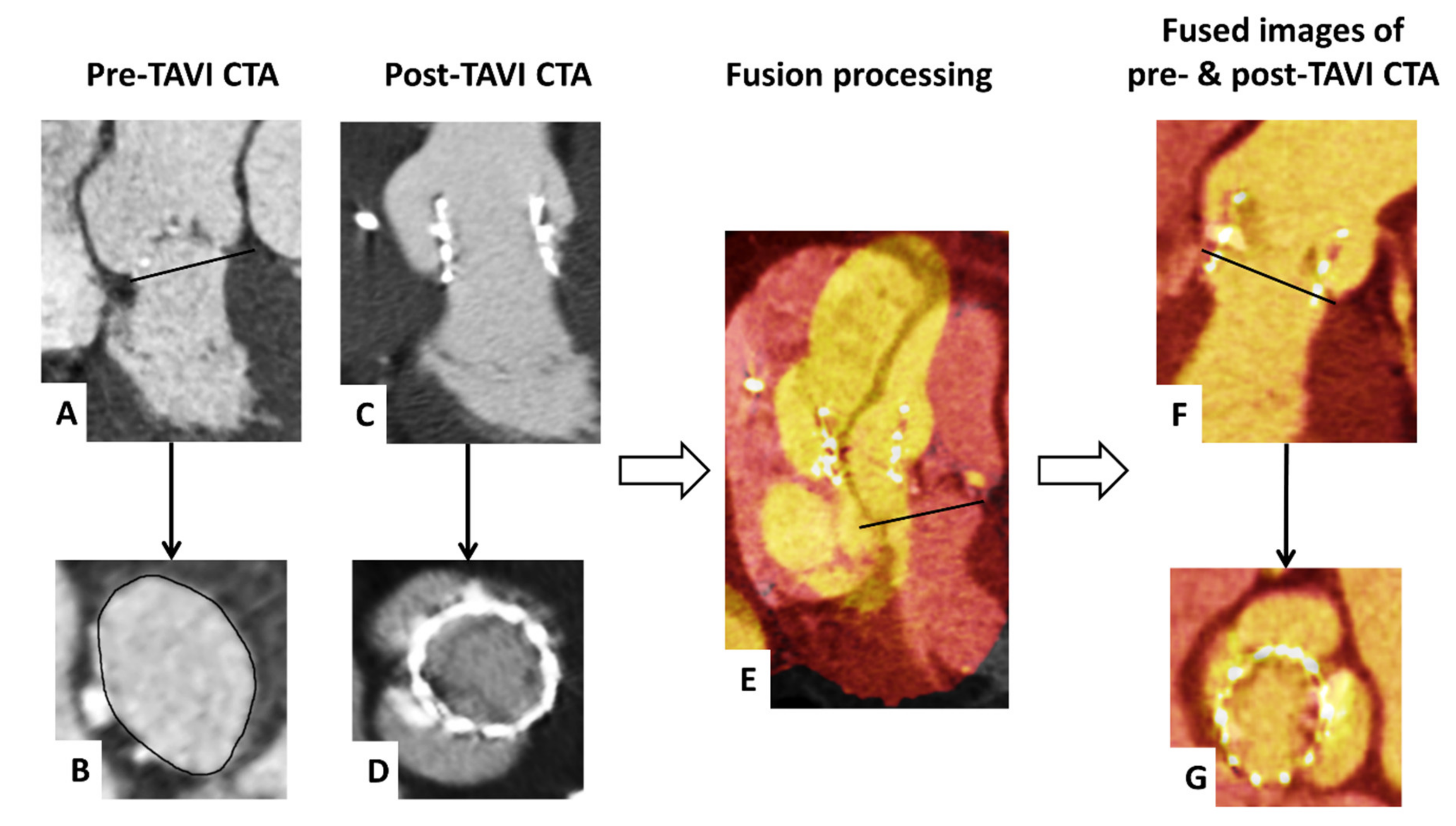
2.4. Process of Fusion Imaging
2.5. Image Analysis
2.6. Statistical Analysis
3. Results
3.1. Procedural- and Prosthesis—Related Characteristics
3.2. Subanalysis of the Bicuspid Aortic Valves
4. Discussion
4.1. Implantation Depth and Conduction Disturbances
4.2. Expansion and Prosthesis Waist
5. Limitations
6. Conclusions and Impact on Daily Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BAV | Bicuspid aortic valve |
| CTA | Computed tomography angiography |
| PVL | Paravalvular THV leakage |
| TAV | Tricuspid aortic valve |
| TAVI | Transcatheter aortic valve implantation |
| THV | Transcatheter heart valve |
References
- Ward, C. Clinical significance of the bicuspid aortic valve. Heart 2000, 83, 81–85. [Google Scholar] [CrossRef]
- Roberts, W.C.; Janning, K.G.; Ko, J.M.; Filardo, G.; Matter, G.J. Frequency of Congenitally Bicuspid Aortic Valves in Patients ≥80 Years of Age Undergoing Aortic Valve Replacement for Aortic Stenosis (with or without Aortic Regurgitation) and Implications for Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2012, 109, 1632–1636. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.; et al. Transcatheter Aortic-Valve Implantation for Aortic Stenosis in Patients who Cannot Undergo Surgery. N. Engl. J. Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.; Makkar, R.; Svensson, L.G.; Kodali, S.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef] [PubMed]
- Mylotte, D.; Lefevre, T.; Søndergaard, L.; Watanabe, Y.; Modine, T.; Dvir, D.; Bosmans, J.; Tchetche, D.; Kornowski, R.; Sinning, J.-M.; et al. Transcatheter Aortic Valve Replacement in Bicuspid Aortic Valve Disease. J. Am. Coll. Cardiol. 2014, 64, 2330–2339. [Google Scholar] [CrossRef]
- Attinger-Toller, A.; Bhindi, R.; Perlman, G.Y.; Murdoch, D.; Weir-McCall, J.; Blanke, P.; Barbanti, M.; Sathananthan, J.; Ruile, P.; Gandolfo, C.; et al. Mid-term outcome in patients with bicuspid aortic valve stenosis following transcatheter aortic valve replacement with a current generation device: A multicenter study. Catheter. Cardiovasc. Interv. 2019, 95, 1186–1192. [Google Scholar] [CrossRef] [PubMed]
- Perlman, G.Y.; Blanke, P.; Dvir, D.; Pache, G.; Modine, T.; Barbanti, M.; Holy, E.W.; Treede, H.; Ruile, P.; Neumann, F.-J.; et al. Bicuspid Aortic Valve Stenosis: Favorable Early Outcomes with a Next-Generation Transcatheter Heart Valve in a Multicenter Study. JACC Cardiovasc. Interv. 2016, 9, 817–824. [Google Scholar] [CrossRef]
- Yoon, S.-H.; Maeno, Y.; Kawamori, H.; Miyasaka, M.; Nomura, T.; Ochiai, T.; Nemanpour, S.; Raschpichler, M.; Sharma, R.; Chakravarty, T.; et al. Diagnosis and Outcomes of Transcatheter Aortic Valve Implantation in Bicuspid Aortic Valve Stenosis. Interv. Cardiol. Rev. 2018, 13, 62–65. [Google Scholar] [CrossRef]
- Kawamori, H.; Yoon, S.-H.; Chakravarty, T.; Maeno, Y.; Kashif, M.; Israr, S.; Abramowitz, Y.; Mangat, G.; Miyasaka, M.; Rami, T.; et al. Computed tomography characteristics of the aortic valve and the geometry of SAPIEN 3 transcatheter heart valve in patients with bicuspid aortic valve disease. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1408–1418. [Google Scholar] [CrossRef]
- Halim, S.A.; Edwards, F.H.; Dai, D.; Li, Z.; Mack, M.J.; Holmes, D.R.; Tuzcu, E.M.; Thourani, V.H.; Harrison, J.K.; Brennan, J.M. Outcomes of Transcatheter Aortic Valve Replacement in Patients with Bicuspid Aortic Valve Disease: A Report from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry. Circulation 2020, 141, 1071–1079. [Google Scholar] [CrossRef]
- Yoon, S.-H.; Ahn, J.-M.; Hayashida, K.; Watanabe, Y.; Shirai, S.; Kao, H.-L.; Yin, W.-H.; Lee, M.K.-Y.; Tay, E.; Araki, M.; et al. Clinical Outcomes Following Transcatheter Aortic Valve Replacement in Asian Population. JACC Cardiovasc. Interv. 2016, 9, 926–933. [Google Scholar] [CrossRef]
- Mack, M.J.; Brennan, J.M.; Brindis, R.; Carroll, J.; Edwards, F.; Grover, F.; Shahian, D.; Tuzcu, E.M.; Peterson, E.D.; Rumsfeld, J.S.; et al. Outcomes Following Transcatheter Aortic Valve Replacement in the United States. JAMA 2013, 310, 2069–2077. [Google Scholar] [CrossRef] [PubMed]
- Sherif, M.A.; Abdel-Wahab, M.; Stöcker, B.; Geist, V.; Richardt, D.; Tölg, R.; Richardt, G. Anatomic and Procedural Predictors of Paravalvular Aortic Regurgitation After Implantation of the Medtronic CoreValve Bioprosthesis. J. Am. Coll. Cardiol. 2010, 56, 1623–1629. [Google Scholar] [CrossRef] [PubMed]
- Almeida, J.G.; Ferreira, S.M.; Fonseca, P.; Dias, T.; Guerreiro, C.; Barbosa, A.R.; Teixeira, P.; Carvalho, M.; Ferreira, W.; Ferreira, N.D.; et al. Association between implantation depth assessed by computed tomography and new-onset conduction disturbances after transcatheter aortic valve implantation. J. Cardiovasc. Comput. Tomogr. 2017, 11, 332–337. [Google Scholar] [CrossRef]
- Ruile, P.; Pache, G.; Minners, J.; Hein, M.; Neumann, F.-J.; Breitbart, P. Fusion imaging of pre- and post-procedural computed tomography angiography in transcatheter aortic valve implantation patients: Evaluation of prosthesis position and its influence on new conduction disturbances. Eur. Heart J. Cardiovasc. Imaging 2018, 20, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Hiratzka, L.F.; Bakris, G.L.; Beckman, J.A.; Bersin, R.M.; Carr, V.F.; Casey, D.E., Jr.; Eagle, K.A.; Hermann, L.K.; Isselbacher, E.M.; Kazerooni, E.A.; et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients with Thoracic Aortic Disease: Executive Summary. Catheter. Cardiovasc. Interv. 2010, 76, E43–E86. [Google Scholar] [CrossRef] [PubMed]
- Pache, G.; Schoechlin, S.; Blanke, P.; Dorfs, S.; Jander, N.; Arepalli, C.D.; Gick, M.; Buettner, H.-J.; Leipsic, J.; Langer, M.; et al. Early hypo-attenuated leaflet thickening in balloon-expandable transcatheter aortic heart valves. Eur. Heart J. 2015, 37, 2263–2271. [Google Scholar] [CrossRef]
- Sievers, H.-H.; Schmidtke, C. A classification system for the bicuspid aortic valve from 304 surgical specimens. J. Thorac. Cardiovasc. Surg. 2007, 133, 1226–1233. [Google Scholar] [CrossRef] [PubMed]
- Breitbart, P.; Pache, G.; Minners, J.; Hein, M.; Schröfel, H.; Neumann, F.-J.; Ruile, P. Predictors for low TAVI-prosthesis position assessed by fusion imaging of pre- and post-procedural CT angiography. Clin. Res. Cardiol. 2021, 110, 93–101. [Google Scholar] [CrossRef]
- Roberts, W.C.; Ko, J.M. Frequency by Decades of Unicuspid, Bicuspid, and Tricuspid Aortic Valves in Adults Having Isolated Aortic Valve Replacement for Aortic Stenosis, with or without Associated Aortic Regurgitation. Circulation 2005, 111, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.-H.; Bleiziffer, S.; De Backer, O.; Delgado, V.; Arai, T.; Ziegelmueller, J.; Barbanti, M.; Sharma, R.; Perlman, G.Y.; Khalique, O.K.; et al. Outcomes in Transcatheter Aortic Valve Replacement for Bicuspid Versus Tricuspid Aortic Valve Stenosis. J. Am. Coll. Cardiol. 2017, 69, 2579–2589. [Google Scholar] [CrossRef]
- Tchetche, D.; de Biase, C.; van Gils, L.; Parma, R.; Ochala, A.; Lefevre, T.; Hovasse, T.; De Backer, O.; Sondergaard, L.; Bleiziffer, S.; et al. Bicuspid Aortic Valve Anatomy and Relationship with Devices: The BAVARD Mutlicenter Registry. Circ. Cardiovasc. Interv. 2019, 12, e007107. [Google Scholar] [CrossRef]
- Schwerg, M.; Fulde, F.; Dreger, H.; Poller, W.C.; Stangl, K.; Laule, M. Optimized Implantation Height of the Edwards SAPIEN 3 Valve to Minimize Pacemaker Implantation After TAVI. J. Interv. Cardiol. 2016, 29, 370–374. [Google Scholar] [CrossRef]
- Fraccaro, C.; Buja, G.; Tarantini, G.; Gasparetto, V.; Leoni, L.; Razzolini, R.; Corrado, D.; Bonato, R.; Basso, C.; Thiene, G.; et al. Incidence, Predictors, and Outcome of Conduction Disorders After Transcatheter Self-Expandable Aortic Valve Implantation. Am. J. Cardiol. 2011, 107, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Mauri, V.; Reimann, A.; Stern, D.; Scherner, M.; Kuhn, E.; Rudolph, V.; Rosenkranz, S.; Eghbalzadeh, K.; Friedrichs, K.; Wahlers, T.; et al. Predictors of Permanent Pacemaker Implantation after Transcatheter Aortic Valve Replacement with the SAPIEN 3. JACC Cardiovasc. Interv. 2016, 9, 2200–2209. [Google Scholar] [CrossRef] [PubMed]
- Latsios, G.; Gerckens, U.; Buellesfeld, L.; Mueller, R.; John, D.; Yuecel, S.; Syring, J.; Sauren, B.; Grube, E. “Device landing zone” calcification, assessed by MSCT, as a predictive factor for pacemaker implantation after TAVI. Catheter. Cardiovasc. Interv. 2010, 76, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Fedak, P.; Verma, S.; David, T.E.; Leask, R.; Weisel, R.D.; Butany, J. Clinical and Pathophysiological Implications of a Bicuspid Aortic Valve. Circulation 2002, 106, 900–904. [Google Scholar] [CrossRef]
- Breitbart, P.; Pache, G.; Minners, J.; Hein, M.; Schröfel, H.; Neumann, F.-J.; Ruile, P. Influence of prosthesis-related factors on the occurrence of early leaflet thrombosis after transcatheter aortic valve implantation. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 1082–1089. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 100) | Patients with Bicuspid Valve (n = 50) | Matched Control Group (n = 50) | p-Value | ||
|---|---|---|---|---|---|
| Age | (years) | 80.0 ± 5.3 | 78.3 ± 5.7 | 81.8 ± 4.1 | 0.001 |
| Female | 40 (40) | 21 (42) | 19 (38) | 0.683 | |
| BMI | (kg/m2) | 26.8 ± 4.6 | 26.3 ± 4.6 | 27.3 ± 4.6 | 0.061 |
| Logistic Euroscore | (%) | 14.8 ± 11.5 | 15.5 ± 13.3 | 14.2 ± 9.5 | 0.941 |
| STS Score | (%) | 3.8 ± 4.1 | 3.5 ± 2.6 | 4.1 ± 5.2 | 0.443 |
| Previous pacemaker | 9 (9) | 5 (10) | 4 (8) | 0.727 | |
| Atrial fibrillation | 29 (29) | 13 (26) | 16 (32) | 0.509 | |
| Oral anticoagulation | 15 (15) | 15 (30) | 15 (30) | 1.000 | |
| Aortic valve area | (cm2) | 0.78 ± 0.17 | 0.80 ± 0.19 | 0.76 ± 0.16 | 0.383 |
| Annulus diameter | (mm) | 25.4 ± 2.2 | 25.7 ± 2.4 | 25.2 ± 2.0 | 0.705 |
| Annulus eccentricity (CTA) | 1.3 ± 0.1 | 1.3 ± 0.1 | 1.3 ± 0.1 | 0.125 | |
| Grade of calcification of the device-landing zone | total | 4.7 ± 1.2 | 5.0 ± 1.1 | 4.4 ± 1.3 | 0.019 |
| Left coronary cusp | 1.5 ± 0.6 | 1.5 ± 0.7 | 1.4 ± 0.5 | 0.478 | |
| Right coronary cusp | 1.5 ± 0.5 | 1.5 ± 0.5 | 1.5 ± 0.5 | 0.821 | |
| Non-coronary cusp | 1.8 ± 0.6 | 2.0 ± 0.5 | 1.6 ± 0.5 | <0.001 | |
| Ejection fraction pre-interventional | (%) | 48.0 ± 10.8 | 46.4 ± 11.7 | 49.5 ± 9.8 | 0.262 |
| 0.558 | |||||
| Access route | Transfemoral | 97 (97) | 49 (98) | 48 (96) | |
| Transapical | 3 (3) | 1 (2) | 2 (4) | ||
| Prosthesis size | 1.000 | ||||
| 23 mm | 14 (14) | 7 (14) | 7 (14) | ||
| 26 mm | 54 (54) | 27 (54) | 27 (54) | ||
| 29 mm | 32 (32) | 16 (32) | 16 (32) | ||
| Post-dilatation | 12 (12) | 6 (12) | 6 (12) | 1.000 | |
| Underfilling | 12 (12) | 6 (12) | 6 (12) | 1.000 | |
| New CD after TAVI a | 42 (46.2) | 23 (51.1) | 19 (41.3) | 0.348 | |
| New PM after TAVI a | 19 (20.9) | 9 (20.0) | 10 (21.7) | 0.838 | |
| Prosthesis oversizing | (%) | 7.0 ± 10.0 | 5.5 ± 10.3 | 8.5 ± 9.5 | 0.212 |
| THV tilt | (°) | 5.4 ± 3.4 | 5.6 ± 3.6 | 5.2 ± 3.4 | 0.436 |
| Extent of the THV waist | (%) | 6.6 ± 3.9 | 7.4 ± 4.5 | 5.8 ± 3.0 | 0.043 |
| THV expansion | (%) | 93.7 ± 9.0 | 91.9 ± 12.2 | 95.5 ± 2.7 | 0.044 |
| Mean expanded THV area | (mm2) | 466.2 ± 76.9 | 457.6 ± 79.7 | 474.9 ± 73.7 | 0.166 |
| MPG after implantation | (mmHg) | 11.0 ± 3.6 | 11.3 ± 3.9 | 10.7 ± 3.3 | 0.334 |
| Leaflet thrombosis | 16 (16) | 7 (14) | 9 (18) | 0.585 | |
| 0.385 | |||||
| None | 47 (47) | 22 (44) | 25 (50) | ||
| Paravalvular | Trivial | 27 (27) | 12 (24) | 15 (30) | |
| leakage | Mild | 26 (26) | 16 (32) | 10 (20) | |
| Moderate | 0 (0) | 0 (0) | 0 (0) | ||
| Severe | 0 (0) | 0 (0) | 0 (0) | ||
| Mean | 3.5 ± 2.3 | 3.8 ± 2.6 | 3.2 ± 2.0 | 0.171 | |
| Implantation depth below | Left coronary cusp | 2.9 ± 2.6 | 3.2 ± 2.9 | 2.6 ± 2.2 | 0.273 |
| annulus (mm) | Right coronary cusp | 3.8 ± 2.8 | 4.2 ± 2.9 | 3.3 ± 2.6 | 0.040 |
| Non-coronary cusp | 3.8 ± 2.7 | 4.1 ± 3.1 | 3.5 ± 2.3 | 0.607 | |
| 0.240 | |||||
| Prosthesis position | Optimal | 93 (93) | 45 (90) | 48 (96) | |
| Low | 7 (7) | 5 (10) | 2 (4) |
| All Patients with Bicuspid Valves (n = 50) | Sievers 0 (n = 5) | Sievers 1 (n = 34) | Functional (n = 11) | p-Value | ||
|---|---|---|---|---|---|---|
| Annulus diameter | (mm) | 25.7 ± 2.4 | 27.0 ± 2.0 | 25.3 ± 2.2 | 26.2 ± 3.2 | 0.221 |
| Annulus eccentricity (CTA) | 1.3 ± 0.1 | 1.1 ± 0.2 | 1.3 ± 0.1 | 1.3 ± 0.2 | 0.082 | |
| Grade of calcification of the device-landing zone | total | 5.0 ± 1.1 | 5.3 ± 0.6 | 5.0 ± 1.2 | 5.0 ± 1.0 | 0.677 |
| Left coronary cusp | 1.5 ± 0.7 | 1.9 ± 0.8 | 1.5 ± 0.7 | 1.5 ± 0.6 | 0.532 | |
| Right coronary cusp | 1.5 ± 0.5 | 1.8 ± 0.7 | 1.4 ± 0.4 | 1.7 ± 0.5 | 0.089 | |
| Non-coronary cusp | 2.0 ± 0.5 | 1.6 ± 0.6 | 2.1 ± 0.5 | 1.8 ± 0.5 | 0.082 | |
| Prosthesis size | 0.143 | |||||
| 23 mm | 7 (14) | 0 (0) | 5 (14.7) | 2 (18.2) | ||
| 26 mm | 27 (54) | 1 (20) | 21 (61.8) | 5 (45.5) | ||
| 29 mm | 16 (32) | 4 (80) | 8 (23.5) | 4 (36.4) | ||
| Post-dilatation | 6 (12) | 3 (60) | 1 (2.9) | 2 (18.2) | 0.001 | |
| Underfilling | 6 (12) | 0 (0) | 5 (14.7) | 1 (9.1) | 0.605 | |
| Prosthesis oversizing | (%) | 5.5 ± 10.3 | 9.4 ± 8.6 | 6.2 ± 9.9 | 1.9 ± 12.0 | 0.342 |
| THV tilt | (°) | 5.6 ± 3.6 | 4.4 ± 2.9 | 5.3 ± 3.7 | 7.0 ± 3.0 | 0.204 |
| Hourglass form of the THV | (%) | 7.4 ± 4.5 | 3.9 ± 6.4 | 7.4 ± 4.3 | 8.9 ± 3.7 | 0.214 |
| THV deployment | (%) | 91.9 ± 12.2 | 94.4 ± 3.6 | 90.6 ± 14.6 | 94.7 ± 3.4 | 0.421 |
| Mean expanded THV area | (mm2) | 457.6 ± 79.7 | 536.1 ± 65.2 | 443.3 ± 70.7 | 466.2 ± 95.5 | 0.098 |
| MPG after implantation | (mmHg) | 11.3 ± 3.9 | 9.8 ± 2.3 | 11.0 ± 3.2 | 13.0 ± 5.7 | 0.292 |
| Mean | 3.8 ± 2.6 | 4.7 ± 4.2 | 4.0 ± 2.4 | 3.1 ± 2.3 | 0.474 | |
| Implantation depth below | Left coronary cusp | 3.2 ± 2.9 | 4.0 ± 4.3 | 3.4 ± 2.7 | 2.4 ± 2.7 | 0.500 |
| annulus (mm) | Right coronary cusp | 4.2 ± 2.9 | 3.4 ± 4.2 | 4.9 ± 2.4 | 2.7 ± 3.5 | 0.130 |
| Non-coronary cusp | 4.1 ± 3.1 | 6.6 ± 4.8 | 3.7 ± 3.0 | 4.1 ± 2.1 | 0.382 | |
| 0.734 | ||||||
| Prosthesis position | Optimal | 45 (90) | 4 (80) | 31 (91.2) | 10 (90.9) | |
| Low | 5 (10) | 1 (20) | 3 (8.8) | 1 (9.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Breitbart, P.; Minners, J.; Czerny, M.; Hein, M.; Neumann, F.-J.; Ruile, P. Prosthesis Position after TAVI with Balloon-Expandable SAPIEN 3 in Bicuspid Aortic Valves. J. Clin. Med. 2021, 10, 2561. https://doi.org/10.3390/jcm10122561
Breitbart P, Minners J, Czerny M, Hein M, Neumann F-J, Ruile P. Prosthesis Position after TAVI with Balloon-Expandable SAPIEN 3 in Bicuspid Aortic Valves. Journal of Clinical Medicine. 2021; 10(12):2561. https://doi.org/10.3390/jcm10122561
Chicago/Turabian StyleBreitbart, Philipp, Jan Minners, Martin Czerny, Manuel Hein, Franz-Josef Neumann, and Philipp Ruile. 2021. "Prosthesis Position after TAVI with Balloon-Expandable SAPIEN 3 in Bicuspid Aortic Valves" Journal of Clinical Medicine 10, no. 12: 2561. https://doi.org/10.3390/jcm10122561
APA StyleBreitbart, P., Minners, J., Czerny, M., Hein, M., Neumann, F.-J., & Ruile, P. (2021). Prosthesis Position after TAVI with Balloon-Expandable SAPIEN 3 in Bicuspid Aortic Valves. Journal of Clinical Medicine, 10(12), 2561. https://doi.org/10.3390/jcm10122561