
Peripartum Pubic Symphysis Diastasis—Practical Guidelines

 , ,
, ,
Abstract
1. Introduction
2. Pubic Symphysis Diastasis—Incidence and Preliminary Characteristics
3. Anatomy and Pathophysiology of Pubic Symphysis
4. Etiology
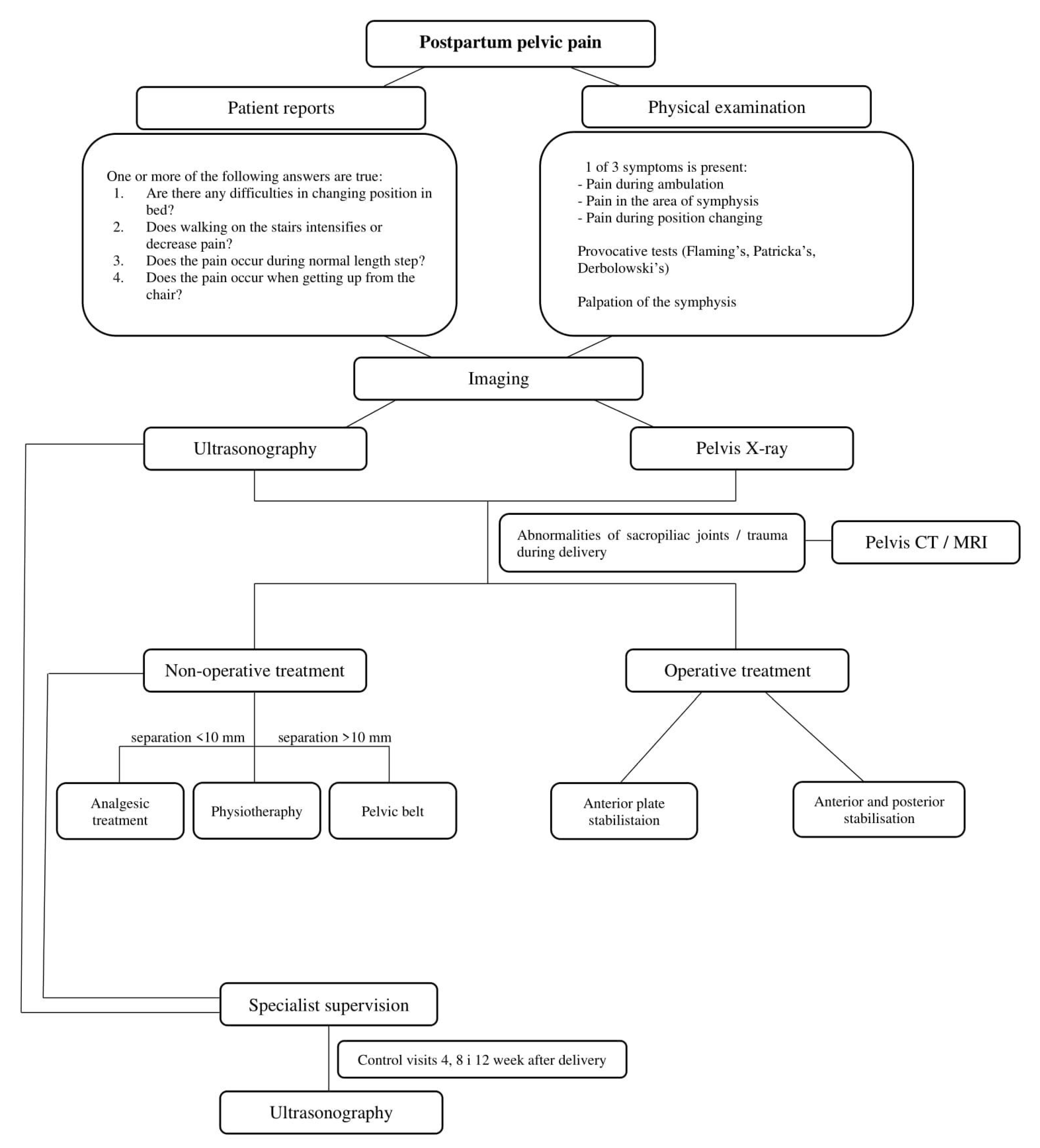
5. Clinical Symptoms
6. Differentiation
- Are you having difficulty rolling over in bed?
- Does pain increase/decrease when climbing stairs?
- Are you feeling uncomfortable during a full-length stride?
- Do you have difficulties getting up from low chairs?
- Does pelvic pain occur when moving small weights?
- Is there any pain when you roll over in bed?
- Is there any pain when getting up from a chair or walking upstairs?
- -
- History of pelvic pain after childbirth;
- -
- After excluding other diseases;
- -
- With obvious clinical symptoms.
7. Imaging
8. Non-Operative Treatment Approach
9. Invasive Methods of Treatment
10. Physiotherapy in the Dissolution of the Pubic Symphysis
11. PSD and Delivery
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Yoo, J.J.; Ha, Y.-C.; Lee, Y.-K.; Hong, J.S.; Kang, B.-J.; Koo, K.-H. Incidence and Risk Factors of Symptomatic Peripartum Diastasis of Pubic Symphysis. J. Korean Med. Sci. 2014, 29, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Rustamova, S.; Predanic, M.; Sumersille, M.; Cohen, W.R. Changes in symphysis pubis width during labor. J. Perinat. Med. 2009, 37, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Krzysztof, R. Zmiany fizjologiczne w organizmie kobiety ciężarnej i ich znaczenie w praktyce lekarza ogólnego. Przegląd Lekarski 2008, 65, 195–202. [Google Scholar]
- Hashem, G.; Zhang, Q.; Hayami, T.; Chen, J.; Wang, W.; Kapila, S. Relaxin and β-estradiol modulate targeted matrix degradation in specific synovial joint fibrocartilages: Progesterone prevents matrix loss. Arthritis Res. Ther. 2006, 8, R98. [Google Scholar] [CrossRef]
- Robson, S.E.; Waught, J. Medical Disorders in Pregnancy—A Manual for Midwives; Blackwell Publishing: Oxford, UK, 2008; p. 320. [Google Scholar]
- Sung, J.-H.; Kang, M.; Lim, S.-J.; Choi, S.-J.; Oh, S.-Y.; Roh, C.-R. A case-control study of clinical characteristics and risk factors of symptomatic postpartum pubic symphysis diastasis. Sci. Rep. 2021, 11, 3289. [Google Scholar] [CrossRef]
- Becker, I.; Woodley, S.J.; Stringer, M.D. The adult human pubic symphysis: A systematic review. J. Anat. 2010, 217, 475–487. [Google Scholar] [CrossRef] [PubMed]
- Casagrande, D.; Gugala, Z.; Clark, S.M.; Lindsey, R.W. Low Back Pain and Pelvic Girdle Pain in Pregnancy. J. Am. Acad. Orthop. Surg. 2015, 23, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Eedarapalli, P.; Jamjute, P.; Sawdy, R. Symphysis pubis dysfunction: A practical approach to management. Obstet. Gynaecol. 2006, 8, 153–158. [Google Scholar] [CrossRef]
- Herren, C.; Sobottke, R.; Dadgar, A.; Ringe, M.J.; Graf, M.; Keller, K.; Eysel, P.; Mallmann, P.; Siewe, J. Peripartum pubic symphysis separation—Current strategies in diagnosis and therapy and presentation of two cases. Injury 2015, 46, 1074–1080. [Google Scholar] [CrossRef]
- Wang, Y.; Li, Y.-Q.; Tian, M.-R.; Wang, N.; Zheng, Z.-C. Role of relaxin in diastasis of the pubic symphysis peripartum. World J. Clin. Cases 2021, 9, 91–101. [Google Scholar] [CrossRef]
- Bjorklund, K.; Bergstrom, S.; Nordstrom, M.L.; Ulmsten, U. Symphyseal distention in relation to serum relaxin levels and pelvic pain in pregnancy. Acta Obstet. Gynecol. Scand. 2000, 79, 269–275. [Google Scholar]
- Sujana, B.; Keepanasseril, A.; Maurya, D.K. Diastasis of the pubic symphysis following vaginal delivery. Int. J. Gynecol. Obstet. 2017, 139, 102–103. [Google Scholar] [CrossRef]
- Chawla, J.J.; Arora, D.; Sandhu, N.; Jain, M.; Kumari, A. Pubic Symphysis Diastasis: A Case Series and Literature Review. Oman Med. J. 2017, 32, 510–514. [Google Scholar] [CrossRef] [PubMed]
- Kumle, M.; Weiderpass, E.; Alsaker, E.; Lund, E. Use of Hormonal Contraceptives and Occurrence of Pregnancy-Related Pelvic Pain: A Prospective Cohort Study in Norway. BMC Pregnancy Childbirth 2004, 4, 11. [Google Scholar] [CrossRef] [PubMed]
- Consonni, S.R.; Werneck, C.C.; Sobreira, D.R.; Kühne, F.; Moraes, S.G.; Alvares, L.E.; Joazeiro, P.P. Elastic Fiber Assembly in the Adult Mouse Pubic Symphysis during Pregnancy and Postpartum1. Biol. Reprod. 2012, 86, 151. [Google Scholar] [CrossRef] [PubMed]
- Consonni, S.R.; Rosa, R.G.; Nascimento, M.A.; Vinagre, C.M.; Toledo, O.M.; Joazeiro, P.P. Recovery of the pubic symphysis on primiparous young and multiparous senescent mice at postpartum. Histol. Histopathol. 2012, 27, 885–896. [Google Scholar] [CrossRef] [PubMed]
- Castelucci, B.G.; Consonni, S.R.; Rosa, V.S.; Joazeiro, P.P. Recruitment of monocytes and mature macrophages in mouse pubic symphysis relaxation during pregnancy and postpartum recovery. Biol. Reprod. 2019, 101, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Castelucci, B.G.; Consonni, S.R.; Rosa, V.S.; Sensiate, L.A.; Delatti, P.C.R.; Alvares, L.E.; Joazeiro, P.P. Time-dependent regulation of morphological changes and cartilage differentiation markers in the mouse pubic symphysis during pregnancy and postpartum recovery. PLoS ONE 2018, 13, e0195304. [Google Scholar] [CrossRef]
- Norvilaite, K.; Kezeviciute, M.; Ramasauskaite, D.; Arlauskiene, A.; Bartkeviciene, D.; Uvarovas, V. Postpartum pubic symphysis diastasis-conservative and surgical treatment methods, incidence of complications: Two case reports and a review of the literature. World J. Clin. Cases 2020, 8, 110–119. [Google Scholar] [CrossRef]
- Urraca-Gesto, M.A.; Manzano, G.P.; Ferragut-Garcías, A.; Pecos-Martín, D.; Gallego-Izquierdo, T.; Romero-Franco, N. Diastasis of symphysis pubis and labor: Systematic review. J. Rehabil. Res. Dev. 2015, 52, 629–640. [Google Scholar] [CrossRef]
- Wellock, V. The ever widening gap—Symphysis pubis dysfunction. Br. J. Midwifery 2002, 10, 348–353. [Google Scholar] [CrossRef]
- William, S.R.; Kathleen, V. Pelvic Girdle Pain in Pregnancy. BMJ 2005, 331, 249–250. [Google Scholar]
- Elden, H.; Ladfors, L.; Olsen, M.F.; Ostgaard, H.C.; Hagberg, H. Effects of acupuncture and stabilising exercises as adjunct to standard treatment in pregnant women with pelvic girdle pain: Randomised single blind controlled trail. BMJ 2005, 330, 761. [Google Scholar] [CrossRef] [PubMed]
- Qiao, J.; Qin, J.; Feng, J.; Huang, M.; Xia, P. Relationship between Pubic Symphysis Separation and Postpartum Pelvic Girdle Pain: A Retrospective Study of 32 Cases. PM&R 2020, 12, 1222–1226. [Google Scholar] [CrossRef]
- Fry, D.; Hay-Smith, J.; Hough, J.; McIntosh, J.; Polden, M.; Shepherd, J.; Watkins, Y. National clinical guidelines for the care of women with symphysis pubis dysfunction. Association of Chartered Physiotherapists in Women’s Health. Midwives 1997, 110, 172–173. [Google Scholar] [PubMed]
- Kogstad, O.; Biornstad, N. Pelvic girdle relaxation. Pathogenesis, etiology, definition, epidemiology. Tidsskr. Nor. Laegeforen. 1990, 110, 2209–2211. [Google Scholar]
- Gupta, A.D. Sacroiliac joint pathologies in low back pain. J. Back Musculoskelet. Rehabil. 2009, 22, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Hou, Z.; Riehl, J.T.; Smith, W.R.; Strohecker, K.A.; Maloney, P.J. Severe postpartum disruption of the pelvic ring: Report of two cases and review of the literature. Patient Saf. Surg. 2011, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- Pires, R.; Labronici, P.; Giordano, V.; Kojima, K.; Kfuri, M.; Barbisan, M.; Wajnsztejn, A.; De Andrade, M. Intrapartum pubic symphysis disruption. Ann. Med. Health Sci. Res. 2015, 5, 476–479. [Google Scholar] [CrossRef]
- Khorashadi, L.; Petscavage, J.M.; Richardson, M.L. Postpartum symphysis pubis diastasis. Radiol. Case Rep. 2011, 6, 542. [Google Scholar] [CrossRef]
- Dunk, R.A.; Langhoff-Roos, J. Osteomyelitis of the pubic symphysis after spontaneous vaginal delivery. BMJ Case Rep. 2010, 2010. [Google Scholar] [CrossRef]
- Cosma, S.; Borella, F.; Carosso, A.; Ingala, A.; Fassio, F.; Robba, T.; Maina, A.; Bertero, L.; Benedetto, C. Osteomyelitis of the pubic symphysis caused by methicillin-resistant Staphylococcus aureus after vaginal delivery: A case report and literature review. BMC Infect. Dis. 2019, 19, 952. [Google Scholar] [CrossRef] [PubMed]
- Knoeller, S.M.; Uhl, M.; Herget, G.W. Osteitis or osteomyelitis of the pubis? A diagnostic and therapeutic challenge: Report of 9 cases and review of the literature. Acta Orthop. Belg. 2006, 72, 541–548. [Google Scholar]
- Yan, C.X.B.; Vautour, L.; Martin, M.-H. Postpartum sacral insufficiency fractures. Skelet. Radiol. 2015, 45, 413–417. [Google Scholar] [CrossRef]
- Budak, M.J.; Oliver, T.B. There’s a hole in my symphysis—A review of disorders causing widening, erosion, and destruction of the symphysis pubis. Clin. Radiol. 2013, 68, 173–180. [Google Scholar] [CrossRef]
- Zhang, S.; Dumas, G.; Hemmerich, A. Measurement of pubic symphysis width in different birthing positions using ultrasound. J. Biomech. 2020, 113, 110114. [Google Scholar] [CrossRef] [PubMed]
- Ianniello, S.; Conte, P.; Di Serafino, M.; Miele, V.; Trinci, M.; Vallone, G.; Galluzzo, M. Diagnostic accuracy of pubic symphysis ultrasound in the detection of unstable pelvis in polytrauma patients during e-FAST: The value of FAST-PLUS protocol. A preliminary experience. J. Ultrasound 2020. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.C.; Endo, Y.; Potter, H.G. Imaging of Groin Pain: Magnetic Resonance and Ultrasound Imaging Features. Sports Health 2017, 9, 428–435. [Google Scholar] [CrossRef]
- Depledge, J.; McNair, P.J.; Keal-Smith, C.; Williams, M. Management of symphysis pubis dysfunction during pregnancy using exercise and pelvic support belts. Phys. Ther. 2005, 85, 1290–1300. [Google Scholar] [CrossRef] [PubMed]
- Henry, L. Chiropractic management of postpartum pubic symphysis diastasis: A case report. J. Can. Chiropr. Assoc. 2015, 59, 30–36. [Google Scholar]
- Shnaekel, K.L.; Magann, E.F.; Ahmadi, S. Pubic Symphysis Rupture and Separation during Pregnancy. Obstet. Gynecol. Surv. 2015, 70, 713–718. [Google Scholar] [CrossRef]
- Seidman, A.; Brossy, K.; Faulkner, A.; Taylor, J. Traumatic Pelvic Ring Injury following Childbirth with Complete Pubic Symphysis Diastasis. Case Rep. Orthop. 2019, 2019, 1785167. [Google Scholar] [CrossRef][Green Version]
- Weil, Y.A.; Hierholzer, C.; Sama, D.; Wright, C.; Nousiainen, M.T.; Kloen, P.; Helfet, D.L. Management of persistent postpartum pelvic pain. Am. J. Orthop. 2008, 37, 621–626. [Google Scholar]
- Hierholzer, C.; Ali, A.; Toro-Arbelaez, J.B.; Suk, M.; Helfet, D.L. Traumatic disruption of pubis symphysis with accompanying posterior pelvic injury after natural childbirth. Am. J. Orthop. 2007, 36, E167–E170. [Google Scholar] [PubMed]
- Chang, J.L.; Wu, V. External fixation of pubic symphysis diastasis from postpartum trauma. Orthopedics 2008, 31, 493. [Google Scholar] [CrossRef]
- Najibi, S.; Tannast, M.; Klenck, R.E.; Matta, J.M. Internal fixation of symphyseal disruption resulting from childbirth. J. Orthop. Trauma 2010, 24, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Kotwal, P.P.; Mittal, R. Disruption of symphysis pubis during labor. Int. J. Gynaecol. Obstet. 1996, 54, 51–53. [Google Scholar] [CrossRef]
- Shippey, S.; Roth, J.; Gaines, R. Pubic symphysis diastasis with urinary incontinence: Collaborative surgical management. Int. Urogynecol. J. 2013, 24, 1757–1759. [Google Scholar] [CrossRef] [PubMed]
- Erickson, D.; Low, J.; Shumway, J. Management of Postpartum Diastasis of the Pubic Symphysis. Orthopedics 2016, 39, e367–e369. [Google Scholar] [CrossRef] [PubMed]
- Tripathy, S.K.; Samanta, S.K.; Varghese, P.; Nanda, S.N.; Agrawal, K. Late-Onset Sacroiliac Osteoarthritis after Surgical Symphysiotomy: A Case Report. Cureus 2020, 12, e11769. [Google Scholar] [CrossRef]
- Fidan, U.; Ulubay, M.; Keskin, U.; Fıratlıgil, F.B.; Karaşahin, K.E.; Ege, T.; Ergün, A. Postpartum symphysis pubis separation. Acta Obstet. Gynecol. Scand. 2013, 92, 1336–1337. [Google Scholar] [CrossRef] [PubMed]
- Heim, J.; Vang, S.; Thomas, A.; Ly, T.; Das, K. Effect of Pregnancy, Labor, Delivery and Postpartum on Physiological Pubic Symphysis Diastasis [23I]. Obstet. Gynecol. 2016, 127, 79S. [Google Scholar] [CrossRef]
- Osterhoff, G.; Ossendorf, C.; Ossendorf-Kimmich, N.; Zimmermann, R.; Wanner, G.A.; Simmen, H.P.; Werner, C.M. Surgical stabilization of postpartum symphyseal instability: Two cases and a review of the literature. Gynecol. Obstet. Investig. 2012, 73, 1–7. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Etiological Factors of Peripartum Pubic Symphysis Separation |
|---|
| Congenital pelvic asymmetry, hyperlordosis, pathological pelvic dimensions Improper regulation of collagen synthesis, generalized joint laxity Increased release of relaxin, estrogen and progesterone Metabolic abnormalities of wit. D and calcium turnover Past history of pelvic trauma Inflammation of sacropelvic joints/pubic symphysis Osteoarthritic changes Macrosomia, high mother’s age, previous complications during delivery Forceps delivery Sports: football, basketball, light athletics |
| Most Common Signs and Symptoms of Pubic Symphysis Separation |
|---|
| Pain radiating to sub-abdominal region, sacroiliac area, inguinal area, and lateral part of the thigh Problems with daily living activities (bending, standing on one leg, rising up, walking on the stairs, changing position in bed) Pain that wears off after rest Clicking in the area of pubic symphysis Swaying while walking (duckling) Urinary retention Urinary/fecal incontinence |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stolarczyk, A.; Stępiński, P.; Sasinowski, Ł.; Czarnocki, T.; Dębiński, M.; Maciąg, B. Peripartum Pubic Symphysis Diastasis—Practical Guidelines. J. Clin. Med. 2021, 10, 2443. https://doi.org/10.3390/jcm10112443
Stolarczyk A, Stępiński P, Sasinowski Ł, Czarnocki T, Dębiński M, Maciąg B. Peripartum Pubic Symphysis Diastasis—Practical Guidelines. Journal of Clinical Medicine. 2021; 10(11):2443. https://doi.org/10.3390/jcm10112443
Chicago/Turabian StyleStolarczyk, Artur, Piotr Stępiński, Łukasz Sasinowski, Tomasz Czarnocki, Michał Dębiński, and Bartosz Maciąg. 2021. "Peripartum Pubic Symphysis Diastasis—Practical Guidelines" Journal of Clinical Medicine 10, no. 11: 2443. https://doi.org/10.3390/jcm10112443
APA StyleStolarczyk, A., Stępiński, P., Sasinowski, Ł., Czarnocki, T., Dębiński, M., & Maciąg, B. (2021). Peripartum Pubic Symphysis Diastasis—Practical Guidelines. Journal of Clinical Medicine, 10(11), 2443. https://doi.org/10.3390/jcm10112443