
Preadmission Statin Prescription and Inpatient Myocardial Infarction in Geriatric Hip Fracture

 ,
, 
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Setting and Population
2.2. Data
2.3. Outcomes
2.4. Statistics
3. Results
3.1. Demographic and Disease-Related Characteristics
3.2. Propensity Score Model
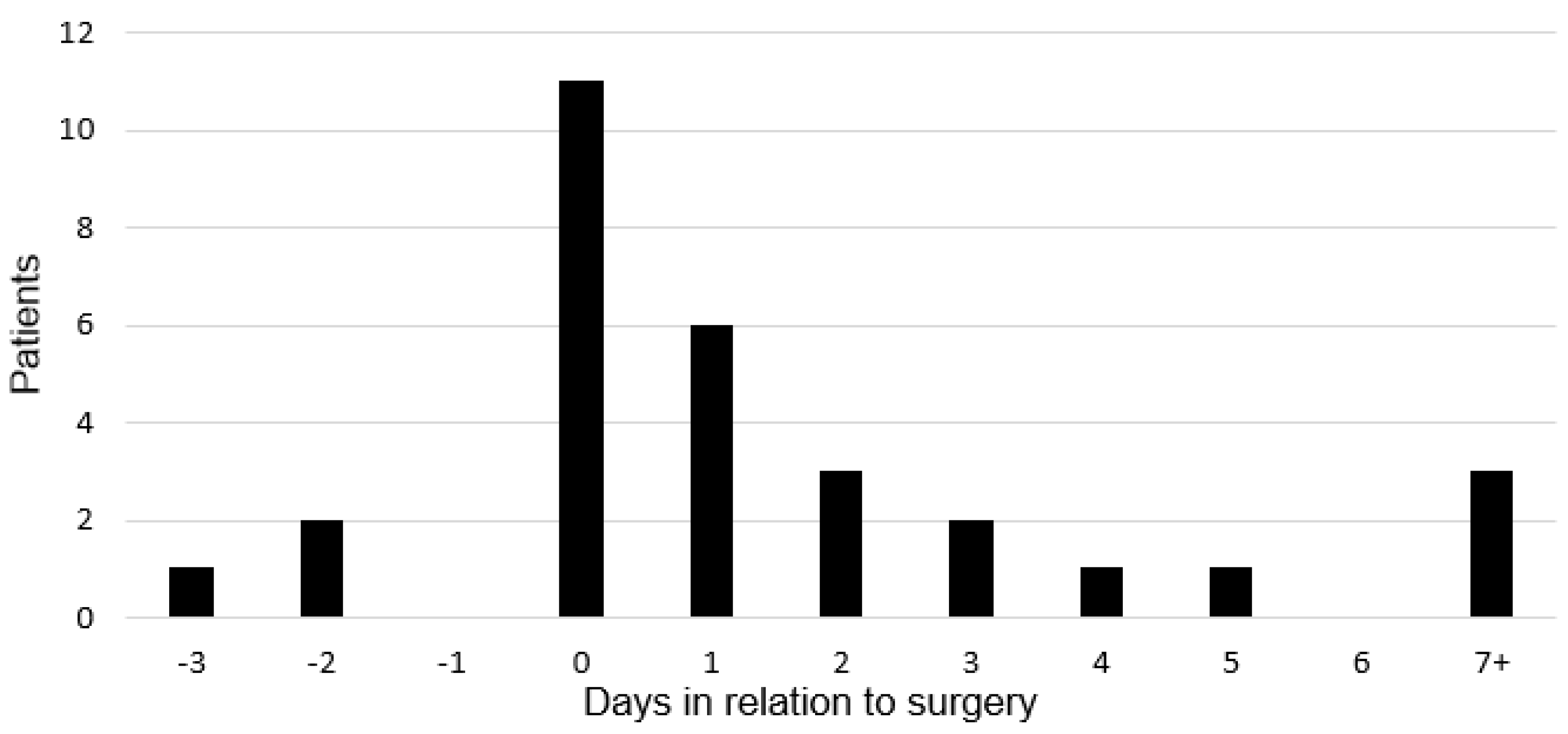
3.3. Myocardial Infarction
3.4. Outcomes
3.4.1. Primary Outcome: Association between Statin Use and Myocardial Infarction
3.4.2. Secondary Outcome: Association between Statin Use, Myocardial Infarction, and Mortality
4. Discussion
4.1. Statin Use in Hip Fracture
4.2. Hip Fracture and MI
4.3. Statin Use and MI in Hip Fracture
4.4. Limitations
4.5. Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cooper, C.; Cole, Z.A.; Holroyd, C.R.; Earl, S.C.; Harvey, N.C.; Dennison, E.M.; Melton, L.J.; Cummings, S.R.; Kanis, J.A. Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos. Int. 2011, 22, 1277–1288. [Google Scholar] [CrossRef]
- Bergstrom, U.; Jönsson, H.; Gustafson, Y.; Pettersson, U.; Stenlund, H.; Svensson, O. The hip fracture incidence curve is shifting to the right. Acta Orthop. 2009, 80, 520–524. [Google Scholar] [CrossRef]
- Roche, J.J.W.; Wenn, R.T.; Sahota, O.; Moran, C.G. Effect of comorbidities and postoperative complications on mortality after hip fracture in elderly people: Prospective observational cohort study. BMJ 2005, 331, 1374. [Google Scholar] [CrossRef] [PubMed]
- Hietala, P.; Strandberg, M.; Kiviniemi, T.; Strandberg, N.; Airaksinen, K.J. Usefulness of Troponin T to Predict Short-Term and Long-Term Mortality in Patients After Hip Fracture. Am. J. Cardiol. 2014, 114, 193–197. [Google Scholar] [CrossRef]
- Juliebø, V.; Krogseth, M.; Skovlund, E.; Engedal, K.; Wyller, T.B. Medical Treatment Predicts Mortality After Hip Fracture. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2009, 65, 442–449. [Google Scholar] [CrossRef]
- Jantzen, C.; Madsen, C.M.; Abrahamsen, B.; Van Der Mark, S.; Duus, B.R.; Howland, J.; Lauritzen, J.B.; Jørgensen, H.L. Pre-fracture medication use as a predictor of 30-day mortality in hip fracture patients: An analysis of 141,201 patients. HIP Int. 2020, 30, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.K.; Ridker, P.M. Anti-Inflammatory Effects of Statins: Clinical Evidence and Basic Mechanisms. Nat. Rev. Drug Discov. 2005, 4, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Chopra, V.; Wesorick, D.H.; Sussman, J.B.; Greene, T.; Rogers, M.; Froehlich, J.B.; Eagle, K.A.; Saint, S. Effect of perioperative statins on death, my-ocardial infarction, atrial fibrillation, and length of stay: A systematic review and meta-analysis. Arch. Surg. 2012, 147, 181–189. [Google Scholar] [CrossRef]
- Hietala, P.; Strandberg, M.; Strandberg, N.; Gullichsen, E.; Airaksinen, K.J. Perioperative myocardial infarctions are common and often unrecognized in patients undergoing hip fracture surgery. J. Trauma Acute Care Surg. 2013, 74, 1087–1091. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Saklad, M. Grading of patients for surgical procedures. Anesthesiology 1941, 2, 281–284. [Google Scholar] [CrossRef]
- Lee, T.H.; Marcantonio, E.R.; Mangione, C.M.; Thomas, E.J.; Polanczyk, C.A.; Cook, E.F.; Sugarbaker, D.J.; Donaldson, M.C.; Poss, R.; Ho, K.K.L.; et al. Derivation and Prospective Validation of a Simple Index for Prediction of Cardiac Risk of Major Noncardiac Surgery. Circulation 1999, 100, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Alpert, J.S.; Thygesen, K.; Antman, E.; Bassand, J.P. Myocardial infarction redefined—A consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J. Am. Coll. Cardiol. 2000, 36, 959–969. [Google Scholar] [PubMed]
- Chong, C.P.; Lim, W.K.; Velkoska, E.; van Gaal, W.J.; Ryan, J.E.; Savige, J.; Burrell, L.M. N-terminal pro-brain natriuretic peptide and angi-otensin-converting enzyme-2 levels and their association with postoperative cardiac complications after emergency orthopedic surgery. Am. J. Cardiol. 2012, 109, 1365–1373. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Zhang, Y.; Yin, L.; Zhang, L.; Wang, Y.; Zhang, H.; Li, B. Statin in the treatment of patients with myocardial infarction: A meta-analysis. Medicine 2018, 97, e0167. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.; Feely, J. Pharmacokinetic-pharmacodynamic drug interactions with HMG-CoA reductase inhibitors. Clin. Pharmacokinet. 2002, 41, 343–370. [Google Scholar] [CrossRef]
- Ushirozako, H.; Ohishi, T.; Fujita, T.; Suzuki, D.; Yamamoto, K.; Banno, T.; Takase, H.; Matsuyama, Y. Does N-terminal Pro-brain Type Natriuretic Peptide Predict Cardiac Complications After Hip Fracture Surgery? Clin. Orthop. Relat. Res. 2017, 475, 1730–1736. [Google Scholar] [CrossRef] [PubMed]
- Nordling, P.; Kiviniemi, T.; Strandberg, M.; Strandberg, N.; Airaksinen, J. Predicting the outcome of hip fracture patients by using N-terminal fragment of pro-B-type natriuretic peptide. BMJ Open 2016, 6, e009416. [Google Scholar] [CrossRef] [PubMed]
- Madsen, C.M.; Jantzen, C.; Lauritzen, J.B.; Abrahamsen, B.; Jorgensen, H.L. Temporal trends in the use of antithrombotics at ad-mission. Acta Orthop. 2016, 87, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Ginsel, B.L.; Taher, A.; Whitehouse, S.L.; Bell, J.J.; Pulle, C.R.; Crawford, R.W. Effects of Anticoagulants on Outcome of Femoral Neck Fracture Surgery. J. Orthop. Surg. 2015, 23, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Chia, P.H.; Gualano, L.; Seevanayagam, S.; Weinberg, L. Outcomes following fractured neck of femurin an Australian metro-politan teaching hospital. Bone Joint. Res. 2013, 2, 162–168. [Google Scholar] [CrossRef]
- Menendez, M.E.; Ring, D. Failure to Rescue After Proximal Femur Fracture Surgery. J. Orthop. Trauma 2015, 29, e96–e102. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.; Chung, A.S.; Walker, J.B.; Hustedt, J.W.; Russell, G.V.; Jones, C.B. Delay in Hip Fracture Surgery Prolongs Postoperative Hospital Length of Stay but Does Not Adversely Affect Outcomes at 30 Days. J. Orthop. Trauma 2018, 32, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, A.B.; Ehrenstein, V.; Szépligeti, S.K.; Sørensen, H.T. Hip Fracture, Comorbidity, and the Risk of Myocardial Infarction and Stroke: A Danish Nationwide Cohort Study, 1995–2015. J. Bone Miner. Res. 2017, 32, 2339–2346. [Google Scholar] [CrossRef] [PubMed]
- Dunkelgrun, M.; Boersma, E.; Schouten, O.; Koopman-van Gemert, A.W.; van Poorten, F.; Bax, J.J.; Thomson, I.R.; Poldermans, D.; Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. Bisoprolol and fluvastatin for the reduction of perioperative cardiac mortality and myocardial infarction in intermediate-risk patients undergoing noncardio-vascular surgery: A randomized controlled trial (DECREASE-IV). Ann. Surg. 2009, 249, 921–926. [Google Scholar] [CrossRef]
- (STAFF) SiHF. 2012. Available online: https://clinicaltrials.gov/ct2/show/NCT01494090 (accessed on 26 April 2021).
- Bass, A.R.; Szymonifka, J.D.; Rondina, M.T.; Bogardus, M.; Scott, M.G.; Woller, S.C.; Stevens, S.M.; Eby, C.; Merritt, K.; della Valle, A.G.; et al. Postoperative Myocardial Injury and Inflammation Is Not Blunted by a Trial of Atorvastatin in Orthopedic Surgery Patients. HSS J. 2018, 14, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Rudd, N.; Subiakto, I.; Asrar Ul Haq, M.; Mutha, V.; Van Gaal, W.J. Use of ivabradine and atorvastatin in emergent orthopedic lower limb surgery and computed tomography coronary plaque imaging and novel biomarkers of cardiovascular stress and lipid me-tabolism for the study and prevention of perioperative myocardial infarction: Study protocol for a randomized controlled trial. Trials 2014, 15, 352. [Google Scholar]
- ANZHFR Bi-National Annual Report of Hip Fracture Care 2018; Australian and New Zealand Hip Fracture Registry: Randwick, NSW, Australia, 2018.
- Sun, T.; Wang, X.; Liu, Z.; Chen, X.; Zhang, J. Plasma concentrations of pro- and anti-inflammatory cytokines and outcome pre-diction in elderly hip fracture patients. Injury 2011, 42, 707–713. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No Statin | Statin | Total | ||
|---|---|---|---|---|
| Characteristic | (n = 775) | (n = 391) | (n = 1166) | p-Value |
| Age (years; mean, SD) | 85 (8) | 82 (7) | 84 (8) | <0.001 |
| Sex (Female; n, %) | 551 (71%) | 257 (66%) | 808 (69%) | 0.061 |
| Type (n, %) | ||||
| Atorvastatin | 184 (47%) | |||
| Simvastatin | 91 (23%) | |||
| Rosuvastatin | 87 (22%) | |||
| Pravastatin | 27 (6.9%) | |||
| Surgery Performed (yes; n, %) | 758 (98%) | 382 (98%) | 1140 (98%) | 0.906 |
| CCI (mean, SD) | 6 (2) | 7 (2) | 6 (2) | 0.357 |
| ASA grade (mean, SD) | 3.1 (0.7) | 3.1 (0.6) | 3.1 (0.7) | 0.169 |
| RCRI (median, Q1–Q3) | 0 (0,1) | 1 (0,2) | 1 (0,1) | <0.001 |
| Cardiac-related Comorbidity | ||||
| Ischaemic Heart Disease | 160 (21%) | 157 (40%) | 317 (27%) | <0.001 |
| Congestive Cardiac Failure | 115 (15%) | 59 (15%) | 174 (15%) | 0.910 |
| Cerebrovascular Disease | 216 (28%) | 155 (40%) | 371 (32%) | <0.001 |
| Hypertension | 451 (58%) | 280 (72%) | 731 (63%) | <0.001 |
| Peripheral Vascular Disease | 45 (5.8%) | 35 (9.0%) | 80 (6.9%) | 0.045 |
| Previous Acute Pulmonary Oedema | 37 (4.8%) | 41 (10%) | 78 (6.7%) | <0.001 |
| Existing Atrial Fibrillation | 215 (19%) | 5 (16%) | 220 (19%) | 0.503 |
| Valvular heart disease | 25 (3.2%) | 14 (3.6%) | 39 (3.3%) | 0.750 |
| Prosthetic valve | 6 (0.8%) | 7 (1.8%) | 13 (1.1%) | 0.119 |
| Aortic aneurysm | 18 (2.3%) | 19 (4.9%) | 37 (3.2%) | 0.020 |
| Pacemaker | 23 (3.0%) | 15 (3.8%) | 38 (3.3%) | 0.430 |
| Non-cardiac Comorbidity | ||||
| Chronic Renal Failure | 81 (10%) | 69 (18%) | 150 (13%) | <0.001 |
| Diabetes Mellitus | 104 (13%) | 116 (30%) | 220 (19%) | <0.001 |
| Gastro-oesophageal Reflux Disease | 215 (28%) | 134 (34%) | 349 (30%) | 0.022 |
| Chronic Obstructive Pulmonary Disease | 117 (15%) | 62 (16%) | 79 (6.8%) | 0.734 |
| Malignancy | 153 (19%) | 71 (18%) | 224 (19%) | 0.517 |
| Dementia | 235 (30%) | 82 (21%) | 317 (27%) | <0.001 |
| Hypercholesterolaemia | 67 (8.6%) | 210 (54%) | 277 (24%) | <0.001 |
| Medications | ||||
| Antiplatelet | 235 (30%) | 223 (57%) | 458 (39%) | <0.001 |
| Beta blocker | 188 (24%) | 169 (43%) | 357 (31%) | <0.001 |
| Calcium channel blocker | 100 (13%) | 86 (22%) | 186 (16%) | <0.001 |
| Angiotensin converting enzyme inhibitor | 91 (12%) | 122 (31%) | 269 (23%) | <0.001 |
| Angiotensin Receptor Blocker | 91 (12%) | 79 (20%) | 170 (15%) | <0.001 |
| Frusemide | 195 (25%) | 111 (28%) | 306 (26%) | 0.237 |
| Spironolactone | 50 (6.5%) | 39 (10%) | 89 (7.6%) | 0.032 |
| Ezetimibe | 7 (0.9%) | 6 (1.5%) | 13 (1.1%) | 0.332 |
| Nitro vasodilators | 124 (16%) | 73 (19%) | 197 (17%) | 0.251 |
| NSAID | 23 (3.0%) | 9 (2.3%) | 32 (2.7%) | 0.511 |
| Corticosteroids | 59 (7.6%) | 18 (4.6%) | 77 (6.6%) | 0.051 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarrant, S.M.; Kim, R.G.; McDonogh, J.M.; Clapham, M.; Palazzi, K.; Attia, J.; Balogh, Z.J. Preadmission Statin Prescription and Inpatient Myocardial Infarction in Geriatric Hip Fracture. J. Clin. Med. 2021, 10, 2441. https://doi.org/10.3390/jcm10112441
Tarrant SM, Kim RG, McDonogh JM, Clapham M, Palazzi K, Attia J, Balogh ZJ. Preadmission Statin Prescription and Inpatient Myocardial Infarction in Geriatric Hip Fracture. Journal of Clinical Medicine. 2021; 10(11):2441. https://doi.org/10.3390/jcm10112441
Chicago/Turabian StyleTarrant, Seth M., Raymond G. Kim, Jack M. McDonogh, Matthew Clapham, Kerrin Palazzi, John Attia, and Zsolt J. Balogh. 2021. "Preadmission Statin Prescription and Inpatient Myocardial Infarction in Geriatric Hip Fracture" Journal of Clinical Medicine 10, no. 11: 2441. https://doi.org/10.3390/jcm10112441
APA StyleTarrant, S. M., Kim, R. G., McDonogh, J. M., Clapham, M., Palazzi, K., Attia, J., & Balogh, Z. J. (2021). Preadmission Statin Prescription and Inpatient Myocardial Infarction in Geriatric Hip Fracture. Journal of Clinical Medicine, 10(11), 2441. https://doi.org/10.3390/jcm10112441