
Inappropriate Use of Oral Antithrombotic Combinations in an Outpatient Setting and Associated Risks: A French Nationwide Cohort Study


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
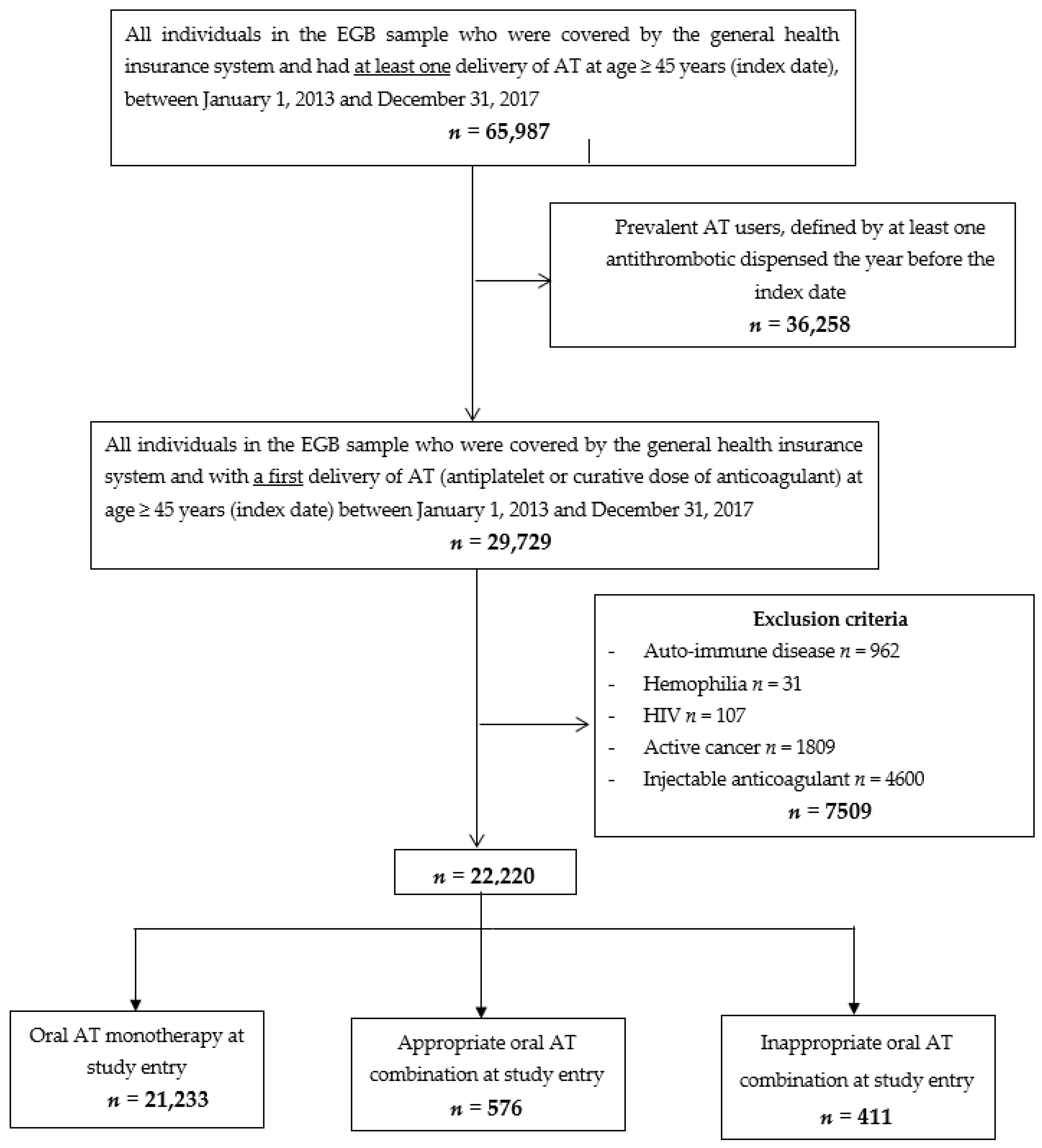
2.2. Study Population
2.3. Exposure
2.4. Outcomes
2.5. Baseline Characteristics of Individuals
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Individuals
3.2. AT Prescriptions
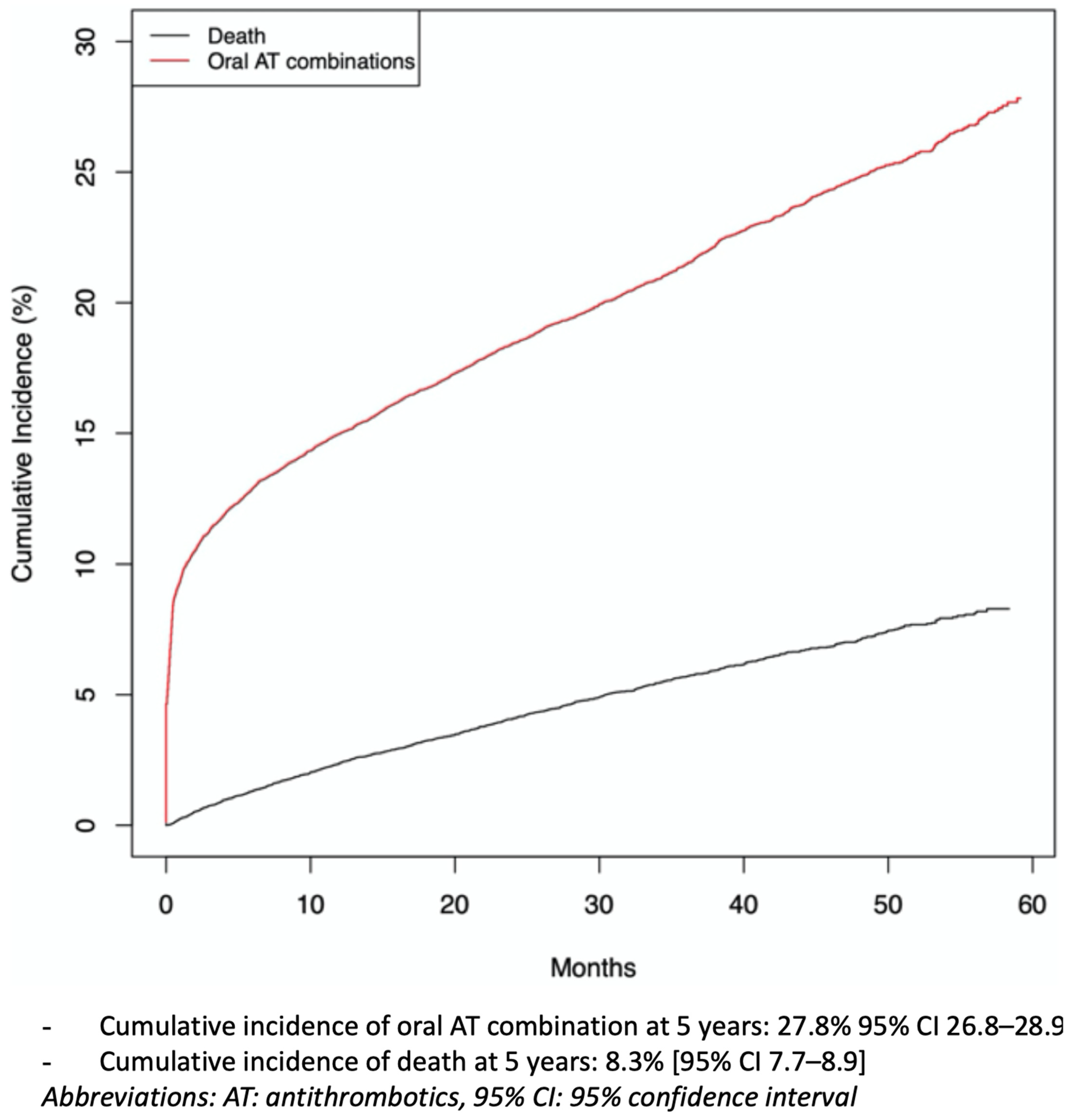
3.3. Cumulative Incidence of Oral AT Combination
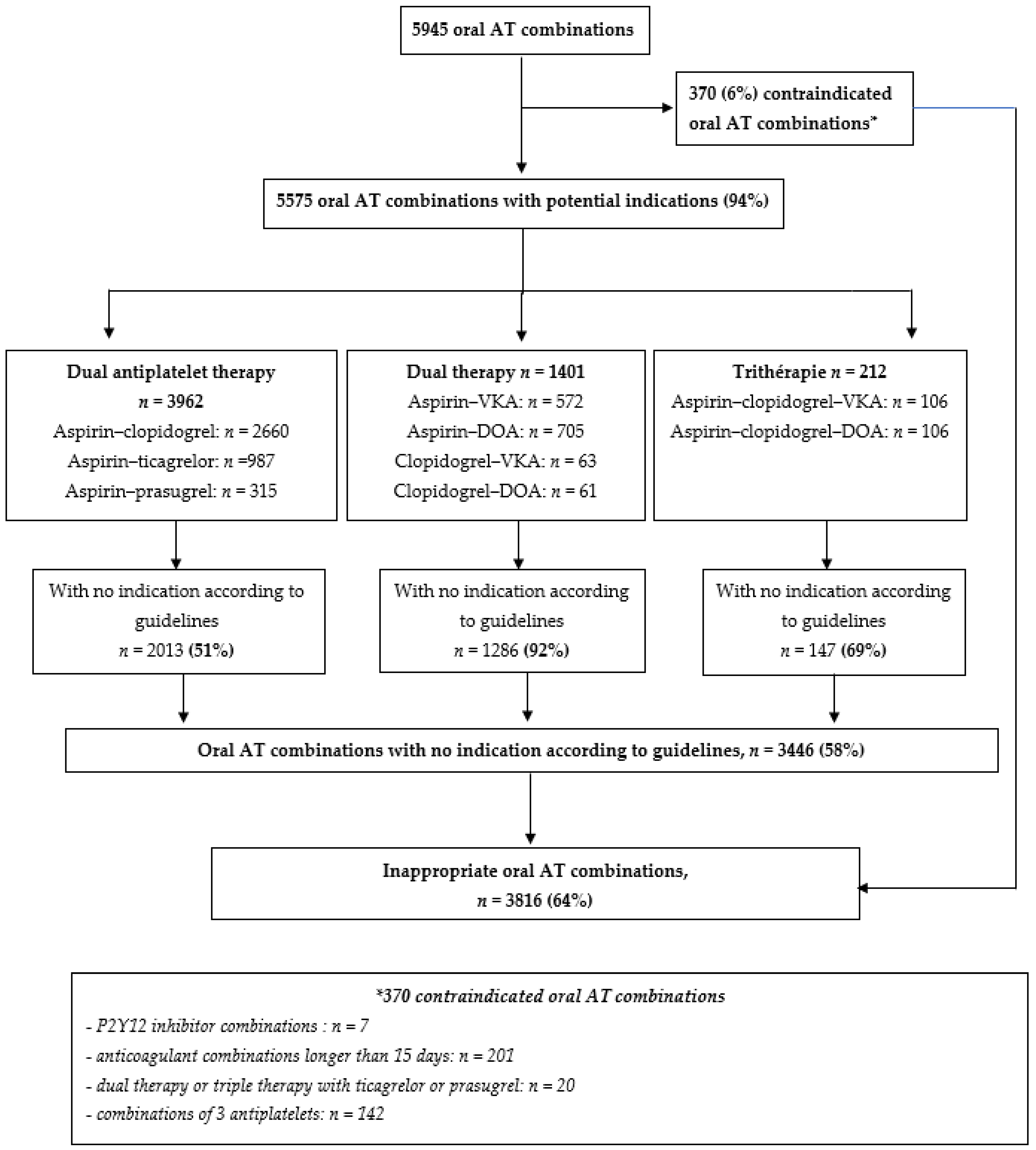
3.4. Appropriateness of Oral AT Combinations
3.5. Risk of Major Bleeding and Death
4. Discussion
4.1. Strengths and Weaknesses of the Study
4.2. Comparisons with Previous Studies
4.3. Implications for Clinical Practice and Public Health
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shehab, N.; Lovegrove, M.C.; Geller, A.I.; Rose, K.O.; Weidle, N.J.; Budnitz, D.S. US Emergency Department Visits for Outpatient Adverse Drug Events, 2013–2014. JAMA 2016, 316, 2115–2125. [Google Scholar] [CrossRef] [PubMed]
- Patel, T.K.; Patel, P.B. Mortality among Patients Due to Adverse Drug Reactions That Lead to Hospitalization: A Meta-Analysis. Eur. J. Clin. Pharmacol. 2018, 74, 819–832. [Google Scholar] [CrossRef]
- Hansen, M.L.; Sørensen, R.; Clausen, M.T.; Fog-Petersen, M.L.; Raunsø, J.; Gadsbøll, N.; Gislason, G.H.; Folke, F.; Andersen, S.S.; Schramm, T.K.; et al. Risk of Bleeding with Single, Dual, or Triple Therapy with Warfarin, Aspirin, and Clopidogrel in Patients with Atrial Fibrillation. Arch. Intern. Med. 2010, 170, 1433–1441. [Google Scholar] [CrossRef] [PubMed]
- van Rein, N.; Heide-Jørgensen, U.; Lijfering, W.M.; Dekkers, O.M.; Sørensen, H.T.; Cannegieter, S.C. Major Bleeding Rates in Atrial Fibrillation Patients on Single, Dual, or Triple Antithrombotic Therapy. Circulation 2019, 139, 775–786. [Google Scholar] [CrossRef] [PubMed]
- Gurwitz, J.H.; Field, T.S.; Harrold, L.R.; Rothschild, J.; Debellis, K.; Seger, A.C.; Cadoret, C.; Fish, L.S.; Garber, L.; Kelleher, M.; et al. Incidence and Preventability of Adverse Drug Events among Older Persons in the Ambulatory Setting. JAMA 2003, 289, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Pirmohamed, M.; James, S.; Meakin, S.; Green, C.; Scott, A.K.; Walley, T.J.; Farrar, K.; Park, B.K.; Breckenridge, A.M. Adverse Drug Reactions as Cause of Admission to Hospital: Prospective Analysis of 18 820 Patients. BMJ 2004, 329, 15–19. [Google Scholar] [CrossRef]
- Hallas, J.; Harvald, B.; Gram, L.F.; Grodum, E.; Brøsen, K.; Haghfelt, T.; Damsbo, N. Drug Related Hospital Admissions: The Role of Definitions and Intensity of Data Collection, and the Possibility of Prevention. J. Intern. Med. 1990, 228, 83–90. [Google Scholar] [CrossRef]
- Mega, J.L.; Simon, T. Pharmacology of Antithrombotic Drugs: An Assessment of Oral Antiplatelet and Anticoagulant Treatments. Lancet 2015, 386, 281–291. [Google Scholar] [CrossRef]
- De Caterina, R.; Ammentorp, B.; Darius, H.; Le Heuzey, J.-Y.; Renda, G.; Schilling, R.J.; Schliephacke, T.; Reimitz, P.-E.; Schmitt, J.; Schober, C.; et al. Frequent and Possibly Inappropriate Use of Combination Therapy with an Oral Anticoagulant and Antiplatelet Agents in Patients with Atrial Fibrillation in Europe. Heart 2014, 100, 1625–1635. [Google Scholar] [CrossRef]
- Zerah, L.; Bonnet-Zamponi, D.; Dechartres, A.; Frappé, P.; Hauguel-Moreau, M.; Collet, J.-P.; Rycke, Y.D.; Tubach, F. Impact of a Prescription Support Tool to Improve Adherence to the Guidelines for the Prescription of Oral Antithrombotics: The Combi-AT Randomized Controlled Trial Using Clinical Vignettes. J. Clin. Med. 2019, 8, 1919. [Google Scholar] [CrossRef]
- Tuppin, P.; Rudant, J.; Constantinou, P.; Gastaldi-Ménager, C.; Rachas, A.; de Roquefeuil, L.; Maura, G.; Caillol, H.; Tajahmady, A.; Coste, J.; et al. Value of a National Administrative Database to Guide Public Decisions: From the Système National d’information Interrégimes de l’Assurance Maladie (SNIIRAM) to the Système National Des Données de Santé (SNDS) in France. Rev. Epidemiol. Sante Publique 2017, 65 (Suppl. 4), S149–S167. [Google Scholar] [CrossRef]
- Bezin, J.; Duong, M.; Lassalle, R.; Droz, C.; Pariente, A.; Blin, P.; Moore, N. The National Healthcare System Claims Databases in France, SNIIRAM and EGB: Powerful Tools for Pharmacoepidemiology. Pharmacoepidemiol. Drug Saf. 2017, 26, 954–962. [Google Scholar] [CrossRef]
- Ray, W.A. Evaluating Medication Effects Outside of Clinical Trials: New-User Designs. Am. J. Epidemiol. 2003, 158, 915–920. [Google Scholar] [CrossRef] [PubMed]
- Raebel, M.A.; Schmittdiel, J.; Karter, A.J.; Konieczny, J.L.; Steiner, J.F. Standardizing Terminology and Definitions of Medication Adherence and Persistence in Research Employing Electronic Databases. Med. Care 2013, 51, S11–S21. [Google Scholar] [CrossRef]
- Forbes, C.A.; Deshpande, S.; Sorio-Vilela, F.; Kutikova, L.; Duffy, S.; Gouni-Berthold, I.; Hagström, E. A Systematic Literature Review Comparing Methods for the Measurement of Patient Persistence and Adherence. Curr. Med. Res. Opin. 2018, 34, 1613–1625. [Google Scholar] [CrossRef] [PubMed]
- Zerah, L.; Bun, R.-S.; Guillo, S.; Collet, J.-P.; Bonnet-Zamponi, D.; Tubach, F. A Prescription Support-Tool for Chronic Management of Oral Antithrombotic Combinations in Adults Based on a Systematic Review of International Guidelines. PLoS ONE 2019, 14, e0211695. [Google Scholar] [CrossRef] [PubMed]
- Brandes, A. Combined Anticoagulation and Antiplatelet Therapy in AF Patients: Why Do We Not Follow Guidelines? Heart 2014, 100, 1565–1566. [Google Scholar] [CrossRef] [PubMed]
- Gnjidic, D.; Hilmer, S.N.; Blyth, F.M.; Naganathan, V.; Waite, L.; Seibel, M.J.; McLachlan, A.J.; Cumming, R.G.; Handelsman, D.J.; Le Couteur, D.G. Polypharmacy Cutoff and Outcomes: Five or More Medicines Were Used to Identify Community-Dwelling Older Men at Risk of Different Adverse Outcomes. J. Clin. Epidemiol. 2012, 65, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C.; Fine, J.P. Practical Recommendations for Reporting Fine-Gray Model Analyses for Competing Risk Data. Stat. Med. 2017, 36, 4391–4400. [Google Scholar] [CrossRef]
- Maura, G.; Billionnet, C.; Drouin, J.; Weill, A.; Neumann, A.; Pariente, A. Oral Anticoagulation Therapy Use in Patients with Atrial Fibrillation after the Introduction of Non-Vitamin K Antagonist Oral Anticoagulants: Findings from the French Healthcare Databases, 2011–2016. BMJ Open 2019, 9, e026645. [Google Scholar] [CrossRef]
- Bouillon, K.; Bertrand, M.; Maura, G.; Blotière, P.-O.; Ricordeau, P.; Zureik, M. Risk of Bleeding and Arterial Thromboembolism in Patients with Non-Valvular Atrial Fibrillation Either Maintained on a Vitamin K Antagonist or Switched to a Non-Vitamin K-Antagonist Oral Anticoagulant: A Retrospective, Matched-Cohort Study. Lancet Haematol. 2015, 2, e150–e159. [Google Scholar] [CrossRef]
- Maura, G.; Blotière, P.-O.; Bouillon, K.; Billionnet, C.; Ricordeau, P.; Alla, F.; Zureik, M. Comparison of the Short-Term Risk of Bleeding and Arterial Thromboembolic Events in Nonvalvular Atrial Fibrillation Patients Newly Treated with Dabigatran or Rivaroxaban versus Vitamin K Antagonists: A French Nationwide Propensity-Matched Cohort Study. Circulation 2015, 132, 1252–1260. [Google Scholar] [CrossRef] [PubMed]
- Barben, J.; Menu, D.; Rosay, C.; Vovelle, J.; Mihai, A.-M.; Nuss, V.; d’Athis, P.; Putot, A.; Manckoundia, P. The Prescription of Direct Oral Anticoagulants in the Elderly: An Observational Study of 19 798 Ambulatory Subjects. Int. J. Clin. Pract. 2020, 74, e13420. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.X.; Adhikari, N.K.J.; McDonald, H.; Rosas-Arellano, M.P.; Devereaux, P.J.; Beyene, J.; Sam, J.; Haynes, R.B. Effects of Computerized Clinical Decision Support Systems on Practitioner Performance and Patient Outcomes: A Systematic Review. JAMA 2005, 293, 1223–1238. [Google Scholar] [CrossRef] [PubMed]
- Bright, T.J.; Wong, A.; Dhurjati, R.; Bristow, E.; Bastian, L.; Coeytaux, R.R.; Samsa, G.; Hasselblad, V.; Williams, J.W.; Musty, M.D.; et al. Effect of Clinical Decision-Support Systems: A Systematic Review. Ann. Intern. Med. 2012, 157, 29–43. [Google Scholar] [CrossRef] [PubMed]
- Sennesael, A.-L.; Krug, B.; Sneyers, B.; Spinewine, A. Do Computerized Clinical Decision Support Systems Improve the Prescribing of Oral Anticoagulants? A Systematic Review. Thromb. Res. 2020, 187, 79–87. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total n = 22,220 | Oral AT Monotherapy n = 21,233 | Appropriate Oral AT Combination n = 576 | Inappropriate Oral AT Combination n = 411 | p | |
|---|---|---|---|---|---|
| Mean (SD) age, years | 68 (12) | 68 (12) | 64 (12) | 68 (12) | <0.0001 |
| 45–64 | 9310 (42) | 8807 (42) | 337 (58) | 166 (40) | |
| 65–79 | 8624 (39) | 8295 (39) | 166 (29) | 163 (40) | |
| ≥80 | 4286 (19) | 4131 (19) | 73 (13) | 82 (20) | |
| Sex | <0.0001 | ||||
| Male | 11,048 (50) | 10,411 (49) | 405 (70) | 232 (56) | |
| Comorbidities | |||||
| Hypertension | 12,862 (58) | 12,311 (58) | 300 (52) | 251 (61) | 0.008 |
| Diabetes | 5109 (23) | 4942 (23) | 78 (14) | 89 (22) | <0.0001 |
| Dyslipidemia | 7243 (33) | 6973 (33) | 142 (25) | 128 (31) | 0.0002 |
| Obesity | 2206 (10) | 2073 (10) | 87 (15) | 46 (11) | <0.0001 |
| Coronary heart disease | 3278 (15) | 2578 (12) | 568 (99) | 132 (32) | <0.0001 |
| Non-valvular atrial fibrillation | 1935 (9) | 1862 (9) | 11 (2) | 62 (15) | <0.0001 |
| Valvular heart disease | 487 (2) | 402 (2) | 7 (1) | 78 (19) | <0.0001 |
| Heart failure | 766 (3) | 721 (3) | 16 (3) | 29 (7) | 0.0002 |
| Peripheral vascular disease | 1512 (7) | 1424 (7) | 42 (7) | 46 (11) | 0.001 |
| VTE disease | 759 (3) | 739 (3) | 10 (2) | 10 (2) | 0.04 |
| Stroke or arterial embolism | 1497 (7) | 1456 (7) | 6 (1) | 35 (9) | <0.0001 |
| Chronic kidney disease | 818 (4) | 773 (4) | 19 (3) | 26 (6) | 0.01 |
| Chronic hepatic disease | 486 (2) | 464 (2) | 11 (2) | 11 (3) | 0.71 |
| Anemia | 1259 (6) | 1203 (6) | 24 (4) | 32 (8) | 0.05 |
| History of bleeding | 612 (3) | 587 (3) | 14 (2) | 11 (3) | 0.89 |
| Dementia | 781 (4) | 767 (4) | 6 (1) | 8 (2) | 0.0009 |
| COPD | 829 (4) | 784 (4) | 22 (4) | 23 (6) | 0.13 |
| Smoking | 952 (4) | 906 (4) | 23 (4) | 23 (6) | 0.39 |
| Alcohol | 946 (4) | 902 (4) | 30 (5) | 14 (3) | 0.37 |
| Comedications | |||||
| Median (IQR) Number of drugs | 9 (6–13) | 9 (6–13) | 10 (7–13) | 10 (7–15) | <0.0001 |
| Polypharmacy a | 18,865 (85) | 17,932 (84) | 557 (97) | 376 (91) | <0.0001 |
| Total (n = 22,220) | <65 Years Old (n = 9310) | ≥65 Years Old (n = 12,910) | ≥80 Years Old (n = 4286) | |
|---|---|---|---|---|
| Oral AT combinations (n = 4466) | 27.8 (26.8–28.9) | 28.1 (26.7–29.6) | 27.8 (26.3–29.2) | 24.8 (22.8–26.8) |
| Dual antiplatelet therapy (n = 3134) | 18.7 (17.9–19.5) | 22.3 (21.0–23.5) | 16.2 (15.1–17.3) | 13.5 (12.0–15.0) |
| Aspirin–clopidogrel (n = 2141) | 13.7 (12.9–14.4) | 14.2 (13.2–15.3) | 13.4 (12.3–14.5) | 11.9 (10.5–13.5) |
| Aspirin–ticagrelor (n = 754) | 4.5 (4.1–4.9) | 7.2 (6.3–8.1) | 2.7 (2.3–3.0) | 1.7 (1.3–2.3) |
| Aspirin–prasugrel (n = 239) | 1.3 (0.01–1.5) | 2.3 (1.9–2.7) | 0.6 (0.5–0.8) | 0.04 (0.001–0.2) |
| Dual therapy (n = 1075) | 9.1 (8.3–9.9) | 5.9 (5.0–7.0) | 11.3 (10.1–12.6) | 11.1 (9.3–12.9) |
| Aspirin–VKA (n = 409) | 3.4 (2.9–4.1) | 2.5 (1.8–3.3) | 4.1 (3.2–5.1) | 4.3 (3.6–5.2) |
| Aspirin–DOA (n = 587) | 5.4 (4.8–5.9) | 3.0 (2.4–3.7) | 6.9 (6.0–7.9) | 6.5 (5.0–8.4) |
| Clopidogrel–VKA (n = 32) | 0.2 (0.1–0.3) | 0.2 (0.08–0.3) | 0.2 (0.1–0.4) | 0.2 (0.08–0.5) |
| Clopidogrel–DOA (n = 47) | 0.4 (0.3–0.6) | 0.3 (0.2–0.6) | 0.5 (0.3–0.7) | 0.4 (0.2–0.7) |
| Triple therapy (n = 67) | 0.8 (0.5–1.3) | 0.5 (0.2–1.1) | 1.0 (0.6–1.8) | 0.7 (0.4–1.3) |
| Aspirin–clopidogrel–VKA (n = 23) | 0.3 (0.1–0.5) | 0.3 (0.06–1.0) | 0.2 (0.1–0.4) | 0.4 (0.1–0.9) |
| Aspirin–clopidogrel–DOA (n = 44) | 0.6 (0.3–1.0) | 0.2 (0.1–0.4) | 0.8 (0.4–1.7) | 0.4 (0.2–0.7) |
| Appropriate a oral AT combinations (n = 1879) | 11.1 (10.4–11.8) | 14.1 (13.0–15.1) | 9.1 (8.2–10.1) | 7.1 (6.0–8.3) |
| Inappropriate a oral AT combinations (n = 2587) | 18.9 (17.9–19.8) | 16.3 (15.0–17.6) | 20.6 (19.2–22.0) | 19.1 (17.2–21.1) |
| Risk of Major Bleeding $ Variables (Number in the Class) | sHR (95% CI) | p Value |
|---|---|---|
| Oral AT combinations at study entry a (n = 987) | 2.16 (1.01–4.63) | 0.048 |
| Male (n = 11,048) | 1.20 (0.77–1.86) | 0.42 |
| Age at study entry, years | 0.007 | |
| Age b 65–79 (n = 8624) | 1.55 (0.90–2.68) | |
| Age b ≥ 80 (n = 4286) | 2.53 (1.41–4.53) | |
| Chronic kidney disease (n = 818) | 2.83 (1.41–5.70) | 0.003 |
| Chronic hepatic disease (n = 486) | 2.37 (0.95–5.93) | 0.06 |
| Coronary heart disease (n = 3278) | 1.12 (0.65–2.14) | 0.59 |
| Peripheral vascular disease (n = 1512) | 0.87 (0.41–1.85) | 0.72 |
| Non-valvular atrial fibrillation (n = 1935) | 1.45 (0.81–2.59) | 0.21 |
| Valvular heart disease (n = 487) | 1.10 (0.40–3.03) | 0.85 |
| Stroke or arterial embolism (n = 1497) | 1.72 (0.92–3.22) | 0.09 |
| Venous thromboembolism disease (n = 759) | 1.53 (0.66–3.59) | 0.32 |
| Hypertension (n = 12,862) | 0.81 (0.51–1.29) | 0.39 |
| Diabetes (n = 5109) | 0.62 (0.34–1.11) | 0.11 |
| Anemia (n = 1259) | 1.48 (0.70–3.10) | 0.30 |
| History of major bleeding (n = 612) | 1.98 (0.81–4.85) | 0.14 |
| Risk of Death $ Variables (Number in the Class) | HR (95% CI) | p Value |
|---|---|---|
| Oral AT combinations at study entry a (n = 987) | 1.42 (0.65–3.14) | 0.38 |
| Male (n = 11,048) | 1.33 (0.97–1.83) | 0.08 |
| Age at study entry, years | <0.0001 | |
| Age b 65–79 (n = 8624) | 1.64 (0.97–2.77) | |
| Age b ≥ 80 (n = 4286) | 9.25 (5.75–14.89) | |
| Chronic kidney disease (n = 818) | 1.27 (0.72–2.22) | 0.41 |
| Chronic hepatic disease (n = 486) | 2.57 (1.24–5.30) | 0.01 |
| Coronary heart disease (n = 3278) | 0.80 (0.50–1.31) | 0.38 |
| Peripheral vascular disease (n = 1512) | 1.41 (0.88–2.62) | 0.14 |
| Non-valvular atrial fibrillation (n = 1935) | 1.37 (0.92–2.05) | 0.12 |
| Valvular heart disease (n = 487) | 0.80 (0.32–1.98) | 0.62 |
| Stroke or arterial embolism (n = 1497) | 1.27 (0.80–2.02) | 0.31 |
| Venous thromboembolism disease (n = 759) | 2.37 (1.43–3.98) | 0.0009 |
| Hypertension (n = 12,862) | 0.95 (0.68–1.33) | 0.77 |
| Diabetes (n = 5109) | 1.04 (0.72–1.52) | 0.83 |
| Anemia (n = 1259) | 1.58 (0.99–2.53) | 0.05 |
| History of major bleeding (n = 612) | 1.46 (0.73–2.89) | 0.28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zerah, L.; Bonnet-Zamponi, D.; Ajrouche, A.; Collet, J.-P.; De Rycke, Y.; Tubach, F. Inappropriate Use of Oral Antithrombotic Combinations in an Outpatient Setting and Associated Risks: A French Nationwide Cohort Study. J. Clin. Med. 2021, 10, 2367. https://doi.org/10.3390/jcm10112367
Zerah L, Bonnet-Zamponi D, Ajrouche A, Collet J-P, De Rycke Y, Tubach F. Inappropriate Use of Oral Antithrombotic Combinations in an Outpatient Setting and Associated Risks: A French Nationwide Cohort Study. Journal of Clinical Medicine. 2021; 10(11):2367. https://doi.org/10.3390/jcm10112367
Chicago/Turabian StyleZerah, Lorène, Dominique Bonnet-Zamponi, Aya Ajrouche, Jean-Philippe Collet, Yann De Rycke, and Florence Tubach. 2021. "Inappropriate Use of Oral Antithrombotic Combinations in an Outpatient Setting and Associated Risks: A French Nationwide Cohort Study" Journal of Clinical Medicine 10, no. 11: 2367. https://doi.org/10.3390/jcm10112367
APA StyleZerah, L., Bonnet-Zamponi, D., Ajrouche, A., Collet, J.-P., De Rycke, Y., & Tubach, F. (2021). Inappropriate Use of Oral Antithrombotic Combinations in an Outpatient Setting and Associated Risks: A French Nationwide Cohort Study. Journal of Clinical Medicine, 10(11), 2367. https://doi.org/10.3390/jcm10112367