
State-Level Health Disparity Is Associated with Sarcoidosis Mortality


Abstract
1. Introduction
2. Methods
2.1. Data Resources and Study Design
2.2. Statistical Analysis
3. Results
3.1. Sarcoidosis Mortality Rates by State
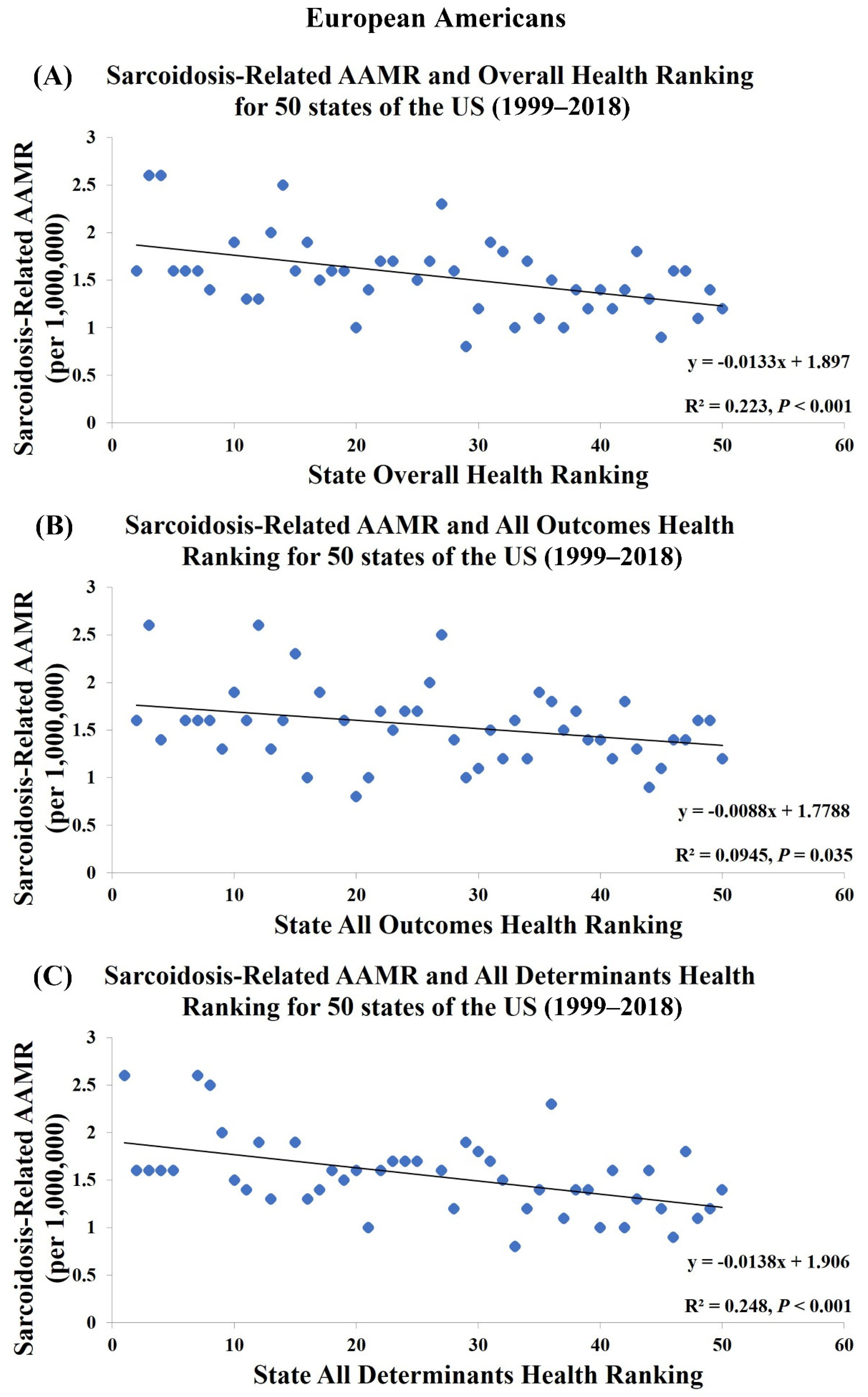
3.2. Association between State Heath Rankings and Sarcoidosis-Related AAMR
3.3. Association between Sarcoidosis Clinics and Sarcoidosis-Related AAMR
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AAMR | Age-Adjusted Mortality Rates |
| AHR | America’s Health Rankings |
| FSR | Foundation for Sarcoidosis Research |
| WASOG | World Association for Sarcoidosis and Other Granulomatous Disorders |
References
- Iannuzzi, M.C.; Fontana, J.R. Sarcoidosis: Clinical presentation, immunopathogenesis, and therapeutics. JAMA 2011, 305, 391–399. [Google Scholar] [CrossRef]
- Cozier, Y.C. Assessing the worldwide epidemiology of sarcoidosis: Challenges and future directions. Eur. Respir. Soc. 2016, 48, 1545–1548. [Google Scholar] [CrossRef] [PubMed]
- Swigris, J.J.; Olson, A.L.; Huie, T.J.; Fernandez-Perez, E.R.; Solomon, J.; Sprunger, D.; Brown, K.K. Sarcoidosis-related mortality in the United States from 1988 to 2007. Am. J. Respir. Crit. Care Med. 2011, 183, 1524–1530. [Google Scholar] [CrossRef] [PubMed]
- Mirsaeidi, M.; Machado, R.F.; Schraufnagel, D.; Sweiss, N.J.; Baughman, R.P. Racial difference in sarcoidosis mortality in the United States. Chest 2015, 147, 438–449. [Google Scholar] [CrossRef] [PubMed]
- Kearney, G.D.; Obi, O.N.; Maddipati, V.; Mohan, A.; Malur, A.; Carter, J.C.; Thomassen, M.J. Sarcoidosis deaths in the United States: 1999–2016. Respir. Med. 2019, 149, 30–35. [Google Scholar] [CrossRef]
- Ogundipe, F.; Mehari, A.; Gillum, R. Disparities in Sarcoidosis Mortality by Region, Urbanization, and Race in the United States: A Multiple Cause of Death Analysis. Am. J. Med. 2019, 132, 1062–1068.e3. [Google Scholar] [CrossRef]
- Baughman, R.P.; Field, S.; Costabel, U.; Crystal, R.G.; Culver, D.A.; Drent, M.; Judson, M.A.; Wolff, G. Sarcoidosis in America. Analysis based on health care use. Ann. Am. Thorac. Soc. 2016, 13, 1244–1252. [Google Scholar] [CrossRef] [PubMed]
- Gerke, A.K.; Judson, M.A.; Cozier, Y.C.; Culver, D.A.; Koth, L.L. Disease burden and variability in sarcoidosis. Ann. Am. Thorac. Soc. 2017, 14 (Suppl. 6), S421–S428. [Google Scholar] [CrossRef]
- Baughman, R.P.; Lower, E.E. Who dies from sarcoidosis and why? Am. Thorac. Soc. 2011, 183. [Google Scholar] [CrossRef]
- Bargagli, E.; Olivieri, C.; Rottoli, P. Cytokine modulators in the treatment of sarcoidosis. Rheumatol. Int. 2011, 31, 1539–1544. [Google Scholar] [CrossRef] [PubMed]
- Baughman, R.; Lower, E.; Drent, M. Inhibitors of tumor necrosis factor (TNF) in sarcoidosis: Who, what, and how to use them. Sarcoidosis Vasc. Diffus. Lung Dis. 2008, 25, 76–89. [Google Scholar]
- Baughman, R.P.; Grutters, J.C. New treatment strategies for pulmonary sarcoidosis: Antimetabolites, biological drugs, and other treatment approaches. Lancet Respir. Med. 2015, 3, 813–822. [Google Scholar] [CrossRef]
- Cremers, J.P.; Drent, M.; Bast, A.; Shigemitsu, H.; Baughman, R.P.; Valeyre, D.; Sweiss, N.J.; Jansen, T.L. Multinational evidence-based World Association of Sarcoidosis and Other Granulomatous Disorders recommendations for the use of methotrexate in sarcoidosis: Integrating systematic literature research and expert opinion of sarcoidologists worldwide. Curr. Opin. Pulm. Med. 2013, 19, 545–561. [Google Scholar] [CrossRef] [PubMed]
- Paramothayan, S.; Lasserson, T.J.; Walters, E.H.; Paramothayan, N.S. Immunosuppressive and cytotoxic therapy for pulmonary sarcoidosis. Cochrane Database Syst. Rev. 2001. [Google Scholar] [CrossRef]
- Schutt, A.C.; Bullington, W.M.; Judson, M.A. Pharmacotherapy for pulmonary sarcoidosis: A Delphi consensus study. Respir. Med. 2010, 104, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Baughman, R.; Lower, E. Fungal infections as a complication of therapy for sarcoidosis. QJM 2005, 98, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Baughman, R.; Nagai, S.; Balter, M.; Costabel, U.; Drent, M.; Du Bois, R.; Grutters, J.; Judson, M.; Lambiri, I.; Lower, E. Defining the clinical outcome status (COS) in sarcoidosis: Results of WASOG Task Force. Sarcoidosis Vasc. Diffus. Lung Dis. 2011, 28, 56–64. [Google Scholar]
- Baughman, R.; Winget, D.; Bowen, E.; Lower, E. Predicting respiratory failure in sarcoidosis patients. Sarcoidosis Vasc. Diffus. Lung Dis. Off. J. WASOG 1997, 14, 154–158. [Google Scholar]
- Baughman, R.P.; Engel, P.J.; Taylor, L.; Lower, E.E. Survival in sarcoidosis-associated pulmonary hypertension: The importance of hemodynamic evaluation. Chest 2010, 138, 1078–1085. [Google Scholar] [CrossRef]
- Gribbin, J.; Hubbard, R.B.; Le Jeune, I.; Smith, C.J.; West, J.; Tata, L.J. Incidence and mortality of idiopathic pulmonary fibrosis and sarcoidosis in the UK. Thorax 2006, 61, 980–985. [Google Scholar] [CrossRef] [PubMed]
- Chappell, A.; Cheung, W.; Hutchings, H. Sarcoidosis: A long-term follow up study. Sarcoidosis Vasc. Diffus. Lung Dis. Off. J. WASOG 2000, 17, 167–173. [Google Scholar]
- Bartter, T.; Irwin, R.S.; Abraham, J.L.; Dascal, A.; Nash, G.; Himmelstein, J.S.; Jederlinic, P.J. Zirconium compound-induced pulmonary fibrosis. Arch. Intern. Med. 1991, 151, 1197–1201. [Google Scholar] [CrossRef]
- Mangiapan, G. Mycobacteria and sarcoidosis: An overview and summary of recent molecular bilological data. Sarcoidosis 1995, 12, 20–37. [Google Scholar]
- Werfel, U.; Schneider, J.; Rodelsperger, K.; Kotter, J.; Popp, W.; Woitowitz, H.; Zieger, G. Sarcoid granulomatosis after zirconium exposure with multiple organ involvement. Eur. Respir. J. 1998, 12, 750. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.-r.; Min, C.; Meng, F.-q.; Wei, J.-y. Pulmonary sarcoid-like granulomatosis induced by aluminum dust: Report of a case and literature review. Chin. Med. J. 2007, 120, 1556–1560. [Google Scholar] [CrossRef] [PubMed]
- Izbicki, G.; Chavko, R.; Banauch, G.I.; Weiden, M.D.; Berger, K.I.; Aldrich, T.K.; Hall, C.; Kelly, K.J.; Prezant, D.J. World Trade Center “sarcoid-like” granulomatous pulmonary disease in New York City Fire Department rescue workers. Chest 2007, 131, 1414–1423. [Google Scholar] [CrossRef] [PubMed]
- Jordan, H.T.; Stellman, S.D.; Prezant, D.; Teirstein, A.; Osahan, S.S.; Cone, J.E. Sarcoidosis diagnosed after September 11, 2001, among adults exposed to the World Trade Center disaster. J. Occup. Environ. Med. 2011, 53, 966–974. [Google Scholar] [CrossRef] [PubMed]
- Newman, L.S.; Rose, C.S.; Bresnitz, E.A.; Rossman, M.D.; Barnard, J.; Frederick, M.; Terrin, M.L.; Weinberger, S.E.; Moller, D.R.; McLennan, G. A case control etiologic study of sarcoidosis: Environmental and occupational risk factors. Am. J. Respir. Crit. Care Med. 2004, 170, 1324–1330. [Google Scholar] [CrossRef] [PubMed]
- Balmes, J.R.; Abraham, J.L.; Dweik, R.A.; Fireman, E.; Fontenot, A.P.; Maier, L.A.; Muller-Quernheim, J.; Ostiguy, G.; Pepper, L.D.; Saltini, C. An official American Thoracic Society statement: Diagnosis and management of beryllium sensitivity and chronic beryllium disease. Am. J. Respir. Crit. Care Med. 2014, 190, e34–e59. [Google Scholar] [CrossRef]
- Rice, J.B.; White, A.; Lopez, A.; Conway, A.; Wagh, A.; Nelson, W.W.; Philbin, M.; Wan, G.J. Economic burden of sarcoidosis in a commercially-insured population in the United States. J. Med. Econ. 2017, 20, 1048–1055. [Google Scholar] [CrossRef]
- Rice, J.B.; White, A.; Lopez, A.; Nelson, W.W. High-cost sarcoidosis patients in the United States: Patient characteristics and patterns of health care resource utilization. J. Manag. Care Spec. Pharm. 2017, 23, 1261–1269. [Google Scholar] [CrossRef]
- Harper, L.J.; Gerke, A.K.; Wang, X.-F.; Ribeiro Neto, M.L.; Baughman, R.P.; Beyer, K.; Drent, M.; Judson, M.A.; Maier, L.A.; Serchuck, L. Income and other contributors to poor outcomes in US patients with sarcoidosis. Am. J. Respir. Crit. Care Med. 2020, 201, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Newman, L.S.; Rose, C.S.; Maier, L.A. Sarcoidosis. N. Engl. J. Med. 1997, 336, 1224–1234. [Google Scholar] [CrossRef]
- Rybicki, B.A.; Major, M.; Popovich, J., Jr.; Maliank, M.J.; lannuzzi, M.C. Racial differences in sarcoidosis incidence: A 5-year study in a health maintenance organization. Am. J. Epidemiol. 1997, 145, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Baughman, R.P.; Lower, E.E.; du Bois, R.M. Sarcoidosis. Lancet 2003, 361, 1111–1118. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| State | 1999–2018 America’s Health Rankings (AHR) | 1999–2018 Age-Adjusted Mortality Rate (AAMR) Per 1,000,000 | FSR-WASOG Sarcoidosis Clinics | ||||
|---|---|---|---|---|---|---|---|
| Overall | All Outcomes | All Determinants | All Population | African Americans | European Americans | ||
| Hawaii | 1 | 1 | 6 | No Data | No Data | No Data | 0 |
| Minnesota | 2 | 2 | 5 | 1.9 | 14.3 | 1.6 | 2 |
| Vermont | 3 | 12 | 1 | 2.7 | No Data | 2.6 | 0 |
| Utah | 4 | 3 | 7 | 2.7 | No Data | 2.6 | 1 |
| New Hampshire | 5 | 6 | 3 | 1.6 | No Data | 1.6 | 0 |
| Massachusetts | 6 | 7 | 2 | 2.1 | 11.1 | 1.6 | 2 |
| Connecticut | 7 | 8 | 4 | 2.7 | 15.4 | 1.6 | 1 |
| Colorado | 8 | 4 | 11 | 1.8 | 13.6 | 1.4 | 1 |
| North Dakota | 9 | 5 | 14 | Unreliable | No Data | Unreliable | 0 |
| Washington | 10 | 10 | 12 | 2.2 | 15.2 | 1.9 | 0 |
| Iowa | 11 | 9 | 16 | 1.6 | 16.6 | 1.3 | 1 |
| Nebraska | 12 | 13 | 13 | 1.6 | No Data | 1.3 | 0 |
| Rhode Island | 13 | 26 | 9 | 2.2 | No Data | 2.0 | 0 |
| Maine | 14 | 27 | 8 | 2.5 | No Data | 2.5 | 0 |
| Idaho | 15 | 11 | 20 | 1.7 | No Data | 1.6 | 0 |
| Wisconsin | 16 | 17 | 15 | 2.8 | 19.6 | 1.9 | 0 |
| New Jersey | 17 | 23 | 10 | 3.5 | 17.4 | 1.5 | 2 |
| Oregon | 18 | 19 | 18 | 1.7 | No Data | 1.6 | 0 |
| South Dakota | 19 | 14 | 22 | 1.6 | No Data | 1.6 | 0 |
| California | 20 | 16 | 21 | 1.6 | 11.7 | 1.0 | 3 |
| Virginia | 21 | 28 | 17 | 4.3 | 17.8 | 1.4 | 3 |
| Kansas | 22 | 25 | 23 | 2.4 | 16.6 | 1.7 | 1 |
| Montana | 23 | 22 | 24 | 1.6 | No Data | 1.7 | 0 |
| Wyoming | 24 | 18 | 26 | 1.9 | No Data | Unreliable | 0 |
| Maryland | 25 | 31 | 19 | 5.8 | 17.5 | 1.5 | 1 |
| New York | 26 | 24 | 25 | 3.4 | 12.9 | 1.7 | 6 |
| Alaska | 27 | 15 | 36 | 2.8 | No Data | 2.3 | 0 |
| Pennsylvania | 28 | 33 | 27 | 3.2 | 19.3 | 1.6 | 3 |
| Arizona | 29 | 20 | 33 | 1.0 | 10.5 | 0.8 | 2 |
| Illinois | 30 | 32 | 28 | 3.1 | 15.4 | 1.2 | 4 |
| Michigan | 31 | 35 | 29 | 4.0 | 18.4 | 1.9 | 3 |
| Delaware | 32 | 36 | 30 | 4.7 | 18.1 | 1.8 | 0 |
| New Mexico | 33 | 21 | 42 | 1.1 | No Data | 1.0 | 0 |
| Ohio | 34 | 38 | 31 | 3.2 | 16.0 | 1.7 | 3 |
| Florida | 35 | 30 | 37 | 2.4 | 11.0 | 1.1 | 3 |
| North Carolina | 36 | 37 | 32 | 5.3 | 20.5 | 1.5 | 3 |
| Texas | 37 | 29 | 40 | 2.1 | 11.1 | 1.0 | 4 |
| Indiana | 38 | 40 | 35 | 2.4 | 15.3 | 1.4 | 0 |
| Missouri | 39 | 41 | 34 | 2.5 | 14.7 | 1.2 | 1 |
| Georgia | 40 | 39 | 38 | 4.7 | 13.7 | 1.4 | 2 |
| Nevada | 41 | 34 | 45 | 1.5 | 7.1 | 1.2 | 0 |
| Kentucky | 42 | 46 | 39 | 2.2 | 12.8 | 1.4 | 0 |
| South Carolina | 43 | 42 | 47 | 6.6 | 20.8 | 1.8 | 1 |
| Tennessee | 44 | 43 | 43 | 3.2 | 14.1 | 1.3 | 2 |
| Oklahoma | 45 | 44 | 46 | 1.9 | 14.3 | 0.9 | 2 |
| West Virginia | 46 | 48 | 41 | 2.1 | 20.2 | 1.6 | 0 |
| Alabama | 47 | 49 | 44 | 5.3 | 17.5 | 1.6 | 1 |
| Arkansas | 48 | 45 | 48 | 2.9 | 13.9 | 1.1 | 0 |
| Louisiana | 49 | 47 | 50 | 4.5 | 12.0 | 1.4 | 2 |
| Mississippi | 50 | 50 | 49 | 5.0 | 12.4 | 1.2 | 0 |
| Geographic Division | 1999–2018 Age-Adjusted Mortality Rate (AAMR) per 1,000,000 | FSR-WASOG Sarcoidosis Clinics | ||
|---|---|---|---|---|
| All Population | African Americans | European Americans | ||
| New England | 2.3 | 12.4 | 1.8 | 3 |
| Middle Atlantic | 3.4 | 15.2 | 1.6 | 11 |
| East North Central | 3.2 | 16.5 | 1.6 | 10 |
| West North Central | 2.1 | 14.3 | 1.4 | 5 |
| South Atlantic | 4.2 | 16.3 | 1.3 | 13 |
| East South Central | 3.7 | 14.6 | 1.4 | 3 |
| West South Central | 2.5 | 11.7 | 1.1 | 8 |
| Mountain | 1.5 | 10.6 | 1.3 | 4 |
| Pacific | 1.6 | 12.1 | 1.2 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.-C.; Chang, K.-Y.; Mirsaeidi, M. State-Level Health Disparity Is Associated with Sarcoidosis Mortality. J. Clin. Med. 2021, 10, 2366. https://doi.org/10.3390/jcm10112366
Lee Y-C, Chang K-Y, Mirsaeidi M. State-Level Health Disparity Is Associated with Sarcoidosis Mortality. Journal of Clinical Medicine. 2021; 10(11):2366. https://doi.org/10.3390/jcm10112366
Chicago/Turabian StyleLee, Yu-Che, Ko-Yun Chang, and Mehdi Mirsaeidi. 2021. "State-Level Health Disparity Is Associated with Sarcoidosis Mortality" Journal of Clinical Medicine 10, no. 11: 2366. https://doi.org/10.3390/jcm10112366
APA StyleLee, Y.-C., Chang, K.-Y., & Mirsaeidi, M. (2021). State-Level Health Disparity Is Associated with Sarcoidosis Mortality. Journal of Clinical Medicine, 10(11), 2366. https://doi.org/10.3390/jcm10112366