
Safety, Efficacy, and Outcomes of N-Butyl Cyanoacrylate Glue Injection through the Endoscopic or Radiologic Route for Variceal Gastrointestinal Bleeding: A Systematic Review and Meta-Analysis

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Definition
2.4. Statistical Analyses
3. Results
3.1. Article Selection and Patient Characteristics
3.2. Types of NBCA Glue and NBCA-Lipiodol® Ratio Used
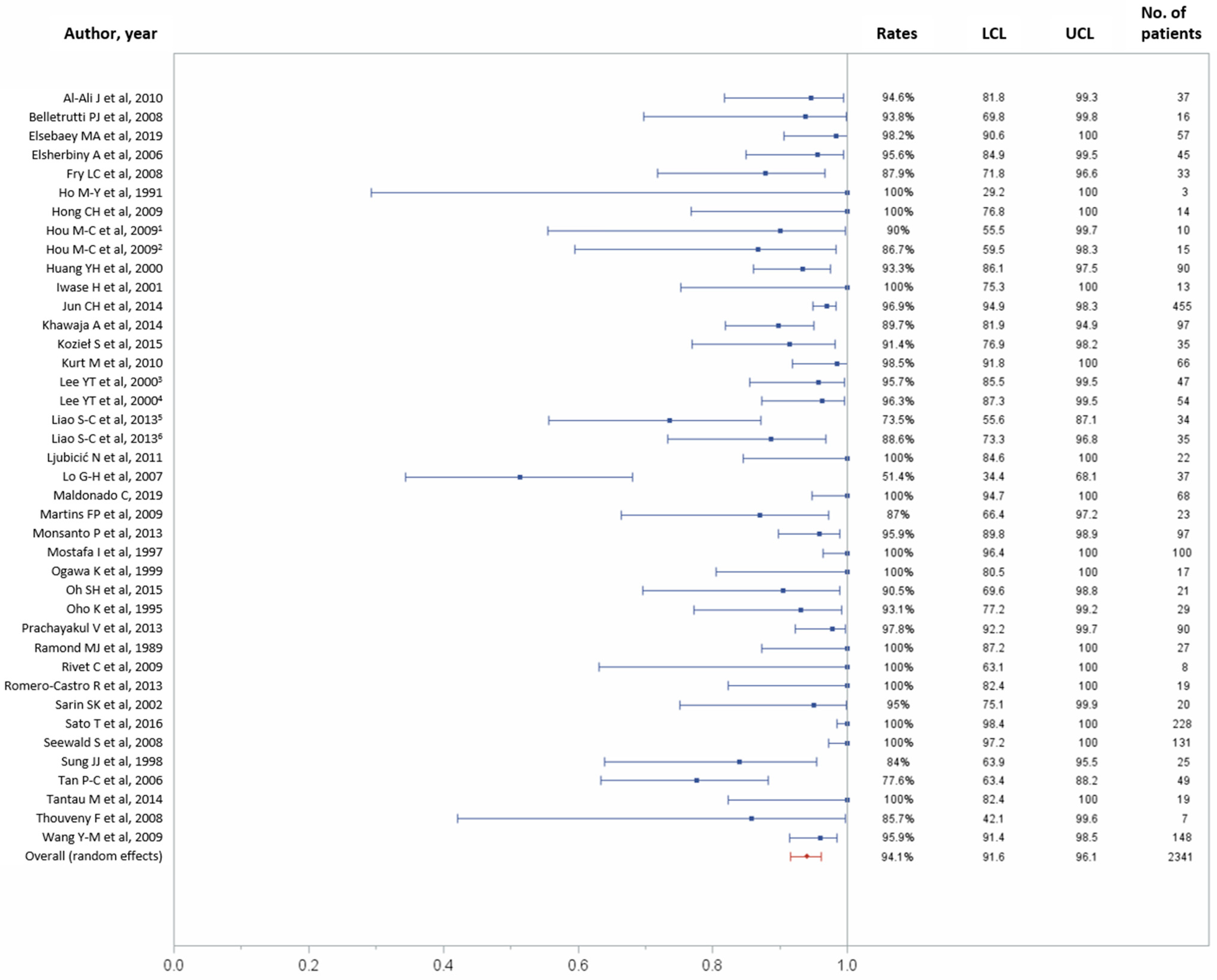
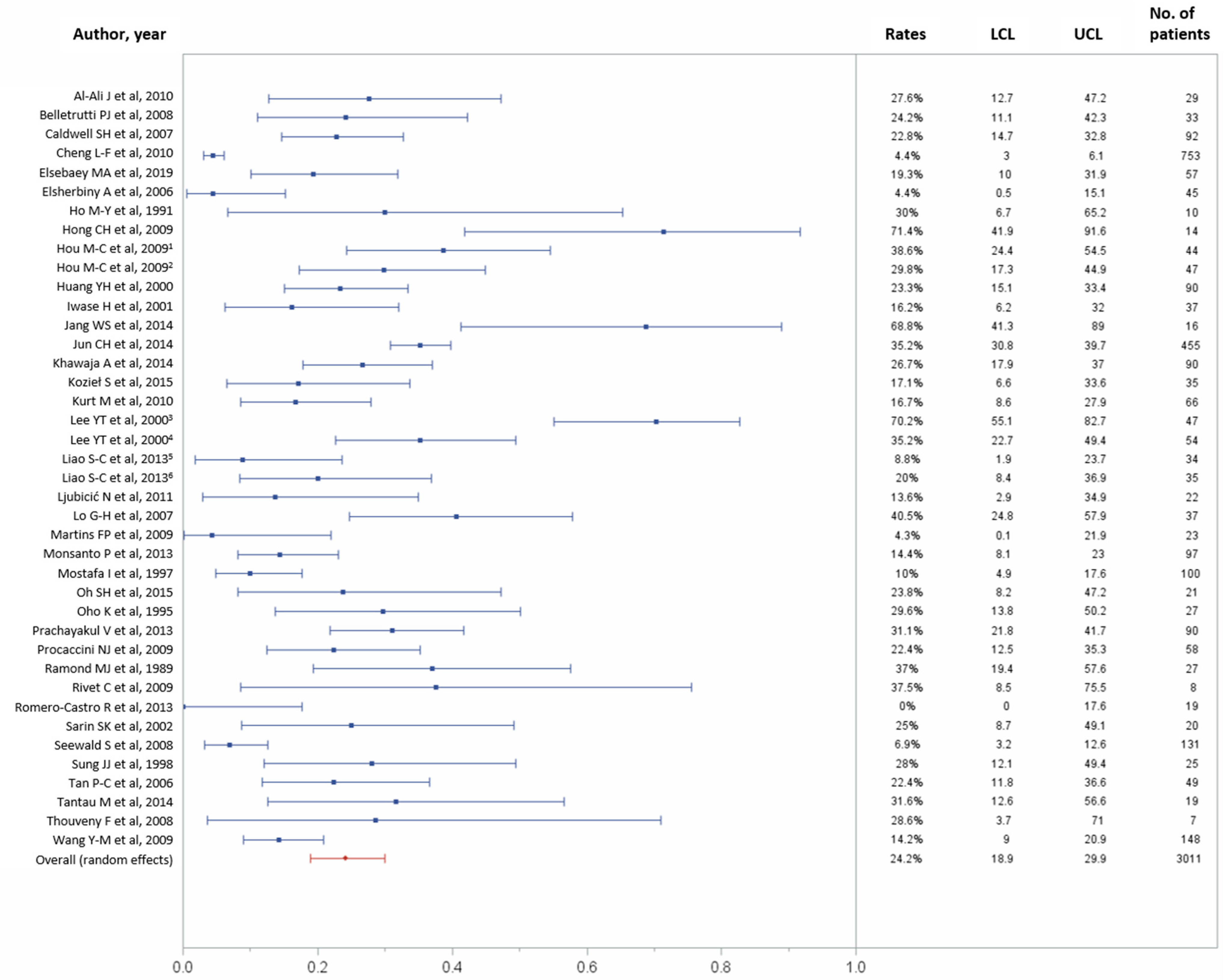
3.3. Technical Success and 30-Day Rebleeding Outcomes
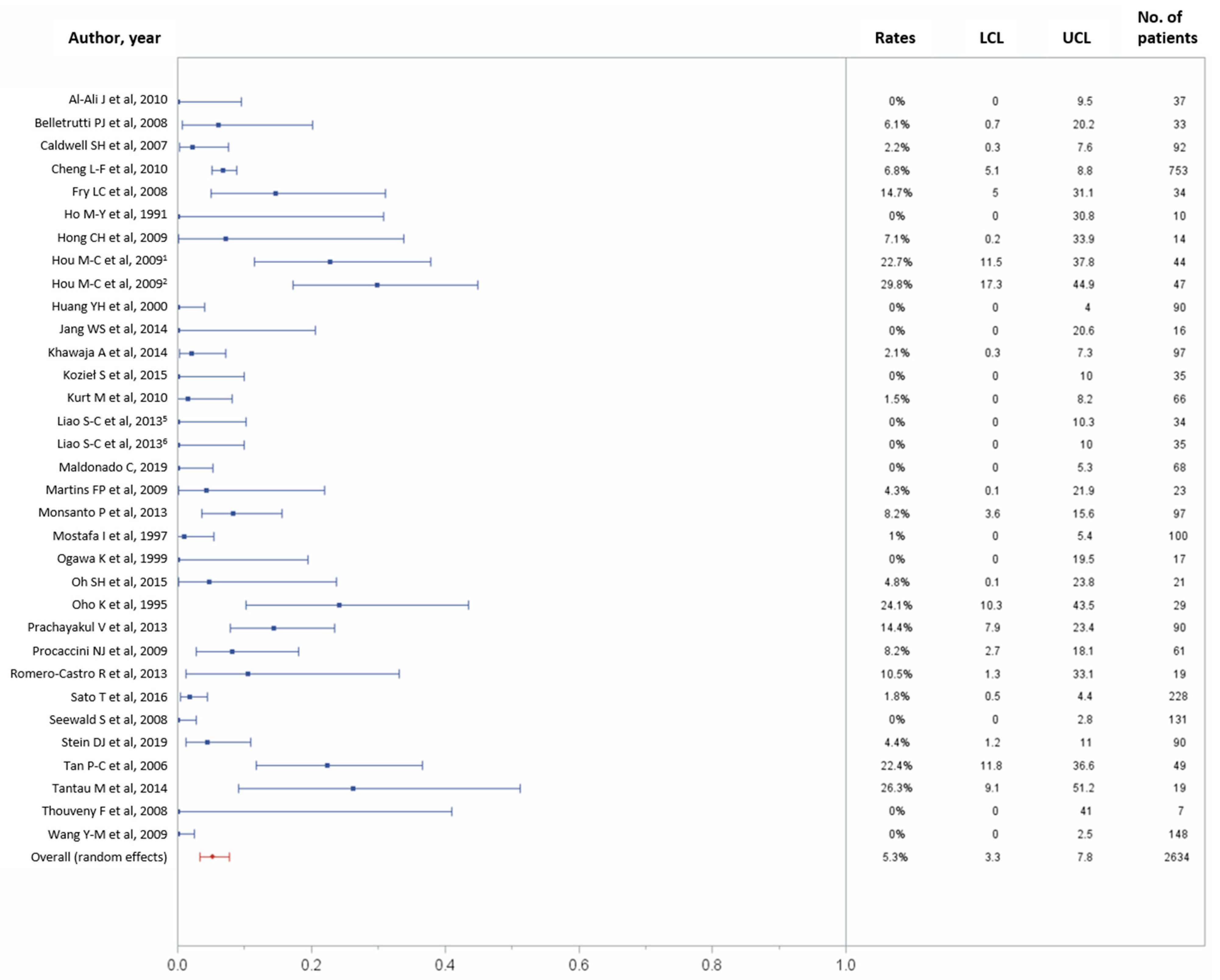
3.4. 30-Day Overall and Major Complication Rates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- de Franchis, R.; Primignani, M. Natural history of portal hypertension in patients with cirrhosis. Clin. Liver Dis. 2001, 5, 645–663. [Google Scholar] [CrossRef]
- Jakab, S.S.; Garcia-Tsao, G. Evaluation and management of esophageal and gastric varices in patients with cirrhosis. Clin. Liver Dis. 2020, 24, 335–350. [Google Scholar] [CrossRef] [PubMed]
- Loffroy, R.; Favelier, S.; Pottecher, P.; Estivalet, L.; Genson, P.Y.; Gehin, S.; Krausé, D.; Cercueil, J.P. Transjugular intrahepatic portosystemic shunt for acute variceal gastrointestinal bleeding: Indications, techniques and outcomes. Diagn. Interv. Imaging 2015, 96, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Vangeli, M.; Patch, D.; Terreni, N.; Tibballs, J.; Watkinson, A.; Davies, N.; Burroughs, A.K. Bleeding ectopic varices--treatment with transjugular intrahepatic porto-systemic shunt (TIPS) and embolisation. J. Hepatol. 2004, 41, 560–566. [Google Scholar] [CrossRef]
- Vidal, V.; Joly, L.; Perreault, P.; Bouchard, L.; Lafortune, M.; Pomier-Layrargues, G. Usefulness of transjugular intrahepatic portosystemic shunt in the management of bleeding ectopic varices in cirrhotic patients. Cardiovasc. Intervent. Radiol. 2006, 29, 216–219. [Google Scholar] [CrossRef]
- Perricone, G.; Vangeli, M.; De Nicola, S.; Airoldi, A.; Belli, L.S. Adding embolization to TIPS implantation: A better therapy to control bleeding from ectopic varices? J. Hepatol. 2017, 67, 200–201. [Google Scholar] [CrossRef]
- Garcia-Tsao, G.; Abraldes, J.G.; Berzigotti, A.; Bosch, J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2017, 65, 310–335. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. European Association for the Study of the Liver EASL clinical practice guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [PubMed]
- de Franchis, R.; on behalf of theBaveno VI Faculty. Revising consensus in portal hypertension: Report of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension. J. Hepatol. 2010, 53, 762–768. [Google Scholar] [CrossRef]
- Stein, D.J.; Salinas, C.; Sabri, S.; Onyeali, R.; Caldwell, S.; Henry, Z. Balloon retrograde transvenous obliteration versus endoscopic cyanoacrylate in bleeding gastric varices: Comparison of rebleeding and mortality with extended follow-up. J. Vasc. Interv. Radiol. 2019, 30, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Elsebaey, M.A.; Tawfik, M.A.; Ezzat, S.; Selim, A.; Elashry, H.; Abd-Elsalam, S. Endoscopic injection sclerotherapy versus N-Butyl-2 Cyanoacrylate injection in the management of actively bleeding esophageal varices: A randomized controlled trial. BMC Gastroenterol. 2019, 19, 23. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Tsao, G.; Sanyal, A.J.; Grace, N.D.; Carey, W.D.; Practice guidelines committee of American Association for Study of Liver Diseases; Practice parameters committee of American College of Gastroenterology. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Am. J. Gastroenterol. 2007, 102, 2086–2102. [Google Scholar] [CrossRef] [PubMed]
- Ríos Castellanos, E.; Seron, P.; Gisbert, J.P.; Cosp, X.B. Endoscopic injection of cyanoacrylate glue versus other endoscopic procedures for acute bleeding gastric varices in people with portal hypertension. Cochrane Database Syst. Rev. 2015, CD010180. [Google Scholar] [CrossRef] [PubMed]
- Norton, I.D.; Andrews, J.C.; Kamath, P.S. Management of ectopic varices. Hepatology 1998, 28, 1154–1158. [Google Scholar] [CrossRef] [PubMed]
- Henry, Z.; Uppal, D.; Saad, W.; Caldwell, S. Gastric and ectopic varices. Clin. Liver Dis. 2014, 18, 371–388. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Sarin, S.K.; Lahoti, D.; Saxena, S.P.; Murthy, N.S.; Makwana, U.K. Prevalence, classification and natural history of gastric varices: A long-term follow-up study in 568 portal hypertension patients. Hepatology 1992, 16, 1343–1349. [Google Scholar] [CrossRef]
- Sacks, D.; McClenny, T.E.; Cardella, J.F.; Lewis, C.A. Society of Interventional Radiology clinical practice guidelines. J. Vasc. Interv. Radiol. 2003, 14, S199–S202. [Google Scholar] [CrossRef]
- de Franchis, R.; on behalf of theBaveno VI Faculty. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J. Hepatol. 2015, 63, 743–752. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Al-Ali, J.; Pawlowska, M.; Coss, A.; Svarta, S.; Byrne, M.; Enns, R. Endoscopic management of gastric variceal bleeding with cyanoacrylate glue injection: Safety and efficacy in a Canadian population. Can. J. Gastroenterol. 2010, 24, 593–596. [Google Scholar] [CrossRef]
- Belletrutti, P.J.; Romagnuolo, J.; Hilsden, R.J.; Chen, F.; Kaplan, B.; Love, J.; Beck, P.L. Endoscopic management of gastric varices: Efficacy and outcomes of gluing with N-Butyl-2-Cyanoacrylate in a North American patient population. Can. J. Gastroenterol. 2008, 22, 931–936. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, S.H.; Hespenheide, E.E.; Greenwald, B.D.; Northup, P.G.; Patrie, J.T. Enbucrilate for gastric varices: Extended experience in 92 patients. Aliment. Pharmacol. Ther. 2007, 26, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.F.; Wang, Z.Q.; Li, C.Z.; Lin, W.; Yeo, A.E.; Jin, B. Low incidence of complications from endoscopic gastric variceal obturation with butyl cyanoacrylate. Clin. Gastroenterol. Hepatol. 2010, 8, 760–766. [Google Scholar] [CrossRef]
- Elsherbiny, A.; Assal, H.S.; Elmabood, M.A.; Hussein, E.A.A. Gastro-esophageal varices: Endoscopic band ligation, alcohol injection and cyanoacrylate injection. J. Med. Sci. 2006, 6, 164–168. [Google Scholar] [CrossRef][Green Version]
- Fry, L.C.; Neumann, H.; Olano, C.; Malfertheiner, P.; Mönkemüller, K. Efficacy, complications and clinical outcomes of endoscopic sclerotherapy with N-Butyl-2-Cyanoacrylate for bleeding gastric varices. Dig. Dis. 2008, 26, 300–303. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.Y.; Wang, T.H.; Lee, W.H.; Wong, J.M. Clinical experience in endoscopic obturation of gastric varices with Histoacryl. Chinese J. Gastroenterol. 1991, 8, 249–253. [Google Scholar] [CrossRef]
- Hong, C.H.; Kim, H.J.; Park, J.H.; Park, D.I.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; Hong, H.P.; Shin, J.H. Treatment of patients with gastric variceal hemorrhage: Endoscopic N-Butyl-2-Cyanoacrylate injection versus balloon-occluded retrograde transvenous obliteration. J. Gastroenterol. Hepatol. 2009, 24, 372–378. [Google Scholar] [CrossRef]
- Hou, M.C.; Lin, H.C.; Lee, H.S.; Liao, W.C.; Lee, F.Y.; Lee, S.D. A randomized trial of endoscopic cyanoacrylate injection for acute gastric variceal bleeding: 0.5 mL versus 1.0 mL. Gastrointest. Endosc. 2009, 70, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.H.; Yeh, H.Z.; Chen, G.H.; Chang, C.S.; Wu, C.Y.; Poon, S.K.; Lien, H.C.; Yang, S.S. Endoscopic treatment of bleeding gastric varices by N-Butyl-2-Cyanoacrylate (Histoacryl) injection: Long-term efficacy and safety. Gastrointest. Endosc. 2000, 52, 160–167. [Google Scholar] [CrossRef]
- Iwase, H.; Maeda, O.; Shimada, M.; Tsuzuki, T.; Peek, R.M.; Nishio, Y.; Ando, T.; Ina, K.; Kusugami, K. Endoscopic ablation with cyanoacrylate glue for isolated gastric variceal bleeding. Gastrointest. Endosc. 2001, 53, 585–592. [Google Scholar] [CrossRef]
- Jang, W.S.; Shin, H.P.; Lee, J.I.; Joo, K.R.; Cha, J.M.; Jeon, J.W.; Lim, J.U. Proton pump inhibitor administration delays rebleeding after endoscopic gastric variceal obturation. World J. Gastroenterol. 2014, 20, 17127–17131. [Google Scholar] [CrossRef] [PubMed]
- Jun, C.H.; Kim, K.R.; Yoon, J.H.; Koh, H.R.; Choi, W.S.; Cho, K.M.; Lim, S.U.; Park, C.H.; Joo, Y.E.; Kim, H.S.; et al. Clinical outcomes of gastric variceal obliteration using N-Butyl-2-Cyanoacrylate in patients with acute gastric variceal hemorrhage. Korean J. Intern. Med. 2014, 29, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Khawaja, A.; Sonawalla, A.A.; Somani, S.F.; Abid, S. Management of bleeding gastric varices: A single session of Histoacryl injection may be sufficient. Eur. J. Gastroenterol. Hepatol. 2014, 26, 661–667. [Google Scholar] [CrossRef]
- Kozieł, S.; Kobryń, K.; Paluszkiewicz, R.; Krawczyk, M.; Wróblewski, T. Endoscopic treatment of gastric varices bleeding with the use of N-Butyl-2 Cyanoacrylate. Prz. Gastroenterol. 2015, 10, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Kurt, M.; Akdogan, M.; Sayilir, A.; Kuran, S.; Ozderin, Y.O.; Arhan, M.; Onal, I.K.; Kekilli, M.; Beyazit, Y.; Hayran, M. Effect of endoscopic injection therapy with combined cyanoacrylate and lipiodol for bleeding gastric varices: A single center experience. J. Dig. Dis. 2010, 11, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.T.; Chan, F.K.; Ng, E.K.; Leung, V.K.; Law, K.B.; Yung, M.Y.; Chung, S.C.; Sung, J.J. EUS-guided injection of cyanoacrylate for bleeding gastric varices. Gastrointest. Endosc. 2000, 52, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Liao, S.C.; Yang, S.S.; Ko, C.W.; Lien, H.C.; Tung, C.F.; Peng, Y.C.; Yeh, H.Z.; Chang, C.S. A miniature ultrasound probe is useful in reducing rebleeding after endoscopic cyanoacrylate injection for hemorrhagic gastric varices. Scand. J. Gastroenterol. 2013, 48, 1347–1353. [Google Scholar] [CrossRef] [PubMed]
- Ljubicić, N.; Bisćanin, A.; Nikolić, M.; Supanc, V.; Hrabar, D.; Pavić, T.; Boban, M. A randomized-controlled trial of endoscopic treatment of acute esophageal variceal hemorrhage: N-Butyl-2-Cyanoacrylate injection vs. variceal ligation. Hepatogastroenterology 2011, 58, 438–443. [Google Scholar]
- Lo, G.H.; Liang, H.L.; Chen, W.C.; Chen, M.H.; Lai, K.H.; Hsu, P.I.; Lin, C.K.; Chan, H.H.; Pan, H.B. A prospective, randomized controlled trial of transjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in the prevention of gastric variceal rebleeding. Endoscopy 2007, 39, 679–685. [Google Scholar] [CrossRef]
- Lôbo, M.R.A.; Chaves, D.M.; DE Moura, D.T.H.; Ribeiro, I.B.; Ikari, E.; DE Moura, E.G.H. Safety and efficacy of EUS-guided coil plus cyanoacrylate versus conventional cyanoacrylate technique in the treatment of gastric varices: A randomized controlled trial. Arq. Gastroenterol. 2019, 56, 99–105. [Google Scholar] [CrossRef]
- Maldonado, C.; Jimenez, F.; Sepulveda, M.; Garcia, J.; Herrera, D.; Castro, A.; Aguirre, M.; Rojas, C.; Rodriguez, F. Sclerosis of fundic varices. Experience in a reference center in the south west of Colombia. 2011–2017. J. Gastroenterol. Hepatol. Res. 2019, 8, 2980–2983. [Google Scholar] [CrossRef]
- Martins, F.P.; Macedo, E.P.; Paulo, G.A.; Nakao, F.S.; Ardengh, J.C.; Ferrari, A.P. Endoscopic follow-up of cyanoacrylate obliteration of gastric varices. Arq. Gastroenterol. 2009, 46, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Monsanto, P.; Almeida, N.; Rosa, A.; Maçôas, F.; Lérias, C.; Portela, F.; Amaro, P.; Ferreira, M.; Gouveia, H.; Sofia, C. Endoscopic treatment of bleeding gastric varices with Histoacryl (N-Butyl-2-Cyanoacrylate): A south european single center experience. Indian J. Gastroenterol. 2013, 32, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, I.; Omar, M.M.; Nouh, A. Endoscopic control of gastric variceal bleeding with butyl cyanoacrylate in patients with schistosomiasis. J. Egypt. Soc. Parasitol. 1997, 27, 405–410. [Google Scholar]
- Ogawa, K.; Ishikawa, S.; Naritaka, Y.; Shimakawa, T.; Wagatsuma, Y.; Katsube, A.; Kajiwara, T. Clinical evaluation of endoscopic injection sclerotherapy using N-Butyl-2-Cyanoacrylate for gastric variceal bleeding. J. Gastroenterol. Hepatol. 1999, 14, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.H.; Kim, S.J.; Rhee, K.W.; Kim, K.M. Endoscopic cyanoacrylate injection for the treatment of gastric varices in children. World J. Gastroenterol. 2015, 21, 2719–2724. [Google Scholar] [CrossRef]
- Oho, K.; Iwao, T.; Sumino, M.; Toyonaga, A.; Tanikawa, K. Ethanolamine oleate versus butyl cyanoacrylate for bleeding gastric varices: A nonrandomized study. Endoscopy 1995, 27, 349–354. [Google Scholar] [CrossRef]
- Prachayakul, V.; Aswakul, P.; Chantarojanasiri, T.; Leelakusolvong, S. Factors influencing clinical outcomes of Histoacryl® glue injection-treated gastric variceal hemorrhage. World J. Gastroenterol. 2013, 19, 2379–2387. [Google Scholar] [CrossRef]
- Procaccini, N.J.; Al-Osaimi, A.M.; Northup, P.; Argo, C.; Caldwell, S.H. Endoscopic cyanoacrylate versus transjugular intrahepatic portosystemic shunt for gastric variceal bleeding: A single-center U.S. analysis. Gastrointest. Endosc. 2009, 70, 881–887. [Google Scholar] [CrossRef]
- Ramond, M.J.; Valla, D.; Mosnier, J.F.; Degott, C.; Bernuau, J.; Rueff, B.; Benhamou, J.P. Successful endoscopic obturation of gastric varices with butyl cyanoacrylate. Hepatology 1989, 10, 488–493. [Google Scholar] [CrossRef]
- Rivet, C.; Robles-Medranda, C.; Dumortier, J.; Le Gall, C.; Ponchon, T.; Lachaux, A. Endoscopic treatment of gastroesophageal varices in young infants with cyanoacrylate glue: A pilot study. Gastrointest. Endosc. 2009, 69, 1034–1038. [Google Scholar] [CrossRef] [PubMed]
- Romero-Castro, R.; Ellrichmann, M.; Ortiz-Moyano, C.; Subtil-Inigo, J.C.; Junquera-Florez, F.; Gornals, J.B.; Repiso-Ortega, A.; Vila-Costas, J.; Marcos-Sanchez, F.; Muñoz-Navas, M.; et al. EUS-guided coil versus cyanoacrylate therapy for the treatment of gastric varices: A multicenter study (with videos). Gastrointest. Endosc. 2013, 78, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Sarin, S.K.; Jain, A.K.; Jain, M.; Gupta, R. A randomized controlled trial of cyanoacrylate versus alcohol injection in patients with isolated fundic varices. Am. J. Gastroenterol. 2002, 97, 1010–1015. [Google Scholar] [CrossRef] [PubMed]
- Sato, T. Endoscopic obliterative therapy with n-butyl-2-cyanoacrylate for gastrointestinal varices. Gastroenterol. Hepatol. Endosc. 2016, 1, 92–96. [Google Scholar] [CrossRef]
- Seewald, S.; Ang, T.L.; Imazu, H.; Naga, M.; Omar, S.; Groth, S.; Seitz, U.; Zhong, Y.; Thonke, F.; Soehendra, N. A standardized injection technique and regimen ensures success and safety of N-butyl-2-cyanoacrylate injection for the treatment of gastric fundal varices (with videos). Gastrointest. Endosc. 2008, 68, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.J.; Yeo, W.; Suen, R.; Lee, Y.T.; Chung, S.C.; Chan, F.K.; Johnson, P.J. Injection sclerotherapy for variceal bleeding in patients with hepatocellular carcinoma: Cyanoacrylate versus sodium tetradecyl sulphate. Gastrointest. Endosc. 1998, 47, 235–239. [Google Scholar] [CrossRef]
- Tan, P.C.; Hou, M.C.; Lin, H.C.; Liu, T.T.; Lee, F.Y.; Chang, F.Y.; Lee, S.D. A randomized trial of endoscopic treatment of acute gastric variceal hemorrhage: N-Butyl-2-Cyanoacrylate injection versus band ligation. Hepatology 2006, 43, 690–697. [Google Scholar] [CrossRef]
- Tantau, M.; Crisan, D.; Popa, D.; Vesa, S.; Tantau, A. band ligation vs. N-Butyl-2-Cyanoacrylate injection in acute gastric variceal bleeding: A prospective follow-up study. Ann. Hepatol. 2013, 13, 75–83. [Google Scholar] [CrossRef]
- Thouveny, F.; Aubé, C.; Konaté, A.; Lebigot, J.; Bouvier, A.; Oberti, F. Direct percutaneous approach for endoluminal glue embolization of stomal varices. J. Vasc. Interv. Radiol. 2008, 19, 774–777. [Google Scholar] [CrossRef]
- Wang, Y.M.; Cheng, L.F.; Li, N.; Wu, K.; Zhai, J.S.; Wang, Y.W. Study of glue extrusion after endoscopic N-Butyl-2-cyanoacrylate injection on gastric variceal bleeding. World J. Gastroenterol. 2009, 15, 4945–4951. [Google Scholar] [CrossRef]
- Onofrio, F.Q.; Pereira-Lima, J.C.; Valença, F.M.; Azeredo-da-Silva, A.L.F.; Tetelbom Stein, A. Efficacy of endoscopic treatments for acute esophageal variceal bleeding in cirrhotic patients: Systematic review and meta-analysis. Endosc. Int. Open 2019, 7, E1503–E1514. [Google Scholar] [CrossRef] [PubMed]
- Loffroy, R. Transjugular Intrahepatic Portosystemic Shunt (TIPS): A major step forward for patients but a growing job for interventional radiologists! Diagn. Interv. Imaging 2016, 97, 1069–1070. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Freedman, A.M.; Luketic, V.A.; Purdum, P.P.; Shiffman, M.L.; Tisnado, J.; Cole, P.E. Transjugular intrahepatic portosystemic shunts for patients with active variceal hemorrhage unresponsive to sclerotherapy. Gastroenterology 1996, 111, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, D.; Castaing, D.; Majno, P.; Saliba, F.; Ichaï, P.; Smail, A.; Delvart, V.; Danaoui, M.; Samuel, D.; Bismuth, H. Salvage transjugular intrahepatic portosystemic shunt for uncontrolled variceal bleeding in patients with decompensated cirrhosis. J. Hepatol. 2001, 35, 590–597. [Google Scholar] [CrossRef]
- D’Amico, G.; Luca, A. TIPS Is a cost effective alternative to surgical shunt as a rescue therapy for prevention of recurrent bleeding from esophageal varices. J. Hepatol. 2008, 48, 387–390. [Google Scholar] [CrossRef] [PubMed]
- Vangeli, M.; Patch, D.; Burroughs, A.K. Salvage tips for uncontrolled variceal bleeding. J. Hepatol. 2002, 37, 703–704. [Google Scholar] [CrossRef]
- García-Pagán, J.C.; Caca, K.; Bureau, C.; Laleman, W.; Appenrodt, B.; Luca, A.; Abraldes, J.G.; Nevens, F.; Vinel, J.P.; Mössner, J.; et al. Early TIPS (Transjugular Intrahepatic Portosystemic Shunt) Cooperative Study Group. Early use of TIPS in patients with cirrhosis and variceal bleeding. N. Engl. J. Med. 2010, 362, 2370–2379. [Google Scholar] [CrossRef]
- Nicoară-Farcău, O.; Han, G.; Rudler, M.; Angrisani, D.; Monescillo, A.; Torres, F.; Casanovas, G.; Bosch, J.; Lv, Y.; Thabut, D.; et al. Effects of early placement of transjugular portosystemic shunts in patients with high-risk acute variceal bleeding: A meta-analysis of individual patient data. Gastroenterology 2021, 160, 193–205. [Google Scholar] [CrossRef]
- Tesdal, I.K.; Filser, T.; Weiss, C.; Holm, E.; Dueber, C.; Jaschke, W. Transjugular intrahepatic portosystemic shunts: Adjunctive embolotherapy of gastroesophageal collateral vessels in the prevention of variceal rebleeding. Radiology 2005, 236, 360–367. [Google Scholar] [CrossRef]
- Yu, J.; Wang, X.; Jiang, M.; Ma, H.; Zhou, Z.; Yang, L.; Li, X. Comparison of transjugular intrahepatic portosystemic shunt (TIPS) alone and combined with embolisation for the management of cardiofundal varices: A retrospective study. Eur. Radiol. 2019, 29, 699–706. [Google Scholar] [CrossRef]
- Shi, Y.; Tian, X.; Hu, J.; Zhang, J.; Zhang, C.; Yang, Y.; Qin, C. Efficacy of transjugular intrahepatic portosystemic shunt with adjunctive embolotherapy with cyanoacrylate for esophageal variceal bleeding. Dig. Dis. Sci. 2014, 59, 2325–2332. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Liu, L.; Bai, M.; Chen, H.; Wang, J.; Yang, Z.; Han, G.; Fan, D. Transjugular intrahepatic portosystemic shunt in combination with or without variceal embolization for the prevention of variceal rebleeding: A meta-analysis. J. Gastroenterol. Hepatol. 2014, 29, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Li, X.; Wei, B.; Tong, H.; Zhang, M.G.; Huang, Z.Y.; Cao, J.W.; Tang, C.W. Recurrent variceal bleeding and shunt patency: Prospective randomized controlled trial of transjugular intrahepatic portosystemic shunt alone or combined with coronary vein embolization. Radiology 2013, 268, 900–906. [Google Scholar] [CrossRef] [PubMed]
- Moulin, B.; Chevallier, O.; Abdulmalak, G.; Luu, M.; Latournerie, M.; Minello, A.; Gehin, S.; Cercueil, J.-P.; Midulla, M.; Loffroy, R. Persistence of gastric or esophageal varices on final angiography increases transjugular intrahepatic portosystemic shunt revision rate after polytetrafluoroethylene-covered stent shunt creation. Quant. Imaging Med. Surg. 2018, 8, 174–181. [Google Scholar] [CrossRef]
- Venturini, M.; Augello, L.; Lanza, C.; Curti, M.; Coppola, A.; Piacentino, F.; De Cobelli, F. Emergency tips recanalisation and gastroesophageal varices embolisation with an ethylene vinyl alcohol copolymer agent (Squid) and detachable coils. Eur. Radiol. Exp. 2020, 4, 67. [Google Scholar] [CrossRef]
- Lakhoo, J.; Bui, J.T.; Lokken, R.P.; Ray, C.E.; Gaba, R.C. Transjugular intrahepatic portosystemic shunt creation and variceal coil or plug embolization ineffectively attain gastric variceal decompression or occlusion: Results of a 26-patient retrospective study. J. Vasc. Interv. Radiol. 2016, 27, 1001–1011. [Google Scholar] [CrossRef]
- Choi, J.W.; Kim, H.C.; Jae, H.J.; Jung, H.S.; Hur, S.; Lee, M.; Chung, J.W. Transcatheter embolotherapy with n-butyl cyanoacrylate for ectopic varices. Cardiovasc. Intervent. Radiol. 2015, 38, 344–351. [Google Scholar] [CrossRef]
- Fukuda, T.; Hirota, S.; Sugimura, K. Long-term results of balloon-occluded retrograde transvenous obliteration for the treatment of gastric varices and hepatic encephalopathy. J. Vasc. Interv. Radiol. 2001, 12, 327–336. [Google Scholar] [CrossRef]
- Luo, X.; Xiang, T.; Wu, J.; Wang, X.; Zhu, Y.; Xi, X.; Yan, Y.; Yang, J.; García-Pagán, J.C.; Yang, L. Endoscopic cyanoacrylate injection vs BRTO for prevention of gastric variceal bleeding: A randomized controlled trial. Hepatology 2021, 14. [Google Scholar] [CrossRef]
- Kim, S.K.; Lee, K.A.; Sauk, S.; Korenblat, K. Comparison of transjugular intrahepatic portosystemic shunt with covered stent and balloon-occluded retrograde transvenous obliteration in managing isolated gastric varices. Korean J. Radiol. 2017, 18, 345–354. [Google Scholar] [CrossRef]
- Gimm, G.; Chang, Y.; Kim, H.C.; Shin, A.; Cho, E.J.; Lee, J.H.; Yu, S.J.; Yoon, J.H.; Kim, Y.J. Balloon-occluded retrograde transvenous obliteration versus transjugular intrahepatic portosystemic shunt for the management of gastric variceal bleeding. Gut Liver 2018, 12, 704–713. [Google Scholar] [CrossRef] [PubMed]
- Sabri, S.S.; Abi-Jaoudeh, N.; Swee, W.; Saad, W.E.; Turba, U.C.; Caldwell, S.H.; Angle, J.F.; Matsumoto, A.H. Short-term rebleeding rates for isolated gastric varices managed by transjugular intrahepatic portosystemic shunt versus balloon-occluded retrograde transvenous obliteration. J. Vasc. Interv. Radiol. 2014, 25, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Kim, S.U.; Kim, M.D.; Kim, Y.H.; Kim, G.M.; Park, S.I.; Won, J.Y.; Lee, D.Y.; Lee, K.H. Comparison of treatment outcomes between balloon-occluded retrograde transvenous obliteration and transjugular intrahepatic portosystemic shunt for gastric variceal bleeding hemostasis. J. Gastroenterol. Hepatol. 2017, 32, 1487–1494. [Google Scholar] [CrossRef] [PubMed]
- Tsuruya, K.; Koizumi, J.; Sekiguchi, T.; Hara, T.; Sekiguchi, Y.; Anzai, K.; Arase, Y.; Hirose, S.; Kagawa, T. Successful balloon-occluded retrograde transvenous obliteration for gastric varices using foam sclerosant followed by glue embolization of gastrorenal shunt via the brachial vein approach in a severely obese patient. Ann. Vasc. Dis. 2019, 12, 562–565. [Google Scholar] [CrossRef]
- Chu, H.H.; Kim, H.C.; Jae, H.J.; Yi, N.J.; Lee, K.W.; Suh, K.S.; Chung, J.W.; Park, J.H. Percutaneous transsplenic access to the portal vein for management of vascular complication in patients with chronic liver disease. Cardiovasc. Intervent. Radiol. 2012, 35, 1388–1395. [Google Scholar] [CrossRef] [PubMed]
- Favard, N.; Moulin, M.; Fauque, P.; Bertaut, A.; Favelier, S.; Estivalet, L.; Michel, F.; Cormier, L.; Sagot, P.; Loffroy, R. Comparison of three different embolic materials for varicocele embolization: Retrospective study of tolerance, radiation and recurrence rate. Quant. Imaging Med. Surg. 2015, 5, 806–814. [Google Scholar] [CrossRef]
- Loffroy, R.; Favelier, S.; Pottecher, P.; Estivalet, L.; Genson, P.Y.; Gehin, S.; Cercueil, J.P.; Krausé, D. Transcatheter arterial embolization for acute nonvariceal upper gastrointestinal bleeding: Indications, techniques and outcomes. Diagn. Interv. Imaging 2015, 96, 731–744. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Type | Study Period | Country | No. of Patients * | Gender * (Male, %) | Mean Age * (Years) | GIB Site | Sarin Classification of GV (%) | Type of Glue | NBCA-Lipiodol® Ratio | Use of Vasoactive Drugs ** | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Al-Ali J et al., 2010 [21] | R | 2001–2006 | Canada | 37 | 59.5 | 60 | GV | NS | Histoacryl® | 1:1 | For 1 patient |
| Belletrutti PJ et al., 2008 [22] | R | 2001–2006 | Canada | 34 | 55.9 | 54.5 | GV | GOV1 (70.2), GOV2 (6.4), IGV1 (23.4) | Histoacryl® | 1:1 | NS |
| Caldwell SH et al., 2007 [23] | P | NS | USA | 92 | 71.7 | 55 | GV | GOV1 (14.1), GOV2 (53.3), IGV1 (29.3), IGV2 (3.3) | Histoacryl® | 1:1 | Yes |
| Cheng LF et al., 2010 [24] | R | 1996–2006, 2003–2007 | China | 753 | 72.6 | 51 | GV | GOV1 (36.4), GOV2 (25.2), GOV1–2 (19.4), IGV1 (19.0) | Histoacryl® | 1:1 | NS |
| Elsebaey MA et al., 2019 [11] | RCT | 2016–2017 | Egypt | 57 | 68.4 | 55 | EV | NBCA (GluStitch®) | 1:1.6 | Yes | |
| Elsherbiny A et al., 2006 [25] | PC | 2004 | Egypt | 45 | 64.4 | 57.6 | GV | GOV1 (NS) GOV2 (NS) | Histoacryl® | 1:1.4 | NS |
| Fry LC et al., 2008 [26] | R | 5-years period | Germany | 33 | 48.5 | 54 | GV | GOV1 (20), GOV2 (80) | Histoacryl® | 1:1.6 | Yes |
| Ho MY et al., 1991 [27] | PC | 1990–1991 | China | 10 | 80.0 | 60 | GV and combined GV + EV | NS | Histoacryl® | 1:1 | NS |
| Hong CH et al., 2009 [28] | PC | 2005–2007 | Korea | 14 | 85.7 | 55.4 | GV | GOV2 (64.3), GOV1 + GOV 2 (14.3), IGV1 (21.4) | Histoacryl® | 1:1.6 | Yes |
| Hou MC et al., 2009 [29] 1 | RCT | 2005–2007 | Taiwan | 47 | 72.3 | 59.19 | GV | GOV1 (46.8), GOV2 (34.0), IGV1 (19.2) | Histoacryl® | 1:1.8 | Yes |
| Hou MC et al., 2009 [29] 2 | 44 | 86.4 | 59.89 | GV | GOV1 (36.4), GOV2 (27.3), IGV1 (36.4) | Histoacryl® | 1:1.6 | Yes | |||
| Huang YH et al., 2000 [30] | P | 1992–1998 | Taiwan | 90 | 77.8 | 58 | GV | NS | Histoacryl® | 1:1 | NS |
| Iwase H et al., 2001 [31] | P | 1992–1999 | USA and Japan | 37 | 64.9 | 61 | GV | IGV1 (100) | Histoacryl® | 1:1 | No |
| Jang WS et al., 2014 [32] | R | 2008–2012 | Korea | 16 | 56.3 | 61.8 | GV | NS | Histoacryl® | 1:1 | NS |
| Jun CH et al., 2014 [33] | R | 2004–2013 | Korea | 455 | 83.3 | 57.65 | GV | GOV1 (61.5), GOV2 (38.5) | Histoacryl® | 1:1 | NS |
| Khawaja A et al., 2014 [34] | R | 1998–2011 | Pakistan | 97 | 63.9 | 51 | GV | GOV1 (20.6), GOV2 (36.1), IGV1 (41.2), IGV2 (2.1) | Histoacryl® | 2:1 | Yes |
| Kozieł S et al., 2015 [35] | P | 2013–2015 | Poland | 35 | NS | NS | GV | GOV2 (28.6), IGV1 (68.6), IGV2 (2.9) | Histoacryl® | 1:1 | Ns |
| Kurt M et al., 2010 [36] | R | 2004–2010 | Turkey | 66 | 62.1 | 52 | GV | GOV1 (4.5), GOV2 (69.7), IGV1 (25.8) | Liquiband® | 1:1 | Yes |
| Lee YT et al., 2000 [37] 3 | PC | 1993–1998 | China | 54 | 63.0 | 61 | GV | GOV1 (37.0), GOV2 (33.3), IGV1 (29.6) | Histoacryl® | 1:1.4 | Yes |
| Lee YT et al., 2000 [37] 4 | 47 | 74.5 | 59 | GV | GOV1 (34.0), GOV2 (42.6), IGV1 (23.4) | Histoacryl® | 1:1.4 | Yes | |||
| Liao SC et al., 2013 [38] 5 | PC | 2001–2007 | Taiwan | 35 | 45.7 | 61 | GV | NS | Histoacryl® | 1:1 | Yes |
| Liao SC et al., 2013 [38] 6 | 34 | 52.9 | 59 | GV | NS | Histoacryl® | 1:1 | Yes | |||
| Ljubicić N et al., 2011 [39] | RCT | 2004–2008 | Croatia | 22 | 72.7 | 57 | EV | Histoacryl® | 1:1.6 | Yes | |
| Lo GH et al., 2007 [40] | RCT | 1999–2004 | Taiwan | 37 | 75.7 | 52 | GV | GOV1 (45.9), GOV2 (51.4), IGV (2.7) | Histoacryl® | 1:3 | Yes |
| Lôbo MR de A et al., 2019 [41] | RCT | 2014–2016 | Brazil | 16 | 31.3 | 57.7 | GV | GOV2 (81.2), IGV1 (18.8) | Histoacryl® | 1:1 | NS |
| Maldonado C, 2019 [42] | R | 2011–2017 | Colombia | 68 | 50.0 | 64 | FV | Histoacryl® | NS | NS | |
| Martins FP et al., 2009 [43] | P | NS | Brazil | 23 | 65.2 | 53.4 | GV | GOV2 (87.0), IGV1 (13.0) | NBCA | 1:1 | NS |
| Monsanto P et al., 2013 [44] | R | 1998–2010 | Portugal | 97 | 80.4 | 59.6 | GV | GOV1 (37.2), GOV2 (27.8), IGV1 (30.9), IGV2 (4.1) | Histoacryl® | 1:1 to 1:1.5 | Yes |
| Mostafa I et al., 1997 [45] | P | NS | Egypt | 100 | 84.0 | 44.7 | GV | GOV1 (20), GOV2 or IGV1 (80) | Histoacryl® | 1:1.4 | NS |
| Ogawa K et al., 1999 [46] | RC | 1980–1996 | Japan | 17 | 76.5 | 63.5 | GV | NS | Histoacryl® | 2.3:1 | NS |
| Oh SH et al., 2015 [47] | R | 2004–2011 | South Korea | 21 | 38.1 | 8.7 | GV | GOV1 (76.2), GOV2 (23.8) | Histoacryl® | 1:1 or 1:1.6 | NS |
| Oho K et al., 1995 [48] | PC | 1989–1992 | Japan | 29 | 72.4 | 57 | CV (n = 12), FV (n = 17) | NBCA | 1:1 | No | |
| Prachayakul V et al., 2013 [49] | R | 2008–2011 | Thailand | 90 | 74.4 | 55.9 | GV | GOV1 (44.4), GOV2 (33.3), IGV1 (21.2), IGV2 (1.1) | Histoacryl® | 1:1.6 | Most patients |
| Procaccini NJ et al., 2009 [50] | RC | 1997–2007 | USA | 61 | 70.5 | 54.5 | GV | NS | Histoacryl® | 1:1 | Majority of patients |
| Ramond MJ et al., 1989 [51] | P | 1984–1988 | France | 27 | 63.0 | NS | GV | NS | Histoacryl® | 1:1 | NS |
| Rivet C et al., 2009 [52] | P | 2001–2005 | France | 8 | 25.0 | 1.3 | GV | GOV (87.5), IGV (12.5) | Glubran2® | 1:1 | NS |
| Romero-Castro R et al., 2013 [53] | RC | 2008–2012 | Spain and Germany | 19 | 73.7 | 60.8 | GV | GOV1 (5.3), GOV2 (47.4), IGV1 (47.4) | Histoacryl® | 1:1 | NS |
| Sarin SK et al., 2002 [54] | RCT | 1995–1998 | India | 20 | 75.0 | 36.1 | GV | IGV (100) | Histoacryl® | 1:1.4 | Yes |
| Sato T et al., 2016 [55] | R | NS | Japan | 228 | 64.5 | 62.5 | GV (n = 221) | GOV2 (48.9), IGV1 (47.1), IGV2 (4.1) | Histoacryl® | # | Not routinely used |
| DV (n = 5) | |||||||||||
| AV (n = 2) | |||||||||||
| Seewald S et al., 2008 [56] | R | 1994–2003 | Germany and Egypt | 131 | 69.5 | NS | GV | GOV2 (17.6), IGV1 (82.4) | Histoacryl® | 1:1.6 | NS |
| Stein DJ et al., 2019 [10] | RC | 1997–2015 | USA | 90 | 70.0 | 55.9 | GV | GOV2 (25.6), IGV1 (74.4) | Histoacryl® | 1:1 | NS |
| Sung JJ et al., 1998 [57] | RCT | NS | Hong Kong | 25 | 88.0 | 49.8 | EV | Histoacryl® | 1:1 | Yes | |
| Tan PC et al., 2006 [5] | RCT | 1996–2002 | Taiwan | 49 | 71.4 | 61.35 | GV | GOV1 (55.1), GOV2 (18.4), IGV1 (26.5) | Histoacryl® | 1:1 | Yes |
| Tantau M et al., 2014 [59] | PC | 2010–2012 | Romania | 19 | 52.6 | 62.3 | GV | GOV1 (57.9), GOV2 (42.1) | Glubran® | 1:1 | Yes |
| Thouveny F et al., 2008 [60] | R | 1998–2006 | France | 7 | 71.4 | 69 | SV | Histoacryl® | 1:8 | NS | |
| Wang YM et al., 2009 [61] | R | 2007–2008 | China | 148 | 73.0 | 50.1 | U | GOV1 (45.9), GOV2 (33.1), IGV1 (20.3), IGV2 (1) | Histoacryl® | 1:1 | Yes |
| Author, Year | Technical Success | 30-Day Rebleeding | Complications | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of Patients Evaluated | No. of Patients with Technical Success | Technical Success Rate (%) | No. of Patients Evaluated | No. of Patients with 30-Day Rebleeding | 30-Day Rebleeding Rate (%) | No. of Patients Evaluated | 1-Month Overall Complications | 1-Month Major Complications | |||
| No. of Patients | Rate (%) | No. of Patients | Rate (%) | ||||||||
| Al-Ali J et al., 2010 [21] | 37 | 35 | 94.6 | 29 | 8 | 27.6 | 37 | 0 | 0.0 | ||
| Belletrutti PJ et al., 2008 [22] | 16 | 15 | 93.8 | 33 | 8 | 24.2 | 33 | 10 | 30.3 | 2 | 6.1 |
| Caldwell SH et al., 2007 [23] | 92 | 21 | 22.8 | 92 | 2 | 2.2 | 2 | 2.2 | |||
| Cheng LF et al., 2010 [24] | 753 | 33 | 4.4 | 753 | 51 | 6.8 | 51 | 6.8 | |||
| Elsebaey MA et al., 2019 [11] | 57 | 56 | 98.2 | 57 | 11 | 19.3 | 57 | 16 | 28.1 | ||
| Elsherbiny A et al., 2006 [25] | 45 | 43 | 95.6 | 45 | 2 | 4.4 | 45 | 7 | 15.6 | ||
| Fry LC et al., 2008 [26] | 33 | 29 | 87.9 | 34 | 5 | 14.7 | 5 | 14.7 | |||
| Ho MY et al., 1991 [27] | 3 | 3 | 100 | 10 | 3 | 30.0 | 10 | 0 | 0.0 | 0 | 0.0 |
| Hong CH et al., 2009 [28] | 14 | 14 | 100 | 14 | 10 | 71.4 | 14 | 1 | 7.1 | 1 | 7.1 |
| Hou MC et al., 2009 [29] 1 | 10 | 9 | 90.0 | 44 | 17 | 38.6 | 44 | 10 | 22.7 | 10 | 22.7 |
| Hou MC et al., 2009 [29] 2 | 15 | 13 | 86.7 | 47 | 14 | 29.8 | 47 | 14 | 29.8 | 14 | 29.8 |
| Huang YH et al., 2000 [30] | 90 | 84 | 93.3 | 90 | 21 | 23.3 | 90 | 3 | 3.3 | 0 | 0.0 |
| Iwase H et al., 2001 [31] | 13 | 13 | 100 | 37 | 6 | 16.2 | 37 | 7 | 18.9 | ||
| Jang WS et al., 2014 [32] | 16 | 11 | 68.8 | 16 | 0 | 0.0 | |||||
| Jun CH et al., 2014 [33] | 455 | 441 | 96.9 | 455 | 160 | 35.2 | 455 | 154 | 33.8 | ||
| Khawaja A et al., 2014 [34] | 97 | 87 | 89.7 | 90 | 24 | 26.7 | 97 | 27 | 27.8 | 2 | 2.1 |
| Kozieł S et al., 2015 [35] | 35 | 32 | 91.4 | 35 | 6 | 17.1 | 35 | 11 | 31.4 | 0 | 0.0 |
| Kurt M et al., 2010 [36] | 66 | 65 | 98.5 | 66 | 11 | 16.7 | 66 | 1 | 1.5 | 1 | 1.5 |
| Lee YT et al., 2000 [37] 3 | 54 | 52 | 95.7 | 54 | 19 | 70.2 | 54 | 22 | 19.1 | ||
| Lee YT et al., 2000 [37] 4 | 47 | 45 | 96.3 | 47 | 33 | 35.2 | 47 | 9 | 40.7 | ||
| Liao SC et al., 2013 [38] 5 | 34 | 25 | 73.5 | 34 | 3 | 8.8 | 34 | 0 | 0.0 | 0 | 0.0 |
| Liao SC et al., 2013 [38] 6 | 35 | 31 | 88.6 | 35 | 7 | 20.0 | 35 | 0 | 0.0 | 0 | 0.0 |
| Ljubicić N et al., 2011 [39] | 22 | 22 | 100.0 | 22 | 3 | 13.6 | - | ||||
| Lo GH et al., 2007 [40] | 37 | 19 | 51.4 | 37 | 15 | 40.5 | 37 | 15 | 40.5 | ||
| Lôbo MR de A et al., 2019 [41] | 16 | 10 | 62.5 | ||||||||
| Maldonado C, 2019 [42] | 68 | 68 | 100 | 68 | 0 | 0.0 | |||||
| Martins FP et al., 2009 [43] | 23 | 20 | 87.0 | 23 | 1 | 4.3 | 23 | 4 | 17.4 | 1 | 4.3 |
| Monsanto P et al., 2013 [44] | 97 | 93 | 95.9 | 97 | 14 | 14.4 | 97 | 17 | 17.5 | 8 | 8.2 |
| Mostafa I et al., 1997 [45] | 100 | 100 | 100 | 100 | 10 | 10.0 | 100 | 1 | 1.0 | 1 | 1.0 |
| Ogawa K et al., 1999 [46] | 17 | 17 | 100 | 17 | 3 | 17.6 | 0 | 0.0 | |||
| Oh SH et al., 2015 [47] | 21 | 19 | 90.5 | 21 | 5 | 23.8 | 21 | 1 | 4.8 | 1 | 4.8 |
| Oho K et al., 1995 [48] | 29 | 27 | 93.1 | 27 | 8 | 29.6 | 29 | 12 | 41.4 | 7 | 24.1 |
| Prachayakul V et al., 2013 [49] | 90 | 88 | 97.8 | 90 | 28 | 31.1 | 90 | 13 | 14.4 | 13 | 14.4 |
| Procaccini NJ et al., 2009 [50] | 58 | 13 | 22.4 | 61 | 5 | 8.2 | 5 | 8.2 | |||
| Ramond MJ et al., 1989 [51] | 27 | 27 | 100 | 27 | 10 | 37.0 | 27 | 9 | 33.3 | ||
| Rivet C et al., 2009 [52] | 8 | 8 | 100 | 8 | 3 | 37.5 | 8 | 1 | 12.5 | ||
| Romero-Castro R et al., 2013 [53] | 19 | 19 | 100 | 19 | 0 | 0.0 | 19 | 11 | 57.9 | 2 | 10.5 |
| Sarin SK et al., 2002 [54] | 20 | 19 | 95.0 | 20 | 5 | 25.0 | |||||
| Sato T et al., 2016 [55] | 228 | 228 | 100 | 228 | 4 | 1.8 | |||||
| Seewald S et al., 2008 [56] | 131 | 131 | 100 | 131 | 9 | 6.9 | 131 | 0 | 0.0 | 0 | 0.0 |
| Stein DJ et al., 2019 [10] | 90 | 6 | 6.7 | 4 | 4.4 | ||||||
| Sung JJ et al., 1998 [57] | 25 | 21 | 84.0 | 25 | 7 | 28.0 | |||||
| Tan PC et al., 2006 [58] | 49 | 38 | 77.6 | 49 | 11 | 22.4 | 49 | 11 | 22.4 | 11 | 22.4 |
| Tantau M et al., 2014 [59] | 19 | 19 | 100 | 19 | 6 | 31.6 | 19 | 5 | 26.3 | 5 | 26.3 |
| Thouveny F et al., 2008 [60] | 7 | 6 | 85.7 | 7 | 2 | 28.6 | 7 | 0 | 0.0 | 0 | 0.0 |
| Wang YM et al., 2009 [61] | 148 | 142 | 95.9 | 148 | 21 | 14.2 | 148 | 1 | 0.7 | 0 | 0.0 |
| Author, Year | Bleeding Site | NBCA-Lipiodol® | Comparator | |
|---|---|---|---|---|
| No. of Patients | Treatment Method | No. of Patients | ||
| Ljubicić N et al., 2011 [39] | EV | 22 | EVL | 21 |
| Lo GH et al., 2007 [40] | GV | 37 | TIPS | 35 |
| Lôbo MR de A et al., 2019 [41] | GV | 16 | EUS-guided coils plus cyanoacrylate-Lipiodol® mixture | 16 |
| Sarin SK et al., 2002 [54] | GV | 20 | Sclerotherapy with alcohol | 17 |
| Sung JJ et al., 1998 [57] | EV | 25 | Sclerotherapy with sodium tetradecyl sulphate | 25 |
| Tan PC et al., 2006 [58] | GV | 49 | EVL | 48 |
| Elsebaey MA et al., 2019 [11] | EV | 57 | Sclerotherapy with ethanolamine oleate | 56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chevallier, O.; Guillen, K.; Comby, P.-O.; Mouillot, T.; Falvo, N.; Bardou, M.; Midulla, M.; Aho-Glélé, L.-S.; Loffroy, R. Safety, Efficacy, and Outcomes of N-Butyl Cyanoacrylate Glue Injection through the Endoscopic or Radiologic Route for Variceal Gastrointestinal Bleeding: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2298. https://doi.org/10.3390/jcm10112298
Chevallier O, Guillen K, Comby P-O, Mouillot T, Falvo N, Bardou M, Midulla M, Aho-Glélé L-S, Loffroy R. Safety, Efficacy, and Outcomes of N-Butyl Cyanoacrylate Glue Injection through the Endoscopic or Radiologic Route for Variceal Gastrointestinal Bleeding: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(11):2298. https://doi.org/10.3390/jcm10112298
Chicago/Turabian StyleChevallier, Olivier, Kévin Guillen, Pierre-Olivier Comby, Thomas Mouillot, Nicolas Falvo, Marc Bardou, Marco Midulla, Ludwig-Serge Aho-Glélé, and Romaric Loffroy. 2021. "Safety, Efficacy, and Outcomes of N-Butyl Cyanoacrylate Glue Injection through the Endoscopic or Radiologic Route for Variceal Gastrointestinal Bleeding: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 11: 2298. https://doi.org/10.3390/jcm10112298
APA StyleChevallier, O., Guillen, K., Comby, P.-O., Mouillot, T., Falvo, N., Bardou, M., Midulla, M., Aho-Glélé, L.-S., & Loffroy, R. (2021). Safety, Efficacy, and Outcomes of N-Butyl Cyanoacrylate Glue Injection through the Endoscopic or Radiologic Route for Variceal Gastrointestinal Bleeding: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 10(11), 2298. https://doi.org/10.3390/jcm10112298