
Targeting Alcohol Septal Ablation in Patients with Obstructive Hypertrophic Cardiomyopathy Candidates for Surgical Myectomy: Added Value of Three-Dimensional Intracoronary Myocardial Contrast Echocardiography

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Echocardiographic Study
2.3. Myocardial Contrast Echocardiography
2.4. Myocardial Contrast Echocardiography Analysis
2.5. Alcohol Septal Ablation
2.6. Follow-Up
2.7. Statistical Analysis
3. Results
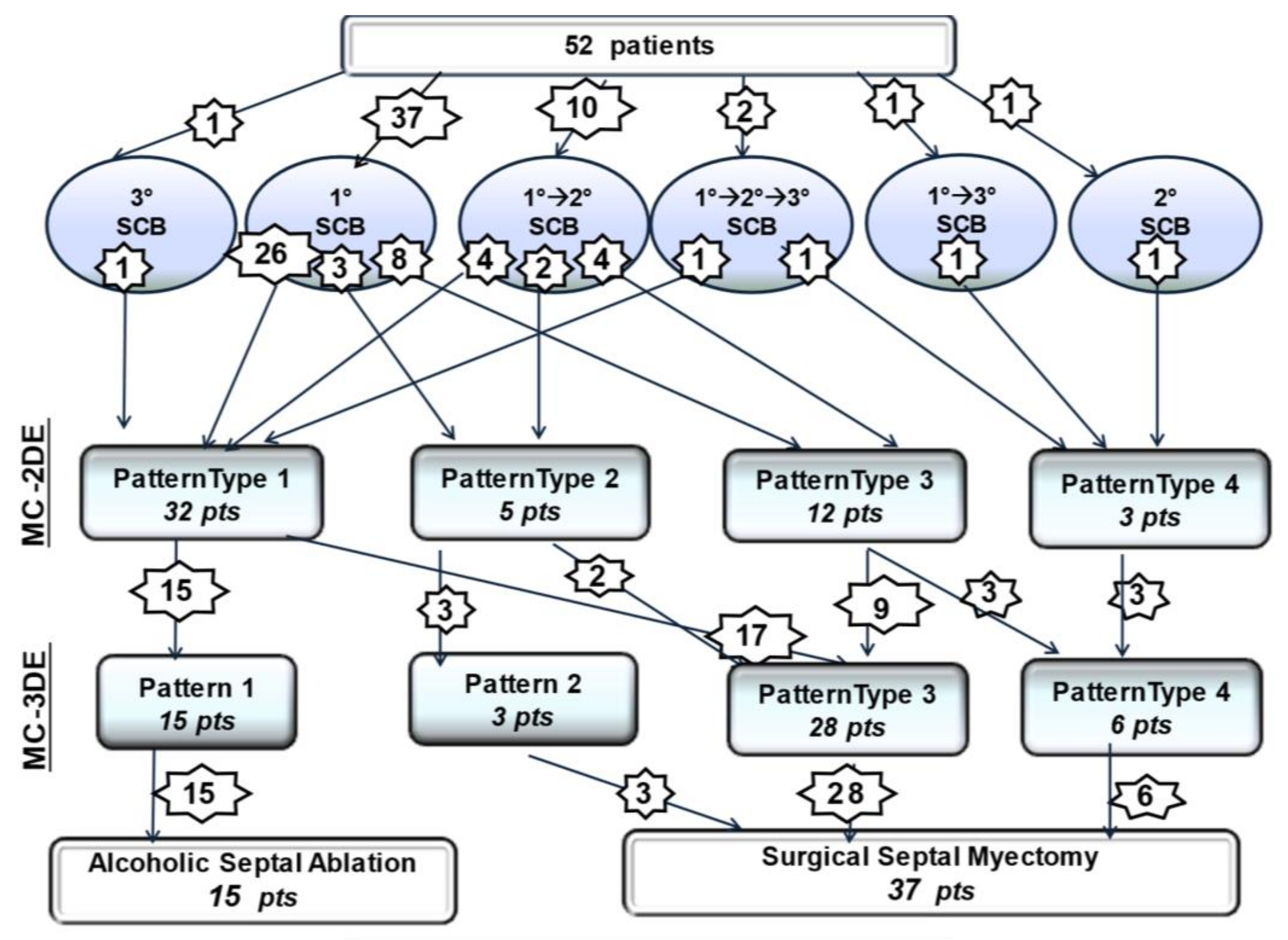
3.1. Two-Dimensional Myocardial Contrast Echocardiography Phenotypes
3.2. Three-Dimensional Myocardial Contrast Echocardiography Phenotypes
3.3. Alcohol Septal Ablation
3.4. Follow-Up Results
4. Discussion
Limitation of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kimmelstiel, C.; Zisa, D.C.; Kuttab, J.S.; Wells, S.; Udelson, J.E.; Wessler, B.S.; Rastegar, H.; Kapur, N.K.; Weintraub, A.R.; Maron, B.J.; et al. Guideline-based referral for septal reduction therapy in obstructive hypertrophic cardiomyopathy is associated with excellent clinical outcomes. Circ. Cardiovasc. Interv. 2019, 12, e007673. [Google Scholar] [CrossRef]
- Nishimura, R.A.; Seggewiss, H.; Schaff, H.V. Hypertrophic obstructive cardiomyopathy: Surgical myectomy and septal ablation. Circ. Res. 2017, 15, 771–783. [Google Scholar] [CrossRef] [PubMed]
- Bytyçi, S.; Nistri, S.; Mörner, S.; Henein, M.Y. Alcohol septal ablation versus septal myectomy treatment of obstructive Hypertrophic Cardiomyopathy: A systematic review and meta-analysis. J. Clin. Med. 2020, 9, 3062. [Google Scholar] [CrossRef]
- Batzner, A.; Pfeiffer, B.; Neugebauer, A.; Aicha, D.; Blank, C.; Seggewiss, H. Survival after alcohol septal ablation in patients with hypertrophic obstructive cardiomyopathy. J. Am. Coll. Cardiol. 2018, 72, 3087–3094. [Google Scholar] [CrossRef]
- Veselka, J.; Jensen, M.K.; Liebregts, M.; Januska, J.; Krejci, J.; Bartel, T.; Dabrowski, M.; Hansen, P.R.; Almaas, V.M.; Seggewiss, H.; et al. Long-term clinical outcome after alcohol septal ablation for obstructive hypertrophic cardiomyopathy: Results from the Euro-ASA registry. Eur. Heart J. 2016, 37, 1517–1523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonardi, R.A.; Kransdorf, E.P.; Simel, D.L.; Wang, A. Meta-analyses of septal reduction therapies for obstructive hypertrophic cardiomyopathy. Circ. Cardiovasc. Interv. 2010, 3, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Liebregts, M.; Vriesendorp, P.A.; Mahmoodi, B.K.; Schinkel, A.F.; Michels, M.; ten Berg, J.M. A systematic review and meta-analysis of long-term outcomes after septal reduction therapy in patients with hypertrophic cardiomyopathy. JACC Hearth Fail. 2015, 3, 896–905. [Google Scholar] [CrossRef] [PubMed]
- Liebregts, M.; Steggerda, R.C.; Vriesendorp, P.A.; van Velzen, H.; Schinkel, A.F.; Willems, R.; van Cleemput, J.; van den Berg, M.P.; Michels, M.; ten Berg, J.M. Long-term outcome of alcohol septal ablation for obstructive hypertrophic cardiomyopathy in the young and the elderly. JACC Cardiovasc. Interv. 2016, 14, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Veselka, J.; Krejci, J.; Tomasov, P.; Jahnlová, D.; Honěk, T.; Januška, J.; Branny, M.; Zemánek, D. Survival of patients ≤50 years of age after alcohol septal ablation for hypertrophic obstructive cardiomyopathy. Can. J. Cardiol. 2014, 30, 634–638. [Google Scholar] [CrossRef] [PubMed]
- Liebregts, M.; Faber, L.; Jensen, M.K.; Vriesendorp, P.A.; Januska, J.; Krejci, J.; Hansen, P.R.; Seggewiss, H.; Horstkotte, D.; Adlova, R.; et al. Outcomes of alcohol septal ablation in younger patients with obstructive hypertrophic cardiomyopathy. JACC Cardiovasc. Interv. 2017, 10, 1134–1143. [Google Scholar] [CrossRef]
- Faber, L.; Seggewiss, H.; Gleichmann, U. Percutaneous transluminal septal myocardial ablation in hypertrophic obstructive cardiomyopathy: Results with respect to intraprocedural myocardial contrast echocardiography. Circulation 1998, 22, 2415–2421. [Google Scholar] [CrossRef] [Green Version]
- Monakier, D.; Woo, A.; Puri, T.; Schwartz, L.; Ross, J.; Jamorski, M.; Yang, H.; Liu, Z.; Vannan, M.; Wigle, E.D.; et al. Usefulness of myocardial contrast echocardiographic quantification of risk area for predicting postprocedural complications in patients undergoing septal ethanol ablation for obstructive hypertrophic cardiomyopathy. Am. J. Cardiol. 2004, 94, 1515–1522. [Google Scholar] [CrossRef] [PubMed]
- Veselka, J.; Zemánek, D.; Fiedler, J.; Šváb, P. Real-time myocardial contrast echo-cardiography for echo-guided alcohol septal ablation. Arch. Med. Sci. 2009, 5, 271–272. [Google Scholar]
- Moya-Mur, J.L.; Mestre-Barcelo, J.L.; Salido-Tahoces, L.; Hinojar-Baydes, R.; Hernan-dez-Antolen, R.; Zamorano-Gomez, J.L. Alcohol ablation in hypertrophic cardiomyopathy: Localization and quantification of target septal artery-dependent myocardium with 3-dimensional echocardiography. Rev. Esp. Cardiol. 2015, 68, 531–535. [Google Scholar] [CrossRef] [PubMed]
- Bogunovic, N.; van Buuren, F.; Horstkotte, D.; Faber, L. Rapid Visualization of PTSMA target area by real time 3D myocardial contrast echocardiography. Echocardiography 2014, 31, E197–E199. [Google Scholar] [CrossRef]
- Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; Mahrholdt, H.; et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the diag-nosis and management of hypertrophic cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar]
- La Canna, G.; Scarfò, I.; Arendar, I.; Alati, E.; Caso, I.; Alfieri, O. Phenotyping left ventricular obstruction with postprandial re-test echocardiography in hypertrophic cardiomyopathy. Am. J. Cardiol. 2020, 125, 1688–1693. [Google Scholar] [CrossRef]
- Maron, M.S.; Olivotto, I.; Betocchi, S.; Casey, S.A.; Lesser, J.R.; Losi, M.A.; Cecchi, F.; Maron, B.J. Effect of left ventricular outflow tract obstruction on clinical outcome in hypertrophic cardiomyopathy. N. Engl. J. Med. 2003, 348, 295–303. [Google Scholar] [CrossRef]
- Elliott, P.M.; Gimeno, J.R.; Tomé, M.T.; Shah, J.; Ward, D.; Thaman, R.; Mogensen, J.; McKenna, W.J. Left ventricular outflow tract obstruction and sudden death risk in patients with hypertrophic cardiomyopathy. Eur. Heart J. 2006, 27, 1933–1941. [Google Scholar] [CrossRef]
- Maron, B.J. Clinical Course and Management of Hypertrophic Cardiomyopathy. N. Engl. J. Med. 2018, 379, 655–668. [Google Scholar] [CrossRef]
- Ball, W.; Ivanov, J.; Rakowski, H.; Wigle, E.D.; Linghorne, M.; Ralph-Edwards, A.; Williams, W.G.; Schwartz, L.; Guttman, A.; Woo, A. Long-term survival in patients with resting obstructive hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2011, 58, 2313–2321. [Google Scholar] [CrossRef] [Green Version]
- Fifer, M.A. Septal reduction therapy for hypertrophic obstructive cardiomyo-pathy. J. Am. Coll. Cardiol. 2018, 72, 3095–3097. [Google Scholar] [CrossRef]
- Ommen, S.R.; Mital, S.; Burke, M.A.; Day, S.M.; Deswal, A.; Elliott, P.; Evanovich, L.L.; Hung, J.; Joglar, J.A.; Kantor, P.; et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients with Hypertrophic Cardiomyopathy: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2020, 142, e558–e631. [Google Scholar]
- Yacoub, M.H.; Afifi, A.; Saad, H.; Aguib, H.; ElGuindy, A. Current state of the art and future of myectomy. Ann. Cardiothorac. Surg. 2017, 6, 307–317. [Google Scholar] [CrossRef] [Green Version]
- Sherrid, M.V.; Arabadjian, M. Echocardiography to Individualize treatment for hypertrophic cardiomyopathy. Progr. Cardiovasc. Dis. 2012, 54, 461–476. [Google Scholar] [CrossRef] [PubMed]
- Collis, R.; Tsang, V.; Pantazis, A.; Tome-Esteband, M.; Perry, M.; Christopher, G.A.E.; McGregor, C.G.A. Individualized surgical strategies for left ventricular outflow tract obstruction in hypertrophic cardiomyopathy. Eur. J. Cardiothorac. Surg. 2018, 53, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- La Canna, G.; Airoldi, F.; Capritti, E.; Grimaldi, A.; Colombo, A.; Alfieri, O. Alcohol septal ablation versus surgical myectomy: A patient with obstructive HCM. Nat. Clin. Pract. Cardiovasc. Med. 2007, 4, 570–576. [Google Scholar] [CrossRef]
- Ferrazzi, P.; Spirito, P.; Iacovoni, A.; Calabrese, A.; Migliorati, K.; Simon, C.; Pentiricci, S.; Poggio, D.; Grillo, M.; Amigoni, P.; et al. Transaortic chordal cutting: Mitral valve repair for obstructive hypertrophic cardiomyopathy with mild septal hypertrophy. J. Am. Coll. Cardiol. 2015, 66, 1687–1696. [Google Scholar] [CrossRef] [Green Version]
- Rowin, E.J.; Maron, B.J.; Chokshi, A.; Kannappan, M.; Arkun, K.; Wang, W.; Rastegar, H.; Maron, M.S. Clinical spectrum and management implications of left ventricular outflow obstruction with mild ventricular septal thickness in hypertrophic cardiomyopathy. Am. J. Cardiol. 2018, 122, 1409–1420. [Google Scholar] [CrossRef]
- Nguyen, A.; Schaff, H.V.; Nishimura, R.A.; Dearani, J.A.; Geske, J.B.; Lahr, B.D.; Ommen, S.R. Does septal thickness influence outcome of myectomy for hypertrophic obstructive cardiomyopathy? Eur. J. Cardiothorac. Surg. 2018, 53, 582–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nampiaparampil, R.G.; Swistel, D.G.; Schlame, M.; Saric, M.; Sherrid, M.V. Intraoperative two- and three-dimensional transesophageal echocardiography in combined myectomy-mitral operations for hypertrophic cardiomyopathy. J. Am. Soc. Echocardiogr. 2018, 31, 275–288. [Google Scholar] [CrossRef]
- Ommen, S.R.; Park, S.H.; Click, R.L.; Freeman, W.K.; Schaff, H.V.; Tajik, A.J.A. Impact of intraoperative transesophageal echocardiography in the surgical management of hypertrophic cardiomyopathy. Am. J. Cardiol. 2002, 90, 1022–1024. [Google Scholar] [CrossRef]
- Elsayes, A.B.; Basura, A.; Zahedi, F.; Moreno-Duarte, I.; Rowin, E.J.; Maron, M.; Rastegar, H.; Frederick, C.; Cobey, F.C. Intraoperative provocative testing in patients with obstructive hypertrophic cardiomyopathy undergoing septal myectomy. J. Am. Soc. Echocardiogr. 2020, 33, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Balaram, S.K.; Sherrid, M.V.; Derose, J., Jr.; Hillel, Z.; Winson, G.; Swistel, D.G. Beyond extended myectomy for hypertrophic cardiomyopathy: The resection-plication-release (RPR) repair. Ann. Thorac. Surg. 2005, 80, 217–223. [Google Scholar] [CrossRef]
- Nguyen, A.; Schaff, H.V. Surgical myectomy: Subaortic, midventricular, and apical. Rev. Cardiol. Clin. 2019, 37, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Schaff, H.V.; Nishimura, R.A.; Geske, J.B.; Dearani, J.A.; Ommen, S.R. Transapical septal myectomy for hypertrophic cardiomyopathy with midventricular obstruction. Ann. Thorac. Surg. 2021, 111, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Solomon, Z.; Breton, C.; Rowin, E.J.; Maron, B.J.; Maron, M.S.; Chen, F.Y.; Rastegar, H. Surgical approaches to hypertrophic obstructive cardiomyopathy. Semin. Thorac. Cardiovasc. Surg. 2018, 30, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Ommen, S.R.; Maron, B.J.; Olivotto, I.; Maron, M.S.; Cecchi, F.; Betocchi, S.; Gersh, B.J.; Ackerman, M.J.; McCully, R.B.; Dearani, J.A.; et al. Long-term effects of surgical septal myectomy on survival in patients with obstructive hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2005, 46, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Iacovoni, A.; Spirito, P.; Simon, C.; Iascone, M.; Di Dedda, G.; De Filippo, P.; Pentiricci, S.; Boni, L.; Senni, M.; Gavazzi, A.; et al. A contemporary European experience with surgical septal myectomy in hypertrophic cardiomyopathy. Eur. Heart. J. 2012, 33, 2080–2087. [Google Scholar] [CrossRef] [Green Version]
- Collis, R.; Watkinson, O.; O’Mahony, C.; Guttmann, O.P.; Pantazis, A.; Tome-Esteban, M.; Tsang, V.; Chandrasekaran, V.; McGregor, C.G.A.; Elliott, P.M. Long-term outcomes for different surgical strategies to treat left ventricular outflow tract obstruction in hypertrophic cardiomyopathy. Eur. J. Heart. Fail. 2018, 20, 398–405. [Google Scholar] [CrossRef] [Green Version]
- Rastegar, H.; Boll, G.; Rowin, E.J.; Dolan, N.; Carroll, C.; Udelson, J.E.; Wang, W.; Carpino, P.; Maron, B.J.; Maron, M.S.; et al. Results of surgical septal myectomy for obstructive hypertrophic cardiomyopathy: The Tufts experience. Ann. Cardiothorac. Surg. 2017, 6, 353–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geske, J.B.; Driver, C.N.; Yogeswaran, V.; Ommen, S.R.; Schaff, H.V. Comparison of expected and observed outcomes for septal myectomy in hypertrophic obstructive cardiomyopathy. Am. Heart. J. 2020, 221, 159–164. [Google Scholar] [CrossRef]
- Maron, B.J.; Dearani, J.A.; Maron, M.S.; Ommen, S.R.; Rastegar, H.; Nishimura, R.A.; Swistel, D.G.; Sherrid, M.V.; Ralph-Edwards, A.; Rakowski, H.; et al. Why we need more septal myectomy surgeons: An emerging recognition. J. Thorac. Cardiovasc. Surg. 2017, 154, 1681–1685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maron, M.S.; Spirito, P.; Maron, B.J. Case for earlier surgical myectomy in patients with obstructive hypertrophic cardiomyopathy. Circulation 2018, 138, 2076–2207. [Google Scholar] [CrossRef] [PubMed]
- Cavigli, L.; Fumagalli, C.; Maurizi, N.; Rossi, A.; Arretini, A.; Targetti, M.; Passantino, S.; Girolami, F.; Tomberli, B.; Baldini, K.; et al. Timing of invasive septal reduction therapies and outcome of patients with obstructive hypertrophic cardiomyopathy. Int. J. Cardiol. 2018, 273, 155–161. [Google Scholar] [CrossRef]
- Sorajja, P.; Ommen, S.R.; Holmes, D.R., Jr.; Dearani, J.A.; Rihal, C.S.; Gersh, B.J.; Lennon, R.J.; Nishimura, R.A. Survival after alcohol septal ablation for obstructive hypertrophic cardiomyopathy. Circulation 2012, 126, 2374–2380. [Google Scholar] [CrossRef] [Green Version]
- Osman, M.; Kheiri, B.; Osman, K.; Barbarawi, M.; Alhamoud, H.; Alqahtani, F.; Alkhouli, M. Alcohol septal ablation vs myectomy for symptomatic hypertrophic obstructive cardiomyopathy: Systematic review and meta-analysis. Clin. Cardiol. 2019, 42, 190–197. [Google Scholar] [CrossRef] [Green Version]
- Jensen, M.K.; Prinz, C.; Horstkotte, D.; van Buuren, F.; Bitter, T.; Faber, L.; Bundgaard, H. Alcohol septal ablation in patients with hypertrophic obstructive cardiomyopathy: Low incidence of sudden cardiac death and reduced risk profile. Heart 2013, 99, 1012–1017. [Google Scholar] [CrossRef]
- Liebregts, M.; Vriesendorp, P.A.; ten Berg, J.M. Alcohol septal ablation for obstructive hypertrophic cardiomyopathy: A word of endorsement. J. Am. Coll. Cardiol. 2017, 25, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Faber, L.; Ziemssen, P.; Seggewiss, H. Targeting percutaneous transluminal septal ablation for hyper-trophic obstructive cardiomyopathy by intraprocedural echocardiographic monitoring. J. Am. Soc. Echocardiogr. 2000, 13, 1074–1079. [Google Scholar] [CrossRef]
- Rigopoulos, A.G.; Sakellaropoulos, S.; Ali, M.; Mavrogeni, S.; Manginas, A.; Pauschinger, M.; Noutsias, M. Transcatheter septal ablation in hypertrophic obstructive cardiomyopathy: A technical guide and review of published results. Heart Fail. Rev. 2018, 23, 907–917. [Google Scholar] [CrossRef]
- van Dockum, W.G.; Beek, A.M.; ten Cate, F.J.; ten Berg, J.M.; Bondarenko, O.; Götte, M.J.; Twisk, J.W.; Hofman, M.B.; Visser, C.A.; van Rossum, A.C. Early onset and progression of left ventricular re-modeling after alcohol septal ablation in hypertrophic obstructive cardiomyopathy. Circulation 2005, 111, 2503–2508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoerger, D.M.; Picard, M.H.; Palacios, I.F.; Vlahakes, G.J.; Lowry, P.A.; Fifer, M.A. Time course of pressure gradient response after first alcohol septal ablation for obstructive hypertrophic cardiomyopathy. Am. J. Cardiol. 2006, 97, 1511–1514. [Google Scholar] [CrossRef]
- Valeti, U.S.; Nishimura, R.A.; Holmes, D.R.; Araoz, P.A.; Glockner, J.F.; Breen, J.F.; Ommen, S.R.; Gersh, B.J.; Tajik, A.J.; Rihal, C.S.; et al. Comparison of surgical septal myectomy and alcohol septal ablation with cardiac magnetic re-sonance imaging in patients with hypertrophic obstructive cardiomyopathy. J. Am. Coll. Cardiol. 2007, 49, 350–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veselka, J.; Faber, L.; Liebregts, M.; Cooper, R.; Januska, J.-S.; Krejci, J.; Bartel, T.; Dabrowski, M.; Han-sen, P.R.; Almaas, V.M.; et al. Outcome of alcohol septal ablation in mildly symptomatic patients with hypertrophic obstructive cardiomyopathy: A long-term follow-up study based on the Euro-Alcohol Septal Ablation Registry. Am. Heart Assoc. 2017, 6, e005735. [Google Scholar] [CrossRef] [Green Version]
- Reinhard, W.; ten Cate, F.J.; Scholten, M.; De Laat, L.E.; Vos, J. Permanent pacing for complete atrioventricular block after nonsurgical (alcohol) septal reduction in patients with obstructive hypertrophic cardiomyopathy. Am. J. Cardiol. 2004, 93, 1064–1066. [Google Scholar] [CrossRef]
- Sorajja, P. Alcohol Septal Ablation for Obstructive Hypertrophic Cardiomyopathy A Word of Balance. J. Am. Coll. Cardiol. 2017, 70, 489–494. [Google Scholar] [CrossRef]
- ten Cate, F.J.; Soliman, O.; Michels, M.; Theuns, D.A.M.J.; de Jong, P.L.; Geleijnse, M.L.; Serruys, P.W. Long-term outcome of alcohol septal ablation in patients with obstructive hypertrophic cardiomyopathy a word of caution. Circ. Heart Fail. 2010, 3, 362–369. [Google Scholar] [CrossRef] [Green Version]
- Lam, M.C.; Naidu, S.S.; Kolte, D.; Kennedy, K.; Feldman, D.N.; Antony, F.; Chu, A.F.; Abbott, D.; Gordon, P.; Aronow, H.D. Cardiac implantable electronic device placement following alcohol septal ablation for hypertrophic cardiomyopathy in the United State. J. Cardiovasc. Electrophysiol. 2020, 31, 2712–2719. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Nishimura, R.A. Revisiting arrhythmic risk after alcohol septal ablation is the pendulum finally swinging. Back to Myectomy? JACC Heart Fail. 2014, 2, 637–640. [Google Scholar] [CrossRef]
- Liebregts, M.; Faber, L.; Jensen, M.K.; Vriesendorp, P.A.; Hansen, P.R.; Seggewiss, H.; Horstkotte, D.; Adlova, R.; Michels, M.; Bundgaard, H.; et al. Validation of the HCM Risk-SCD model in patients with hy-pertrophic cardiomyopathy following alcohol septal ablation. Europace 2018, 20, f198–f203. [Google Scholar] [CrossRef]
- Veselka, J.; Tomašov, P.; Januška, J.; Krejčí, J.; Adlová, R. Obstruction after alcohol septal ablation is associated with cardiovascular mortality events. Heart 2016, 15, 793–1796. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, A.; Schaff, H.V.; Hang, D.; Nishimura, R.A.; Geske, J.B.; Dearani, J.A.; Lahr, B.D.; Ommen, S.R. Surgical myectomy versus alcohol septal ablation for obstructive hypertrophic cardiomyopathy: A propensity score-matched cohort. J. Thorac. Cardiovasc. Surg. 2019, 157, 306–315. [Google Scholar] [CrossRef]
- Veselka, J.; Faber, L.; Liebregts, M.; Cooper, R.; Januska, J.; Krejci, J.; Dabrowski, M.; Hansen, P.R.; Seggewiss, H.; Horstkotte, D.; et al. Long-term outcome of repeated septal reduction therapy after alcohol septal ablation for hypertrophic obstructive cardiomyopathy: Insight from the Euro-ASA registry. Arch. Med. Sci. 2020, 16, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Wallace, E.I.; Thompson, J.; Faulkner, M.W.; Gurley, J.C.; Smith, M.D. Septal perforator anatomy and variability of perfusion bed by myocardial contrast echocardiography: A study of hypertrophic cardiomyopathy patients undergoing alcohol septal ablation. J. Interven. Cardiol. 2013, 26, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Edwards, W.D.; Holmes, D.R., Jr.; Tajik, A.J.; Nishimura, R.A. Anatomy of the first septal perforating artery: A study with implications for ablation therapy for hypertrophic cardiomyopathy. Mayo Clin. Proc. 2001, 76, 799–802. [Google Scholar] [CrossRef]
- Chan, W.; Williams, L.; Kotowycz, M.A.; Woo, A.; Rakowski, H.; Schwartz, L.; Overgaard, C.B. Angiographic and echocardiographic correlates of suitable septal perforators for alcohol septal ablation in hypertrophic obstructive cardiomyopathy. Can. J. Cardiol. 2014, 30, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.K.; Swaminathan, R.V.; Looser, P.; Minutello, R.M.; Wong, S.C.; Bergman, G.; Naidu, S.S.; Gade, C.L.F.; Charitakis, K.; Singh, H.S.; et al. Hospital volume outcomes after septal myectomy and alcohol septal ablation for treatment of obstructive hypertrophic cardiomyopathy US Nationwide Inpatient Database, 2003–2011. JAMA Cardiol. 2016, 1, 324–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veselka, J.; Faber, L.; Jensen, M.K.; Cooper, R.; Januska, J.; Krejci, J.; Bartel, T.; Dabrowski, M.; Hansen, P.R.; Almaas, V.M.; et al. Effect of institutional experience on outcomes of alcohol septal ablation for hypertrophic obstructive cardiomyopathy. Can. J. Cardiol. 2018, 34, 16–22. [Google Scholar] [CrossRef]
- Leonardi, R.A.; Townsend, J.C.; Patel, C.A.; Wolf, B.J.; Todoran, T.M.; Powers, E.R.; Steinberg, D.H.; Fernandes, V.L.; Nielsen, C.D. Alcohol septal ablation for obstructive hypertrophic cardiomyopathy: Outcomes in young, middle-aged, and elderly patients. Catheter. Cardiovasc. Interv. 2013, 82, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Veselka, J.; Duchonová, R.; Pálenícková, J.; Zemánek, D.; Sváb, P.; Hájek, P.; Maly, M.; Blásko, P.; Tesar, D.; Cervinka, P. Age-related hemodynamic and morphologic differences in patients undergoing alcohol septal ablation for hypertrophic obstructive cardiomyopathy. Circ. J. 2006, 70, 880–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veselka, J.; Faber, L.; Liebregts, M.; Cooper, R.; Januska, J.; Kashtanov, M.; Dabrowski, M.; Hansen, P.R.; Seggewiss, H.; Hansvenclova, E.; et al. Short- and long-term outcomes of alcohol septal ablation for hypertrophic obstructive cardiomyopathy in patients with mild left ventricular hypertrophy: A propensity score matching analysis. Eur. Heart J. 2019, 40, 1681–1687. [Google Scholar] [CrossRef] [PubMed]
- Veselka, J.; Jensen, M.; Liebregts, M.; Cooper, R.M.; Januska, J.; Kashtanov, M.; Dabrowski, M.; Hansen, P.R.; Seggewiss, H.; Hansvenclova, E.; et al. Alcohol septal ablation in patients with severe septal hypertrophy. Heart 2020, 106, 462–466. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients (n°) | 52 |
|---|---|
| Age (years) | 55 ± 15 |
| Female (n°) | 27 (52%) |
| Male (n°) | 25 (48%) |
| HCM family history (n°) | 8 (15%) |
| NYHA class III or IV dyspnea (n°) | 38 (73%) |
| CCS class III or IV angina (n°) | 18 (35%) |
| Syncope (n°) | 12 (23%) |
| Smoking (n°) | 11 (21%) |
| Atrial Fibrillation (n°) | 14 (27%) |
| NSVT (n°) | 1 (2%) |
| Mild Arterial Hypertension (n°) | 14 (27%) |
| Diabetes mellitus (n°) | 7 (13.5%) |
| Non-significant CAD (n°) | 4 (8%) |
| Left Bundle Branch Block (n°) | 3 (0.5%) |
| Right Bundle Branch Block (n°) | 1(0.2%) |
| Pacemaker (n°) | 1 (0.5%) |
| ICD (n°) | 2 (0.4%) |
| Medical therapy | |
| Beta-blockers (n°) | 50 (96%) |
| Calcium-antagonist (n°) | 20 (38%) |
| Antiarrhythmic drugs (n°) | 7 (13.5%) |
| Disopyramide (n°) | 8 (15%) |
| Echocardiographic parameters | |
| Ejection Fraction (%) | 61.58% ± 4.1 |
| LV end-diastolic diameter (mm) | 44.6 ± 4.6 |
| Myocardial Hypertrophy | |
| -Asymmetric (n°) | 47(90%) |
| -Symmetric (n°) | 5 (10%) |
| SAM-aortic valve distance (mm) | 24 ± 4 |
| Septal thickness of target septal zone (mm) | 20 ± 5 |
| LVOT gradient (mmHg) | 69.15 ± 42 |
| SAM | |
| -at rest fasting (n°) | 35 (67%) |
| -at rest eating (n°) | 52 (100%) |
| -inducible (n°) | 15 (29%) |
| SAM-related MR >2 + (n°) | 42 (89%) |
| Mitral annular calcification (n°) | 12 (23%) |
| Left atrium dilation (vol > 50 mL/m2) (n°) | 14 (27%) |
| sPAP ≥ 50 mm Hg (n°) | 14 (27%) |
| Variables | Baseline (15 pts) | Post-ASA (15 pts) | Pre-Discharge (15 pts) | 1-Year FU (14 pts) | 5-Year FU (14 pts) | 10-Year FU (13 pts) * | >10-Year FU (10 pts) ** |
|---|---|---|---|---|---|---|---|
| TSZ Thickness (mm) | 20 ± 5 # | 19 ± 4 | 18 ± 7 | 16 ± 6 | 15 ± 8 | 15 ± 6 | 14 ± 2 |
| IVG (mm Hg) | 72 ± 44 ## | 20 ± 3 | 20 ± 4 | 20 ± 6 | 18 ± 7 | 16 ± 7 | 15 ± 6 |
| SAM-related MR >2+ <2+ | 15 0 | 0 8 | 0 7 | 0 6 | 0 5 | 0 5 | 0 10 |
| LVOT-area (cm2) | 2.7 ± 4 § | 3.2 ± 2 | 3.3 ± 4 | 5.2 ± 3 | 6 ± 3 | 6 ± 4 | 5 ± 4 |
| NYHA class III–IV I–II | 13 2 | NA NA | 1 14 | 0 14 | 0 14 | 0 13 | 0 10 |
| Bundle Branch Block Pacemaker | 0 0 | 0 0 | 0 0 | 0 0 | 0 0 | 0 0 | 0 1 |
| ICD | 1 | 0 | 0 | 1 | 0 | 0 | 0 |
| Complex ventricular arrhythmias | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| ICD discharge | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Medication dose reduction | 0 | 0 | 0 | 11 | 10 | 9 | 10 |
| Cardiac death | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Noncardiac death | 0 | 0 | 0 | 1 | 0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Canna, G.; Scarfò, I.; Arendar, I.; Colombo, A.; Torracca, L.; Margonato, D.; Montorfano, M.; Alfieri, O. Targeting Alcohol Septal Ablation in Patients with Obstructive Hypertrophic Cardiomyopathy Candidates for Surgical Myectomy: Added Value of Three-Dimensional Intracoronary Myocardial Contrast Echocardiography. J. Clin. Med. 2021, 10, 2166. https://doi.org/10.3390/jcm10102166
La Canna G, Scarfò I, Arendar I, Colombo A, Torracca L, Margonato D, Montorfano M, Alfieri O. Targeting Alcohol Septal Ablation in Patients with Obstructive Hypertrophic Cardiomyopathy Candidates for Surgical Myectomy: Added Value of Three-Dimensional Intracoronary Myocardial Contrast Echocardiography. Journal of Clinical Medicine. 2021; 10(10):2166. https://doi.org/10.3390/jcm10102166
Chicago/Turabian StyleLa Canna, Giovanni, Iside Scarfò, Irina Arendar, Antonio Colombo, Lucia Torracca, Davide Margonato, Matteo Montorfano, and Ottavio Alfieri. 2021. "Targeting Alcohol Septal Ablation in Patients with Obstructive Hypertrophic Cardiomyopathy Candidates for Surgical Myectomy: Added Value of Three-Dimensional Intracoronary Myocardial Contrast Echocardiography" Journal of Clinical Medicine 10, no. 10: 2166. https://doi.org/10.3390/jcm10102166
APA StyleLa Canna, G., Scarfò, I., Arendar, I., Colombo, A., Torracca, L., Margonato, D., Montorfano, M., & Alfieri, O. (2021). Targeting Alcohol Septal Ablation in Patients with Obstructive Hypertrophic Cardiomyopathy Candidates for Surgical Myectomy: Added Value of Three-Dimensional Intracoronary Myocardial Contrast Echocardiography. Journal of Clinical Medicine, 10(10), 2166. https://doi.org/10.3390/jcm10102166