
The Diagnostic Significance of Ultrasonographic Measurement of the Achilles Tendon Thickness for the Insertional Achilles Tendinopathy in Patients with Heel Pain

 , ,
, ,
Abstract
1. Introduction
2. Methods
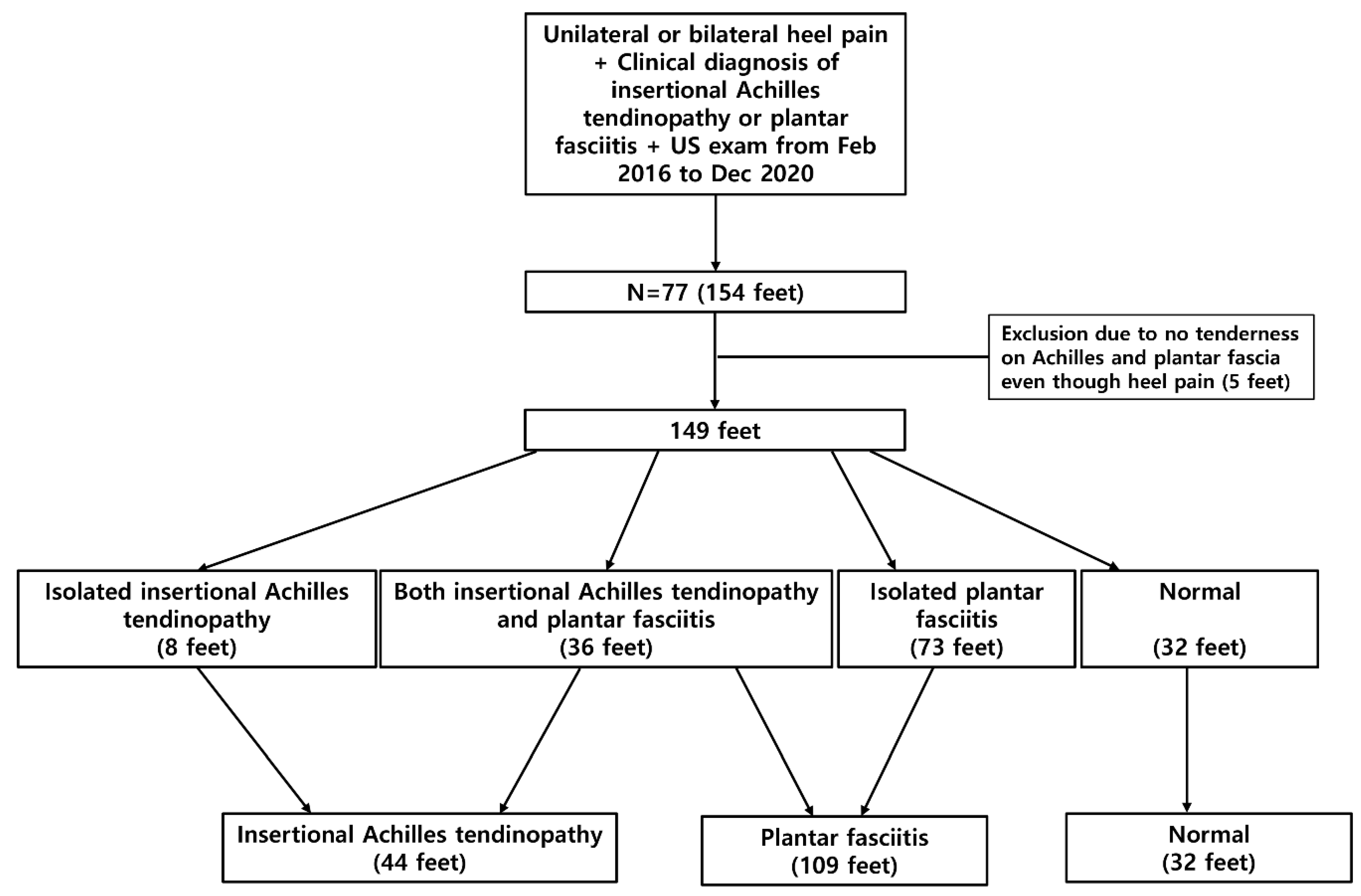
2.1. Subjects
2.2. US and Radiographic Evaluation
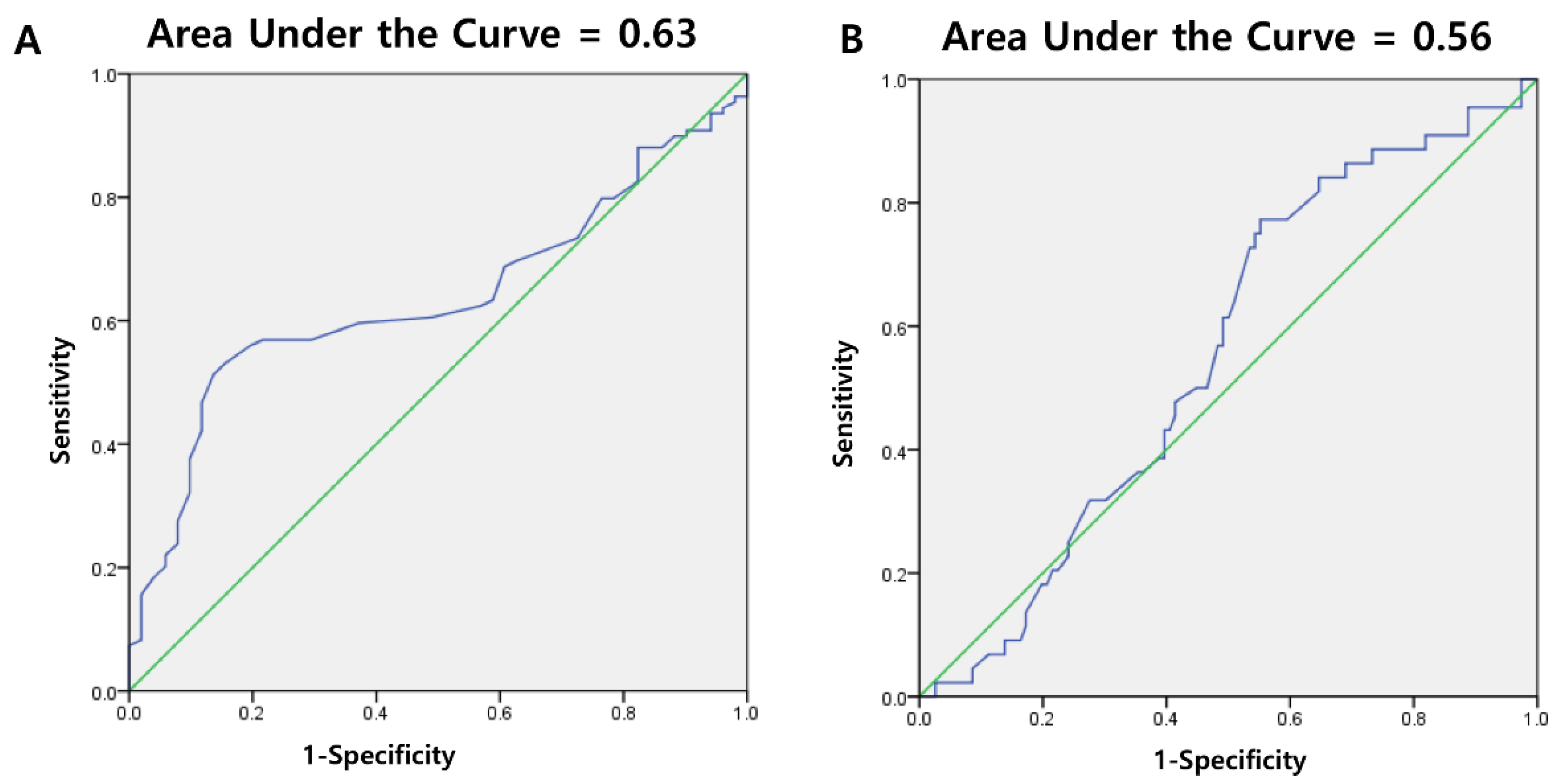
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tu, P. Heel Pain: Diagnosis and Management. Am. Fam. Physician 2018, 97, 86–93. [Google Scholar] [PubMed]
- Mahan, J.; Damodar, D.; Trapana, E.; Barnhill, S.; Nuno, A.U.; Smyth, N.A.; Aiyer, A.; Jose, J. Achilles tendon complex: The anatomy of its insertional footprint on the calcaneus and clinical implications. J. Orthop. 2020, 17, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Kader, D. Tendinopathy of tendo achillis. J. Bone Jt. Surg. Br. 2002, 84, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ramskov, D.; Rasmussen, S.; Sørensen, H.; Parner, E.T.; Lind, M.; Nielsen, R. Progression in Running Intensity or Running Volume and the Development of Specific Injuries in Recreational Runners: Run Clever, a Randomized Trial Using Competing Risks. J. Orthop. Sports Phys. Ther. 2018, 48, 740–748. [Google Scholar] [CrossRef]
- Zabrzyński, J.; Paczesny, Ł.; Zabrzyńska, A.; Grzanka, D.; Łapaj, Ł. Sonography in the instability of the long head of the biceps tendon confronted with histopathologic and arthroscopic findings. Folia Morphol. 2018, 77, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, P.; Jirankali, V.; Garg, S.K. Evaluation of plantar fascia using high-resolution ultrasonography in clinically diagnosed cases of plantar fasciitis. Pol. J. Radiol. 2020, 85, e375–e380. [Google Scholar] [CrossRef] [PubMed]
- McMillan, A.M.; Landorf, K.B.; Barrett, J.T.; Menz, H.B.; Bird, A.R. Diagnostic imaging for chronic plantar heel pain: A systematic review and meta-analysis. J. Foot Ankle Res. 2009, 2, 32. [Google Scholar] [CrossRef]
- Yoon, K.; Kim, S.B.; Park, J.S. Ultrasonographic Findings in Plantar Fasciitis. J. Korean Acad. Rehabil. Med. 2002, 26, 181–186. [Google Scholar]
- Khan, K.M.; Forster, B.B.; Robinson, J.; Cheong, Y.; Louis, L.; Maclean, L.; Taunton, J.E. Are ultrasound and magnetic resonance imaging of value in assessment of Achilles tendon disorders? A two year prospective study. Br. J. Sports Med. 2003, 37, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Richards, P.J.; Dheer, A.K.; McCall, I.M. Achilles tendon (TA) size and power Doppler ultrasound (PD) changes compared to MRI: A preliminary observational study. Clin. Radiol. 2001, 56, 843–850. [Google Scholar] [CrossRef]
- Toumi, H.; Davies, R.; Mazor, M.; Coursier, R.; Best, T.M.; Jennane, R.; Lespessailles, E. Changes in prevalence of calcaneal spurs in men & women: A random population from a trauma clinic. BMC Musculoskelet Disord. 2014, 15, 87. [Google Scholar] [CrossRef]
- Usuelli, F.G.; Di Silvestri, C.A.; D’Ambrosi, R.; Maccario, C.; Tan, E.W. Return to sport activities after medial displacement calcaneal osteotomy and flexor digitorum longus transfer. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 892–896. [Google Scholar] [CrossRef]
- Bakkegaard, M.; Johannsen, F.E.; Højgaard, B.; Langberg, H. Ultrasonography as a prognostic and objective parameter in Achilles tendinopathy: A prospective observational study. Eur. J. Radiol. 2015, 84, 458–462. [Google Scholar] [CrossRef] [PubMed]
- Chimenti, R.L.; Flemister, A.S.; Tome, J.; McMahon, J.M.; Flannery, M.A.; Xue, Y.; Houck, J.R. Altered tendon characteristics and mechanical properties associated with insertional achilles tendinopathy. J. Orthop. Sports Phys. Ther. 2014, 44, 680–689. [Google Scholar] [CrossRef] [PubMed]
- De Jonge, S.; Tol, J.L.; Weir, A.; Waarsing, J.H.; Verhaar, J.A.; de Vos, R.J. The Tendon Structure Returns to Asymptomatic Values in Nonoperatively Treated Achilles Tendinopathy but Is Not Associated with Symptoms: A Prospective Study. Am. J. Sports Med. 2015, 43, 2950–2958. [Google Scholar] [CrossRef] [PubMed]
- Karjalainen, P.T.; Soila, K.; Aronen, H.J.; Pihlajamäki, H.K.; Tynninen, O.; Paavonen, T.; Tirman, P.F. MR imaging of overuse injuries of the Achilles tendon. AJR Am. J. Roentgenol. 2000, 175, 251–260. [Google Scholar] [CrossRef]
- Arya, S.; Kulig, K. Tendinopathy alters mechanical and material properties of the Achilles tendon. J. Appl. Physiol. 2010, 108, 670–675. [Google Scholar] [CrossRef]
- Child, S.; Bryant, A.L.; Clark, R.A.; Crossley, K.M. Mechanical properties of the achilles tendon aponeurosis are altered in athletes with achilles tendinopathy. Am. J. Sports Med. 2010, 38, 1885–1893. [Google Scholar] [CrossRef]
- Chimenti, R.L.; Cychosz, C.C.; Hall, M.M.; Phisitkul, P. Current Concepts Review Update: Insertional Achilles Tendinopathy. Foot Ankle Int. 2017, 38, 1160–1169. [Google Scholar] [CrossRef] [PubMed]
- Kulig, K.; Chang, Y.J.; Winiarski, S.; Bashford, G.R. Ultrasound-Based Tendon Micromorphology Predicts Mechanical Characteristics of Degenerated Tendons. Ultrasound Med. Biol. 2016, 42, 664–673. [Google Scholar] [CrossRef]
- Ooi, C.C.; Schneider, M.E.; Malliaras, P.; Chadwick, M.; Connell, D.A. Diagnostic performance of axial-strain sonoelastography in confirming clinically diagnosed achilles tendinopathy: Comparison with B-mode ultrasound and color Doppler imaging. Ultrasound Med. Biol. 2015, 41, 15–25. [Google Scholar] [CrossRef]
- Wang, H.K.; Lin, K.H.; Su, S.C.; Shih, T.T.; Huang, Y.C. Effects of tendon viscoelasticity in achilles tendinosis on explosive performance and clinical severity in athletes. Scand. J. Med. Sci. Sports 2012, 22, e147–e155. [Google Scholar] [CrossRef]
- Nicholson, C.W.; Berlet, G.C.; Lee, T.H. Prediction of the success of nonoperative treatment of insertional achilles tendinosis based on MRI. Foot Ankle Int. 2007, 28, 472–477. [Google Scholar] [CrossRef]
- Obst, S.J.; Heales, L.J.; Schrader, B.L.; Davis, S.A.; Dodd, K.A.; Holzberger, C.J.; Beavis, L.B.; Barrett, R.S. Are the Mechanical or Material Properties of the Achilles and Patellar Tendons Altered in Tendinopathy? A Systematic Review with Meta-analysis. Sports Med. 2018, 48, 2179–2198. [Google Scholar] [CrossRef] [PubMed]
- Christie, S.; Styn, G., Jr.; Ford, G.; Terryberry, K. Proximal Plantar Intrinsic Tendinopathy: Anatomical and Biomechanical Considerations in Plantar Heel Pain. J. Am. Podiatr. Med. Assoc. 2019, 109, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Soila, K.; Karjalainen, P.T.; Aronen, H.J.; Pihlajamäki, H.K.; Tirman, P.J. High-resolution MR imaging of the asymptomatic Achilles tendon: New observations. AJR Am. J. Roentgenol. 1999, 173, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Pierre-Jerome, C.; Moncayo, V.; Terk, M.R. MRI of the Achilles tendon: A comprehensive review of the anatomy, biomechanics, and imaging of overuse tendinopathies. Acta Radiol. 2010, 51, 438–454. [Google Scholar] [CrossRef] [PubMed]
- Gatz, M.; Bode, D.; Betsch, M.; Quack, V.; Tingart, M.; Kuhl, C.; Schrading, S.; Dirrichs, T. Multimodal Ultrasound Versus MRI for the Diagnosis and Monitoring of Achilles Tendinopathy: A Prospective Longitudinal Study. Orthop. J. Sports Med. 2021, 9. [Google Scholar] [CrossRef]
- Maffulli, N.; Longo, U.G.; Kadakia, A.; Spiezia, F. Achilles tendinopathy. Foot Ankle Surg. 2020, 26, 240–249. [Google Scholar] [CrossRef]
- Khan, K.M.; Cook, J.L.; Kannus, P.; Maffulli, N.; Bonar, S.F. Time to abandon the “tendinitis” myth. BMJ 2002, 324, 626–627. [Google Scholar] [CrossRef]
- Zabrzyński, J.; Gagat, M.; Paczesny, Ł.; Łapaj, Ł.; Grzanka, D. Electron microscope study of the advanced tendinopathy process of the long head of the biceps brachii tendon treated arthroscopically. Folia Morphol. 2018, 77, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Turan, A.; Tufan, A.; Mercan, R.; Teber, M.A.; Tezcan, M.E.; Bitik, B.; Goker, B.; Haznedaroğlu, S. Real-time sonoelastography of Achilles tendon in patients with ankylosing spondylitis. Skeletal. Radiol. 2013, 42, 1113–1118. [Google Scholar] [CrossRef]
- Ermutlu, C.; Aksakal, M.; Gümüştaş, A.; Özkaya, G.; Kovalak, E.; Özkan, Y. Thickness of plantar fascia is not predictive of functional outcome in plantar fasciitis treatment. Acta Orthop. Traumatol. Turc. 2018, 52, 442–446. [Google Scholar] [CrossRef] [PubMed]
- Hansen, L.; Krogh, T.P.; Ellingsen, T.; Bolvig, L.; Fredberg, U. Long-Term Prognosis of Plantar Fasciitis: A 5- to 15-Year Follow-up Study of 174 Patients with Ultrasound Examination. Orthop. J. Sports Med. 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, H.; Yilmaz, E.; Murat, A.; Karakurt, L.; Poyraz, A.K.; Ogur, E. Sonographic evaluation of plantar fasciitis and relation to body mass index. Eur. J. Radiol. 2005, 54, 443–447. [Google Scholar] [CrossRef]
- Park, J.W.; Yoon, K.; Chun, K.S.; Lee, J.Y.; Park, H.J.; Lee, S.Y.; Lee, Y.T. Long-term outcome of low-energy extracorporeal shock wave therapy for plantar fasciitis: Comparative analysis according to ultrasonographic findings. Ann. Rehabil. Med. 2014, 38, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Sabir, N.; Demirlenk, S.; Yagci, B.; Karabulut, N.; Cubukcu, S. Clinical utility of sonography in diagnosing plantar fasciitis. J. Ultrasound Med. 2005, 24, 1041–1048. [Google Scholar] [CrossRef]
- Pang, B.S.; Ying, M. Sonographic measurement of achilles tendons in asymptomatic subjects: Variation with age, body height, and dominance of ankle. J. Ultrasound Med. 2006, 25, 1291–1296. [Google Scholar] [CrossRef]
- Qahtani, M.A.; Mirza, E.H. Thickness of Achilles Tendon is BMI Dependant. J. Coll. Physicians Surg. Pak. 2016, 26, 803–804. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Plantar Fasciitis (n = 109) | Normal (n = 32) | p-Value | |
|---|---|---|---|
| Thickness (mm) | 3.74 ± 1.17 | 3.18 ± 0.75 | 0.032 |
| Abnormal echogenicity (n) | 60 | 2 | <0.001 |
| Cutoff Value (mm) | Sensitivity | Specificity | Youden’s Index |
|---|---|---|---|
| 3.65 | 53.2% | 84.4% | 0.376 |
| 3.75 | 51.4% | 87.5% | 0.389 |
| 3.80 | 48.6% | 90.6% | 0.392 |
| 4.00 | 37.6% | 90.6% | 0.282 |
| Insertional Achilles Tendinopathy (n = 44) | Normal (n = 32) | p-Value | |
|---|---|---|---|
| Thickness (mm) | 4.23 ± 0.67 | 4.01 ± 0.86 | 0.132 |
| Abnormal echogenicity (n) | 20 | 0 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.-H.; Choi, J.-H.; Park, C.-H.; Park, H.-J.; Yoon, K.-J.; Lee, Y.-T. The Diagnostic Significance of Ultrasonographic Measurement of the Achilles Tendon Thickness for the Insertional Achilles Tendinopathy in Patients with Heel Pain. J. Clin. Med. 2021, 10, 2165. https://doi.org/10.3390/jcm10102165
Kim D-H, Choi J-H, Park C-H, Park H-J, Yoon K-J, Lee Y-T. The Diagnostic Significance of Ultrasonographic Measurement of the Achilles Tendon Thickness for the Insertional Achilles Tendinopathy in Patients with Heel Pain. Journal of Clinical Medicine. 2021; 10(10):2165. https://doi.org/10.3390/jcm10102165
Chicago/Turabian StyleKim, Du-Hwan, Jae-Hyeong Choi, Chul-Hyun Park, Hee-Jin Park, Kyung-Jae Yoon, and Yong-Taek Lee. 2021. "The Diagnostic Significance of Ultrasonographic Measurement of the Achilles Tendon Thickness for the Insertional Achilles Tendinopathy in Patients with Heel Pain" Journal of Clinical Medicine 10, no. 10: 2165. https://doi.org/10.3390/jcm10102165
APA StyleKim, D.-H., Choi, J.-H., Park, C.-H., Park, H.-J., Yoon, K.-J., & Lee, Y.-T. (2021). The Diagnostic Significance of Ultrasonographic Measurement of the Achilles Tendon Thickness for the Insertional Achilles Tendinopathy in Patients with Heel Pain. Journal of Clinical Medicine, 10(10), 2165. https://doi.org/10.3390/jcm10102165