
Contrast Associated Acute Kidney Injury and Mortality in Older Adults with Acute Coronary Syndrome: A Pooled Analysis of the FRASER and HULK Studies

 , ,
, ,  , , , , ,
, , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Measurements
2.3. Procedures for CA-AKI Prevention
2.4. Definition of CA-AKI
2.5. Clinical Follow-Up
2.6. Outcomes
2.7. Statistical Analysis
3. Results
3.1. CA-AKI and 3-Month Mortality
3.2. Three-Month Recovery of Renal Functioned in Patients with CA-AKI
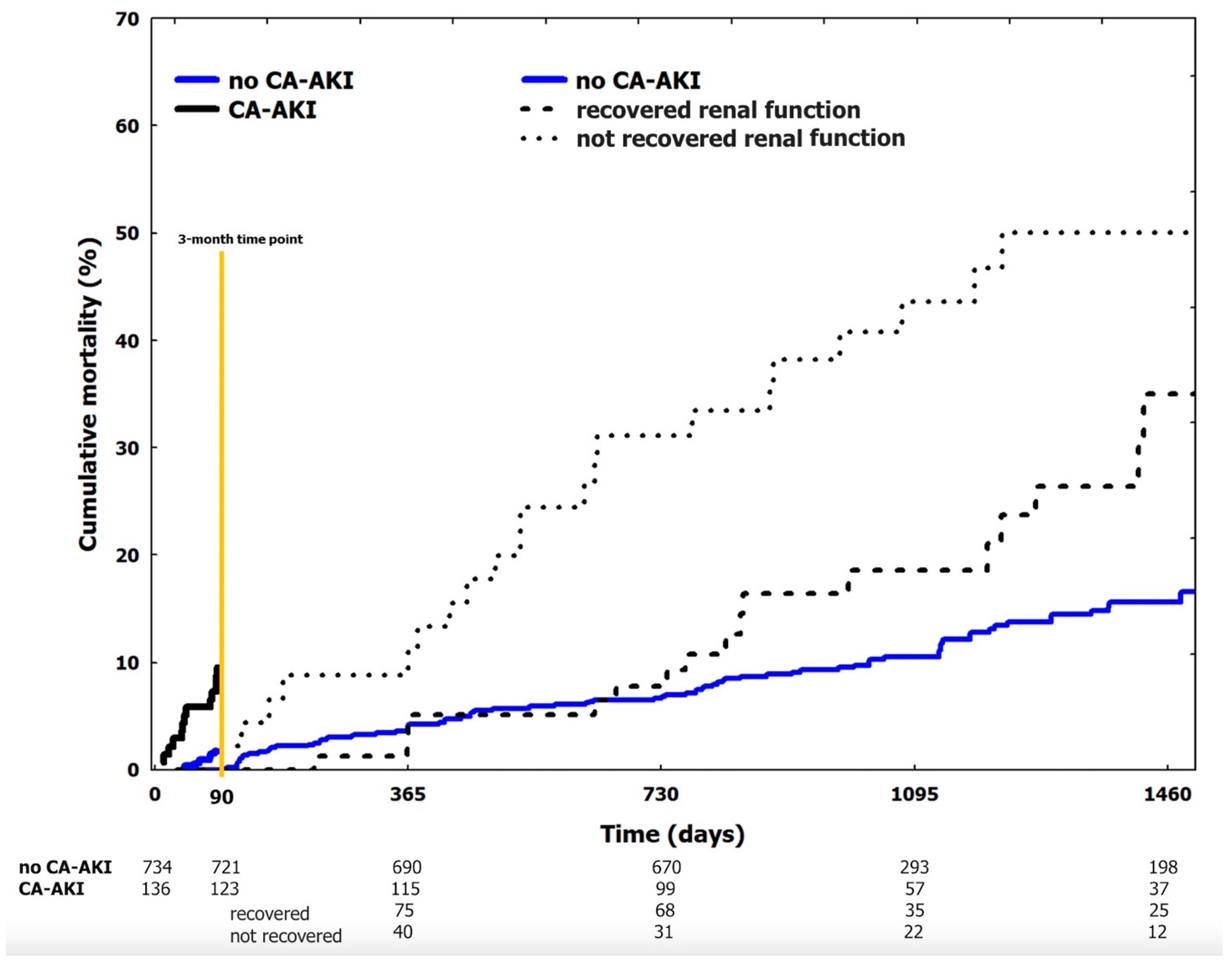
3.3. CA-AKI and Mortality beyond 3-Month Visit
3.4. Predictors of CA-AKI
4. Discussion
- In older adults admitted to hospital for MI and undergoing invasive strategy with PCI, CA-AKI is a frequent complication occurring in 16% (95%CI 13–18%) of patients,
- baseline creatinine clearance, total amount of contrast media higher than the MACD and Mehran risk score emerged as independent predictors of CA-AKI,
- the occurrence of CA-AKI was independently associated with 3-month mortality,
- Among patients with CA-AKI, renal function did not return to baseline values after 3 months in 37% (95%CI 28–46%), and these subjects showed a significantly higher risk of death.
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levy, E.M.; Viscoli, C.M.; Horwitz, R.I. The effect of acute renal failure on mortality: A cohort analysis. JAMA 1996, 275, 1489–1494. [Google Scholar] [CrossRef] [PubMed]
- Solomon, R.J.; Mehran, R.; Natarajan, M.K.; Doucet, S.; Katholi, R.E.; Staniloae, C.S.; Sharma, S.K.; Labinaz, M.; Gelormini, J.L.; Barrett, B.J. Contrast-induced nephropathy and long-term adverse events: Cause and effect? Clin. J. Am. Soc. Nephrol. 2009, 4, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.R.; Malenka, D.J.; DeVries, J.T.; Robb, J.F.; Jayne, J.E.; Friedman, B.J.; Hettleman, B.D.; Niles, N.W.; Kaplan, A.V.; Schoolwerth, A.C.; et al. Transient and persistent renal dysfunction are predictors of survival after percutaneous coronary intervention: Insights from the Dartmouth Dynamic Registry. Catheter. Cardiovasc. Interv. 2008, 72, 347–354. [Google Scholar] [CrossRef]
- Goldenberg, I.; Chonchol, M.; Guetta, V. Reversible acute kidney injury following contrast exposure and the risk of long-term mortality. Am. J. Nephrol. 2009, 29, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Andreis, A.; Budano, C.; Levis, M.; Garrone, P.; Usmiani, T.; D’Ascenzo, F.; De Filippo, O.; D’Amico, M.; Bergamasco, L.; Biancone, L.; et al. Contrast-induced kidney injury: How does it affect long-term cardiac mortality? J. Cardiovasc. Med. (Hagerstown) 2017, 18, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Roghi, A.; Savonitto, S.; Cavallini, C.; Arraiz, G.; Angoli, L.; Castriota, F.; Bernardi, G.; Sansa, M.; De Servi, S.; Pitscheider, W.; et al. Impact of acute renal failure following percutaneous coronary intervention on long-term mortality. J. Cardiovasc. Med. (Hagerstown) 2008, 9, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.T.; Patel, U.D.; Chang, T.I.; Kennedy, K.F.; Masoudi, F.A.; Matheny, M.E.; Kosiborod, M.; Amin, A.P.; Messenger, J.C.; Rumsfeld, J.S.; et al. Contemporary incidence, predictors, and outcomes of acute kidney injury in patients undergoing percutaneous coronary interventions: Insights from the NCDR Cath-PCI registry. JACC Cardiovasc. Interv. 2014, 7, 1–9. [Google Scholar] [CrossRef]
- Rihal, C.S.; Textor, S.C.; Grill, D.E.; Berger, P.B.; Ting, H.H.; Best, P.J.; Singh, M.; Bell, M.R.; Barsness, G.W.; Mathew, V.; et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation 2002, 105, 2259–2264. [Google Scholar] [CrossRef]
- Madhavan, M.V.; Gersh, B.J.; Alexander, K.P.; Granger, C.B.; Stone, G.W. Coronary Artery Disease in Patients ≥80 Years of Age. J. Am. Coll. Cardiol. 2018, 71, 2015–2040. [Google Scholar] [CrossRef]
- Dodson, J.A.; Hajduk, A.; Curtis, J.; Geda, M.; Krumholz, H.M.; Song, X.; Tsang, S.; Blaum, C.; Miller, P.; Parikh, C.R.; et al. Acute Kidney Injury Among Older Patients Undergoing Coronary Angiography for Acute Myocardial Infarction: The SILVER-AMI Study. Am. J. Med. 2019, 132, e817–e826. [Google Scholar] [CrossRef]
- Jacobs, F.M. Iodinated contrast and acute kidney injury: Major culprit or innocent bystander? Time for reappraisal. Crit. Care Med. 2013, 41, 1149. [Google Scholar] [CrossRef] [PubMed]
- Lakhal, K.; Robert-Edan, V.; Ehrmann, S. In the Name of Contrast-Induced Acute Kidney Injury. Chest 2020, 157, 751–752. [Google Scholar] [CrossRef] [PubMed]
- Dauerman, H.L.; Solomon, R.J. Innocent, Guilty, and Acute Kidney Injury. J. Am. Coll. Cardiol. 2020, 75, 1321–1323. [Google Scholar] [CrossRef] [PubMed]
- Pavasini, R.; Maietti, E.; Tonet, E.; Bugani, G.; Tebaldi, M.; Biscaglia, S.; Cimaglia, P.; Serenelli, M.; Ruggiero, R.; Vitali, F.; et al. Bleeding Risk Scores and Scales of Frailty for the Prediction of Haemorrhagic Events in Older Adults with Acute Coronary Syndrome: Insights from the FRASER study. Cardiovasc. Drugs Ther. 2019, 33, 523–532. [Google Scholar] [CrossRef]
- Campo, G.; Pavasini, R.; Maietti, E.; Tonet, E.; Cimaglia, P.; Scillitani, G.; Bugani, G.; Serenelli, M.; Zaraket, F.; Balla, C.; et al. The frailty in elderly patients receiving cardiac interventional procedures (FRASER) program: Rational and design of a multicenter prospective study. Aging Clin. Exp. Res. 2017, 29, 895–903. [Google Scholar] [CrossRef] [PubMed]
- Campo, G.; Maietti, E.; Tonet, E.; Biscaglia, S.; Ariza-Solè, A.; Pavasini, R.; Tebaldi, M.; Cimaglia, P.; Bugani, G.; Serenelli, M.; et al. The Assessment of Scales of Frailty and Physical Performance Improves Prediction of Major Adverse Cardiac Events in Older Adults with Acute Coronary Syndrome. J. Gerontol. A. Biol. Sci. Med. Sci. 2020, 75, 1113–1119. [Google Scholar] [CrossRef]
- Tonet, E.; Maietti, E.; Chiaranda, G.; Vitali, F.; Serenelli, M.; Bugani, G.; Mazzoni, G.; Ruggiero, R.; Myers, J.; Villani, G.Q.; et al. Physical activity intervention for elderly patients with reduced physical performance after acute coronary syndrome (HULK study): Rationale and design of a randomized clinical trial. BMC Cardiovasc. Disord. 2018, 18, 98. [Google Scholar] [CrossRef]
- Campo, G.; Tonet, E.; Chiaranda, G.; Sella, G.; Maietti, E.; Mazzoni, G.; Biscaglia, S.; Pavasini, R.; Myers, J.; Grazzi, G. Exercise Intervention to Improve Functional Capacity in Older Adults After Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2019, 74, 2948–2950. [Google Scholar] [CrossRef]
- Campo, G.; Tonet, E.; Chiaranda, G.; Sella, G.; Maietti, E.; Bugani, G.; Vitali, F.; Serenelli, M.; Mazzoni, G.; Ruggiero, R.; et al. Exercise intervention improves quality of life in older adults after myocardial infarction: Randomised clinical trial. Heart 2020, 106, 1658–1664. [Google Scholar] [CrossRef]
- Mehran, R.; Aymong, E.D.; Nikolsky, E.; Lasic, Z.; Iakovou, I.; Fahy, M.; Mintz, G.S.; Lansky, A.J.; Moses, J.W.; Stone, G.W.; et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: Development and initial validation. J. Am. Coll. Cardiol. 2004, 44, 1393.e9. [Google Scholar]
- Cigarroa, R.G.; Lange, R.A.; Williams, R.H.; Hillis, L.D. Dosing of contrast material to prevent contrast nephropathy in patients with renal disease. Am. J. Med. 1989, 86, 649–652. [Google Scholar] [CrossRef]
- Chawla, L.S.; Bellomo, R.; Bihorac, A.; Goldstein, S.L.; Siew, E.D.; Bagshaw, S.M.; Bittleman, D.; Cruz, D.; Endre, Z.; Fitzgerald, R.L.; et al. Acute kidney disease and renal recovery: Consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat. Rev. Nephrol. 2017, 13, 241–257. [Google Scholar] [CrossRef] [PubMed]
- Weisbord, S.D.; Palevsky, P.M.; Kaufman, J.S.; Wu, H.; Androsenko, M.; Ferguson, R.E.; Parikh, C.R.; Bhatt, D.L.; Gallagher, M.; PRESERVE Trial Investigators. Contrast-Associated Acute Kidney Injury and Serious Adverse Outcomes Following Angiography. J. Am. Coll. Cardiol. 2020, 75, 1311–1320. [Google Scholar] [CrossRef] [PubMed]
- Bartels, E.D.; Brun, G.C.; Gammeltoft, A.; Gjorup, P. Acute anuria following intravenous pyelographyin a patient with myelomatosis. Acta MedScand. 1954, 150, 297–302. [Google Scholar]
- McCullough, P.A.; Choi, J.P.; Feghali, G.A.; Schussler, J.M.; Stoler, R.M.; Vallabahn, R.C.; Mehta, A. Contrast-Induced Acute Kidney Injury. J. Am. Coll. Cardiol. 2016, 68, 1465–1473. [Google Scholar] [CrossRef]
- Wi, J.; Ko, Y.G.; Kim, J.S.; Kim, B.K.; Choi, D.; Ha, J.W.; Hong, M.K.; Jang, Y. Impact of contrast-induced acute kidney injury with transient or persistent renal dysfunction on long-term outcomes of patients with acute myocardial infarction undergoing percutaneous coronary intervention. Heart 2011, 97, 1753–1757. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Pavasini, R.; Biscaglia, S.; Barbato, E.; Tebaldi, M.; Dudek, D.; Escaned, J.; Casella, G.; Santarelli, A.; Guiducci, V.; Gutierrez-Ibanes, E.; et al. Complete revascularization reduces cardiovascular death in patients with ST-segment elevation myocardial infarction and multivessel disease: Systematic review and meta-analysis of randomized clinical trials. Eur. Heart J. 2020, 41, 4103–4110. [Google Scholar] [CrossRef]
- Mehta, S.R.; Wood, D.A.; Storey, R.F.; Mehran, R.; Bainey, K.R.; Nguyen, H.; Meeks, B.; Di Pasquale, G.; López-Sendón, J.; Faxon, D.P.; et al. Complete Revascularization with Multivessel PCI for Myocardial Infarction. N. Engl. J. Med. 2019, 381, 1411–1421. [Google Scholar] [CrossRef]
- Biscaglia, S.; Guiducci, V.; Santarelli, A.; Amat Santos, I.; Fernandez-Aviles, F.; Lanzilotti, V.; Varbella, F.; Fileti, L.; Moreno, R.; Giannini, F.; et al. Physiology-guided revascularization versus optimal medical therapy of nonculprit lesions in elderly patients with myocardial infarction: Rationale and design of the FIRE trial. Am. Heart J. 2020, 229, 100–109. [Google Scholar] [CrossRef]


{kind=link}
| All (n = 870) | 3-Month Renal Function in CA-AKI pts (n = 123) | |||||
|---|---|---|---|---|---|---|
| No CA-AKI (n = 734) | Yes CA-AKI (n = 136) | p | Recovered (n = 78) | Not Recovered (n = 45) | p | |
| Age, (years) | 77 ± 5 | 80 ± 6 | <0.001 | 79 ± 7 | 79 ± 5 | 0.454 |
| Female sex, (%) | 194 (26) | 53 (39) | 0.004 | 29 (37) | 18 (40) | 0.847 |
| BMI, (Kg/m2) | 26 (24–29) | 27 (24–30) | 0.219 | 27 (25–30) | 27 (25–29) | 0.843 |
| Medical history, no. (%) | ||||||
| Diabetes | 221 (30) | 41 (30) | 0.926 | 24 (31) | 13 (29) | 0.987 |
| Hypertension | 599 (82) | 125 (92) | 0.005 | 72 (92) | 40 (89) | 0.528 |
| Hyperlipidemia | 391 (53) | 54 (40) | 0.006 | 35 (45) | 17 (38) | 0.456 |
| Current smoker | 153 (21) | 44 (32) | 0.005 | 26 (33) | 18 (40) | 0.558 |
| MI | 204 (28) | 51 (37) | 0.029 | 31 (39) | 16 (35) | 0.702 |
| PCI | 203 (28) | 37 (27) | 0.997 | 23 (29) | 8 (18) | 0.196 |
| CABG | 75 (10) | 22 (16) | 0.067 | 9 (11) | 12 (16) | 0.045 |
| COPD | 39 (5) | 25 (18) | <0.001 | 17 (22) | 6 (13) | 0.338 |
| PAD | 166 (23) | 46 (34) | 0.007 | 17 (22) | 21 (47) | 0.004 |
| Presentation characteristics | ||||||
| STEMI, no. (%) | 228 (31) | 47 (34) | 0.481 | 27 (35) | 10 (22) | 0.160 |
| Killip class ≥ 2, no. (%) | 65 (9) | 25 (18) | 0.002 | 13 (17) | 7 (16) | 0.901 |
| SBP, mmHg | 135 ± 30 | 133 ± 35 | 0.991 | 133 ± 35 | 134 ± 35 | 0.987 |
| Heart rate, bpm | 85 ± 20 | 89 ± 25 | 0.254 | 90 ± 25 | 88 ± 28 | 0.574 |
| Hypotension * | 30 (4) | 10 (7) | 0.148 | 4 (5) | 4 (9) | 0.663 |
| Anemia † | 318 (43) | 80 (59) | <0.001 | 42 (54) | 27 (60) | 0.635 |
| IABP | 5 (0.7) | 4 (2.9) | <0.001 | 2 (2.5) | 3 (6.6) | 0.524 |
| White blood cells, (u/μL) | 8.8 (7.3–10.5) | 10.9 (8.9–14.5) | <0.001 | 10.7 (8.1–13.2) | 11.2 (8.9–12.9) | 0.664 |
| Hemoglobin, (g/dL) | 12.5 (11–13.8) | 11.2 (9.5–12.8) | <0.001 | 11.6 (9.8–13.1) | 10.8 (9.4–12.7) | 0.288 |
| Albumin, (g/dL) | 3.4 (3.2–3.7) | 3.5 (3.1–3.7) | 0.337 | 3.5 (3.2–3.7) | 3.5 (3.3–3.7) | 0.956 |
| Creatinine Clearance, (mL/min) | 59 (48–73) | 44 (32–54) | <0.001 | 47 (40–61) | 41 (28–48) | 0.007 |
| LVEF, (%) | 50 ± 10 | 49 ± 12 | 0.708 | 53 ± 10 | 49 ± 11 | 0.088 |
| Troponin I at peak, (ng/dL) | 59 (25–84) | 60 (28–85) | 0.734 | 60 (30–90) | 60 (25–88) | 0.977 |
| CK-MB at peak, (ng/dL) | 31 (24–69) | 35 (25–80) | 0.481 | 35 (24–85) | 35 (25–80) | 0.892 |
| Procedural data | ||||||
| Radial access, no. (%) | 705 (96) | 130 (96) | 0.998 | 76 (97) | 43 (96) | 0.879 |
| Multivessel disease, no. (%) | 558 (76) | 102 (75) | 0.883 | 61 (78) | 30 (67) | 0.201 |
| Multivessel PCI, no. (%) | 270 (37) | 57 (42) | 0.299 | 34 (57) | 19 (47) | 0.411 |
| Staged procedure, no. (5) | 110 (15) | 19 (14) | 0.436 | 10 (13) | 6 (13) | 0.895 |
| MACD, (mL) | 355 (299–423) | 280 (223–330) | <0.001 | 293 (256–382) | 267 (199–302) | 0.005 |
| Total contrast media, (mL) | 170 (120–243) | 179 (125–323) | 0.968 | 179 (125–212) | 200 (133–279) | 0.144 |
| Total contrast media > MACD, no. (%) | 34 (5) | 28 (20) | <0.001 | 5 (7) | 18 (43) | <0.001 |
| Mehran score, u. | 8 (5–11) | 10 (8–15) | <0.001 | 9 (6–13) | 11 (8–15) | 0.019 |
| Medical therapy at discharge | ||||||
| ACE-inhibitor | 528 (72) | 63 (46) | <0.001 | 37 (47) | 23 (51) | 0.694 |
| Angiotensin receptor blocker | 127 (17) | 26 (19) | 0.610 | 17 (22) | 7 (16) | 0.408 |
| Beta-blocker | 582 (79) | 108 (79) | 0.923 | 62 (79) | 36 (80) | 0.861 |
| Statin | 667 (91) | 122 (90) | 0.871 | 70 (90) | 40 (89) | 0.963 |
| Diuretic | 236 (32) | 77 (57) | <0.001 | 38 (49) | 28 (62) | 0.148 |
| Univariate | Multivariable | |||||
|---|---|---|---|---|---|---|
| HR | 95%CI | p | HR | 95%CI | p | |
| Age | 1.23 | 1.16–1.31 | <0.001 | 1.20 | 1.08–1.34 | 0.004 |
| Female sex | 3.52 | 1.62–7.63 | 0.001 | |||
| BMI | 1.01 | 0.91–1.35 | 0.841 | |||
| Diabetes | 1.25 | 0.75–1.89 | 0.836 | |||
| Hypertension | 1.07 | 0.71–1.63 | 0.740 | |||
| Hyperlipidemia | 0.89 | 0.65–1.62 | 0.578 | |||
| Current smoker | 1.04 | 0.73–1.48 | 0.827 | |||
| MI | 0.71 | 0.28–1.76 | 0.713 | |||
| PCI | 0.77 | 0.53–1.10 | 0.156 | |||
| CABG | 0.98 | 0.60–1.63 | 0.950 | |||
| COPD | 1.07 | 0.25–4.48 | 0.930 | |||
| PAD | 2.71 | 1.26–5.85 | 0.011 | |||
| STEMI | 6.03 | 2.54–14.2 | <0.001 | |||
| Killip class ≥ 2 | 2.47 | 1.72–3.55 | <0.001 | 2.21 | 1.08–2.84 | 0.032 |
| SBP | 0.99 | 0.97–1.03 | 0.652 | |||
| Heart rate | 1.01 | 0.96–1.06 | 0.783 | |||
| Hypotension | 1.82 | 0.76–4.54 | 0.541 | |||
| Anemia | 1.96 | 1.44–2.68 | <0.001 | 1.51 | 1.01–2.56 | 0.045 |
| IABP | 2.01 | 0.71–5.21 | 0.653 | |||
| White blood cells | 1.07 | 1.02–1.12 | 0.008 | |||
| Hemoglobin | 0.69 | 0.57–0.82 | <0.001 | |||
| Albumin | 0.17 | 0.06–0.48 | <0.001 | |||
| Creatinine Clearance | 0.94 | 0.92–0.96 | <0.001 | |||
| LVEF | 0.92 | 0.88–0.95 | <0.001 | 0.89 | 0.83–0.95 | <0.001 |
| Troponin I at peak | 1.01 | 0.98–1.12 | 0.496 | |||
| CK-MB at peak | 1.01 | 0.89–1.12 | 0.189 | |||
| Radial access | 0.91 | 0.78–1.76 | 0.654 | |||
| Multivessel disease | 1.80 | 1.12–2.50 | 0.016 | |||
| Multivessel PCI | 0.86 | 0.62–1.22 | 0.410 | |||
| ACE-inhibitor | 0.81 | 0.59–1.09 | 0.148 | |||
| Angiotensin receptor blocker | 0.56 | 0.38–1.19 | 0.311 | |||
| Beta-blocker | 0.97 | 0.53–1.49 | 0.442 | |||
| Statin | 0.91 | 0,64–1.78 | 0.645 | |||
| Diuretic | 3.38 | 2.46–4.63 | <0.001 | |||
| CA-AKI | 5.65 | 2.63–12.1 | <0.001 | 3.51 | 1.05–7.01 | 0.039 |
| Univariate Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| OR | 95%CI | p | OR | 95%CI | p | |
| Age, (years) | 1.08 | 1.04–1.11 | <0.001 | 1.01 | 0.94–1.09 | 0.840 |
| Female sex, (%) | 1.78 | 1.21–2.60 | 0.003 | 1.62 | 1.01–2.63 | 0.049 |
| BMI, (Kg/m2) | 1.03 | 0.98–1.08 | 0.248 | |||
| Medical history, no. (%) | ||||||
| Diabetes | 1.01 | 0.67–1.49 | 0.992 | |||
| Hypertension | 2.56 | 1.34–4.88 | 0.004 | 2.03 | 0.95–4.34 | 0.066 |
| Hyperlipidemia | 0.88 | 0.40–1.94 | 0.469 | |||
| Current smoker | 1.51 | 0.72–1.71 | 0.504 | |||
| MI | 1.56 | 1.06–2.29 | 0.023 | 1.22 | 0.74–2.02 | 0.438 |
| PCI | 0.98 | 0.65–1.47 | 0.914 | |||
| CABG | 1.70 | 1.01–2.84 | 0.045 | 2.37 | 0.90–4.63 | 0.101 |
| COPD | 2.01 | 1.34–4.89 | 0.018 | 1.99 | 0.99–3.10 | 0.071 |
| PAD | 1.75 | 1.18–2.60 | 0.009 | 1.85 | 1.04–2.99 | 0.041 |
| Presentation characteristics | ||||||
| STEMI, no. (%) | 1.17 | 0.80–1.73 | 0.421 | |||
| Killip class ≥ 2, no. (%) | 1.63 | 1.24–2.15 | <0.001 | 1.18 | 0.84–1.64 | 0.342 |
| SBP, mmHg | 1.01 | 0.85–1.26 | 0.985 | |||
| Heart rate, bpm | 0.99 | 0.75–1.39 | 0.857 | |||
| White blood cells, (u/μL) | 1.08 | 0.95–1.14 | 0.251 | |||
| Hemoglobin, (g/dL) | 0.79 | 0.71–0.85 | <0.001 | 0.94 | 0.84–1.06 | 0.310 |
| Albumin, (g/dL) | 1.27 | 0.73–2.19 | 0.398 | |||
| Creatinine Clearance, (mL/min) | 0.96 | 0.95–0.97 | <0.001 | 0.98 | 0.96–0.99 | 0.002 |
| LVEF, (%) | 0.99 | 0.98–1.02 | 0.707 | |||
| Procedural data | ||||||
| Radial access, no. (%) | 0.96 | 0.80–1.69 | 0.587 | |||
| Multivessel disease, no. (%) | 0.95 | 0.62–1.45 | 0.798 | |||
| Multivessel PCI, no. (%) | 0.98 | 0.65–1.48 | 0.943 | |||
| Staged procedure, no. (5) | 0.78 | 0.46–1.33 | 0.366 | |||
| Total contrast media, (mL) | 1 | 0.99–1.01 | 0.842 | |||
| Total contrast media > MACD, no. (%) | 4.48 | 2.60–7.71 | <0.001 | 2.32 | 1.18–4.57 | 0.015 |
| Mehran score, u. | 1.16 | 1.01–1.21 | <0.001 | 1.07 | 1.01–1.13 | 0.022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavasini, R.; Tebaldi, M.; Bugani, G.; Tonet, E.; Campana, R.; Cimaglia, P.; Maietti, E.; Grazzi, G.; Pompei, G.; Fabbri, G.; et al. Contrast Associated Acute Kidney Injury and Mortality in Older Adults with Acute Coronary Syndrome: A Pooled Analysis of the FRASER and HULK Studies. J. Clin. Med. 2021, 10, 2151. https://doi.org/10.3390/jcm10102151
Pavasini R, Tebaldi M, Bugani G, Tonet E, Campana R, Cimaglia P, Maietti E, Grazzi G, Pompei G, Fabbri G, et al. Contrast Associated Acute Kidney Injury and Mortality in Older Adults with Acute Coronary Syndrome: A Pooled Analysis of the FRASER and HULK Studies. Journal of Clinical Medicine. 2021; 10(10):2151. https://doi.org/10.3390/jcm10102151
Chicago/Turabian StylePavasini, Rita, Matteo Tebaldi, Giulia Bugani, Elisabetta Tonet, Roberta Campana, Paolo Cimaglia, Elisa Maietti, Giovanni Grazzi, Graziella Pompei, Gioele Fabbri, and et al. 2021. "Contrast Associated Acute Kidney Injury and Mortality in Older Adults with Acute Coronary Syndrome: A Pooled Analysis of the FRASER and HULK Studies" Journal of Clinical Medicine 10, no. 10: 2151. https://doi.org/10.3390/jcm10102151
APA StylePavasini, R., Tebaldi, M., Bugani, G., Tonet, E., Campana, R., Cimaglia, P., Maietti, E., Grazzi, G., Pompei, G., Fabbri, G., Fiorio, A., Rubboli, A., Mazzoni, G., Vitali, F., Serenelli, M., Campo, G., & Biscaglia, S. (2021). Contrast Associated Acute Kidney Injury and Mortality in Older Adults with Acute Coronary Syndrome: A Pooled Analysis of the FRASER and HULK Studies. Journal of Clinical Medicine, 10(10), 2151. https://doi.org/10.3390/jcm10102151