Predictive Value of Estimated Lean Body Mass for Neurological Outcomes after Out-of-Hospital Cardiac Arrest †



Abstract
1. Background
2. Materials and Methods
2.1. Postcardiac Arrest Care and TTM
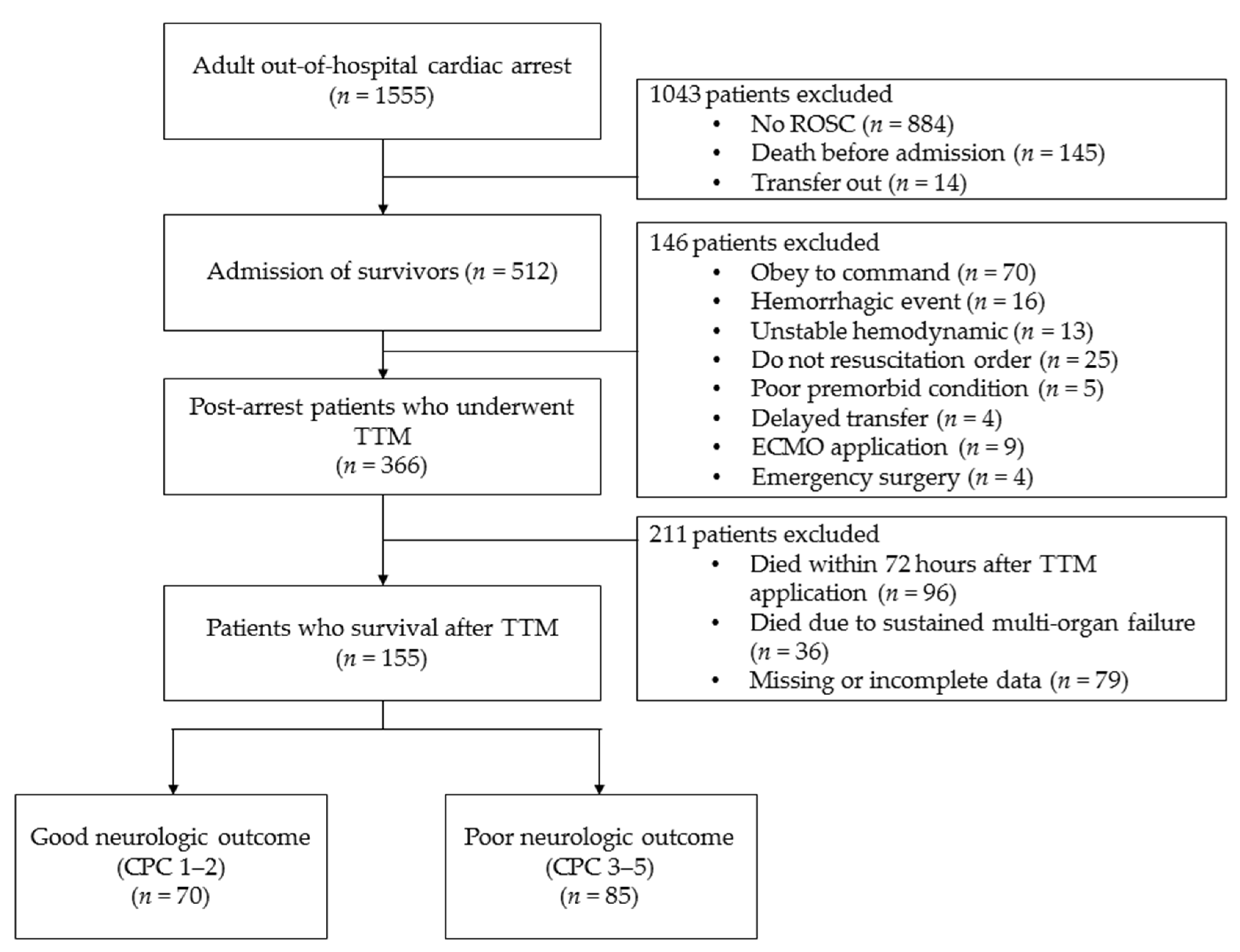
2.2. Enrolled Patients and Study Design
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Patients
3.2. Analysis of Factors Associated with Neurological Outcomes
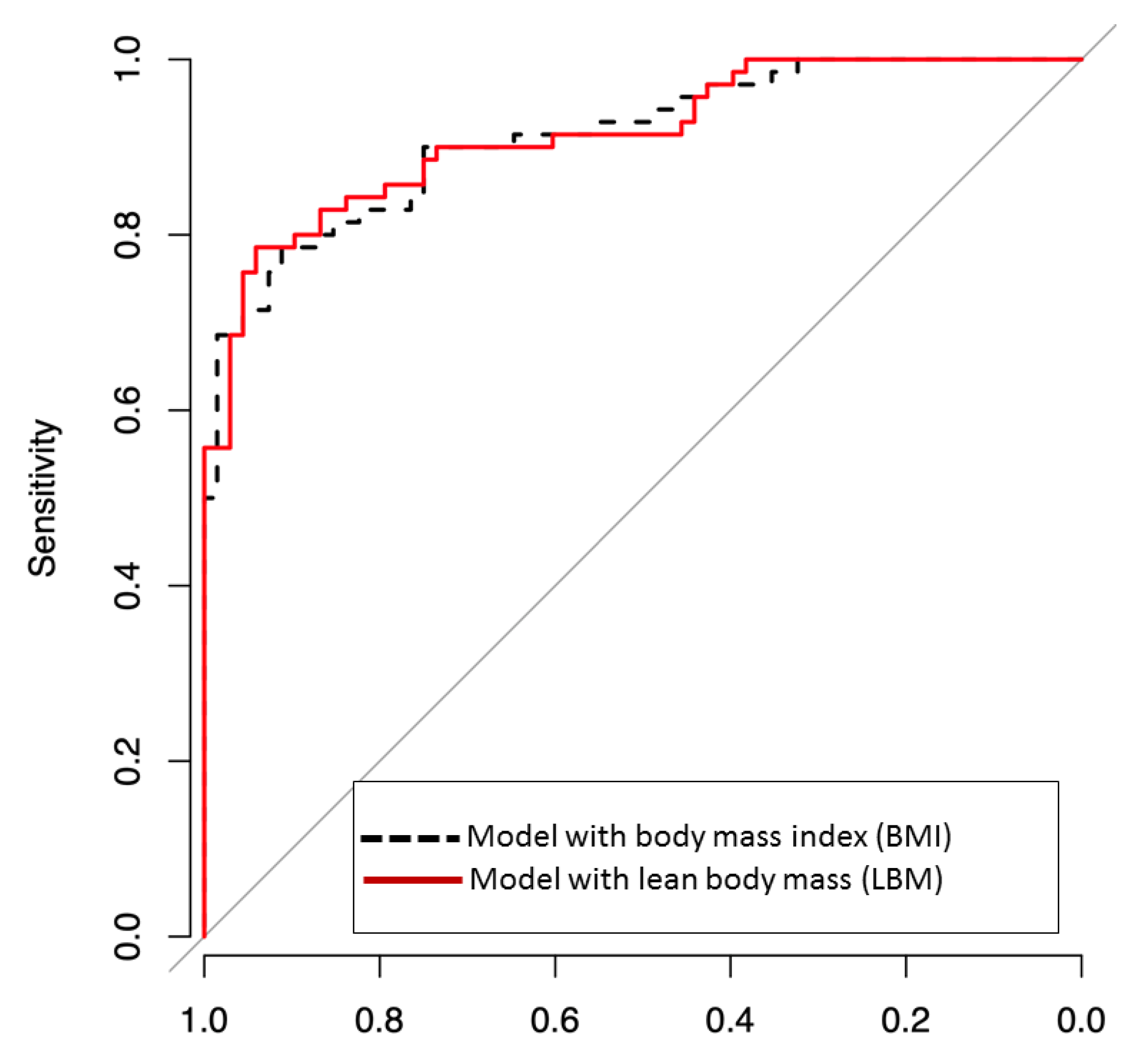
3.3. Prediction of Neurological Outcomes
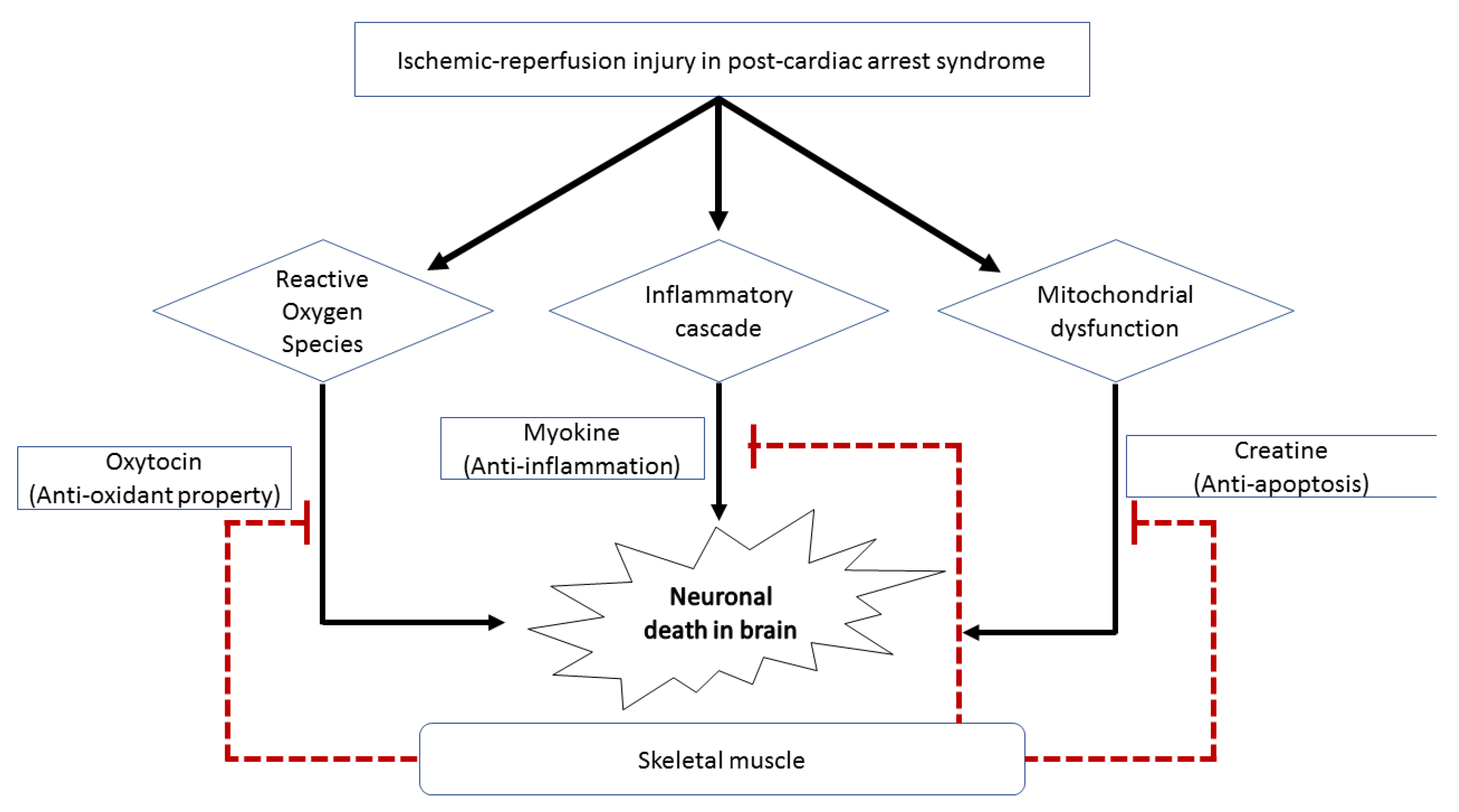
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sandroni, C.; D’Arrigo, S.; Nolan, J.P. Prognostication after cardiac arrest. Crit. Care 2018, 22, 150. [Google Scholar] [CrossRef]
- Yao, Y.; Johnson, N.J.; Perman, S.M.; Ramjee, V.; Grossestreuer, A.V.; Gaieski, D.F. Myocardial dysfunction after out-of-hospital cardiac arrest: Predictors and prognostic implications. Intern. Emerg. Med. 2018, 13, 765–772. [Google Scholar] [CrossRef]
- Van den Brule, J.M.D.; van der Hoeven, J.G.; Hoedemaekers, C.W.E. Cerebral Perfusion and Cerebral Autoregulation after Cardiac Arrest. Biomed. Res. Int. 2018, 2018, 4143636. [Google Scholar] [CrossRef]
- Roberts, B.W.; Trzeciak, S. Systemic inflammatory response after cardiac arrest: Potential target for therapy? Crit. Care Med. 2015, 43, 1336–1337. [Google Scholar] [CrossRef]
- Lavie, C.J.; Alpert, M.A.; Arena, R.; Mehra, M.R.; Milani, R.V.; Ventura, H.O. Impact of Obesity and the Obesity Paradox on Prevalence and Prognosis in Heart Failure. JACC Heart Fail. 2013, 1, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.J.; Zhou, Y.J.; Galper, B.Z.; Gao, F.; Yeh, R.W.; Mauri, L. Association of body mass index with mortality and cardiovascular events for patients with coronary artery disease: A systematic review and meta-analysis. Heart 2015, 101, 1631–1638. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, R.K.; Ezekowitz, J.; Andersson, U.; Alexander, J.H.; Granger, C.B.; Halvorsen, S.; Hanna, M.; Hijazi, Z.; Jansky, P.; Lopes, R.D.; et al. The ‘obesity paradox’ in atrial fibrillation: Observations from the ARISTOTLE (Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation) trial. Eur. Heart J. 2016, 37, 2869–2878. [Google Scholar] [CrossRef] [PubMed]
- Geri, G.; Savary, G.; Legriel, S.; Dumas, F.; Merceron, S.; Varenne, O.; Livarek, B.; Richard, O.; Mira, J.P.; Bedos, J.P.; et al. Influence of body mass index on the prognosis of patients successfully resuscitated from out-of-hospital cardiac arrest treated by therapeutic hypothermia. Resuscitation 2016, 109, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Huang, L.; Zhang, L.; Yu, H.; Liu, B. Association between body mass index and clinical outcomes of patients after cardiac arrest and resuscitation: A meta-analysis. Am. J. Emerg. Med. 2018, 36, 1270–1279. [Google Scholar] [CrossRef] [PubMed]
- Leary, M.; Cinousis, M.J.; Mikkelsen, M.E.; Gaieski, D.F.; Abella, B.S.; Fuchs, B.D. The association of body mass index with time to target temperature and outcomes following post-arrest targeted temperature management. Resuscitation 2014, 85, 244–247. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; McAuley, P.A.; Church, T.S.; Milani, R.V.; Blair, S.N. Obesity and cardiovascular diseases: Implications regarding fitness, fatness, and severity in the obesity paradox. J. Am. Coll. Cardiol. 2014, 63, 1345–1354. [Google Scholar] [CrossRef] [PubMed]
- Hioki, H.; Miura, T.; Motoki, H.; Kobayashi, H.; Kobayashi, M.; Nakajima, H.; Kimura, H.; Mawatari, E.; Akanuma, H.; Sato, T.; et al. Lean body mass index prognostic value for cardiovascular events in patients with coronary artery disease. Heart Asia 2015, 7, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Streja, E.; Rhee, C.M.; SooHoo, M.; Feng, M.; Brunelli, S.M.; Kovesdy, C.P.; Gillen, D.; Kalantar-Zadeh, K.; Chen, J.L. Lean Body Mass and Survival in Hemodialysis Patients and the Roles of Race and Ethnicity. J. Ren. Nutr. 2016, 26, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.W.; Lien, Y.C.; Wu, H.Y.; Yen, C.J.; Pan, C.C.; Hung, T.W.; Su, C.T.; Chiang, C.K.; Cheng, H.T.; Hung, K.Y. Lean Body Mass Predicts Long-Term Survival in Chinese Patients on Peritoneal Dialysis. PLoS ONE 2013, 8, e54976. [Google Scholar] [CrossRef]
- Seo, M.H.; Lee, W.Y.; Kim, S.S.; Kang, J.H.; Kang, J.H.; Kim, K.K.; Kim, B.Y.; Kim, Y.H.; Kim, W.J.; Kim, E.M.; et al. 2018 Korean Society for the Study of Obesity Guideline for the Management of Obesity in Korea. J. Obes. Metab. Syndr. 2019, 28, 40–45. [Google Scholar] [CrossRef]
- Kulkarni, B.; Kuper, H.; Taylor, A.; Wells, J.C.; Radhakrishna, K.V.; Kinra, S.; Ben-Shlomo, Y.; Smith, G.D.; Ebrahim, S.; Byrne, N.M.; et al. Development and validation of anthropometric prediction equations for estimation of lean body mass and appendicular lean soft tissue in Indian men and women. J. Appl. Physiol. 2013, 115, 1156–1162. [Google Scholar] [CrossRef]
- Herzog, C.A.; Ma, J.Z.; Collins, A.J. Poor Long-Term Survival after Acute Myocardial Infarction among Patients on Long-Term Dialysis. N. Engl. J. Med. 1998, 339, 799–805. [Google Scholar] [CrossRef]
- Chae, M.K.; Lee, S.E.; Min, Y.G.; Park, E.J. Initial serum cholesterol level as a potential marker for post cardiac arrest patient outcomes. Resuscitation 2020, 146, 50–55. [Google Scholar] [CrossRef]
- Looijaard, W.; Molinger, J.; Weijs, P.J.M. Measuring and monitoring lean body mass in critical illness. Curr. Opin. Crit. Care 2018, 24, 241–247. [Google Scholar] [CrossRef]
- Lee, M.J.; Kim, E.H.; Bae, S.J.; Choe, J.; Jung, C.H.; Lee, W.J.; Kim, H.K. Protective role of skeletal muscle mass against progression from metabolically healthy to unhealthy phenotype. Clin. Endocrinol. 2019, 90, 102–113. [Google Scholar] [CrossRef]
- Riesberg, L.A.; Weed, S.A.; McDonald, T.L.; Eckerson, J.M.; Drescher, K.M. Beyond muscles: The untapped potential of creatine. Int. Immunopharmacol. 2016, 37, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Perasso, L.; Spallarossa, P.; Gandolfo, C.; Ruggeri, P.; Balestrino, M. Therapeutic Use of Creatine in Brain or Heart Ischemia: Available Data and Future Perspectives. Med. Res. Rev. 2013, 33, 336–363. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Febbraio, M.A. Muscle as an Endocrine Organ: Focus on Muscle-Derived Interleukin-6. Physiol. Rev. 2008, 88, 1379–1406. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Wang, Y.I.; Yang, Y. Neuroprotective effect of interleukin-6 in a rat model of cerebral ischemia. Exp. Ther. Med. 2015, 9, 1695–1701. [Google Scholar] [CrossRef]
- Adamo, S.; Pigna, E.; Lugara, R.; Moresi, V.; Coletti, D.; Bouche, M. Skeletal Muscle: A Significant Novel Neurohypophyseal Hormone-Secreting Organ. Front. Physiol. 2018, 9, 1885. [Google Scholar] [CrossRef]
- Senturk, G.E.; Erkanli, K.; Aydin, U.; Yucel, D.; Isiksacan, N.; Ercan, F.; Arbak, S. The protective effect of oxytocin on ischemia/reperfusion injury in rat urinary bladder. Peptides 2013, 40, 82–88. [Google Scholar] [CrossRef]
- Gonzalez-Reyes, A.; Menaouar, A.; Yip, D.; Danalache, B.; Plante, E.; Noiseux, N.; Gutkowska, J.; Jankowski, M. Molecular mechanisms underlying oxytocin-induced cardiomyocyte protection from simulated ischemia–reperfusion. Mol. Cell. Endocrinol. 2015, 412, 170–181. [Google Scholar] [CrossRef]
- Moghadam, S.E.; Tameh, A.A.; Vahidinia, Z.; Atlasi, M.A.; Bafrani, H.H.; Naderian, H. Neuroprotective Effects of Oxytocin Hormone after an Experimental Stroke Model and the Possible Role of Calpain-1. J. Stroke Cerebrovasc. Dis. 2018, 27, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Fernando, R.; Drescher, C.; Nowotny, K.; Grune, T.; Castro, J.P. Impaired proteostasis during skeletal muscle aging. Free Radic. Biol. Med. 2019, 132, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Hume, R. Prediction of lean body mass from height and weight. J. Clin. Pathol. 1966, 19, 389–391. [Google Scholar] [CrossRef] [PubMed]
- De Branco, F.M.S.; de Paula, A.L.B.; Rossato, L.T.; Barreiro, S.M.; Nahas, P.C.; Murta, E.F.C.; Orsatti, F.L.; de Oliveira, E.P. Comparison of predictive equations of lean mass in young and postmenopausal women. Clin. Nutr. ESPEN 2018, 24, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Moisey, L.L.; Mourtzakis, M.; Kozar, R.A.; Compher, C.; Heyland, D.K. Existing equations to estimate lean body mass are not accurate in the critically ill: Results of a multicenter observational study. Clin. Nutr. 2017, 36, 1701–1706. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Good CPC (n = 70) | Poor CPC (n = 85) | p-Value | |
|---|---|---|---|
| Patient characteristics | |||
| Age, (mean) years | 50.34 (±13.03) | 58.14 (±16.02) | <0.01 |
| Female, n (%) | 14 (20.00) | 29 (34.12) | 0.08 |
| Height, (mean) cm | 171.30 (±7.59) | 165.44 (±8.22) | <0.01 |
| Weight, (mean) kg | 70.40 (±13.91) | 60.86 (±13.29) | <0.01 |
| Known prearrest health conditions | |||
| Diabetes mellitus, n (%) | 16 (22.86) | 26 (30.59) | 0.37 |
| Hypertension, n (%) | 25 (35.71) | 40 (47.06) | 0.06 |
| Resuscitation factors | |||
| Witnessed cardiac arrest, n (%) | 60 (85.71) | 65 (76.47) | 0.34 |
| Bystander CPR, n (%) | 50 (71.43) | 59 (69.41) | 0.58 |
| Initial shockable rhythm, n (%) | 55 (78.57) | 10 (11.76) | <0.01 |
| No-flow time, min (IQR) | 2.74 (0.00–4.00) | 6.14 (0.00–10.00) | 0.02 |
| Total CPR time, mean | 20.03 (±12.26) | 29.54 (±17.83) | <0.01 |
| Out of hospital BLS time, min | 15.37 (±10.95) | 20.64 (±12.58) | 0.01 |
| ACLS time after hospital arrival, min (IQR) | 4.63 (0–4.00) | 9.45 (4.00–12.00) | <0.01 |
| Use of AED, n (%) | 59 (84.29) | 23 (27.06) | <0.01 |
| TTM factors | |||
| TTM method, n (%) | 0.16 | ||
| Gel pads with feedback loop | 62 (87.27) | 69 (81.18) | |
| Intravascular cooling with feedback loop | 5 (7.14) | 5 (5.88) | |
| Cooling water blanket | 3 (4.29) | 11 (12.94) | |
| Target temperature, n (%) | 0.70 | ||
| From 32 to 34 °C | 58 (82.86) | 74 (87.06) | |
| From 35 to 37 °C | 12 (17.14) | 11 (12.94) | |
| Body-weight-related index | |||
| BMI, mean | 24.35 (±4.10) | 22.44 (±4.59) | <0.01 |
| Underweight (<18.50), n (%) | 3 (4.29) | 13 (15.29) | <0.01 |
| Normal (18.50–22.99), n (%) | 25 (35.71) | 40 (47.06) | |
| Overweight (23.00–24.99), n (%) | 13 (18.57) | 18 (21.18) | |
| Obese (≥25.00), n (%) | 29 (41.43) | 14 (16.47) | |
| LBM, mean | 48.90 (±9.21) | 42.64 (±10.74) | <0.01 |
| Level 1 (<32.71), n (%) | 6 (8.58) | 21 (24.71) | <0.01 |
| Level 2 (32.72–44.17), n (%) | 12 (17.14) | 23 (27.06) | |
| Level 3 (44.18–48.97), n (%) | 11 (15.71) | 21 (24.71) | |
| Level 4 (≥48.98), n (%) | 41 (58.57) | 20 (23.53) |
| Univariate OR (95% CI) | p-Value | Multivariate OR (95% CI), Model Including BMI e | p Value | Multivariate OR (95% CI), Model Including LBM f | p-Value | |
|---|---|---|---|---|---|---|
| Age | 0.96 (0.94–0.98) | <0.01 | 0.96 (0.93–0.99) | 0.02 | 0.96 (0.92–0.99) | 0.03 |
| Initial shockable rhythm | 27.50 (11.97–69.18) | <0.01 | 18.32 (5.04–79.17) | <0.01 | 17.38 (4.64–70.27) | <0.01 |
| No-flow time a | 0.93 (0.87–0.98) | 0.01 | 0.96 (0.88–1.02) | 0.24 | 0.96 (0.89–1.03) | 0.30 |
| Total CPR time b | 0.95 (0.93–0.97) | <0.01 | 0.96 (0.92–0.99) | 0.01 | 0.95 (0.91–0.98) | 0.01 |
| Use of AED | 13.53 (6.25–31.51) | <0.01 | 1.39 (0.33–5.27) | 0.63 | 1.59 (0.38–6.03) | 0.51 |
| BMI (Cont.) | 1.13 (1.04–1.25) | <0.01 | 1.10 (0.98–1.25) | 0.13 | ||
| BMI c | ||||||
| Underweight (<18.50) | 0.37 (0.07–1.28) | 0.15 | 0.40 (0.04–3.39) | 0.44 | - | - |
| Normal (18.50–22.99) | 1 | 1 | 1 | 1 | - | - |
| Overweight (23.00–24.99) | 1.16 (0.48–2.76) | 0.74 | 1.96 (0.56–7.12) | 0.30 | - | - |
| Obese (≥25.00) | 3.31 (1.50–7.62) | <0.01 | 3.27 (1.04–11.07) | 0.04 | - | - |
| LBM (Cont.) | 1.07 (1.03–1.11) | <0.01 | 1.05 (0.99–1.10) | 0.09 | ||
| LBM d | ||||||
| Level 1 (<32.71) | 1 | 1 | - | - | 1 | 1 |
| Level 2 (32.72–44.17) | 1.82 (0.60–6.06) | 0.30 | - | - | 1.31 (0.25–7.37) | 0.75 |
| Level 3 (44.18–48.97) | 1.83 (0.59–6.18) | 0.31 | - | - | 9.85 (0.18–5.52) | 0.98 |
| Level 4 (≥48.98) | 7.18 (2.63–22.17) | <0.01 | - | - | 4.81 (1.10–25.55) | 0.04 |
- a No-flow time: time from collapse to administration of resuscitation
- b Total CPR time: time from administration of resuscitation to return of spontaneous circulation (BLS time + ACLS time)
- c Normal body mass index group as reference group.
- d Lowest lean body mass group as reference group.
- e Hosmer–Lemeshow X squared = 6.95, df = 8, p-value = 0.541, indicating good model fit. Hosmer and Lemeshow test (binary model).
- f Hosmer–Lemeshow X squared = 9.77, df = 8, p-value = 0.281, indicating good model fit. Hosmer and Lemeshow test (binary model).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.E.; Kim, H.H.; Chae, M.K.; Park, E.J.; Choi, S. Predictive Value of Estimated Lean Body Mass for Neurological Outcomes after Out-of-Hospital Cardiac Arrest. J. Clin. Med. 2021, 10, 71. https://doi.org/10.3390/jcm10010071
Lee SE, Kim HH, Chae MK, Park EJ, Choi S. Predictive Value of Estimated Lean Body Mass for Neurological Outcomes after Out-of-Hospital Cardiac Arrest. Journal of Clinical Medicine. 2021; 10(1):71. https://doi.org/10.3390/jcm10010071
Chicago/Turabian StyleLee, Sung Eun, Hyuk Hoon Kim, Minjung Kathy Chae, Eun Jung Park, and Sangchun Choi. 2021. "Predictive Value of Estimated Lean Body Mass for Neurological Outcomes after Out-of-Hospital Cardiac Arrest" Journal of Clinical Medicine 10, no. 1: 71. https://doi.org/10.3390/jcm10010071
APA StyleLee, S. E., Kim, H. H., Chae, M. K., Park, E. J., & Choi, S. (2021). Predictive Value of Estimated Lean Body Mass for Neurological Outcomes after Out-of-Hospital Cardiac Arrest. Journal of Clinical Medicine, 10(1), 71. https://doi.org/10.3390/jcm10010071