
Dialysis Membranes for Acute Kidney Injury

 ,
, 


 , ,
, ,
Abstract
1. Introduction
2. Uremic Toxins
2.1. Small Water-Soluble Uremic Toxins
2.2. Middle Molecules
2.3. Protein-Bound Uremic Toxins
3. Dialysis Membrane
3.1. Low-Flux Membrane
3.2. High-Flux Membrane
4. Haemofiltration and Haemodiafiltration
5. Adsorptive Membrane/Sorbent
5.1. Sorbent in Haemodialysis
5.2. Haemoperfusion
6. Roles in Removing Cytokines and Endotoxins
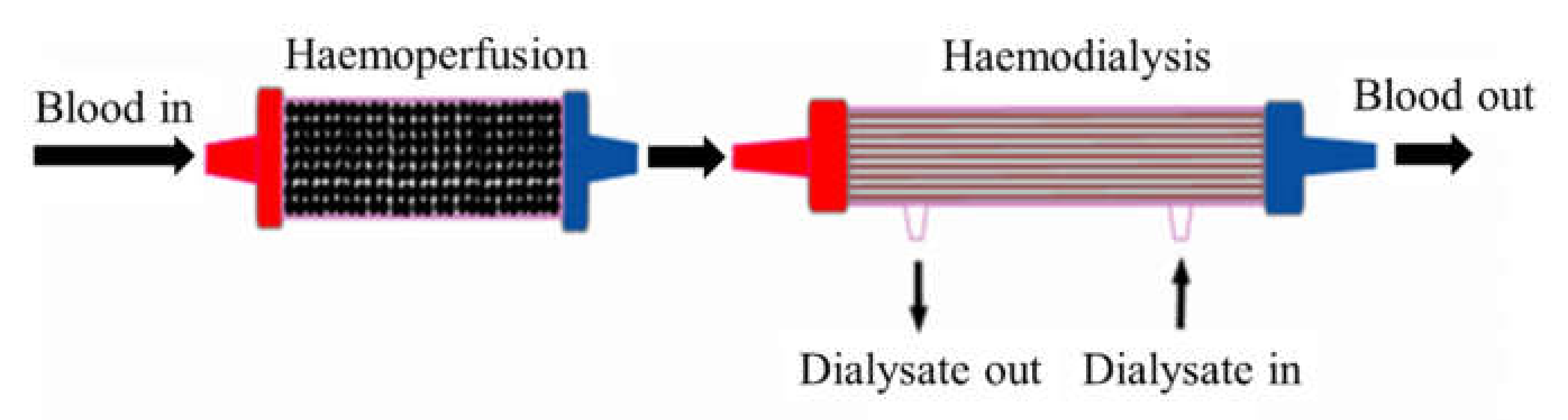
7. Combination of Haemodialysis and Haemoperfusion
8. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- De, S.; Roy, A. Hemodialysis Membranes, for Engineers to Medical Practitioners; CRC Press Taylor & Francis Group: London, UK; New York, NY, USA, 2017. [Google Scholar]
- Lopes, J.A.; Jorge, S. The RIFLE and AKIN Classifications for Acute Kidney Injury: A Critical and Comprehensive Review. Clin. Kidney J. 2013, 6, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Palevsky, P.M.; Liu, K.D.; Brophy, P.D.; Chawla, L.S.; Parikh, C.R.; Thakar, C.V.; Tolwani, A.J.; Waikar, S.S.; Weisbord, S.D. KDOQI US Commentary on the 2012 KDIGO Clinical Practice Guideline for Acute Kidney Injury. Am. J. Kidney Dis. 2013, 61, 649–672. [Google Scholar] [CrossRef] [PubMed]
- Dirkes, S. Acute Kidney Injury: Not Just Acute Renal Failure Anymore? Crit. Care Nurse 2011, 31, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an Initiative to Improve Outcomes in Acute Kidney Injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef]
- Glorieux, G.; Tattersall, J. Uraemic Toxins and New Methods to Control Their Accumulation: Game Changers for the Concept of Dialysis Adequacy. Clin. Kidney J. 2015, 8, 353–362. [Google Scholar] [CrossRef]
- Vanholder, R.; Smet, R.D.; Glorieux, G.; Argiles, A.; Baur eister, U.; Brunet, P.; Clark, W.; Cohen, G.; Deyn, P.P.D.; Deppisch, R.; et al. Review on Uremic Toxins: Classification, Concentration, and Interindividual Variability. Kidney Int. 2003, 63, 1934–1943. [Google Scholar] [CrossRef]
- Yamamoto, S.; Kazama, J.J.; Wakamatsu, T.; Takahashi, Y.; Kaneko, Y.; Goto, S.; Narita, I. Removal of Uremic Toxins by Renal Replacement Therapies: A Review of Current Progress and Future Perspectives. Ren. Replace Ther. 2016, 2, 43. [Google Scholar] [CrossRef]
- Cui, Z.F.; Muralidhara, H.S. Membrane Technology-A Practical Guide to Membrane Technology and Applications in Food and Bioprocessing; Elsevier: Burlington, MA, USA, 2010. [Google Scholar]
- Sakai, K. Determination of Pore Size and Pore Size Distribution: 2. Dialysis Membrane. J. Memb. Sci. 1994, 96, 91–130. [Google Scholar] [CrossRef]
- Baker, R.W. Membrane Technology and Applications; John Wiley & Sons: West Sussex, UK, 2004. [Google Scholar]
- Gautham, A.; Muhammed, J.M.; Manavalan, M.; Najeb, M. A Hemodialysis Membranes: Past, Present and Future Trends. Int. Res. J. Pharm. 2013, 4, 16–19. [Google Scholar] [CrossRef]
- Hoenich, N.A. Update on the Biocompatibility of Hemodialysis Membranes. Hong Kong J. Nephrol. 2004, 6, 74–78. [Google Scholar] [CrossRef]
- Zhang, Q.; Lu, X.; Zhao, L. Preparation of Polyvinylidene Fluoride (PVDF) Hollow Fiber Hemodialysis Membranes. Membranes 2014, 4, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, V.; Gupte, O. Functionalization of Poly (Ether Sulfone) (PES) and Polysulfone (PSF) Membrane Case Studies and Discussion. Bombay Technol. 2014, 64, 22–26. [Google Scholar]
- Mansur, S.; Othman, M.H.D.; Ismail, A.F.; Sheikh Abdul Kadir, S.H.; Kamal, F.; Goh, P.S.; Hasbullah, H.; Ng, B.C.; Abdullah, M.S. Investigation on the Effect of Spinning Conditions on the Properties of Hollow Fiber Membrane for Hemodialysis Application. J. Appl. Polym. Sci. 2016, 133, 1–10. [Google Scholar] [CrossRef]
- Ronco, C.; Cruz, D. Hemodialysis—From Basic Research to Clinical Trials; Karger: Basel, Switzerland, 2008. [Google Scholar]
- Hayama, M.; Yamamoto, K.I.; Kohori, F.; Sakai, K. How Polysulfone Dialysis Membranes Containing Polyvinylpyrrolidone Achieve Excellent Biocompatibility? J. Memb. Sci. 2004, 234, 41–49. [Google Scholar] [CrossRef]
- Zhao, C.; Xue, J.; Ran, F.; Sun, S. Modification of Polyethersulfone Membranes—A Review of Methods. Prog. Mater. Sci. 2013, 58, 76–150. [Google Scholar] [CrossRef]
- Dahe, G.J.; Teotia, R.S.; Kadam, S.S.; Bellare, J.R. The Biocompatibility and Separation Performance of Antioxidative Polysulfone/Vitamin E TPGS Composite Hollow Fiber Membranes. Biomaterials 2011, 32, 352–365. [Google Scholar] [CrossRef]
- Hoffman, R.; Nyu, N.; Holubek, W.J.; Hoffman, R.S.; Goldfarb, D.S.; Nelson, L.S. Use of Hemodialysis and Hemoperfusion in Poisoned Patients Use of Hemodialysis and Hemoperfusion in Poisoned Patients. Kidney Int. 2008, 74, 1327–1334. [Google Scholar] [CrossRef]
- Raharjo, Y.; Ismail, A.F.; Dzarfan Othman, M.H.; Rosid, S.M.; Azali, M.A.; Santoso, D. Effect of Polymer Loading on Membrane Properties and Uremic Toxins Removal for Hemodialysis Application. J. Membr. Sci. Res. 2021, 7, 14–19. [Google Scholar] [CrossRef]
- Waheed, H.; Hussain, A. Effect of Polyvinyl Pyrolidone on Morphology and Performance of Cellulose Acetate Based Dialysis Membrane. Eng. Technol. Appl. Sci. Res. 2019, 9, 3744–3749. [Google Scholar] [CrossRef]
- Mansur, S.; Othman, M.H.D.; Ismail, A.F.; Zainol Abidin, M.N.; Said, N.; Sean, G.P.; Hasbullah, H.; Sheikh Abdul Kadir, S.H.; Kamal, F. Study on the Effect of Spinning Conditions on the Performance of PSf/PVP Ultrafiltration Hollow Fiber Membrane. Malays. J. Fundam. Appl. Sci. 2018, 14, 343–347. [Google Scholar] [CrossRef]
- Bergé-Lefranc, D.; Vagner, C.; Schäf, O.; Boulet, P.; Pizzala, H.; Paillaud, J.L.; Denoyel, R. Adsorption of Small Uremic Toxin Molecules onto Zeolites: A First Step towards an Alternative Kidney. Stud. Surf. Sci. Catal. 2007, 170, 1015–1020. [Google Scholar] [CrossRef]
- Wernert, V.; Schäf, O.; Ghobarkar, H.; Denoyel, R. Adsorption Properties of Zeolites for Artificial Kidney Applications. Microporous Mesoporous Mater. 2005, 83, 101–113. [Google Scholar] [CrossRef]
- Lu, L.; Yeow, J.T.W. An Adsorption Study of Indoxyl Sulfate by Zeolites and Polyethersulfone—Zeolite Composite Membranes. Mater. Des. 2017, 120, 328–335. [Google Scholar] [CrossRef]
- Bergé-Lefranc, D.; Pizzala, H.; Paillaud, J.L.; Schäf, O.; Vagner, C.; Boulet, P.; Kuchta, B.; Denoyel, R. Adsorption of Small Uremic Toxin Molecules on MFI Type Zeolites from Aqueous Solution. Adsorption 2008, 14, 377–387. [Google Scholar] [CrossRef]
- Sun, J.; Wu, L. Polyether Sulfone/Hydroxyapatite Mixed Matrix Membranes for Protein Purification. Appl. Surf. Sci. 2014, 308, 155–160. [Google Scholar] [CrossRef]
- Guo, C.; Zhou, L.; Lv, J. Effects of Expandable Graphite and Modified Ammonium Polyphosphate on the Flame-Retardant and Mechanical Properties of Wood Flour-Polypropylene Composites. Polym. Polym. Compos. 2013, 21, 449–456. [Google Scholar] [CrossRef]
- Su, B.H.; Fu, P.; Li, Q.; Tao, Y.; Li, Z.; Zao, H.S.; Zhao, C.S. Evaluation of Polyethersulfone Highflux Hemodialysis Membrane in Vitro and in Vivo. J. Mater. Sci. Mater. Med. 2008, 19, 745–751. [Google Scholar] [CrossRef]
- Clark, W.R.; Gao, D. Properties of Membranes Used for Hemodialysis Therapy. Semin. Dial. 2002, 15, 191–195. [Google Scholar] [CrossRef]
- Huang, J.; Zhang, K.; Wang, K.; Xie, Z.; Ladewig, B.; Wang, H. Fabrication of Polyethersulfone-Mesoporous Silica Nanocomposite Ultrafiltration Membranes with Antifouling Properties. J. Memb. Sci. 2012, 423–424, 362–370. [Google Scholar] [CrossRef]
- Vilar, E.; Farrington, K. Haemodialysis. Medicine 2011, 39, 429–433. [Google Scholar] [CrossRef]
- Oshvandi, K.; Kavyannejad, R.; Borzuo, S.R.; Gholyaf, M. High-Flux and Low-Flux Membranes: Efficacy in Hemodialysis. Nurs. Midwifery Stud. 2014, 3, e21764. [Google Scholar] [CrossRef] [PubMed]
- Saiful, S. Mixed Matrix Membrane Adsorbers for Protein and Blood Purification; University of Twente: Enschede, The Netherlands, 2007. [Google Scholar]
- Nissenson, A.R.; Fine, R.N. Handbook of Dialysis Therapy, 4th ed.; Elsevier: Philadelphia, PA, USA, 2008. [Google Scholar] [CrossRef]
- Lonnemann, G. The Quality of Dialysate: An Integrated Approach. Kidney Int. Suppl. 2000, 58, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Su, B.; Sun, S.; Zhao, C. Polyethersulfone Hollow Fiber Membranes for Hemodialysis. Prog. Hemodial. Emergent Biotechnol. Clin. Pract. 2011, 1, 65–92. [Google Scholar] [CrossRef]
- Yu, X.; Shen, L.; Zhu, Y.; Li, X.; Yang, Y.; Wang, X.; Zhu, M.; Hsiao, B.S. High Performance Thin-Film Nanofibrous Composite Hemodialysis Membranes with Efficient Middle-Molecule Uremic Toxin Removal. J. Memb. Sci. 2017, 523, 173–184. [Google Scholar] [CrossRef]
- Mortada, W.I.; Nabieh, K.A.; Donia, A.F.; Ismail, A.M.; Kenawy, I.M.M. Impact of Dialyzer Membrane Flux on Metal Clearance in Hemodialysis Patients. J. Trace Elem. Med. Biol. 2016, 36, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Eknoyan, G.; Beck, G.J.; Cheung, A.K.; Daugirdas, J.T.; Greene, T.; Kusek, J.W.; Allon, M.; Bailey, J.; Delmez, J.A.; Depner, T.A.; et al. Effect of Dialysis Dose and Membrane Flux in Maintenance Hemodialysis. N. Engl. J. Med. 2002, 347, 2010–2019. [Google Scholar] [CrossRef] [PubMed]
- Boure, T. Which Dialyser Membrane to Choose? Nephrol. Dial. Transplant. 2004, 19, 293–296. [Google Scholar] [CrossRef]
- Tsimihodimos, V.; Mitrogianni, Z.; Elisaf, M. Dyslipidemia Associated with Chronic Kidney Disease. Open Cardiovas. Med. J. 2011, 5, 41–48. [Google Scholar] [CrossRef]
- Raharjo, Y.; Ismail, A.F.; Othman, M.H.D.; Malek, N.A.N.N.; Santoso, D. Preparation and Characterization of Imprinted Zeolite-Y for p-Cresol Removal in Haemodialysis. Mater. Sci. Eng. C 2019, 103, 109722. [Google Scholar] [CrossRef]
- Villa, G.; Zaragoza, J.J.; Sharma, A.; Neri, M.; De Gaudio, A.R.; Ronco, C. Cytokine Removal with High Cut-off Membrane: Review of Literature. Blood Purif. 2014, 38, 167–173. [Google Scholar] [CrossRef]
- Tijink, M.S.L.; Wester, M.; Sun, J.; Saris, A.; Bolhuis-Versteeg, L.A.M.; Saiful, S.; Joles, J.A.; Borneman, Z.; Wessling, M.; Stamatialis, D.F. A Novel Approach for Blood Purification: Mixed-Matrix Membranes Combining Diffusion and Adsorption in One Step. Acta Biomater. 2012, 8, 2279–2287. [Google Scholar] [CrossRef] [PubMed]
- Tijink, M.S.L.; Wester, M.; Glorieux, G.; Gerritsen, K.G.F.; Sun, J.; Swart, P.C.; Borneman, Z.; Wessling, M.; Vanholder, R.; Joles, J.A.; et al. Mixed Matrix Hollow Fiber Membranes for Removal of Protein-Bound Toxins from Human Plasma. Biomaterials 2013, 34, 7819–7828. [Google Scholar] [CrossRef] [PubMed]
- Pavlenko, D.; van Geffen, E.; van Steenbergen, M.J.; Glorieux, G.; Vanholder, R.; Gerritsen, K.G.F.; Stamatialis, D. New Low-Flux Mixed Matrix Membranes That Offer Superior Removal of Protein-Bound Toxins from Human Plasma. Sci. Rep. 2016, 6, 34429. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Miyake, T.; Kitamura, N.; Tani, M.; Endo, Y. Endotoxin Adsorption: Direct Hemoperfusion with the Polymyxin B-Immobilized Fiber Column (PMX). Transfus. Apher. Sci. 2017, 56, 682–688. [Google Scholar] [CrossRef]
- Saiful; Borneman, Z.; Wessling, M. Double Layer Mixed Matrix Membrane Adsorbers Improving Capacity and Safety Hemodialysis. IOP Conf. Ser. Mater. Sci. Eng. 2018, 352, 012048. [Google Scholar] [CrossRef]
- Cheah, W.K.; Ishikawa, K.; Othman, R.; Yeoh, F.Y. Nanoporous Biomaterials for Uremic Toxin Adsorption in Artificial Kidney Systems: A Review. J. Biomed. Mater. Res.-Part B Appl. Biomater. 2017, 105, 1232–1240. [Google Scholar] [CrossRef]
- Ghezzi, P.M.; Sanz-Moreno, C.; Gervasio, R.; Nigrelli, S.; Botella, J. Technical Requirements for Rapid High Efficiency Therapy in Uremic Patients. Am. Soc. Artif. Int. Organs 1987, 33, 546–550. [Google Scholar]
- Pescatore, N.A. Graphitic Carbon Materials Tailored for the Rapid Adsorption of Biomolecules; Drexel University: Philadelphia, PA, USA, 2016. [Google Scholar]
- Lu, L. New Membrane Technologies for Dialysis; University of Waterloo: Waterloo, ON, Canada, 2016. [Google Scholar]
- Basu, R.; Pathak, S.; Goyal, J.; Chaudhry, R.; Goel, R.B.; Barwal, A. Use of a Novel Hemoadsorption Device for Cytokine Removal as Adjuvant Therapy in a Patient with Septic Shock with Multi-Organ Dysfunction: A Case Study. Indian J. Crit. Care Med. 2014, 18, 822–824. [Google Scholar] [CrossRef]
- De Vriese, A.; Colardyn, F.A.; Philippé, J.; Vanholder, R.C.; DE Sutter, J.H.; Lameire, N.H. Cytokine Removal during Continuous Hemofiltration in Septic Patients. J. Am. Soc. Nephrol. 1999, 10, 846–853. [Google Scholar] [CrossRef]
- Malard, B.; Lambert, C.; Kellum, J.A. In Vitro Comparison of the Adsorption of Inflammatory Mediators by Blood Purification Devices. Intensive Care Med. Exp. 2018, 6, 12. [Google Scholar] [CrossRef]
- Botella, J.; Ghezzi, P.M.; Sanz-Moreno, C. Adsorption in Hemodialysis. Kidney Int. Suppl. 2000, 58, 60–65. [Google Scholar] [CrossRef] [PubMed][Green Version]


{kind=link}
| Water-Soluble Low-Molecular-Weight | MW | Middle-Molecules | MW | Protein-Bound | MW |
|---|---|---|---|---|---|
| 1-methyladenosine | 281 | Adrenomedullin | 5729 | 2-methoxyresorcinol | 140 |
| 1-methylguanosine | 297 | Atrial natriuretic peptide | 3080 | 3-deoxyglucosone | 162 |
| 1-methylinosine | 282 | β2-microglobulin | 11,818 | 3-carboxyl-4-methyl-5-propyl-2-furanpropionic acid | 240 |
| Asymmetrical dinethylarginine | 202 | β-endorphin | 3465 | Fructoselysine | 308 |
| α-keto-δ-guanidinovaleric adic | 151 | Cholecystokinin | 3866 | Glyoxal | 58 |
| α-N-acetylarginine | 216 | Clara cell protein | 15,800 | Hippuric acid | 179 |
| Arab(in)itol | 152 | Complement factor D | 23,750 | Homocysteine | 135 |
| Arginnic acid | 175 | Cystatin C | 13,300 | Hydroquinone | 110 |
| Benzylalcohol | 108 | Degranulation inhibiting protein | 14,100 | Indole-3-acetic acid | 175 |
| β-guanidinopropionic acid | 131 | Delta-sleep inducing peptide | 848 | Indoxyl sulphate | 251 |
| β-lipoprotin | 461 | Endothelin | 4283 | Kynurenine | 208 |
| Creatine | 131 | Hyaluronic acid | 25,000 | Kynurenic acid | 189 |
| Creatinine | 113 | Interleukin-1β | 32,000 | Leptin | 16,000 |
| Cytidine | 234 | Interleukin-6 | 24,500 | Melatonin | 126 |
| Dimethylglycine | 103 | κ-Ig light chain | 25,000 | Methylglyoxal | 72 |
| Erythritol | 122 | λ-Ig light chain | 25,000 | Nε-(carboxymethyl)lysine | 204 |
| γ-guanidinobutyric acid | 145 | Leptin | 16,000 | p-cresol | 108 |
| Guanidine | 59 | Methionine-enkephalin | 555 | Pentosidine | 342 |
| Guanidinoacetic acid | 117 | Neuropeptide | 4272 | Phenol | 94 |
| Guanidinosuccinic acid | 175 | Parathyroid hormone | 9225 | P-OH hippuric acid | 195 |
| Hypoxanthine | 136 | Retinol-binding protein | 21,200 | Putrescine | 88 |
| Malondialdehyde | 71 | Tumor necrosis factor-α | 26,000 | Quinolinic acid | 167 |
| Mannitol | 182 | Retinol-binding protein | 21,200 | ||
| Methyguanidine | 73 | Spermidine | 145 | ||
| Myoinositol | 180 | Spermine | 202 | ||
| N2,N2-dimethylguanosine | 311 | ||||
| N4-acetylcytidine | 285 | ||||
| N6-methyladenosine | 281 | ||||
| N6-threonylcarbamoyladenosine | 378 | ||||
| Orotic acid | 174 | ||||
| Orotidine | 288 | ||||
| Oxalate | 90 | ||||
| Phenylacetylgluatmine | 264 | ||||
| Pseudouridine | 244 | ||||
| Symmetrical dimethylarginine | 202 | ||||
| Sorbitol | 182 | ||||
| Taurocyamine | 174 | ||||
| Threitol | 122 | ||||
| Thymine | 126 | ||||
| Uracil | 112 | ||||
| Urea | 60 | ||||
| Uric acid | 168 | ||||
| Uridine | 244 | ||||
| Xanthine | 152 | ||||
| Xanthosine | 284 |
| Basic Principle | Treatment/Membrane Type | Uremic Toxins Removed |
|---|---|---|
| Diffusion | Dialysis/Low-flux membrane | Water-soluble |
| Dialysis/High-flux membrane | Middle-molecules and Protein-bound | |
| Adsorption | Haemoperfusion | Protein-bound |
| Combination of diffusion and adsorption | Dialysis/Mixed Matrix Membrane (MMM) | Water-soluble, middle-molecules, and protein-bound |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raharjo, Y.; Zainol Abidin, M.N.; Ismail, A.F.; Fahmi, M.Z.; Saiful; Elma, M.; Santoso, D.; Haula’, H.; Habibi, A.R. Dialysis Membranes for Acute Kidney Injury. Membranes 2022, 12, 325. https://doi.org/10.3390/membranes12030325
Raharjo Y, Zainol Abidin MN, Ismail AF, Fahmi MZ, Saiful, Elma M, Santoso D, Haula’ H, Habibi AR. Dialysis Membranes for Acute Kidney Injury. Membranes. 2022; 12(3):325. https://doi.org/10.3390/membranes12030325
Chicago/Turabian StyleRaharjo, Yanuardi, Muhammad Nidzhom Zainol Abidin, Ahmad Fauzi Ismail, Mochamad Zakki Fahmi, Saiful, Muthia Elma, Djoko Santoso, Hamizah Haula’, and Ahlan Riwahyu Habibi. 2022. "Dialysis Membranes for Acute Kidney Injury" Membranes 12, no. 3: 325. https://doi.org/10.3390/membranes12030325
APA StyleRaharjo, Y., Zainol Abidin, M. N., Ismail, A. F., Fahmi, M. Z., Saiful, Elma, M., Santoso, D., Haula’, H., & Habibi, A. R. (2022). Dialysis Membranes for Acute Kidney Injury. Membranes, 12(3), 325. https://doi.org/10.3390/membranes12030325