
In Vitro and In Vivo Feasibility Study for a Portable VV-ECMO and ECCO2R System

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
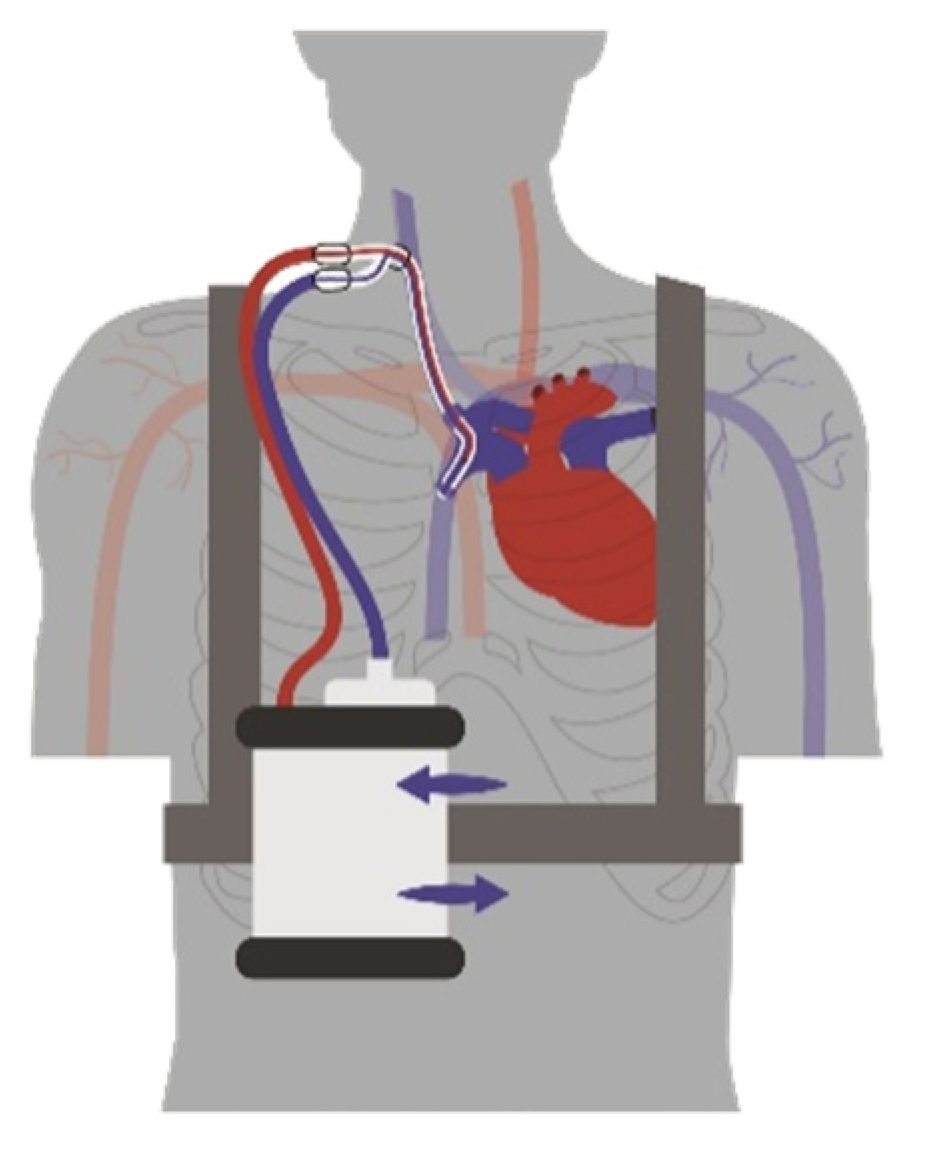
2.1. System Components
2.2. In Vitro Evaluation
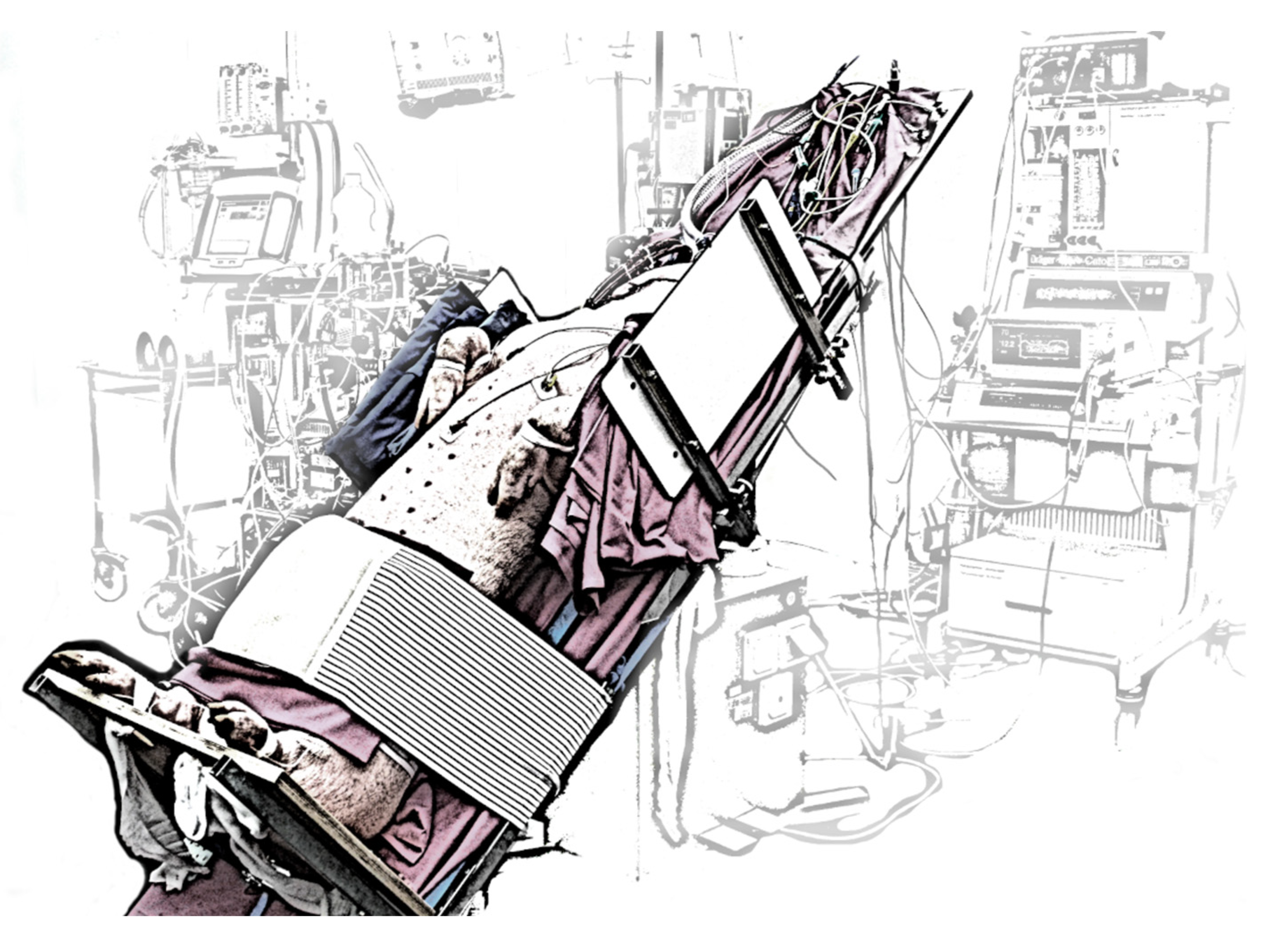
2.3. In Vivo Evaluation

2.4. Statistical Analysis
3. Results
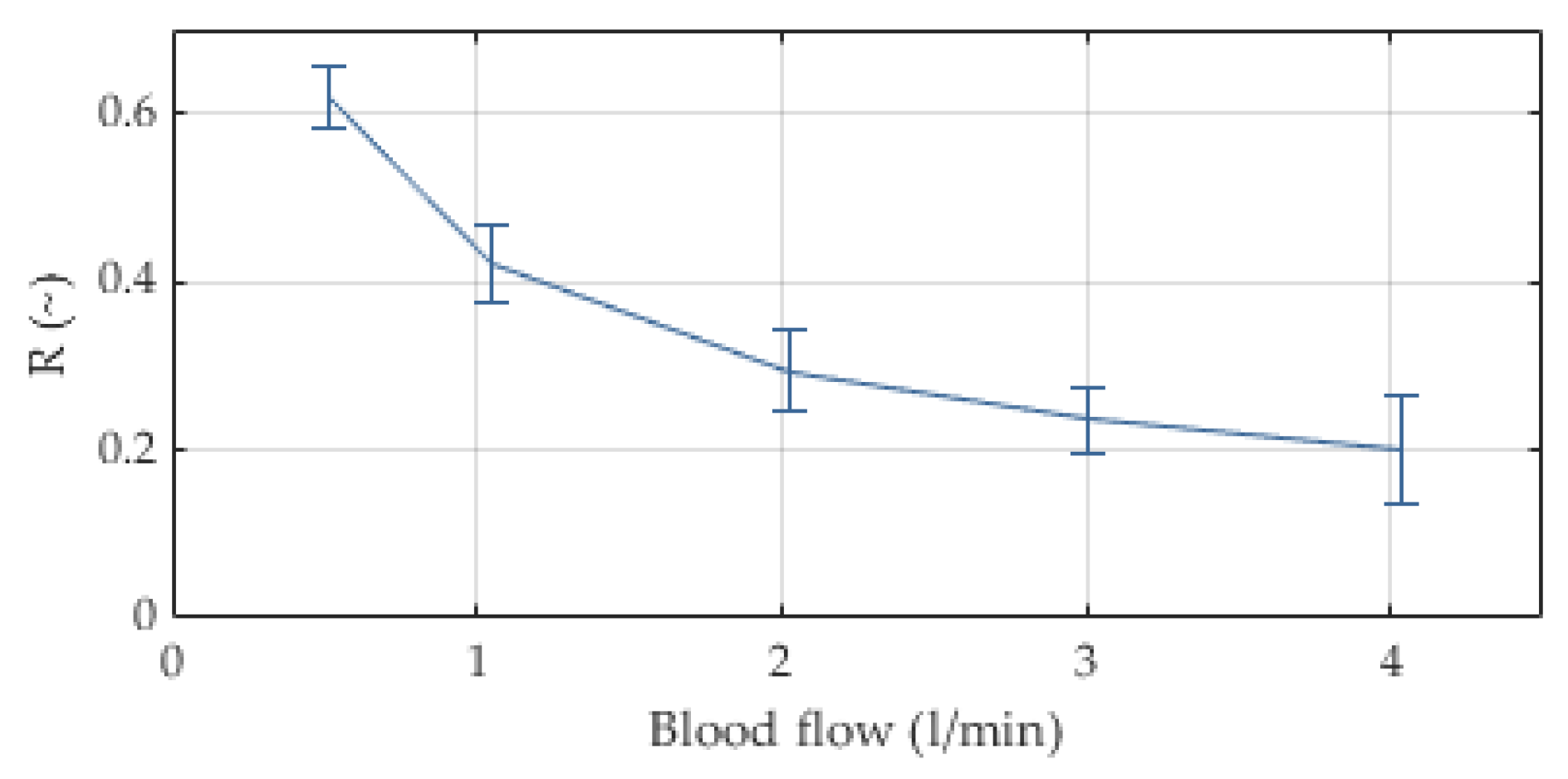
3.1. In Vitro Evaluation
3.2. In Vivo Evaluation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Supine 12 | Supine 10 | Supine 8 | Trend 12 | Trend 10 | p-Value | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | Unit | Mean | Median | SD | Mean | Median | SD | Mean | Median | SD | Mean | Median | SD | Mean | Median | SD | |
| RMV | L/min | 4 | 5 | 2 | 4 | 4 | 1 | 3 | 3 | 2 | 5 | 5 | 1 | 5 | 4 | 1 | 0.040 *, (0) |
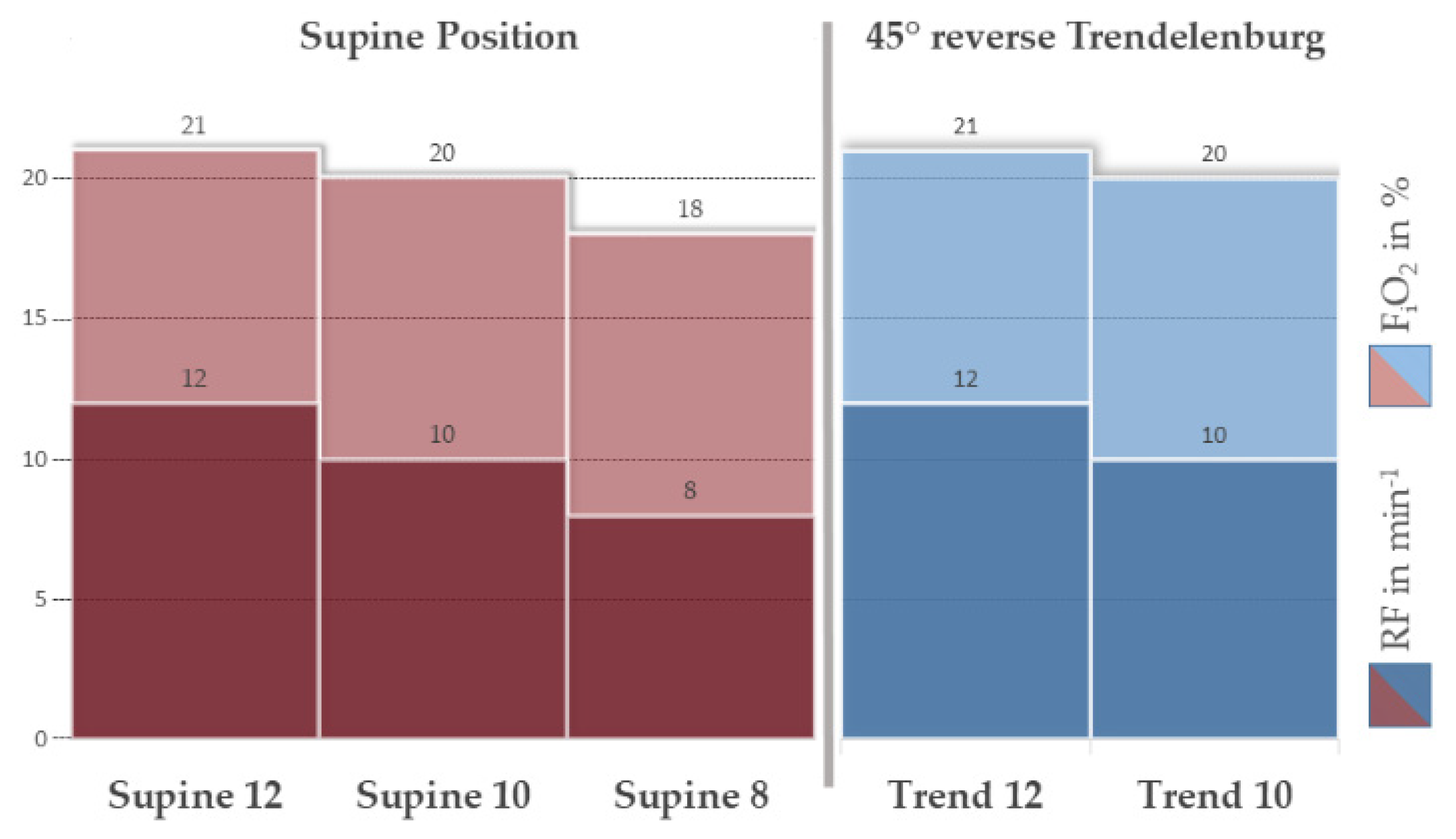
| FiO2 | % | 21 | 21 | 1 | 20 | 20 | 3 | 18 | 18 | 0 | 21 | 21 | 1 | 20 | 19 | 1 | 0.004 *, (1) |
| HF | 1/min | 119 | 111 | 34 | 119 | 121 | 51 | 151 | 169 | 56 | 166 | 168 | 40 | 171 | 171 | 36 | 0.035 *, (0) |
| MAP | mmHg | 75 | 71 | 14 | 105 | 94 | 38 | 94 | 84 | 18 | 79 | 75 | 20 | 71 | 71 | 15 | 0.040 *, (0) |
| MPAP | mmHg | 22 | 20 | 8 | 24 | 21 | 10 | 24 | 23 | 5 | 14 | 14 | 12 | 17 | 15 | 16 | 0.355 *, (0) |
| SaO2 | % | 84 | 87 | 11 | 80 | 85 | 14 | 73 | 77 | 24 | 83 | 87 | 10 | 73 | 74 | 11 | 0.483 † |
| ScvO2 | % | 71 | 72 | 10 | 61 | 67 | 13 | 52 | 61 | 17 | 56 | 56 | 7 | 57 | 54 | 11 | 0.235 † |
| SvO2 | % | 65 | 67 | 6 | 68 | 72 | 13 | 55 | 62 | 18 | 57 | 58 | 5 | 56 | 55 | 4 | 0.231 † |
| paO2 | mmHg | 66 | 64 | 15 | 67 | 67 | 19 | 54 | 50 | 19 | 62 | 65 | 10 | 52 | 50 | 8 | 0.311 † |
| pcvO2 | mmHg | 49 | 47 | 6 | 43 | 43 | 5 | 60 | 40 | 35 | 40 | 42 | 3 | 41 | 40 | 4 | 0.157 † |
| pvO2 | mmHg | 44 | 44 | 2 | 50 | 45 | 12 | 38 | 39 | 5 | 40 | 41 | 3 | 40 | 40 | 3 | 0.075 † |
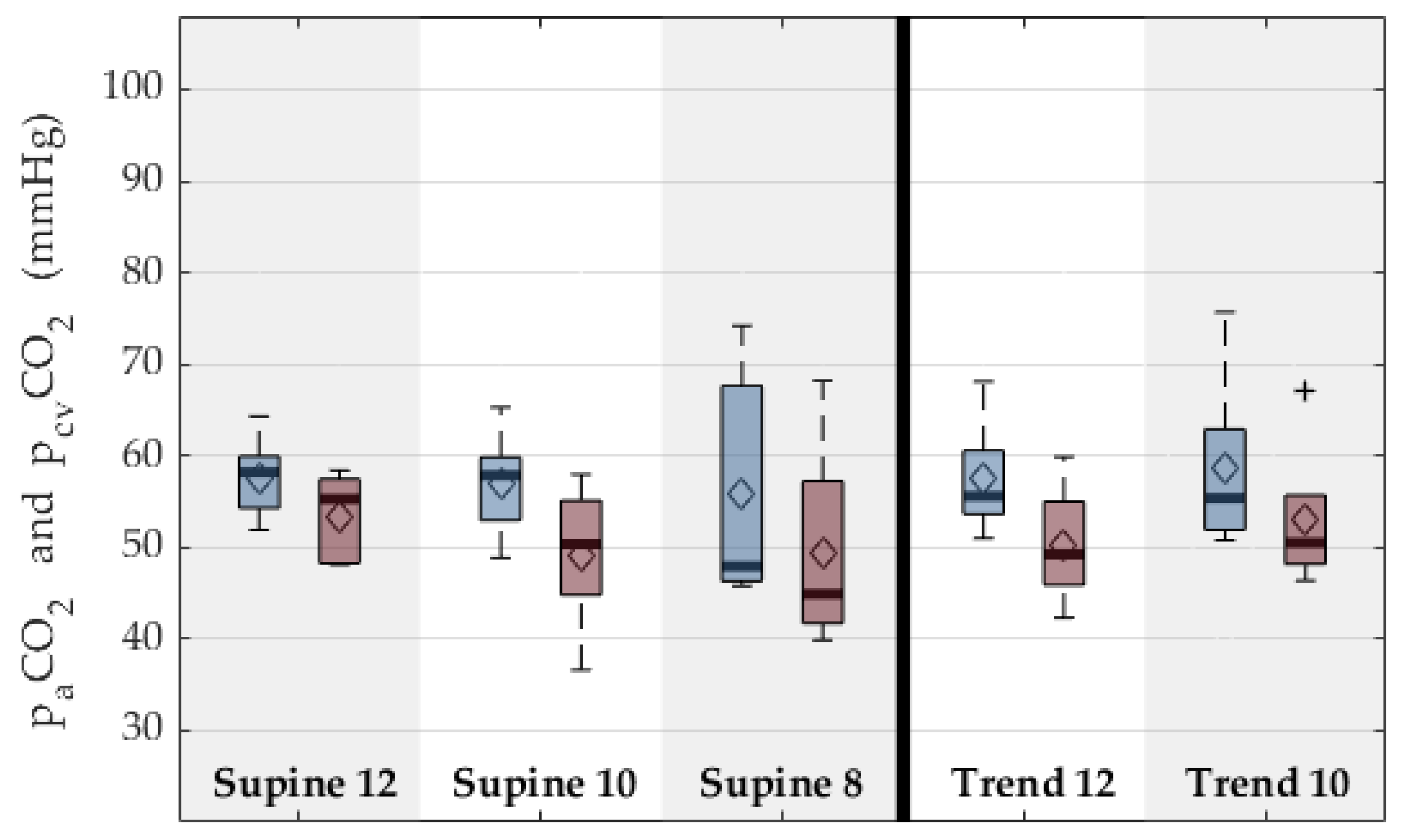
| paCO2 | mmHg | 53 | 55 | 5 | 49 | 50 | 8 | 49 | 45 | 13 | 50 | 49 | 7 | 53 | 51 | 8 | 0.556 † |
| pcvCO2 | mmHg | 58 | 58 | 5 | 57 | 58 | 6 | 56 | 48 | 16 | 57 | 56 | 6 | 59 | 55 | 10 | 0.873 † |
| pvCO2 | mmHg | 56 | 55 | 5 | 52 | 51 | 7 | 51 | 47 | 16 | 54 | 53 | 7 | 57 | 56 | 9 | 0.744 † |
| etCO2 | % | 7 | 6 | 1 | 6 | 7 | 2 | 7 | 6 | 1 | 7 | 7 | 1 | 7 | 7 | 1 | 0.747 * |
| Arterial lactate | mmol/L | 2.8 | 1.0 | 4.1 | 3.5 | 1.7 | 4.1 | 3.0 | 1.8 | 2.7 | 4.1 | 2.6 | 4.0 | 5.6 | 4.5 | 4.8 | 0.255 |
| Arterial pH | [] | 7.4 | 7.4 | 0.1 | 7.4 | 7.4 | 0.1 | 7.4 | 7.4 | 0.1 | 7.4 | 7.4 | 0.1 | 7.3 | 7.3 | 0.1 | 0.321 † |
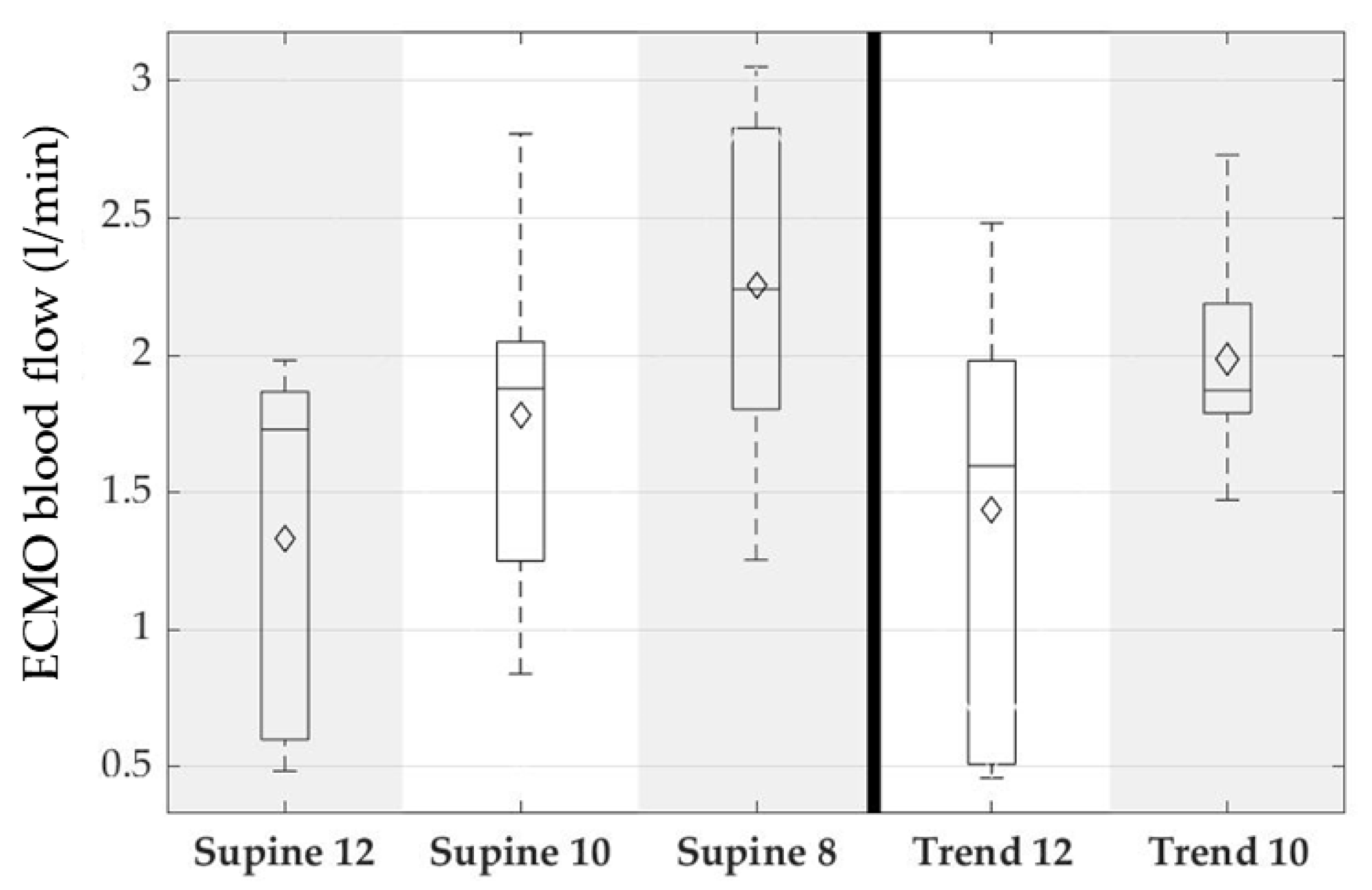
| Blood flow ECMO | L/min | 1.3 | 1.7 | 0.7 | 1.8 | 1.9 | 0.7 | 2.3 | 2.2 | 0.7 | 1.4 | 1.6 | 0.8 | 2.0 | 1.9 | 0.4 | 0.045 *, (0) |
| Pump speed | min−1 | 5470 | 5617 | 2878 | 6803 | 7188 | 2287 | 7457 | 7992 | 1774 | 5797 | 6967 | 2647 | 8097 | 8100 | 1581 | 0.082 * |
| Gas flow | L/min | 4 | 4 | 4 | 5 | 4 | 3 | 6 | 6 | 3 | 4 | 4 | 3 | 5 | 5 | 3 | 0.749 * |
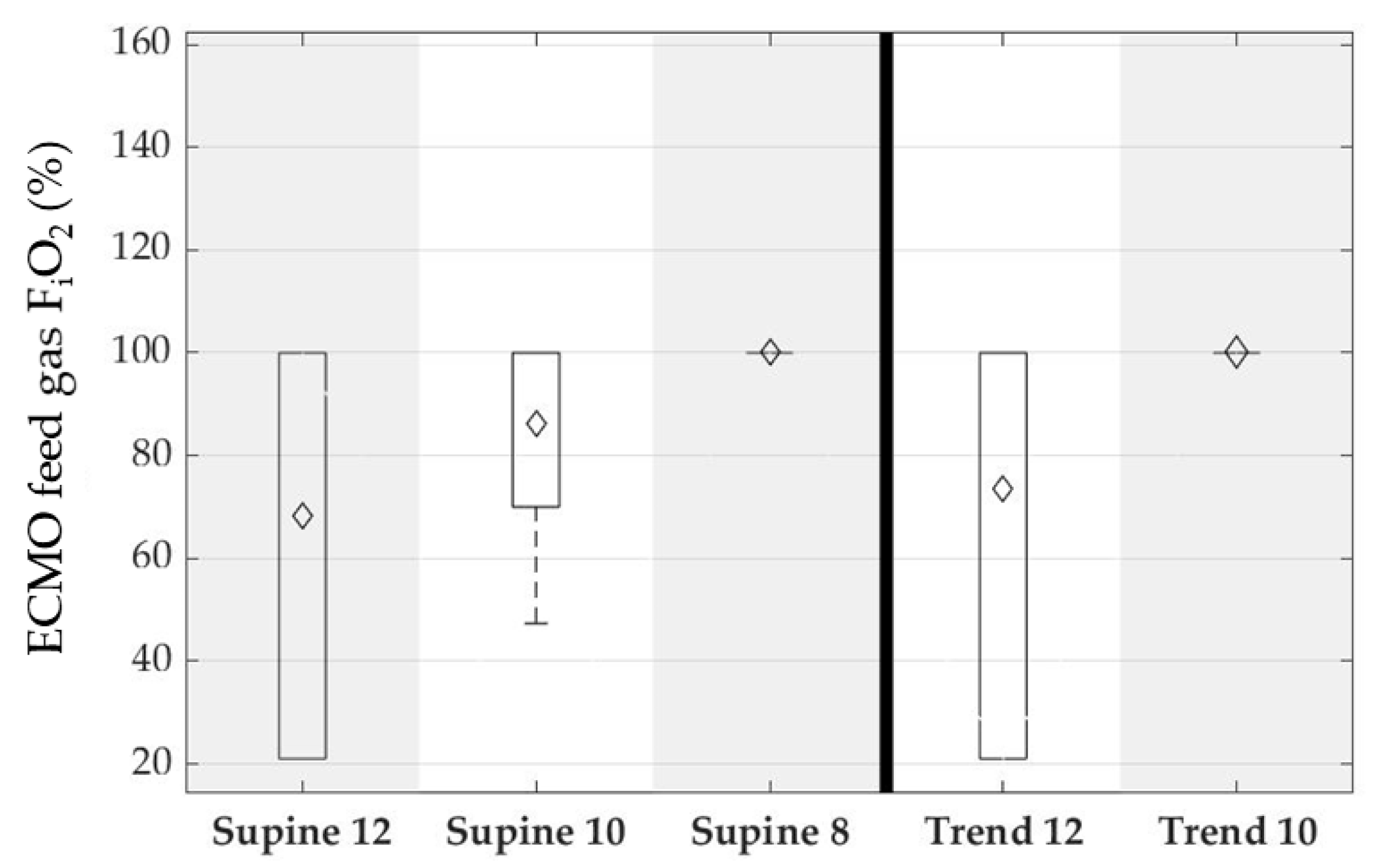
| FiO2 ECMO | % | 68 | 100 | 43 | 86 | 100 | 23 | 100 | 100 | 0 | 74 | 100 | 41 | 100 | 100 | 0 | 0.171 * |
| ΔP ECMO | mmHg | 7 | 7 | 13 | 18 | 20 | 14 | 30 | 28 | 16 | 12 | 16 | 15 | 23 | 26 | 10 | 0.075 * |
| fPHb | mg/dL | 15 | 13 | 6 | 12 | 12 | 7 | 12 | 12 | 7 | 14 | 12 | 4 | 13 | 14 | 6 | 0.920 * |
| SO2 post ECMO | % | 96 | 100 | 8 | 100 | 100 | 1 | 98 | 100 | 5 | 98 | 100 | 3 | 100 | 100 | 0 | 0.922 * |
| SO2 pre ECMO | % | 69 | 76 | 10 | 63 | 68 | 12 | 55 | 58 | 14 | 64 | 68 | 9 | 56 | 55 | 5 | 0.323 * |
| pO2 post ECMO | mmHg | 278 | 322 | 199 | 239 | 227 | 86 | 223 | 182 | 125 | 228 | 232 | 139 | 234 | 181 | 107 | 0.736 * |
| pO2 pre ECMO | mmHg | 48 | 50 | 5 | 48 | 45 | 11 | 52 | 40 | 27 | 45 | 46 | 4 | 41 | 40 | 2 | 0.171 * |
| pCO2 post ECMO | mmHg | 38 | 37 | 13 | 36 | 36 | 5 | 40 | 36 | 7 | 37 | 36 | 3 | 41 | 41 | 3 | 0.073 * |
| pCO2 pre ECMO | mmHg | 58 | 60 | 5 | 54 | 56 | 8 | 54 | 51 | 11 | 55 | 55 | 6 | 59 | 57 | 8 | 0.294 * |
| VCO2 ECMO | mL/min | 106 | 69 | 126 | 85 | 86 | 28 | 78 | 88 | 41 | 58 | 57 | 29 | 60 | 55 | 20 | 0.255 * |
| VO2 ECMO | mL/min | 56 | 57 | 48 | 90 | 93 | 49 | 122 | 133 | 45 | 69 | 74 | 46 | 116 | 123 | 32 | 0.220 * |
4. Discussion
4.1. In Vitro Evaluation
4.2. In Vivo Evaluation
4.3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Tramm, R.; Ilic, D.; Davies, A.R.; Pellegrino, V.A.; Romero, L.; Hodgson, C. Extracorporeal membrane oxygenation for critically ill adults. Cochrane Database Syst. Rev. 2015, 1, CD010381. [Google Scholar] [CrossRef]
- Weill, D.; Benden, C.; Corris, P.A.; Dark, J.H.; Davis, R.D.; Keshavjee, S.; Lederer, D.J.; Mulligan, M.J.; Patterson, G.A.; Singer, L.G.; et al. A consensus document for the selection of lung transplant candidates: 2014--An update from the Pulmonary Transplantation Council of the International Society for Heart and Lung Transplantation. J. Heart Lung Transplant. 2015, 34, 1–15. [Google Scholar] [CrossRef]
- Benazzo, A.; Schwarz, S.; Frommlet, F.; Schweiger, T.; Jaksch, P.; Schellongowski, P.; Staudinger, T.; Klepetko, W.; Lang, G.; Hoetzenecker, K. Twenty-year experience with extracorporeal life support as bridge to lung transplantation. J. Thorac. Cardiovasc. Surg. 2019, 157, 2515–2525.e10. [Google Scholar] [CrossRef]
- Biscotti, M.; Gannon, W.D.; Agerstrand, C.; Abrams, D.; Sonett, J.; Brodie, D.; Bacchetta, M. Awake Extracorporeal Membrane Oxygenation as Bridge to Lung Transplantation: A 9-Year Experience. Ann. Thorac. Surg. 2017, 104, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Fuehner, T.; Kuehn, C.; Hadem, J.; Wiesner, O.; Gottlieb, J.; Tudorache, I.; Olsson, K.M.; Greer, M.; Sommer, W.; Welte, T.; et al. Extracorporeal membrane oxygenation in awake patients as bridge to lung transplantation. Am. J. Respir. Crit. Care Med. 2012, 185, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Hoetzenecker, K.; Donahoe, L.; Yeung, J.C.; Azad, S.; Fan, E.; Ferguson, N.D.; Del Sorbo, L.; de Perrot, M.; Pierre, A.; Yasufuku, K.; et al. Extracorporeal life support as a bridge to lung transplantation-experience of a high-volume transplant center. J. Thorac. Cardiovasc. Surg. 2018, 155, 1316–1328.e1. [Google Scholar] [CrossRef]
- Quaderi, S.A.; Hurst, J.R. The unmet global burden of COPD. Glob. Health Epidemiol. Genom. 2018, 3, e4. [Google Scholar] [CrossRef] [PubMed]
- Varmaghani, M.; Dehghani, M.; Heidari, E.; Sharifi, F.; Moghaddam, S.S.; Farzadfar, F. Global prevalence of chronic obstructive pulmonary disease: Systematic review and meta-analysis. East. Mediterr. Health J. 2019, 25, 47–57. [Google Scholar] [CrossRef]
- Chambers, D.C.; Cherikh, W.S.; Harhay, M.O.; Hayes, D.; Hsich, E.; Khush, K.K.; Meiser, B.; Potena, L.; Rossano, J.W.; Toll, A.E.; et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-sixth adult lung and heart-lung transplantation Report-2019; Focus theme: Donor and recipient size match. J. Heart Lung Transplant. 2019, 38, 1042–1055. [Google Scholar] [CrossRef]
- Shah, R.J.; Kotloff, R.M. Lung transplantation for obstructive lung diseases. Semin. Respir. Crit. Care Med. 2013, 34, 288–296. [Google Scholar] [CrossRef]
- Kozower, B.D.; Meyers, B.F.; Smith, M.A.; de Oliveira, N.C.; Cassivi, S.D.; Guthrie, T.J.; Wang, H.; Ryan, B.J.; Shen, K.R.; Daniel, T.M.; et al. The impact of the lung allocation score on short-term transplantation outcomes: A multicenter study. J. Thorac. Cardiovasc. Surg. 2008, 135, 166–171. [Google Scholar] [CrossRef]
- Turner, D.A.; Cheifetz, I.M.; Rehder, K.J.; Williford, W.L.; Bonadonna, D.; Banuelos, S.V.J.; Peterson-Carmichael, S.; Lin, S.S.; Davis, R.D.; Zaas, D. Active rehabilitation and physical therapy during extracorporeal membrane oxygenation while awaiting lung transplantation: A practical approach. Crit. Care Med. 2011, 39, 2593–2598. [Google Scholar] [CrossRef] [PubMed]
- Cypel, M.; Keshavjee, S. Extracorporeal life support as a bridge to lung transplantation. Clin. Chest Med. 2011, 32, 245–251. [Google Scholar] [CrossRef] [PubMed]
- de Jonghe, B.; Sharshar, T.; Lefaucheur, J.-P.; Authier, F.-J.; Durand-Zaleski, I.; Boussarsar, M.; Cerf, C.; Renaud, E.; Mesrati, F.; Carlet, J.; et al. Paresis acquired in the intensive care unit: A prospective multicenter study. JAMA 2002, 288, 2859–2867. [Google Scholar] [CrossRef]
- Needham, D.M.; Korupolu, R.; Zanni, J.M.; Pradhan, P.; Colantuoni, E.; Palmer, J.B.; Brower, R.G.; Fan, E. Early physical medicine and rehabilitation for patients with acute respiratory failure: A quality improvement project. Arch. Phys. Med. Rehabil. 2010, 91, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Truong, A.D.; Fan, E.; Brower, R.G.; Needham, D.M. Bench-to-bedside review: Mobilizing patients in the intensive care unit--from pathophysiology to clinical trials. Crit. Care 2009, 13, 216. [Google Scholar] [CrossRef]
- Crotti, S.; Iotti, G.A.; Lissoni, A.; Belliato, M.; Zanierato, M.; Chierichetti, M.; Di Meo, G.; Meloni, F.; Pappalettera, M.; Nosotti, M.; et al. Organ allocation waiting time during extracorporeal bridge to lung transplant affects outcomes. Chest 2013, 144, 1018–1025. [Google Scholar] [CrossRef]
- Lehr, C.J.; Zaas, D.W.; Cheifetz, I.M.; Turner, D.A. Ambulatory extracorporeal membrane oxygenation as a bridge to lung transplantation: Walking while waiting. Chest 2015, 147, 1213–1218. [Google Scholar] [CrossRef]
- Abrams, D.; Combes, A.; Brodie, D. Extracorporeal membrane oxygenation in cardiopulmonary disease in adults. J. Am. Coll. Cardiol. 2014, 63, 2769–2778. [Google Scholar] [CrossRef]
- Abrams, D.; Javidfar, J.; Farrand, E.; Mongero, L.B.; Agerstrand, C.L.; Ryan, P.; Zemmel, D.; Galuskin, K.; Morrone, T.M.; Boerem, P.; et al. Early mobilization of patients receiving extracorporeal membrane oxygenation: A retrospective cohort study. Crit. Care 2014, 18, R38. [Google Scholar] [CrossRef]
- Abrams, D.; Madahar, P.; Eckhardt, C.M.; Short, B.; Yip, N.H.; Parekh, M.; Serra, A.; Dubois, R.L.; Saleem, D.; Agerstrand, C.; et al. Early Mobilization during ECMO for Cardiopulmonary Failure in Adults: Factors Associated with Intensity of Treatment. Ann. Am. Thorac. Soc. 2021, 19, 90–98. [Google Scholar] [CrossRef]
- Ko, Y.; Cho, Y.H.; Park, Y.H.; Lee, H.; Suh, G.Y.; Yang, J.H.; Park, C.-M.; Jeon, K.; Chung, C.R. Feasibility and Safety of Early Physical Therapy and Active Mobilization for Patients on Extracorporeal Membrane Oxygenation. ASAIO J. 2015, 61, 564–568. [Google Scholar] [CrossRef]
- Pruijsten, R.; van Thiel, R.; Hool, S.; Saeijs, M.; Verbiest, M.; Reis Miranda, D. Mobilization of patients on venovenous extracorporeal membrane oxygenation support using an ECMO helmet. Intensive Care Med. 2014, 40, 1595–1597. [Google Scholar] [CrossRef] [PubMed]
- Haji, J.Y.; Mehra, S.; Doraiswamy, P. Awake ECMO and mobilizing patients on ECMO. Indian J. Thorac. Cardiovasc. Surg. 2021, 37, 1–10. [Google Scholar] [CrossRef]
- ISO 7199:2016; Cardiovascular Implants and Artificial Organs: Cardiovascular Implants and Artificial Organs—Blood-Gas Exchangers (Oxygenators), 11.040.40 Implants for Surgery, Prosthetics and Orthotics (7199:2016). International Organization for Standardization: Geneva, Switzerland, 2016.
- Food and Drug Administration. Guidance for Cardiopulmonary Bypass Oxygenators 510 (k) Submissions: Final Guidance for Industry and FDA Staff; Food and Drug Administration: Washington, DC, USA, 2010.
- Hesselmann, F.; Focke, J.M.; Schlanstein, P.C.; Steuer, N.B.; Kaesler, A.; Reinartz, S.D.; Schmitz-Rode, T.; Steinseifer, U.; Jansen, S.V.; Arens, J. Introducing 3D-potting: A novel production process for artificial membrane lungs with superior blood flow design. Bio-Des. Manuf. 2021. [Google Scholar] [CrossRef]
- Kopp, R.; Bensberg, R.; Stollenwerk, A.; Arens, J.; Grottke, O.; Walter, M.; Rossaint, R. Automatic Control of Veno-Venous Extracorporeal Lung Assist. Artif. Organs 2016, 40, 992–998. [Google Scholar] [CrossRef] [PubMed]
- Douglas, A.R.; Jones, N.L.; Reed, J.W. Calculation of whole blood CO2 content. J. Appl. Physiol. (1985) 1988, 65, 473–477. [Google Scholar] [CrossRef]
- Leach, R.M.; Treacher, D.F. The pulmonary physician in critical care * 2: Oxygen delivery and consumption in the critically ill. Thorax 2002, 57, 170–177. [Google Scholar] [CrossRef]
- Maquet Cardiopulmonary GmbH. Instructions for Use: HLS Set Advanced 5.0 | HLS Set Advanced 7.0 1.4|G-270|01; Maquet Cardiopulmonary GmbH: Rastatt, Germany.
- Xenios AG. Data Sheet: Novalung iLA Membrane Ventilator; Xenios AG: Heilbronn, Germany.
- Ficial, B.; Vasques, F.; Zhang, J.; Whebell, S.; Slattery, M.; Lamas, T.; Daly, K.; Agnew, N.; Camporota, L. Physiological Basis of Extracorporeal Membrane Oxygenation and Extracorporeal Carbon Dioxide Removal in Respiratory Failure. Membranes 2021, 11, 225. [Google Scholar] [CrossRef]
- von Petersdorff-Campen, K.; Abeken, J.; de Zélicourt, D.; Kurtcuoglu, V.; Meboldt, M.; Schmid Daners, M. In Vitro Testing and Comparison of Additively Manufactured Polymer Impellers for the CentriMag Blood Pump. ASAIO J. 2021, 67, 306–313. [Google Scholar] [CrossRef]
- Kopp, R.; Bensberg, R.; Arens, J.; Steinseifer, U.; Schmitz-Rode, T.; Rossaint, R.; Henzler, D. A miniaturized extracorporeal membrane oxygenator with integrated rotary blood pump: Preclinical in vivo testing. ASAIO J. 2011, 57, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Madhani, S.P.; Frankowski, B.J.; Ye, S.-H.; Burgreen, G.W.; Wagner, W.R.; Kormos, R.; D’Cunha, J.; Federspiel, W.J. In Vivo 5 Day Animal Studies of a Compact, Wearable Pumping Artificial Lung. ASAIO J. 2019, 65, 94–100. [Google Scholar] [CrossRef]
- Kopp, R.; Mottaghy, K.; Kirschfink, M. Mechanism of complement activation during extracorporeal blood-biomaterial interaction: Effects of heparin coated and uncoated surfaces. ASAIO J. 2002, 48, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Lappa, A.; Cottini, M.; Ranocchi, S.D.F.; Luzi, G.; Montalto, A.; Contento, C.; Bruno, A.; Pisani, P.; Antonio, P.; Emiliano, V.; et al. Single or Double Site Cannuation for Veno-Venous Ecmo in Severe Obese Patient? ARC J. Anesthesiol. 2016, 1, 19–24. [Google Scholar] [CrossRef]
- Chen, R.H.-S.; Yam, N.; Lun, K.-S.; Au, T.W.-K. Migrated Avalon-Elite cannula in an infant transcatheter repositioning without interruption of ECMO flow. J. Artif. Organs 2021, 24, 382–386. [Google Scholar] [CrossRef]
- Kalbhenn, J.; Maier, S.; Heinrich, S.; Schallner, N. Bedside repositioning of a dislocated Avalon-cannula in a running veno-venous ECMO. J. Artif. Organs 2017, 20, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Simons, A.P.; Donker, D.W.; Weerwind, P.W. Optimized safety and function of the bicaval dual-lumen cannula by refined positioning and bedside management. Intensive Care Med. 2013, 39, 984–985. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, D.; Pitcher, H.T.; Cavarocchi, N.; Hirose, H. Migrated Avalon Veno-Venous Extracorporeal Membrane Oxygenation Cannula: How to Adjust Without Interruption of Flow. J. Card. Surg. 2015, 30, 865–868. [Google Scholar] [CrossRef]
- Betancor, J.; Xu, B.; Rehman, K.A.; Rivas, C.G.; Patel, K.; Tong, M.Z.; Rodriguez, L.L. Transesophageal Echocardiographic Guidance of Venovenous Extracorporeal Membrane Oxygenation Cannula (Avalon Cannula) Repositioning. CASE 2017, 1, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Reis Miranda, D.; Dabiri Abkenari, L.; Nieman, K.; Dijkshoorn, M.; Duckers, E.; Gommers, D. Myocardial infarction due to malposition of ECMO cannula. Intensive Care Med. 2012, 38, 1233–1234. [Google Scholar] [CrossRef][Green Version]
- Steuer, N.B.; Hugenroth, K.; Beck, T.; Spillner, J.; Kopp, R.; Reinartz, S.; Schmitz-Rode, T.; Steinseifer, U.; Wagner, G.; Arens, J. Long-Term Venovenous Connection for Extracorporeal Carbon Dioxide Removal (ECCO2R)-Numerical Investigation of the Connection to the Common Iliac Veins. Cardiovasc. Eng. Technol. 2020, 11, 362–380. [Google Scholar] [CrossRef] [PubMed]
- Palmér, O.; Palmér, K.; Hultman, J.; Broman, M. Cannula Design and Recirculation During Venovenous Extracorporeal Membrane Oxygenation. ASAIO J. 2016, 62, 737–742. [Google Scholar] [CrossRef] [PubMed]
- Conrad, S.A.; Wang, D. Evaluation of Recirculation During Venovenous Extracorporeal Membrane Oxygenation Using Computational Fluid Dynamics Incorporating Fluid-Structure Interaction. ASAIO J. 2021, 67, 943–953. [Google Scholar] [CrossRef] [PubMed]
- Broman, M.; Frenckner, B.; Bjällmark, A.; Broomé, M. Recirculation during veno-venous extra-corporeal membrane oxygenation--a simulation study. Int. J. Artif. Organs 2015, 38, 23–30. [Google Scholar] [CrossRef]
- Müller, T.; Lubnow, M.; Philipp, A.; Bein, T.; Jeron, A.; Luchner, A.; Rupprecht, L.; Reng, M.; Langgartner, J.; Wrede, C.E.; et al. Extracorporeal pumpless interventional lung assist in clinical practice: Determinants of efficacy. Eur. Respir. J. 2009, 33, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Kopp, R.; Bensberg, R.; Wardeh, M.; Rossaint, R.; Kuhlen, R.; Henzler, D. Pumpless arterio-venous extracorporeal lung assist compared with veno-venous extracorporeal membrane oxygenation during experimental lung injury. Br. J. Anaesth. 2012, 108, 745–753. [Google Scholar] [CrossRef] [PubMed]














Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strudthoff, L.J.; Lüken, H.; Jansen, S.V.; Petran, J.; Schlanstein, P.C.; Schraven, L.; Schürmann, B.J.; Steuer, N.B.; Wagner, G.; Schmitz-Rode, T.; et al. In Vitro and In Vivo Feasibility Study for a Portable VV-ECMO and ECCO2R System. Membranes 2022, 12, 133. https://doi.org/10.3390/membranes12020133
Strudthoff LJ, Lüken H, Jansen SV, Petran J, Schlanstein PC, Schraven L, Schürmann BJ, Steuer NB, Wagner G, Schmitz-Rode T, et al. In Vitro and In Vivo Feasibility Study for a Portable VV-ECMO and ECCO2R System. Membranes. 2022; 12(2):133. https://doi.org/10.3390/membranes12020133
Chicago/Turabian StyleStrudthoff, Lasse J., Hannah Lüken, Sebastian V. Jansen, Jan Petran, Peter C. Schlanstein, Lotte Schraven, Benjamin J. Schürmann, Niklas B. Steuer, Georg Wagner, Thomas Schmitz-Rode, and et al. 2022. "In Vitro and In Vivo Feasibility Study for a Portable VV-ECMO and ECCO2R System" Membranes 12, no. 2: 133. https://doi.org/10.3390/membranes12020133
APA StyleStrudthoff, L. J., Lüken, H., Jansen, S. V., Petran, J., Schlanstein, P. C., Schraven, L., Schürmann, B. J., Steuer, N. B., Wagner, G., Schmitz-Rode, T., Steinseifer, U., Arens, J., & Kopp, R. (2022). In Vitro and In Vivo Feasibility Study for a Portable VV-ECMO and ECCO2R System. Membranes, 12(2), 133. https://doi.org/10.3390/membranes12020133