
A Dedicated Veno-Venous Extracorporeal Membrane Oxygenation Unit during a Respiratory Pandemic: Lessons Learned from COVID-19 Part I: System Planning and Care Teams

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Results
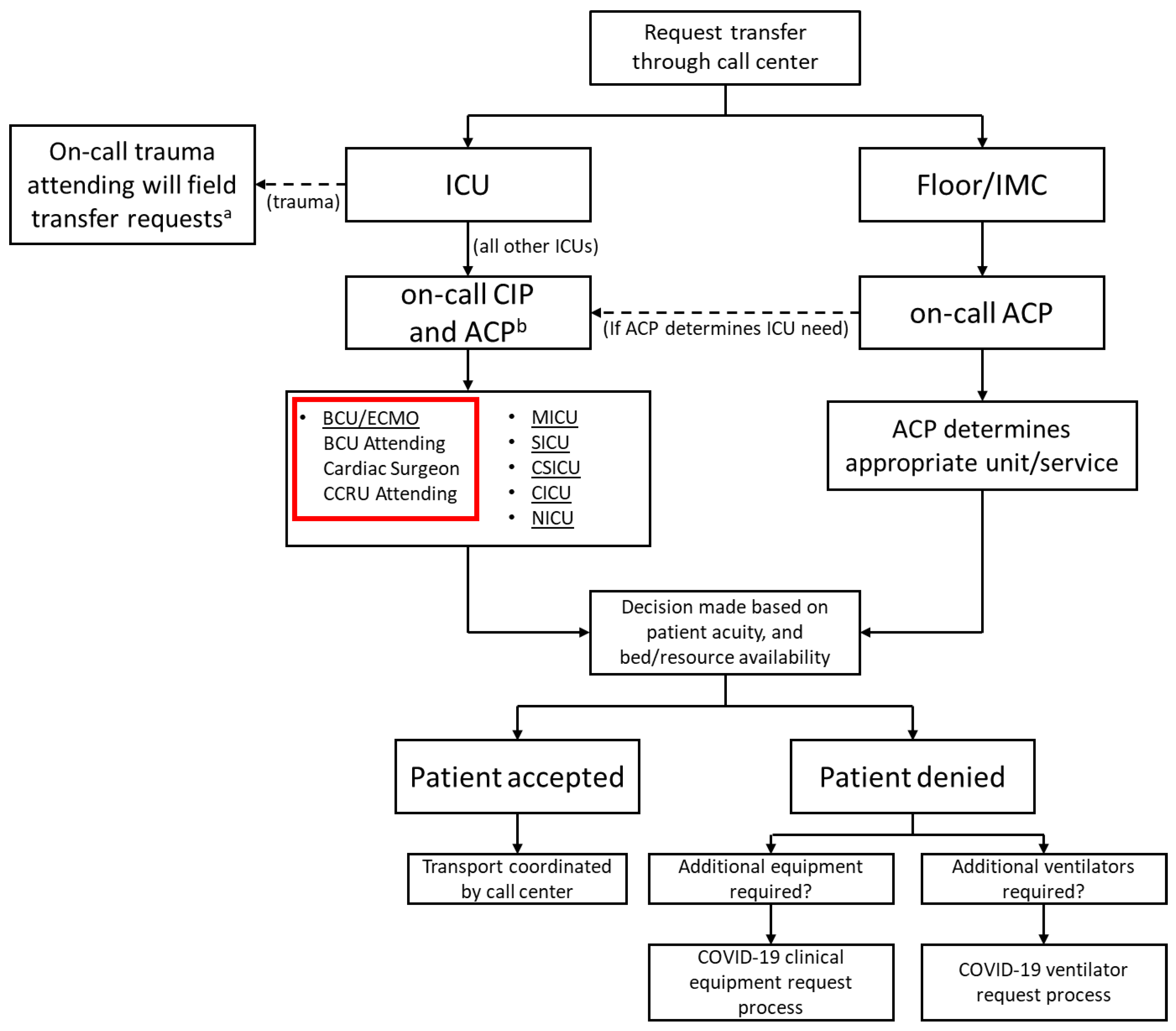
3.1. System Set Up/Approach
- Early planning is critical when facing a disaster event, such as a viral respiratory pandemic.
- Creation of a formal HICS structure with assigned triage officers is vital for preserving the workforce, abolishing redundant processes, and improving overall patient access throughout a healthcare system.
- A centralized, computerized platform to track resource availability can inform decisions regarding scarcity of supplies.
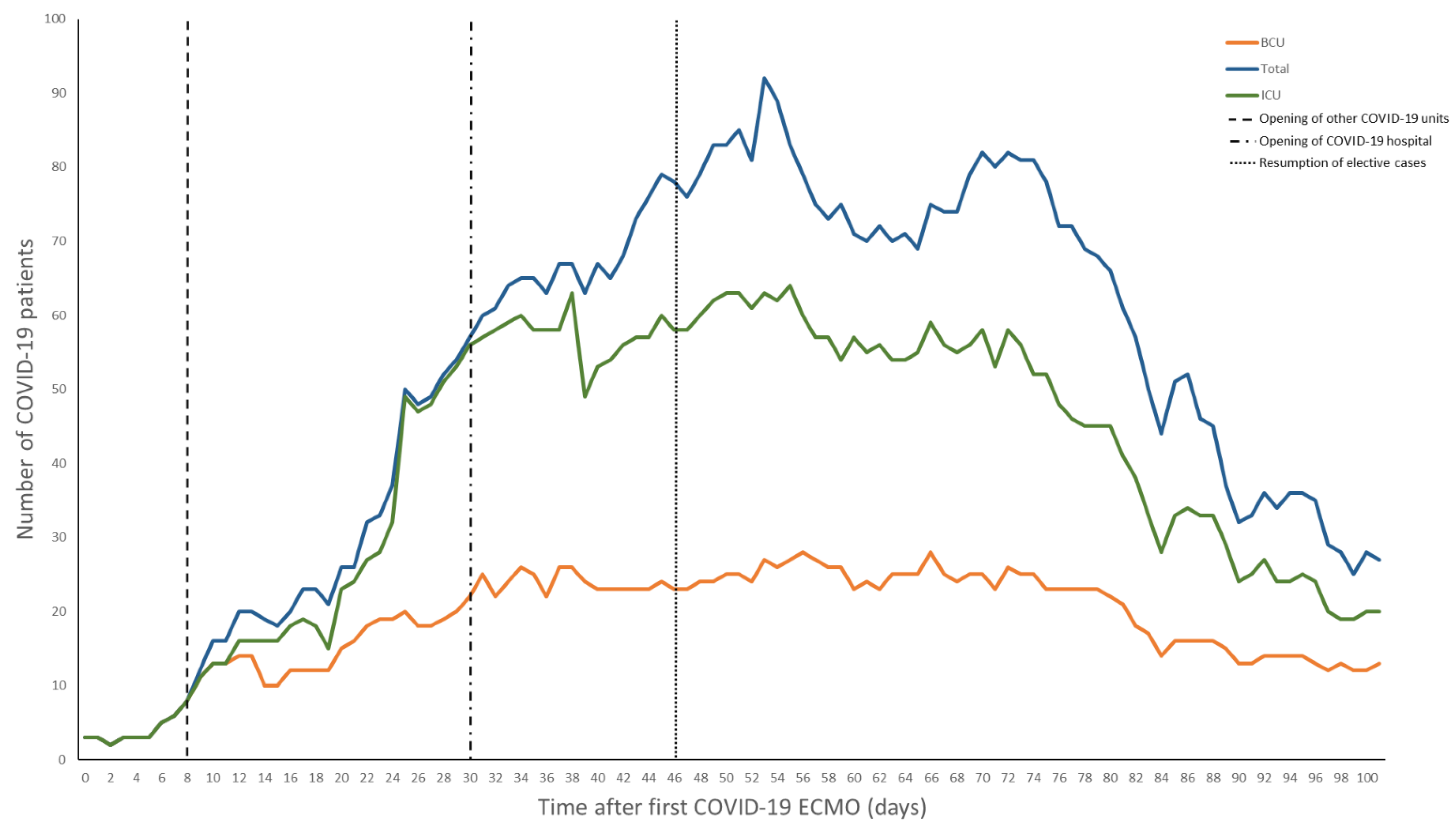
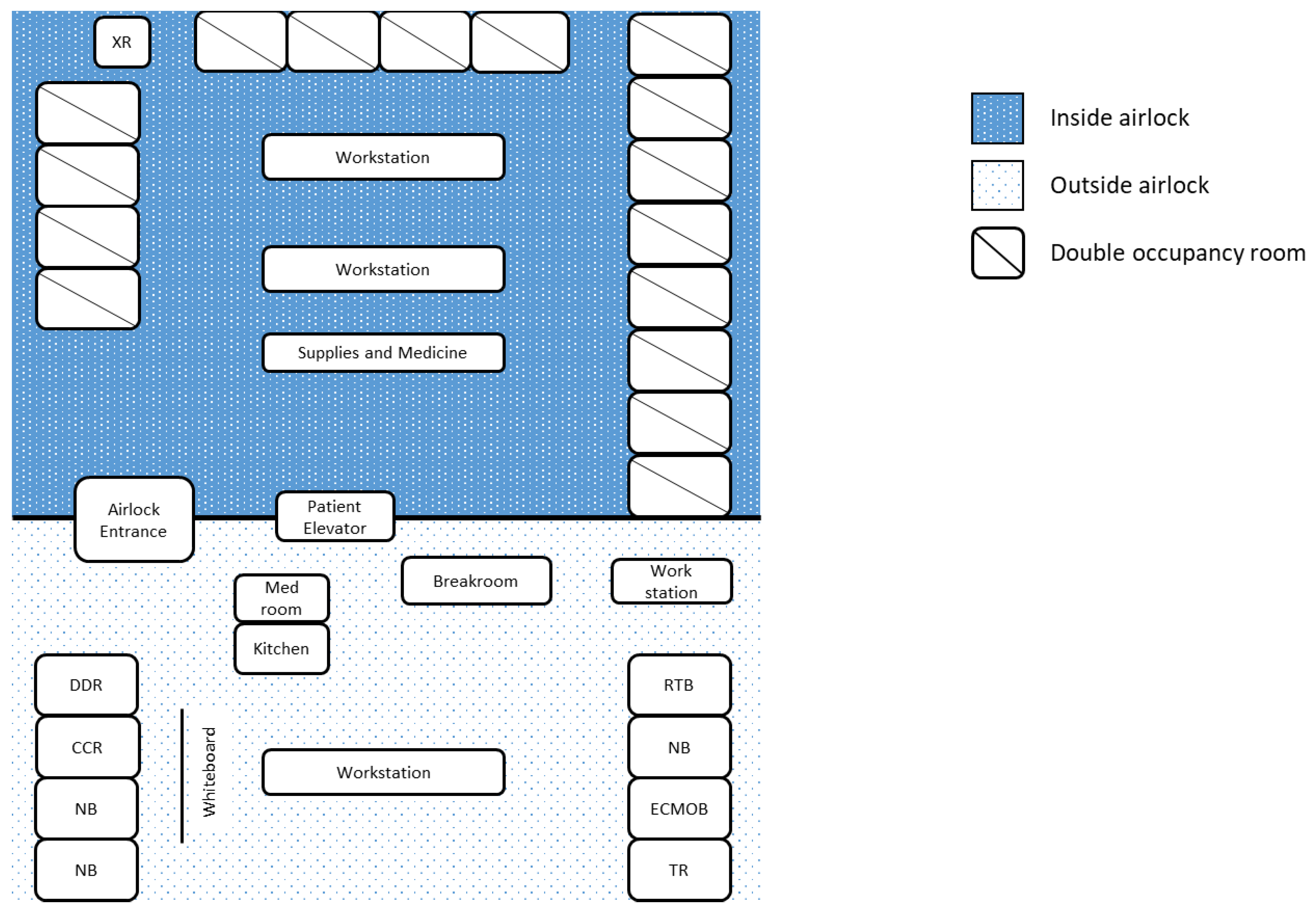
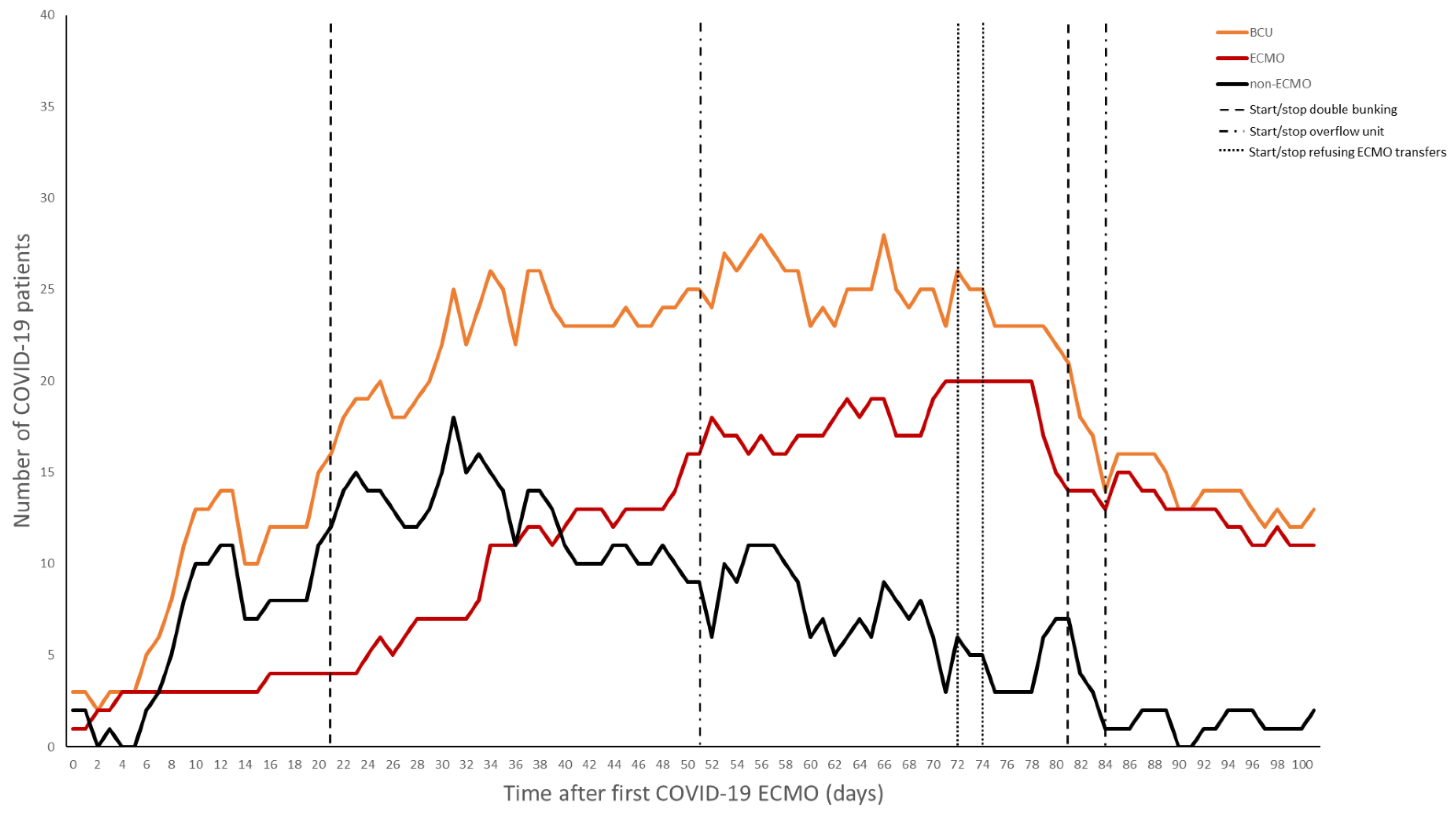
3.2. Evolution of the Biocontainment Unit
- An airlock unit for treating a contagious pathogen can facilitate the care of a large group of critically ill patients.
- Social distancing of staff outside the airlock is crucial to minimizing the risk of secondary exposures.
- The added capacity with double-bunking critically ill patients comes with the potential for increased cross-contamination and should be considered a last resort, even in a pandemic.
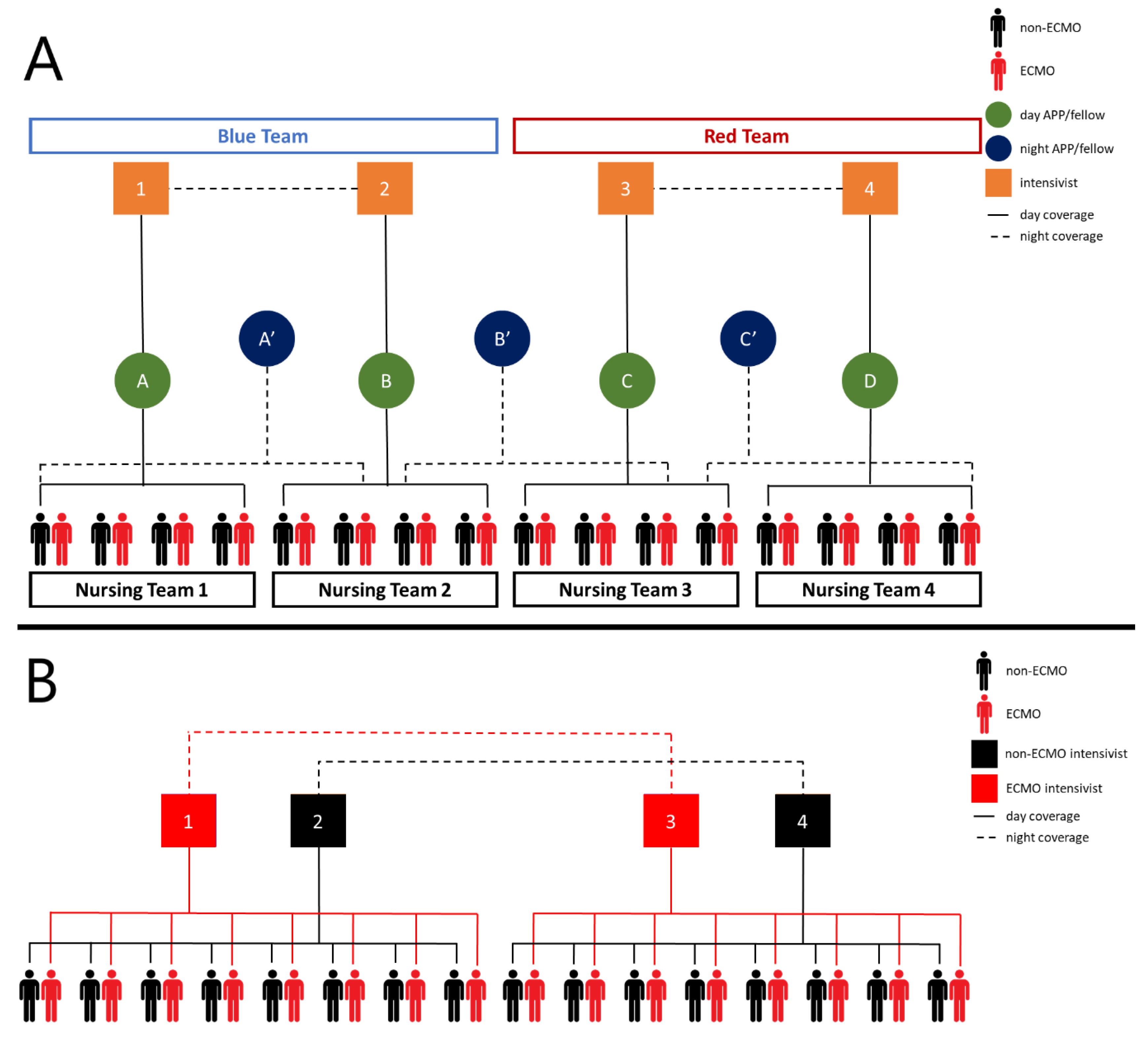
3.3. Intensivist and Provider Teams
- A tiered staffing model to employ team-based approach from attendings to providers to nurses is effective.
- A dedicated ECMO and non-ECMO intensive care team is beneficial when caring for a mixed unit.
- Maintaining a standardized approach for continuity of patient care is difficult but vital to the care of critically ill patients during a pandemic
3.4. Nursing
- Team nursing can allow for increased patient-to-nurse ratios; however, there are trade-offs that must be considered.
- Understand the limitations of patient assessments when relying on team nursing, especially when reallocating staff from non-critical care settings, and the importance for firsthand provider assessments.
3.5. Communication/Technology
- Expeditious communication within the team is essential for the care of critically ill patients.
- The use of technology (tablets, mobile phones, secure messaging applications) can prove helpful within an airlock unit.
- Consider the use of a designated team to communicate with family members for routine updates.
- A centralized system to track availability of medications that is accessible by the care team helps work around true versus perceived shortages.
3.6. ECMO Planning
- With an anticipated increased need for ECMO, the process of acquiring additional equipment should begin early.
- Total ECMO capacity can be augmented by various means such as reallocating from within the system, adding an oxygenator to extracorporeal VADs, and trialing new platforms.
- Minimize variability when caring for high volumes during a pandemic.
- Have an algorithmic approach to augmenting ECMO staff and consider outside contracts as well as training VAD and RT staff.
- Consider the use of alternatives when there are shortages of ancillary ECMO equipment such as forced-air warming blankets for temperature management or room in-line air for sweep flow.
- Have a central place to update important clinical parameters for ECMO patients with rotating staff, intensivists, and cardiac surgeons.
3.7. Physical Therapy
- Staff and PPE within an airlock unit may limit the ability to provide physical therapy and safely ambulate patients.
- A strict schedule of positioning changes, in the absence of physical therapy, is important for prevention of pressure injury.
- Consider the routine use of alternatives, such as positioning beds, in this setting.
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tung, J.; Carter, D.; Rappold, J. Empyema commission of 1918-Impact on acute care surgery 100 years later. J. Trauma Acute Care Surg. 2019, 86, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Ashton, J. COVID-19 and the ‘Spanish’ flu. J. R. Soc. Med. 2020, 113, 197–198. [Google Scholar] [CrossRef]
- Autrey, P.; Moss, J. High-reliability teams and situation awareness: Implementing a hospital emergency incident command system. J. Nurs. Adm. 2006, 36, 67–72. [Google Scholar] [CrossRef]
- Djalali, A.; Castren, M.; Hosseinijenab, V.; Khatib, M.; Ohlen, G.; Kurland, L. Hospital Incident Command System (HICS) perfor-mance in Iran; decision making during disasters. Scand. J. Trauma Resusc. Emerg. Med. 2012, 20, 14. [Google Scholar] [CrossRef]
- Vargas, M.; De Marco, G.; De Simone, S.; Servillo, G. Logistic and organizational aspects of a dedicated intensive care unit for COVID-19 patients. Crit. Care 2020, 24, 1–3. [Google Scholar] [CrossRef]
- Li, X.; Guo, Z.; Li, B.; Zhang, X.; Tian, R.; Wu, W.; Zhang, Z.; Lu, Y.; Chen, N.; Clifford, S.P.; et al. Extracorporeal Membrane Oxygenation for Coronavirus Disease 2019 in Shanghai, China. ASAIO J. 2020, 66, 475–481. [Google Scholar] [CrossRef]
- Menaker, J.; Dolly, K.; Rector, R.; Kufera, J.; Lee, E.E.; Tabatabai, A.; Rabinowitz, R.P.; Kon, Z.N.; Sanchez, P.; Pham, S.; et al. The lung rescue unit—Does a dedicated intensive care unit for venovenous extracorporeal membrane oxygenation improve survival to discharge? J. Trauma Acute Care Surg. 2017, 83, 438–442. [Google Scholar] [CrossRef]
- Shekar, K.; Badulak, J.; Peek, G.; Boeken, U.; Dalton, H.J.; Arora, L.; Zakhary, B.; Ramanathan, K.; Starr, J.; Akkanti, B.; et al. Extracorporeal Life Support Organization Coronavirus Disease 2019 Interim Guidelines: A Consensus Document from an International Group of Interdisciplinary Extracorporeal Membrane Oxygenation Providers. ASAIO J. 2020, 66, 707–721. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, S.; Shooshtari, S.; Tofighi, S. Benefits, barriers, and limitations on the use of Hospital Incident Command System. J. Res. Med. Sci. 2017, 22, 36. [Google Scholar] [CrossRef] [PubMed]
- English, J.F.; Cundiff, M.Y.; Malone, J.D.; Pfeiffer, J.A. Bioterrorism Readiness Plan: A Template for Healthcare Facilities; APIC Bioterrorism Task Force, CDC Hospital Infections Program Bioterrorism Working Group: Washington, DC, USA, 1999; [online] HHS.gov. Available online: https://emergency.cdc.gov/bioterrorism/pdf/13apr99APIC-CDCBioterrorism.pdf (accessed on 18 March 2021).
- Smith, P.W.; Anderson, A.O.; Christopher, G.W.; Cieslak, T.J.; Devreede, G.J.; Fosdick, G.A.; Greiner, C.B.; Hauser, J.M.; Hinrichs, S.H.; Huebner, K.D.; et al. Designing a biocontainment unit to care for patients with serious communicable diseases: A consensus statement. Biosecurity and Bioterrorism. Biodefense Strategy Pract. Sci. 2006, 4, 351–365. [Google Scholar]
- Liew, M.F.; Siow, W.T.; MacLaren, G.; See, K.C. Preparing for COVID-19: Early experience from an intensive care unit in Singapore. Crit. Care 2020, 24, 1–3. [Google Scholar] [CrossRef]
- Greenberg, N.; Docherty, M.; Gnanapragasam, S.; Wessely, S. Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ 2020, 368, m1211. [Google Scholar] [CrossRef] [PubMed]
- Gan, W.H.; Lim, J.W.; Koh, D. Preventing intra-hospital infection and transmission of COVID-19 in healthcare workers. [published online ahead of print, 2020 Mar 24]. Saf. Health Work 2020, 11, 241–243. [Google Scholar] [CrossRef] [PubMed]
- CDC COVID-19 Response Team. Severe Outcomes among Patients with Coronavirus Disease 2019 (COVID-19)—United States, February 12-March 16. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 3–43. [Google Scholar]
- Halpern, N.; Tan, K. United States Resource Availability for COVID-19. [online] Sccm.org. Available online: https://sccm.org/Blog/March-2020/United-States-Resource-Availability-for-COVID-19 (accessed on 18 March 2021).
- Na, S.J.; Chung, C.R.; Choi, H.J.; Cho, Y.H.; Sung, K.; Yang, J.H.; Suh, G.Y.; Jeon, K. The effect of multidisciplinary extracorporeal membrane oxygenation team on clinical out-comes in patients with severe acute respiratory failure. Ann. Intensive Care 2018, 8. [Google Scholar]
- Cioffi, J.; Ferguson, L. Team nursing in acute care settings: Nurses’ experiences. Contemp. Nurse 2009, 33, 2–12. [Google Scholar] [CrossRef]
- Fairbrother, G.; Jones, A.; Rivas, K. Changing model of nursing care from individual patient allocation to team nursing in the acute inpatient environment. Contemp. Nurse 2010, 35, 202–220. [Google Scholar] [CrossRef]
- Hanidziar, D.; Bittner, E.A. Sedation of Mechanically Ventilated COVID-19 Patients: Challenges and Special Considerations. Anesthesia Analg. 2020, 131, e40–e41. [Google Scholar] [CrossRef] [PubMed]
- Grant, M. Resolving Communication Challenges in the Intensive Care Unit. AACN Adv. Crit. Care 2015, 26, 123–130. [Google Scholar] [CrossRef]
- Munster, V.J.; Koopmans, M.; van Doremalen, N.; van Riel, D.; de Wit, E.A. Novel Coronavirus Emerging in China—Key Questions for Impact Assessment. N. Engl. J. Med. 2020, 382, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, L. Facing Covid-19 in Italy—Ethics, Logistics, and Therapeutics on the Epidemic’s Front Line. N. Engl. J. Med. 2020, 382, 1873–1875. [Google Scholar] [CrossRef]
- Goh, K.J.; Choong, M.C.; Cheong, E.H.; Kalimuddin, S.; Wen, S.D.; Phua, G.C.; Chan, K.S.; Mohideen, S.H. Rapid Progression to Acute Respiratory Distress Syndrome: Review of Current Understanding of Critical Illness from Coronavirus Disease 2019 (COVID-19) Infection. Ann. Acad. Med. Singap. 2020, 49, 108–118. [Google Scholar] [CrossRef] [PubMed]
- MacLaren, G.; Fisher, D.; Brodie, D. Preparing for the Most Critically Ill Patients with COVID-19: The potential role of extracorporeal membrane oxygenation. JAMA 2020, 323, 1245. [Google Scholar] [CrossRef]
- Zhan, W.-Q.; Li, M.-D.; Xu, M.; Lu, Y.-B. Successful treatment of COVID-19 using extracorporeal membrane oxygenation, a case report. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 3385–3389. [Google Scholar]
- Wells, C.L.; Forrester, J.; Vogel, J.; Rector, R.; Tabatabai, A.; Herr, D. Safety and Feasibility of Early Physical Therapy for Patients on Extracorporeal Membrane Oxygenator: University of Maryland Medical Center Experience. Crit. Care Med. 2018, 46, 53–59. [Google Scholar] [CrossRef]
- Pasrija, C.; Mackowick, K.M.; Raithel, M.; Tran, D.; Boulos, F.M.; Deatrick, K.B.; Mazzeffi, M.A.; Rector, R.; Pham, S.M.; Griffith, B.P.; et al. Ambulation With Femoral Arterial Cannulation Can Be Safely Performed on Venoarterial Extracorporeal Membrane Oxygenation. Ann. Thorac. Surg. 2019, 107, 1389–1394. [Google Scholar] [CrossRef] [PubMed]
- Abrams, D.; Javidfar, J.; Farrand, E.; Mongero, L.B.; Agerstrand, C.L.; Ryan, P.; Zemmel, D.; Galuskin, K.; Morrone, T.M.; Boerem, P.; et al. Early mobilization of patients receiving extracorporeal membrane oxygenation: A retrospective cohort study. Crit. Care 2014, 18, R38. [Google Scholar] [CrossRef]
- Ferreira, D.D.C.; Marcolino, M.A.Z.; Macagnan, F.E.; Plentz, R.D.M.; Kessler, A. Safety and potential benefits of physical therapy in adult patients on extracorporeal membrane oxygenation support: A systematic review. Segurança e potenciais benefícios da fisioterapia em adultos submetidos ao suporte de vida com oxigenação por membrana extracorpórea: Uma revisão sistemática. Rev. Bras. Ter. Intensiva 2019, 31, 227, Published 2019 May 13. [Google Scholar] [PubMed]
- Ramanathan, K.; Antognini, D.; Combes, A.; Paden, M.; Zakhary, B.; Ogino, M.; MacLaren, G.; Brodie, D.; Shekar, K. Planning and provision of ECMO services for severe ARDS during the COVID-19 pandemic and other outbreaks of emerging infectious diseases. Lancet Respir. Med. 2020, 8, 518–526. [Google Scholar] [CrossRef]
- Savarimuthu, S.; Binsaeid, J.; Harky, A. The role of ECMO in COVID-19: Can it provide rescue therapy in those who are critically ill? J. Card. Surg. 2020, 35, 1298–1301. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dave, S.; Shah, A.; Galvagno, S.; George, K.; Menne, A.R.; Haase, D.J.; McCormick, B.; Rector, R.; Dahi, S.; Madathil, R.J.; et al. A Dedicated Veno-Venous Extracorporeal Membrane Oxygenation Unit during a Respiratory Pandemic: Lessons Learned from COVID-19 Part I: System Planning and Care Teams. Membranes 2021, 11, 258. https://doi.org/10.3390/membranes11040258
Dave S, Shah A, Galvagno S, George K, Menne AR, Haase DJ, McCormick B, Rector R, Dahi S, Madathil RJ, et al. A Dedicated Veno-Venous Extracorporeal Membrane Oxygenation Unit during a Respiratory Pandemic: Lessons Learned from COVID-19 Part I: System Planning and Care Teams. Membranes. 2021; 11(4):258. https://doi.org/10.3390/membranes11040258
Chicago/Turabian StyleDave, Sagar, Aakash Shah, Samuel Galvagno, Kristen George, Ashley R. Menne, Daniel J. Haase, Brian McCormick, Raymond Rector, Siamak Dahi, Ronson J. Madathil, and et al. 2021. "A Dedicated Veno-Venous Extracorporeal Membrane Oxygenation Unit during a Respiratory Pandemic: Lessons Learned from COVID-19 Part I: System Planning and Care Teams" Membranes 11, no. 4: 258. https://doi.org/10.3390/membranes11040258
APA StyleDave, S., Shah, A., Galvagno, S., George, K., Menne, A. R., Haase, D. J., McCormick, B., Rector, R., Dahi, S., Madathil, R. J., Deatrick, K. B., Ghoreishi, M., Gammie, J. S., Kaczorowski, D. J., Scalea, T. M., Menaker, J., Herr, D., Krause, E., & Tabatabai, A. (2021). A Dedicated Veno-Venous Extracorporeal Membrane Oxygenation Unit during a Respiratory Pandemic: Lessons Learned from COVID-19 Part I: System Planning and Care Teams. Membranes, 11(4), 258. https://doi.org/10.3390/membranes11040258