
A Systematic Literature Review of Packed Red Cell Transfusion Usage in Adult Extracorporeal Membrane Oxygenation

Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Inclusion and Exclusion
2.3. Data Extraction, Quality Assessment and Analysis
3. Results
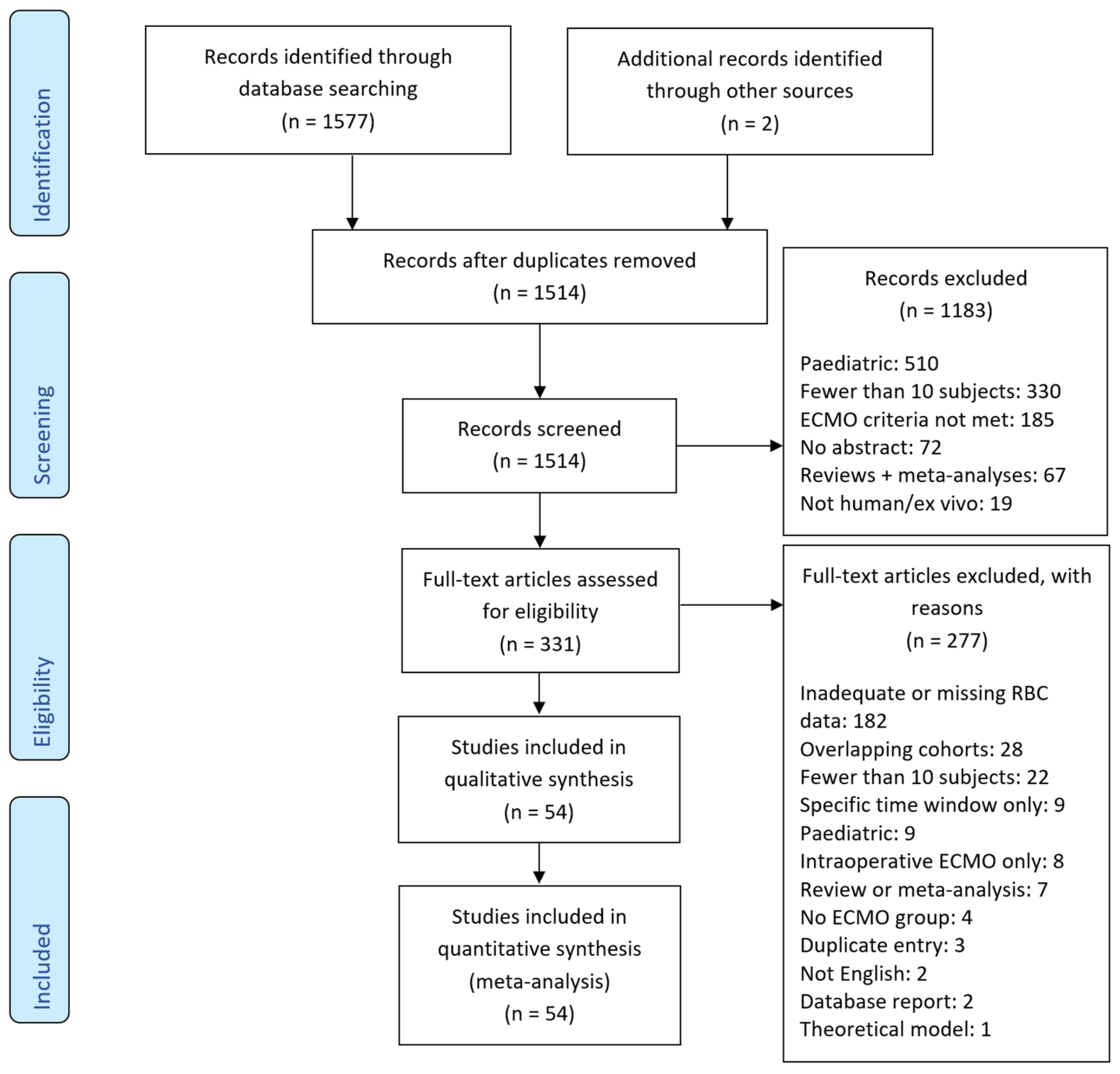
3.1. Search Results and Characteristics of Included Studies
3.2. Methodological Quality
3.3. Patient and ECMO Characteristics
3.4. Reported Complications
3.5. Transfusion Rates
4. Discussion
4.1. Data Quality
4.2. Limitations and Sources of Error
4.3. Implications for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Sy, E.; Sklar, M.C.; Lequier, L.; Fan, E.; Kanji, H.D. Anticoagulation practices and the prevalence of major bleeding, thromboembolic events, and mortality in venoarterial extracorporeal membrane oxygenation: A systematic review and meta-analysis. J. Crit. Care 2017, 39, 87–96. [Google Scholar] [CrossRef]
- Sklar, M.C.; Sy, E.; Lequier, L.; Fan, E.; Kanji, H.D. Anticoagulation practices during venovenous extracorporeal membrane oxygenation for respiratory failure. A systematic review. Ann. Am. Thorac. Soc. 2016, 13, 2242–2250. [Google Scholar] [CrossRef]
- Hebert, P.C.; Wells, G.; Blajchman, M.A.; Marshall, J.; Martin, C.; Pagliarello, G.; Tweeddale, M.; Schweitzer, I.; Yetisir, E. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. transfusion requirements in critical care investigators, canadian critical care trials group. N. Engl. J. Med. 1999, 340, 409–417. [Google Scholar] [CrossRef]
- Carson, J.L.; Stanworth, S.J.; Roubinian, N.; Fergusson, D.A.; Triulzi, D.; Doree, C.; Hebert, P.C. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst. Rev. 2016, 10, Cd002042. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’connell, D.; Peterson, V.; Welch, M.; Losos, M.; Tugwell, P.; Zello, G.A.; Robertson, J. The Newcastle-Ottawa Scale (NOS) For Assessing The Quality Of Nonrandomised Studies In Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 26 October 2020).
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Balduzzi, S.; Rucker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Anselmi, A.; Guinet, P.; Ruggieri, V.G.; Aymami, M.; Lelong, B.; Granry, S.; Malledant, Y.; Tulzo, L.Y.; Gueret, P.; Verhoye, J.P.; et al. Safety of recombinant factor VIIa in patients under extracorporeal membrane oxygenation. Eur. J. Cardiothorac. Surg. 2016, 49, 78–84. [Google Scholar] [CrossRef]
- Buscher, H.; Vukomanovic, A.; Benzimra, M.; Okada, K.; Nair, P. Blood and anticoagulation management in extracorporeal membrane oxygenation for surgical and nonsurgical patients: A Single-Center retrospective review. J. Cardiothorac. Vasc. Anesth. 2016, 31, 869–875. [Google Scholar] [CrossRef]
- Czobor, P.; Venturini, J.M.; Parikh, K.S.; Retzer, E.M.; Friant, J.; Jeevanandam, V.; Russo, M.J.; Uriel, N.; Paul, J.D.; Blair, J.E.; et al. Sequential organ failure assessment score at presentation predicts survival in patients treated with percutaneous veno-arterial extracorporeal membrane oxygenation. J. Invasive Cardiol. 2016, 28, 133–138. [Google Scholar]
- Hryniewicz, K.; Sandoval, Y.; Samara, M.; Bennett, M.; Cabuay, B.; Chavez, I.J.; Seatter, S.; Eckman, P.; Zimbwa, P.; Dunn, A.; et al. Percutaneous venoarterial extracorporeal membrane oxygenation for refractory cardiogenic shock is associated with improved short-and long-term survival. ASAIO J. 2016, 62, 397–402. [Google Scholar] [CrossRef]
- Krueger, K.; Schmutz, A.; Zieger, B.; Kalbhenn, J. Venovenous extracorporeal membrane oxygenation with prophylactic subcutaneous anticoagulation only: An observational study in more than 60 patients. Artif. Organs 2016, 41, 186–192. [Google Scholar] [CrossRef]
- Mazzeffi, M.; Greenwood, J.; Tanaka, K.; Menaker, J.; Rector, R.; Herr, D.; Kon, Z.; Lee, J.; Griffith, B.; Rajagopal, K.; et al. Bleeding, transfusion, and mortality on extracorporeal life support: ECLS working group on thrombosis and hemostasis. Ann. Thorac. Surg. 2016, 101, 682–689. [Google Scholar] [CrossRef]
- Opfermann, P.; Bevilacqua, M.; Fellim, A.; Mouhieddine, M.; Bachleda, T.; Pichler, T.; Hiesmayr, M.; Zuckermann, A.; Dworschak, M.; Steinlechner, B. Prognostic impact of persistent thrombocytopenia during extracorporeal membrane oxygenation: A retrospective analysis of prospectively collected data from a cohort of patients with left ventricular dysfunction after cardiac surgery. Crit. Care Med. 2016, 44, e1208–e1218. [Google Scholar] [CrossRef]
- Pan, K.C.; McKenzie, D.P.; Pellegrino, V.; Murphy, D.; Butt, W. The meaning of a high plasma free haemoglobin: Retrospective review of the prevalence of haemolysis and circuit thrombosis in an adult ECMO centre over 5 years. Perfusion 2016, 31, 223–231. [Google Scholar] [CrossRef]
- Staudacher, D.L.; Biever, P.M.; Benk, C.; Ahrens, I.; Bode, C.; Wengenmayer, T. Dual Antiplatelet Therapy (DAPT) versus no antiplatelet therapy and incidence of major bleeding in patients on venoarterial extracorporeal membrane oxygenation. PLoS ONE 2016, 11, e0159973. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, D.; Hirose, H.; Cavarocchi, N.; Entwistle, J.W.C. The impact of vascular complications on survival of patients on venoarterial extracorporeal membrane oxygenation. Ann. Thorac. Surg. 2016, 101, 1729–1734. [Google Scholar] [CrossRef] [PubMed]
- Tauber, H.; Streif, W.; Fritz, J.; Ott, H.; Weigel, G.; Loacker, L.; Heinz, A.; Velik-Salchner, C. Predicting transfusion requirements during extracorporeal membrane oxygenation. J. Cardiothorac. Vasc. Anesth. 2016, 30, 692–701. [Google Scholar] [CrossRef] [PubMed]
- Trudzinski, F.C.; Minko, P.; Rapp, D.; Fähndrich, S.; Haake, H.; Haab, M.; Bohle, R.M.; Flaig, M.; Kaestner, F.; Bals, R.; et al. Runtime and aPTT predict venous thrombosis and thromboembolism in patients on extracorporeal membrane oxygenation: A retrospective analysis. Ann. Intensive Care 2016, 6, 66. [Google Scholar] [CrossRef]
- Agerstrand, C.L.; Burkart, K.M.; Abrams, D.C.; Bacchetta, M.D.; Brodie, D. Blood conservation in extracorporeal membrane oxygenation for acute respiratory distress syndrome. Ann. Thorac. Surg. 2015, 99, 590–595. [Google Scholar] [CrossRef]
- Esper, S.A.; Bermudez, C.; Dueweke, E.J.; Kormos, R.; Subramaniam, K.; Mulukutla, S.; Sappington, P.; Waters, J.; Khandhar, S.J. Extracorporeal Membrane oxygenation support in acute coronary syndromes complicated by cardiogenic shock. Catheter. Cardiovasc. Interv. 2015, 86, S45–S50. [Google Scholar] [CrossRef]
- Halaweish, I.; Cole, A.; Cooley, E.; Lynch, W.R.; Haft, J.W. Roller and centrifugal pumps: A retrospective comparison of bleeding complications in extracorporeal membrane oxygenation. ASAIO J. 2015, 61, 496–501. [Google Scholar] [CrossRef]
- Marius, H.; Sommer, W.; Tudorache, I.; Avsar, M.; Siemeni, T.; Salman, J.; Puntigam, J.; Optenhoefel, J.; Greer, M.; Welte, T.; et al. Veno-veno-arterial extracorporeal membrane oxygenation for respiratory failure with severe haemodynamic impairment: Technique and early outcomes. Interact. Cardiovasc. Thorac. Surg. 2015, 20, 761–767. [Google Scholar]
- Lehle, K.; Philipp, A.; Zeman, F.; Lunz, D.; Lubnow, M.; Wendel, H.-P.; Göbölös, L.; Schmid, C.; Müller, T. Technical-induced hemolysis in patients with respiratory failure supported with veno-venous ECMO—Prevalence and risk factors. PLoS ONE 2015, 10, e0143527. [Google Scholar] [CrossRef] [PubMed]
- Li, C.-L.; Wang, H.; Jia, M.; Ma, N.; Meng, X.; Hou, X.-T. The early dynamic behavior of lactate is linked to mortality in postcardiotomy patients with extracorporeal membrane oxygenation support: A retrospective observational study. J. Thorac. Cardiovasc. Surg. 2015, 149, 1445–1450. [Google Scholar] [CrossRef] [PubMed]
- Mohite, P.N.; Kaul, S.; Sabashnikov, A.; Rashid, N.; Fatullayev, J.; Zych, B.; Popov, A.-F.; Maunz, O.; Patil, N.P.; Garcia-Saez, D.; et al. Extracorporeal life support in patients with refractory cardiogenic shock: Keep them awake. Interact. Cardiovasc. Thorac. Surg. 2015, 20, 755–760. [Google Scholar] [CrossRef]
- Omar, H.R.; Mirsaeidi, M.; Socias, S.; Sprenker, C.; Caldeira, C.; Camporesi, E.M.; Mangar, D. Plasma free hemoglobin is an independent predictor of mortality among patients on extracorporeal membrane oxygenation support. PLoS ONE 2015, 10, e0124034. [Google Scholar]
- Panigada, M.; L’Acqua, C.; Passamonti, S.M.; Mietto, C.; Protti, A.; Riva, R.; Gattinoni, L. Comparison between clinical indicators of transmembrane oxygenator thrombosis and multidetector computed tomographic analysis. J. Crit. Care 2015, 30, 441.e7–441.e13. [Google Scholar] [CrossRef]
- Poss, J.; Kriechbaum, S.; Ewen, S.; Graf, J.; Hager, I.; Hennersdorf, M.; Petros, S.; Link, A.; Bohm, M.; Thiele, H.; et al. First-in-man analysis of the i-cor assist device in patients with cardiogenic shock. Eur. Heart J. Acute Cardiovasc. Care 2015, 4, 475–481. [Google Scholar] [CrossRef]
- San Roman, E.; Venuti, M.S.; Ciarrocchi, N.M.; Fernandez Ceballos, I.; Gogniat, E.; Villarroel, S.; Carini, F.C.; Giannasi, S.E. Implementation and results of a new ECMO program for lung transplantation and acute respiratory distress. Rev. Bras. Ter. Intensiva 2015, 27, 134–140. [Google Scholar] [CrossRef]
- Voelker, M.T.; Busch, T.; Bercker, S.; Fichtner, F.; Kaisers, U.X.; Laudi, S. Restrictive transfusion practice during extracorporeal membrane oxygenation therapy for severe acute respiratory distress syndrome. Artif. Organs 2015, 39, 374–378. [Google Scholar] [CrossRef]
- Wu, S.-C.; Chen, W.T.-L.; Lin, H.-H.; Fu, C.-Y.; Wang, Y.-C.; Lo, H.-C.; Cheng, H.-T.; Tzeng, C.-W. Use of extracorporeal membrane oxygenation in severe traumatic lung injury with respiratory failure. Am. J. Emerg. Med. 2015, 33, 658–662. [Google Scholar] [CrossRef]
- Guirand, D.M.; Okoye, O.T.; Schmidt, B.S.; Mansfield, N.J.; Aden, J.K.; Martin, R.S.; Cestero, R.F.; Hines, M.H.; Pranikoff, T.; Inaba, K.; et al. Venovenous extracorporeal life support improves survival in adult trauma patients with acute hypoxemic respiratory failure: A multicenter retrospective cohort study. J. Trauma Acute Care Surg. 2014, 76, 1275–1281. [Google Scholar] [CrossRef] [PubMed]
- Loforte, A.; Marinelli, G.; Musumeci, F.; Folesani, G.; Pilato, E.; Martin Suarez, S.; Montalto, A.; Lilla Della Monica, P.; Grigioni, F.; Frascaroli, G.; et al. Extracorporeal membrane oxygenation support in refractory cardiogenic shock: Treatment strategies and analysis of risk factors. Artif. Organs 2014, 38, 129–141. [Google Scholar] [CrossRef]
- DaRocha, T.; Kosiński, S.; Jarosz, A.; Sobczyk, D.; Gałązkowski, R.; Piątek, J.; Konstany-Kalandyk, J.; Drwiła, R. The chain of survival in hypothermic circulatory arrest: Encouraging preliminary results when using early identification, risk stratification and extracorporeal rewarming. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 85. [Google Scholar] [CrossRef]
- Shum, H.-P.; Kwan, A.M.-C.; Chan, K.-C.; Yan, W.-W. The use of regional citrate anticoagulation continuous venovenous hemofiltration in extracorporeal membrane oxygenation. ASAIO J. 2014, 60, 413–418. [Google Scholar] [CrossRef]
- Fagnoul, D.; Taccone, F.S.; Belhaj, A.; Rondelet, B.; Argacha, J.-F.; Vincent, J.L.; De Backer, D. Extracorporeal life support associated with hypothermia and normoxemia in refractory cardiac arrest. Resuscitation 2013, 84, 1519–1524. [Google Scholar] [CrossRef]
- Michaels, A.J.; Hill, J.G.; Bliss, D.; Sperley, B.P.; Young, B.P.; Quint, P.; Shanks, T.R.; Dalthorp, J.; Long, W.B.; Morgan, L.J. Pandemic flu and the sudden demand for ECMO resources: A mature trauma program can provide surge capacity in acute critical care crises. J. Trauma Acute Care Surg. 2013, 74, 1493–1497. [Google Scholar] [CrossRef]
- Mikus, E.; Tripodi, A.; Calvi, S.; Del Giglio, M.; Cavallucci, A.; Lamarra, M. CentriMag venoarterial extracorporeal membrane oxygenation support as treatment for patients with refractory postcardiotomy cardiogenic shock. ASAIO J. 2013, 59, 18–23. [Google Scholar] [CrossRef]
- Pieri, M.; Turla, O.G.; Calabro, M.G.; Ruggeri, L.; Agracheva, N.; Zangrillo, A.; Pappalardo, F. A new phosphorylcholine-coated polymethylpentene oxygenator for extracorporeal membrane oxygenation: A preliminary experience. Perfusion 2013, 28, 132–137. [Google Scholar] [CrossRef]
- Repesse, X.; Au, S.M.; Brechot, N.; Trouillet, J.-L.; Leprince, P.; Chastre, J.; Combes, A.; Luyt, C.-E. Recombinant factor VIIa for uncontrollable bleeding in patients with extracorporeal membrane oxygenation: Report on 15 cases and literature review. Crit. Care 2013, 17, R55. [Google Scholar] [CrossRef]
- Loforte, A.; Montalto, A.; Ranocchi, F.; Della Monica, P.L.; Casali, G.; Lappa, A.; Menichetti, A.; Contento, C.; Musumeci, F. Peripheral extracorporeal membrane oxygenation system as salvage treatment of patients with refractory cardiogenic shock: Preliminary outcome evaluation. Artif. Organs 2012, 36, E53–E61. [Google Scholar] [CrossRef]
- Park, M.; Azevedo, L.C.; Mendes, P.V.; Carvalho, C.R.; Amato, M.B.; Schettino, G.P.; Tucci, M.; Maciel, A.T.; Taniguchi, L.U.; Barbosa, E.V.; et al. First-year experience of a Brazilian tertiary medical center in supporting severely ill patients using extracorporeal membrane oxygenation. Clinics 2012, 67, 1157–1163. [Google Scholar] [CrossRef]
- Garcia, J.P.; Kon, Z.N.; Evans, C.; Wu, Z.; Iacono, A.T.; McCormick, B.; Griffith, B.P. Ambulatory veno-venous extracorporeal membrane oxygenation: Innovation and pitfalls. J. Thorac. Cardiovasc. Surg. 2011, 142, 755–761. [Google Scholar] [CrossRef]
- Han, S.J.; Kim, H.S.; Kim, K.I.; Whang, S.M.; Hong, K.S.; Lee, W.K.; Lee, S.H. Use of nafamostat mesilate as an anticoagulant during extracorporeal membrane oxygenation. J. Korean Med. Sci. 2011, 26, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Lamarche, Y.; Cheung, A.; Ignaszewski, A.; Higgins, J.; Kaan, A.; Griesdale, D.E.; Moss, R. Comparative outcomes in cardiogenic shock patients managed with Impella microaxial pump or extracorporeal life support. J. Thorac. Cardiovasc. Surg. 2011, 142, 60–65. [Google Scholar] [CrossRef]
- Formica, F.; Avalli, L.; Colagrande, L.; Ferro, O.; Greco, G.; Maggioni, E.; Paolini, G. Extracorporeal membrane oxygenation to support adult patients with cardiac failure: Predictive factors of 30-day mortality. Interact. Cardiovasc. Thorac. Surg. 2010, 10, 721–726. [Google Scholar] [CrossRef]
- Kanji, H.D.; Schulze, C.J.; Oreopoulos, A.; Lehr, E.J.; Wang, W.; MacArthur, R.M. Peripheral versus central cannulation for extracorporeal membrane oxygenation: A comparison of limb ischemia and transfusion requirements. Thorac. Cardiovasc. Surg. 2010, 58, 459–462. [Google Scholar] [CrossRef]
- Marasco, S.F.; Vale, M.; Pellegrino, V.; Preovolos, A.; Leet, A.; Kras, A.; Schulberg, E.; Bergin, P.; Esmore, D.S. Extracorporeal membrane oxygenation in primary graft failure after heart transplantation. Ann. Thorac. Surg. 2010, 90, 1541–1546. [Google Scholar] [CrossRef]
- Rastan, A.J.; Dege, A.; Mohr, M.; Doll, N.; Falk, V.; Walther, T.; Mohr, F.W. Early and late outcomes of 517 consecutive adult patients treated with extracorporeal membrane oxygenation for refractory postcardiotomy cardiogenic shock. J. Thorac. Cardiovasc. Surg. 2010, 139, 302–311.e1. [Google Scholar] [CrossRef]
- Ang, A.L.; Teo, D.; Lim, C.H.; Leou, K.K.; Tien, S.L.; Koh, M.B.C. Blood transfusion requirements and independent predictors of increased transfusion requirements among adult patients on extracorporeal membrane oxygenation - a single centre experience. Vox Sang. 2009, 96, 34–43. [Google Scholar] [CrossRef]
- Davies, A.; Jones, D.; Bailey, M.; Beca, J.; Bellomo, R.; Blackwell, N.; Forrest, P.; Gattas, D.; Granger, E.; Herkes, R.; et al. Extracorporeal membrane oxygenation for 2009 influenza A(H1N1) acute respiratory distress syndrome. J. Am. Med. Assoc. 2009, 302, 1888–1895. [Google Scholar]
- Müller, T.; Philipp, A.; Luchner, A.; Karagiannidis, C.; Bein, T.; Hilker, M.; Rupprecht, L.; Langgartner, J.; Zimmermann, M.; Arlt, M.; et al. A new miniaturized system for extracorporeal membrane oxygenation in adult respiratory failure. Crit. Care 2009, 13, R205. [Google Scholar] [CrossRef]
- Bakhtiary, F.; Keller, H.; Dogan, S.; Dzemali, O.; Oezaslan, F.; Meininger, D.; Ackermann, H.; Zwissler, B.; Kleine, P.; Moritz, A. Venoarterial extracorporeal membrane oxygenation for treatment of cardiogenic shock: Clinical experiences in 45 adult patients. J. Thorac. Cardiovasc. Surg. 2008, 135, 382–388. [Google Scholar] [CrossRef]
- Dietl, C.A.; Wernly, J.A.; Pett, S.B.; Yassin, S.F.; Sterling, J.P.; Dragan, R.; Milligan, K.; Crowley, M.R. Extracorporeal membrane oxygenation support improves survival of patients with severe Hantavirus cardiopulmonary syndrome. J. Thorac. Cardiovasc. Surg. 2008, 135, 579–584. [Google Scholar] [CrossRef]
- Frenckner, B.; Palmér, P.; Lindén, V. Extracorporeal respiratory support and minimally invasive ventilation in severe ARDS. Minerva Anestesiol. 2002, 68, 381–386. [Google Scholar]
- Smith, C.; Bellomo, R.; Raman, J.S.; Matalanis, G.; Rosalion, A.; Buckmaster, J.; Hart, G.; Silvester, W.; Gutteridge, G.A.; Smith, B.; et al. An extracorporeal membrane oxygenation-based approach to cardiogenic shock in an older population. Ann. Thorac. Surg. 2001, 71, 1421–1427. [Google Scholar] [CrossRef]
- Lewandowski, K.; Rossaint, R.; Pappert, D.; Gerlach, H.; Slama, K.-J.; Weidemann, H.; Frey, D.J.M.; Hoffmann, O.; Keske, U.; Falke, K.J. High survival rate in 122 ARDS patients managed according to a clinical algorithm including extracorporeal membrane oxygenation. Intensiv. Care Med. 1997, 23, 819–835. [Google Scholar] [CrossRef]
- Peek, G.J.; Moore, H.M.; Moore, N.; Sosnowski, A.W.; Firmin, R.K. Extracorporeal membrane oxygenation for adult respiratory failure. Chest 1997, 112, 759–764. [Google Scholar] [CrossRef]
- Butch, S.H.; Knafl, P.; Oberman, H.A.; Bartlett, R.H. Blood utilization in adult patients undergoing extracorporeal membrane oxygenated therapy. Transfusion 1996, 36, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Muehrcke, D.D.; McCarthy, P.M.; Stewart, R.W.; Foster, R.C.; Ogella, D.A.; Borsh, J.A.; Cosgrove, D.M., 3rd. Extracorporeal membrane oxygenation for postcardiotomy cardiogenic shock. Ann. Thorac. Surg. 1996, 61, 684–691. [Google Scholar] [CrossRef]
- Winkler, A.; Brogan, T.; Lequier, L.; Lorusso, R. Transfusion management during extracorporeal support. In Extracorporeal Life Support: ELSO Red Book; ELSO—Extracorporeal Life Support Organization: Ann Arbor, MI, USA, 2018. [Google Scholar]
- Guimbretière, G.; Anselmi, A.; Roisne, A.; Lelong, B.; Corbineau, H.; Langanay, T.; Flécher, E.; Verhoye, J.-P. Prognostic impact of blood product transfusion in VA and VV ECMO. Perfusion 2019, 34, 246–253. [Google Scholar] [CrossRef]
- Mariscalco, G.; Salsano, A.; Fiore, A.; Dalén, M.; Ruggieri, V.G.; Saeed, D.; Jónsson, K.; Gatti, G.; Zipfel, S.; Dell’Aquila, A.M.; et al. Peripheral versus central extracorporeal membrane oxygenation for postcardiotomy shock: Multicenter registry, systematic review, and meta-analysis. J. Thorac. Cardiovasc. Surg. 2020, 160, 1207–1216.e44. [Google Scholar] [CrossRef]
- Jäämaa-Holmberg, S.; Salmela, B.; Suojaranta, R.; Jokinen, J.J.; Lemström, K.B.; Lommi, J. Extracorporeal membrane oxygenation for refractory cardiogenic shock: Patient survival and health-related quality of life. Eur. J. Cardio-Thorac. Surg. 2018, 55, 780–787. [Google Scholar] [CrossRef]
- Aubron, C.; Depuydt, J.; Belon, F.; Bailey, M.; Schmidt, M.; Sheldrake, J.; Murphy, D.; Scheinkestel, C.; Cooper, D.J.; Capellier, G.; et al. Predictive factors of bleeding events in adults undergoing extracorporeal membrane oxygenation. Ann. Intensiv. Care 2016, 6, 97. [Google Scholar] [CrossRef]
- Paone, G.; Likosky, D.S.; Brewer, R.; Theurer, P.F.; Bell, G.F.; Cogan, C.M.; Prager, R.L. Transfusion of 1 and 2 units of red blood cells is associated with increased morbidity and mortality. Ann. Thorac. Surg. 2014, 97, 87–94. [Google Scholar] [CrossRef]
- Khoshbin, E.; Roberts, N.; Harvey, C.; Machin, D.; Killer, H.; Peek, G.J.; Sosnowski, A.W.; Firmin, R.K. Poly-Methyl pentene oxygenators have improved gas exchange capability and reduced transfusion requirements in adult extracorporeal membrane oxygenation. ASAIO J. 2005, 51, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Cahill, C.M.; Blumberg, N.; Schmidt, A.E.; Knight, P.A.; Melvin, A.L.; Massey, H.T.; Delehanty, J.M.; Zebrak, S.B.; Refaai, M.A. Implementation of a standardized transfusion protocol for cardiac patients treated with venoarterial extracorporeal membrane oxygenation is associated with decreased blood component utilization and may improve clinical outcome. Anesth. Analg. 2018, 126, 1262–1267. [Google Scholar] [CrossRef] [PubMed]
- De Bruin, S.; Scheeren, T.W.L.; Bakker, J.; van Bruggen, R.; Vlaar, A.P.J. Transfusion practice in the non-bleeding critically ill: An international online survey-the TRACE survey. Crit. Care 2019, 23, 309. [Google Scholar] [CrossRef] [PubMed]
- Martucci, G.; Grasselli, G.; Tanaka, K.; Tuzzolino, F.; Panarello, G.; Schmidt, M.; Bellani, G.; Arcadipane, A. hemoglobin trigger and approach to red blood cell transfusions during veno-venous extracorporeal membrane oxygenation: The international TRAIN-ECMO survey. Perfusion 2019, 34, 39–48. [Google Scholar] [CrossRef]
- Holst, L.B.; Haase, N.; Wetterslev, J.; Wernerman, J.; Guttormsen, A.B.; Karlsson, S.; Johansson, P.I.; Åneman, A.; Vang, M.L.; Winding, R.; et al. Lower versus higher hemoglobin threshold for transfusion in septic shock. N. Engl. J. Med. 2014, 371, 1381–1391. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, C.; Colomo, A.; Bosch, A.; Concepción, M.; Hernandez-Gea, V.; Aracil, C.; Graupera, I.; Poca, M.; Alvarez-Urturi, C.; Gordillo, J.; et al. Transfusion strategies for acute upper gastrointestinal bleeding. N. Engl. J. Med. 2013, 368, 11–21. [Google Scholar] [CrossRef]
- Mazer, C.D.; Whitlock, R.P.; Fergusson, D.A.; Hall, J.; Belley-Cote, E.; Connolly, K.; Khanykin, B.; Gregory, A.J.; De Médicis, É.; McGuinness, S.; et al. Restrictive or liberal red-cell transfusion for cardiac surgery. N. Engl. J. Med. 2017, 377, 2133–2144. [Google Scholar] [CrossRef]
- Lamarche, Y.; Chow, B.; Bédard, A.; Johal, N.; Kaan, A.; Humphries, K.H.; Cheung, A. Thromboembolic events in patients on extracorporeal membrane oxygenation without anticoagulation. Innov. Technol. Tech. Cardiothorac. Vasc. Surg. 2010, 5, 424–429. [Google Scholar] [CrossRef]
- Wood, K.L.; Ayers, B.; Gosev, I.; Kumar, N.; Melvin, A.L.; Barrus, B.; Prasad, S. Venoarterial-extracorporeal membrane oxygenation without routine systemic anticoagulation decreases adverse events. Ann. Thorac. Surg. 2020, 109, 1458–1466. [Google Scholar] [CrossRef]
- Carter, K.T.; Kutcher, M.E.; Shake, J.G.; Panos, A.L.; Cochran, R.P.; Creswell, L.L.; Copeland, H. Heparin-sparing anticoagulation strategies are viable options for patients on veno-venous ECMO. J. Surg. Res. 2019, 243, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author/Year (Reference) | Location | Study Period Start and End Year | N | ECMO Type (VA/VV/Not Spec) | ECMO Days (Mean +/−SD) | Transfusion Trigger (g/dL or HCt %) | % Not Transfused PRBC on ECMO | PRBC/Day (Mean +/−SD) | Survival to Discharge (%) | Study Type | Brief Description |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Anselmi 2016 [9] | France | 2005–2014 | 30 | 27/3/0 | 8.9 (+/−7.3) | 24% | 0.0% | 2.97 (+/−1.63) | 50.0% | R. obs | Mixed—cardiogenic shock after heart transplant (47%) or cardiotomy (40%) and small number of respiratory failures—cohort report on use of recombinant factor VIIa |
| Buscher 2016 [10] | Australia | 2009–2010 | 48 | 32/16/0 | 8.0 (+/−7.0) | 8 g/dl | 8.3% | 1.57 (+/−1.79) | 69.0% | R. obs | Mixed—cardiogenic shock of all causes, including eCPR and severe respiratory failure (mostly ARDS but 3 post-transplant) |
| Czobor 2016 [11] | USA | 2012–2014 | 25 | 25/0/0 | NR | 8.0% | 40.0% | R. obs | Nonsurgical—cardiogenic shock and eCPR—cohort report on predictive utility of SOFA score | ||
| Hryniewicz 2016 [12] | USA | 2012–2013 | 37 | 37/0/0 | 4.7 (+/−2.3) | 8.1% | 2.52 (+/−1.61) | 64.9% | R. obs | Mixed cardiogenic shock post-AMI (18), cardiotomy (5), decompensated failure (6) | |
| Krueger 2016 [13] | Germany | 2011–2015 | 61 | 0/61/0 | 12.0 (+/−6.5) | 10 g/dL | 1.15 (+/−1.35) | R. obs | Nonsurgical—respiratory failure, principally ARDS—cohort review for outcomes of anticoagulation with VTE prophylaxis only in VV ECMO patients | ||
| Mazzeffi 2016 [14] | USA | 2010–2013 | 132 | 68/54/0 | 8.0 (+/−6.7) | 2.42 (+/−1.97) | 50.8% | R. obs | Mixed—cardiogenic shock, mostly postcardiotomy (38) and ARDS (54)—cohort review for predictors of bleeding events | ||
| Opfermann 2016 [15] | Austria | 2001–2014 | 300 | 300/0/0 | 6.1 (+/−4.8) | 0.74 (+/−0.79) | 51.7% | R. obs | Surgical—cardiogenic shock postcardiotomy—cohort review for predictors of survival | ||
| Pan 2016 [16] | Australia | 2010–2014 | 184 | 128/56/0 | 7.0 (+/−4.9) | 1.30 (+/−1.33) | 73.4% | R. obs | Mixed—cardiogenic shock of varying causes, including postcardiotomy, post-transplant and severe respiratory failure of multiple causes—cohort review for predictors of elevated plasma-free Hb | ||
| Staudacher 2016 [17] | Germany | 2010–2013 | 90 | 90/0/0 | 2.2 (+/−2.7) | 8 g/dL | 67.8% | 0.79 (+/−1.51) | 24.4% | R. obs | Nonsurgical—cardiogenic shock after arrest or AMI—cohort comparison of outcomes of antiplatelet therapy vs. none |
| Tanaka 2016 [18] | USA | 2010–2014 | 84 | 84/0/0 | 41.7% | R. obs | Mixed—mostly cardiogenic shock, small postcardiotomy group—cohort review of predictors for vascular access complications | ||||
| Tauber 2016 [19] | Austria | 2010–2012 | 38 | 26/12/0 | 8.5 g/dL | 0.0% | 1.65 (+/−1.87) | Prosp. obs | Mixed—cardiogenic shock and severe respiratory failure—cohort review for predictors of higher transfusion requirement | ||
| Trudzinski 2016 [20] | Germany | 2010–2015 | 63 | 0/63/0 | 22.4 (+/−17.4) | 7 g/dL (or ScvO2<65%) | 0.98 (+/−1.17) | 66.7% | R. obs | Nonsurgical—half ARDS, half chronic lung disease awaiting transplant | |
| Agerstrand 2015 [21] | USA | 2010–2012 | 38 | 4/34/0 | 9.2 (+/−3.5) | 7g/dL | 36.8% | 0.15 (+/−0.25) | 73.7% | R. obs | Nonsurgical—respiratory +/− cardiac failure due to ARDS of varying aetiologies—cohort report on restrictive approach to transfusions |
| Esper 2015 [22] | USA | 2007–2013 | 18 | 18/0/0 | 3.3 (+/−2.2) | 5.6% | 3.47 (+/−2.36) | 66.7% | R. obs | Nonsurgical—cardiogenic shock after AMI | |
| Halaweish 2015 [23] | USA | 2002–2013 | 95 | 18/66/11 | 15.5 (+/−13.4) | 0.18 (+/−0.16) | 63.2% | R. obs | Mixed—mainly respiratory failure (75); also cardiogenic shock (14) and eCPR (6)—cohort comparison of roller and centrifugal pumps, only duration >5days | ||
| Ius 2015 [24] | Germany | 2012–2014 | 10 | 10/0/0 | 10.2 (+/−4.2) | 10.0% | 1.75 (+/−1.78) | 50.0% | R. obs | Nonsurgical—acute on chronic respiratory failure—cohort of VV ECMO requiring conversion to VV-A | |
| Lehle 2015 [25] | Germany | 2009–2014 | 318 | 0/318/0 | 8 g/dL | 0.31 (+/−0.36) | R. obs | Nonsurgical—mixed respiratory failure cohort (pneumonia, trauma, acute on chronic lung disease, pulmonary haemorrhage)—cohort report on predictors of ECMO-associated haemolysis | |||
| Li 2015 [26] | China | 2011–2012 | 123 | 123/0/0 | 4.3 (+/−3.7) | 30% | 4.49 (+/−2.88) | 34.1% | R. obs | Surgical—cardiogenic shock post-cardiotomy | |
| Mohite 2015 [27] | UK | 2010–2014 | 59 | 59/0/0 | 8.9 (+/−5.1) | 2.56 (+/−1.81) | R. obs | Mixed—cardiogenic shock (decompensated heart failure, postcardiotomy, post-AMI)—cohort comparison of outcomes between sedated and “awake” ECMO patients | |||
| Omar 2015 [28] | USA | 2007–2013 | 154 | 126/28/0 | 5.6 (+/−6.6) | 5.50 (+/−5.71) | 33.1% | R. obs | Mixed—mainly cardiogenic shock (cardiomyopathy, eCPR, AMI, postcardiotomy, heart transplant, PE) with smaller group respiratory failure and lung transplant—cohort report on predictors of mortality on ECMO, including plasma-free Hb | ||
| Panigada 2015 [29] | Italy | 2011–2013 | 22 | 0/22/0 | 9.0 (+/−5.5) | 0.97 (+/−1.09) | Prosp. obs | Nonsurgical—respiratory failure due to ARDS/COPD or bridge to lung transplant—cohort report comparing clinical, lab and CT findings for oxygenator thrombosis | |||
| Poss 2015 [30] | Germany | 2012–2013 | 15 | 15/0/0 | 26.7% | 66.7% | R. obs 3ctr | Nonsurgical—cardiogenic shock, mostly post-AMI, some myocarditis—cohort comparison of ECMO vs. i-Cor assist device | |||
| San Roman 2015 [31] | Argentina | 2011–2014 | 22 | 9/13/0 | 5.1 (+/−4.3) | 0.0% | 0.89 (+/−1.02) | 68.2% | R. obs | Mixed—cardiorespiratory failure in pre- and postoperative lung transplant plus group of non-transplant respiratory failure | |
| Voelker 2015 [32] | Germany | 2009–2011 | 18 | 0/18/0 | 21.7 (+/−30.0) | 7 g/dL | 1.35 (+/−1.16) | 61.1% | R. obs | Nonsurgical—respiratory failure (pneumonia, trauma, other)—cohort report on restrictive transfusion approach | |
| Wu 2015 [33] | Taiwan | 2008–2014 | 19 | 10/9/0 | 7.0 (+/−4.8) | 3.49 (+/−3.62) | 68.4% | R. obs | Nonsurgical—respiratory failure (trauma-associated ARDS) | ||
| Guirand 2014 [34] | USA | 2001–2009 | 26 | 0/26/0 | 9.3 (+/−9.5) | 0.90 (+/−0.36) | 57.7% | R. obs | Nonsurgical—respiratory failure (trauma-associated ARDS) | ||
| Loforte 2014 [35] | Italy | 2006–2012 | 228 | 228/0/0 | 10.8 (+/−9.2) | 28% | 0.0% | 1.29 (+/−1.03) | 63.2% | R. obs 2 ctr | Mixed—cardiogenic shock, mostly postcardiotomy (118), transplant failure (37), post-AMI (27), decompensated heart failure (40) and myocarditis (6) |
| Roch 2014 [36] | France | 2009–2013 | 85 | 8/77/0 | 9.7 (+/−4.5) | 10 g/dL | 0.90 (+/−0.86) | 43.5% | R. obs | Nonsurgical—respiratory failure (ARDS) | |
| Shum 2014 [37] | Hong Kong | 2009–2013 | 37 | 13/24/0 | 5.5 (+/−2.3) | 0.0% | 0.53 (+/−0.72) | 73.0% | R. obs | Nonsurgical—mostly pneumonia, smaller cohort myocarditis—cohort report on regional citrate anticoagulation for haemodialysis access via ECMO circuit | |
| Fagnoul 2013 [38] | Belgium | 2012–2012 | 24 | 24/0/0 | 1.6 (+/−2.1) | 7 g/dL | 12.5% | 8.90 (+/−11.25) | 25.0% | Prosp. obs | Nonsurgical—eCPR |
| Michaels 2013 [39] | USA | 2009–2010 | 15 | 7/8/0 | 9.8 (+/−1.0) | 3.90 (NR) | 60.0% | R. obs | Nonsurgical—respiratory failure (H1N1 influenza) | ||
| Mikus 2013 [40] | Italy | 2007–2011 | 14 | 14/0/0 | 9.0 (+/−13.8) | 28% | 0.0% | 6.00 (+/−0.84) | 42.9% | R. obs | Surgical—postcardiotomy cardiogenic shock—cohort report on CentriMag pump |
| Pieri 2013 [41] | Italy | 2009–2012 | 16 | 13/3/0 | 6.0 (+/−4.0) | 8 g/dL28% | 1.58 (+/−1.20) | R. obs | Mixed—cardiogenic shock (mixed primary CS or postsurgical) or ARDS—cohort report on use of phosphorylcholine-coated oxygenator | ||
| Repesse 2013 [42] | France | 2006–2011 | 15 | 11/4/0 | 17.3 (+/−8.9) | 24% | 0.96 (+/−0.26) | R. obs | Mixed—cardiogenic shock (mixed primary CS or postsurgical) or ARDS—cohort report of use of recombinant factor VIIa for refractory bleeding on ECMO | ||
| Loforte 2012 [43] | Italy | 2007–2011 | 73 | 73/0/0 | 10.9 (+/−7.6) | 28% | 0.0% | 1.23 (+/−1.04) | 45.2% | R. obs | Mixed—cardiogenic shock, mostly postcardiotomy (50/73), 12/73 post-AMI and 8/73 post-heart transplant |
| Park 2012 [44] | Brazil | Not reported | 10 | 2/8/0 | 9.2 (+/−9.4) | 60.0% | 0.24 (+/−0.39) | 40.0% | R. obs | Nonsurgical—mixed respiratory failure (mostly pneumonia)—cohort of patients from commencement of ECMO service in this hospital | |
| Garcia 2011 [45] | USA | 2009–2009 | 10 | 0/10/0 | 20.0 (+/−15.0) | 35% | 2.44 (+/−1.60) | 60.0% | R. obs | Nonsurgical—mixed respiratory failure (ARDS, advanced chronic respiratory disease pending lung Tx)—cohort report on ambulating VV ECMO patients | |
| Han 2011 [46] | South Korea | 2006–2009 | 68 | 59/9/0 | 5.3 (+/−6.6) | 35% | 6.03 (+/−6.23) | R. obs | Nonsurgical—cardiogenic shock or respiratory failure (ARDS)—comparison of nafamostat vs. heparin for anticoagulation during ECMO; large cohort of eCPR (41/68) | ||
| Lamarche 2011 [47] | Canada | 2000–2009 | 32 | 32/0/0 | 2.2 (+/−2.0) | 9.08 (+/−8.66) | R. obs | Mixed—cardiogenic shock, primary or associated with cardiac surgery, some eCPR-comparison of Impella vs. ECMO | |||
| Formica 2010 [48] | Italy | 2002–2009 | 42 | 42/0/0 | 7.9 (+/−5.3) | 30% | 3.10 (+/−3.90) | 38.1% | R. obs | Mixed—cardiogenic shock, primary or associated with cardiac surgery, 2/42 massive PE | |
| Kanji 2010 [49] | Canada | 2002–2006 | 50 | 50/0/0 | 2.9 (+/−2.6) | 10 g/dL | 12.38 (NR) | R. obs | Mixed—cardiogenic shock, primary or associated with cardiac surgery—comparison of peripheral vs. central cannulation with respect to transfusion and bleeding events | ||
| Marasco 2010 [50] | Australia | 2000–2009 | 39 | 39/0/0 | 6.8 (+/−2.6) | 8 g/dL | 3.15 (+/−1.99) | R. obs | Surgical—post-heart transplant primary graft failure | ||
| Rastan 2010 [51] | Germany | 1996–2008 | 517 | 517/0/0 | 3.3 (+/−2.9) | 4.12 (+/−3.67) | 24.8% | R. obs | Surgical—postcardiotomy cardiogenic shock | ||
| Ang 2009 [52] | Singapore | 2003–2006 | 42 | 37/5/0 | 6.5 (+/−3.2) | 10 g/dL | 2.08 (+/−1.49) | 26.2% | R. obs | Mixed—pre- and post-cardiac surgery, myocarditis, PE, severe respiratory failure | |
| Davies 2009 [53] | Australia | 2009–2009 | 68 | 5/65/0 | 10.7 (+/−6.1) | 0.68 (+/−0.67) | R. obs 15 ctr | Nonsurgical—H1N1 pneumonia and other viral ARDS | |||
| Muller 2009 [54] | Germany | 2006–2008 | 60 | 0/60/0 | 9.0 (+/−6.1) | 8 g/dL | 1.00 (+/−1.06) | 45.0% | R. obs | Nonsurgical—mixed severe respiratory failure (pneumonia/trauma/aspiration/sepsis/other) | |
| Bakhtiary 2008 [55] | Germany | 2003–2006 | 45 | 45/0/0 | 6.4 (+/−4.5) | 2.55 (+/−2.03) | 28.9% | R. obs | Surgical—postcardiotomy cardiogenic shock—mixed indications (CABG/valves/LVAD, 2/45 post heart transplant) | ||
| Dietl 2008 [56] | USA | 1994–2006 | 38 | 38/0/0 | 5.6 (+/−2.6) | 5.05 (+/−2.45) | 60.5% | R. obs | Nonsurgical—Hantavirus cardiopulmonary syndrome | ||
| Frenckner 2002 [57] | Sweden | 1995–2002 | 38 | 0/0/38 | 17.0 (+/−12.9) | 2.53 (+/−1.70) | R. obs | Nonsurgical—mixed severe respiratory failure (pneumonia/trauma/PE/aspiration/other) | |||
| Smith 2001 [58] | Australia | 1995–1998 | 17 | 17/0/0 | 4.1 (+/−2.1) | 10 g/dL | 7.21 (+/−3.13) | 41.2% | R. obs | Surgical—postcardiotomy cardiogenic shock | |
| Lewandowski 1997 [59] | Germany | 1989–1995 | 49 | 0/49/0 | 23.1 (+/−19.7) | 15 g/dL | 2.10 (+/−1.90) | 55.1% | R. obs | Nonsurgical—respiratory failure (ARDS) | |
| Peek 1997 [60] | UK | 1989–1995 | 50 | 2/48/0 | 8.6 (+/−7.4) | 14 g/dL | 4.0% | 2.20 (+/−2.00) | 66.0% | R. obs | Nonsurgical—respiratory failure (ARDS/pneumonia/asthma)—mixed cohort |
| Author/year (reference) | Location | Study period start and end year | N | ECMO type (VA/VV/not spec) | ECMO days (mean +/−SD) | Transfusion trigger (g/dL or HCt %) | % not transfused PRBC on ECMO | PRBC/day (mean +/−SD) | Survival to discharge (%) | Study type | Brief description |
| Butch 1996 [61] | USA | 1988–1994 | 74 | 0/0/74 | 10.9 (+/−10.9) | 14 g/dL | 1.4% | 4.60 (+/−3.77) | 45.9% | R. obs | Nonsurgical—respiratory failure (ARDS/pneumonia/asthma)—mixed cohort (infection, trauma, post-solid organ transplant) |
| Muehrcke 1996 [62] | USA | 1992–1994 | 23 | 23/0/0 | 2.4 (+/−1.5) | 17.84 (+/−8.88) | 31.8% | R. obs | Surgical—postcardiotomy cardiogenic shock |
| Variable | Finding (95% Confidence Range) | Number of Papers (Patients) Included | Cochrane’s Q Test | I2 Test of Heterogeneity | p-Value for Comparison | |
|---|---|---|---|---|---|---|
| Baseline Characteristics | ||||||
| Age (years) | 48.9 (46.3–51.5) | 53 (3786) | 2128 | 98% | n/a | |
| Gender (% male) | 68.4% (IQR 61.1–75.2) | 50 (3624) | n/a | n/a | n/a | |
| Modality (patients) | Venovenous | 1177 | 54 (3808) | n/a | ||
| Venoarterial and combined | 2508 | |||||
| Not specified | 123 | |||||
| ECMO duration (days) | All patients | 8.2 (7.0–9.4) | 49 (3328) | 1781 | 97% | n/a |
| Venoarterial patients only | 5.6 (4.4–6.8) | 20 (1895) | 557 | 97% | <0.001 | |
| Venovenous patients only | 14.6 (10.6–18.6) | 9 (309) | 63 | 87% | ||
| Variable | Finding (95% Confidence Range) | Number of Papers (Patients) Included | Cochrane’s Q Test | I2 Test of Heterogeneity | p-Value for Comparison | |
|---|---|---|---|---|---|---|
| ECMO Modality | PRBC Units/Run or PRBC Units/Day | |||||
| Whole ECMO run | All patients | 17.7 (14.2–21.2) | 52 (3452) | 2816 | 98% | |
| VA patients only | 18.3 (14.2–22.4) | 24 (2043) | 1207 | 98% | 0.85 | |
| VV patients only | 19.3 (10.4–28.1) | 9 (309) | 95 | 90% | ||
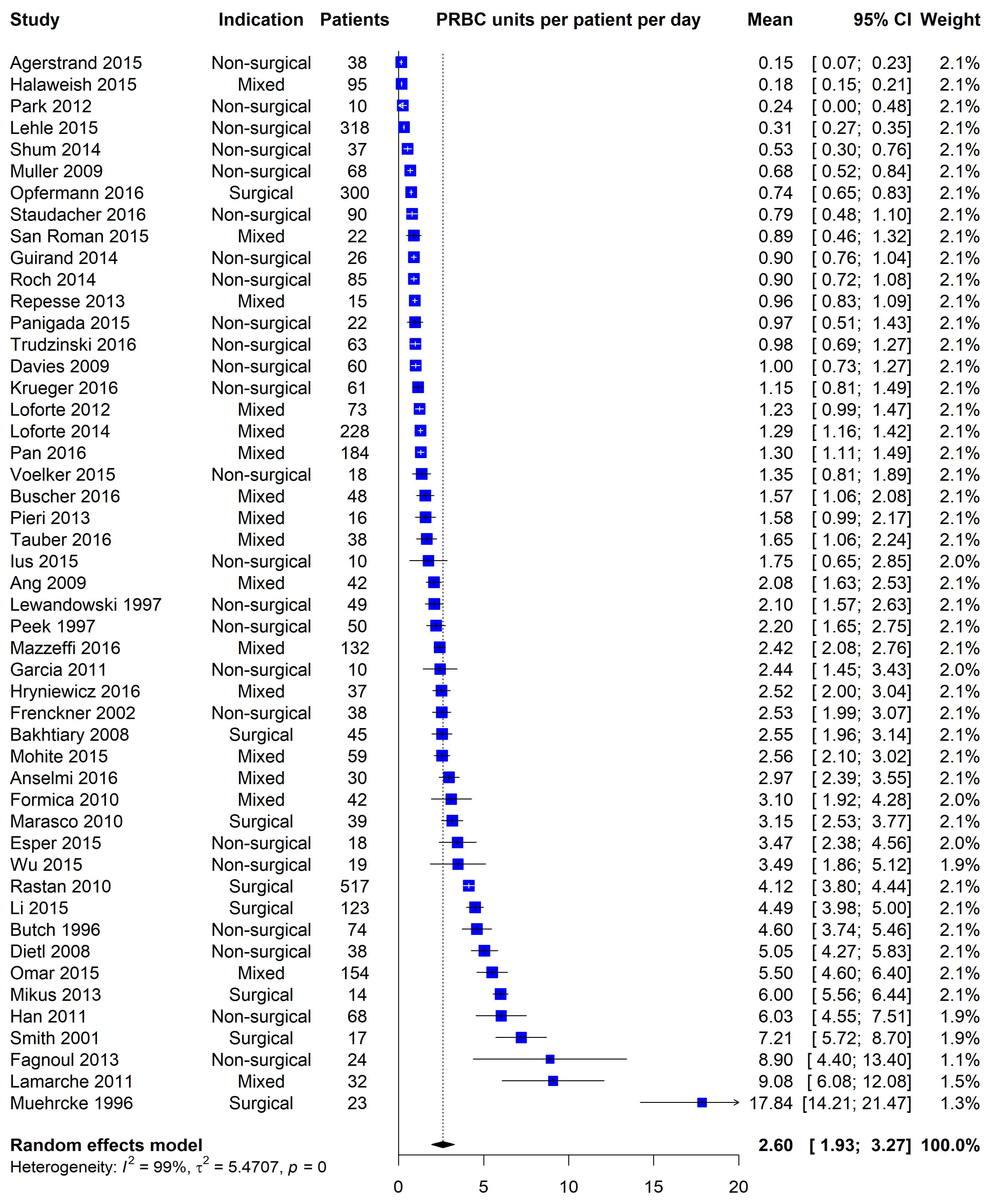
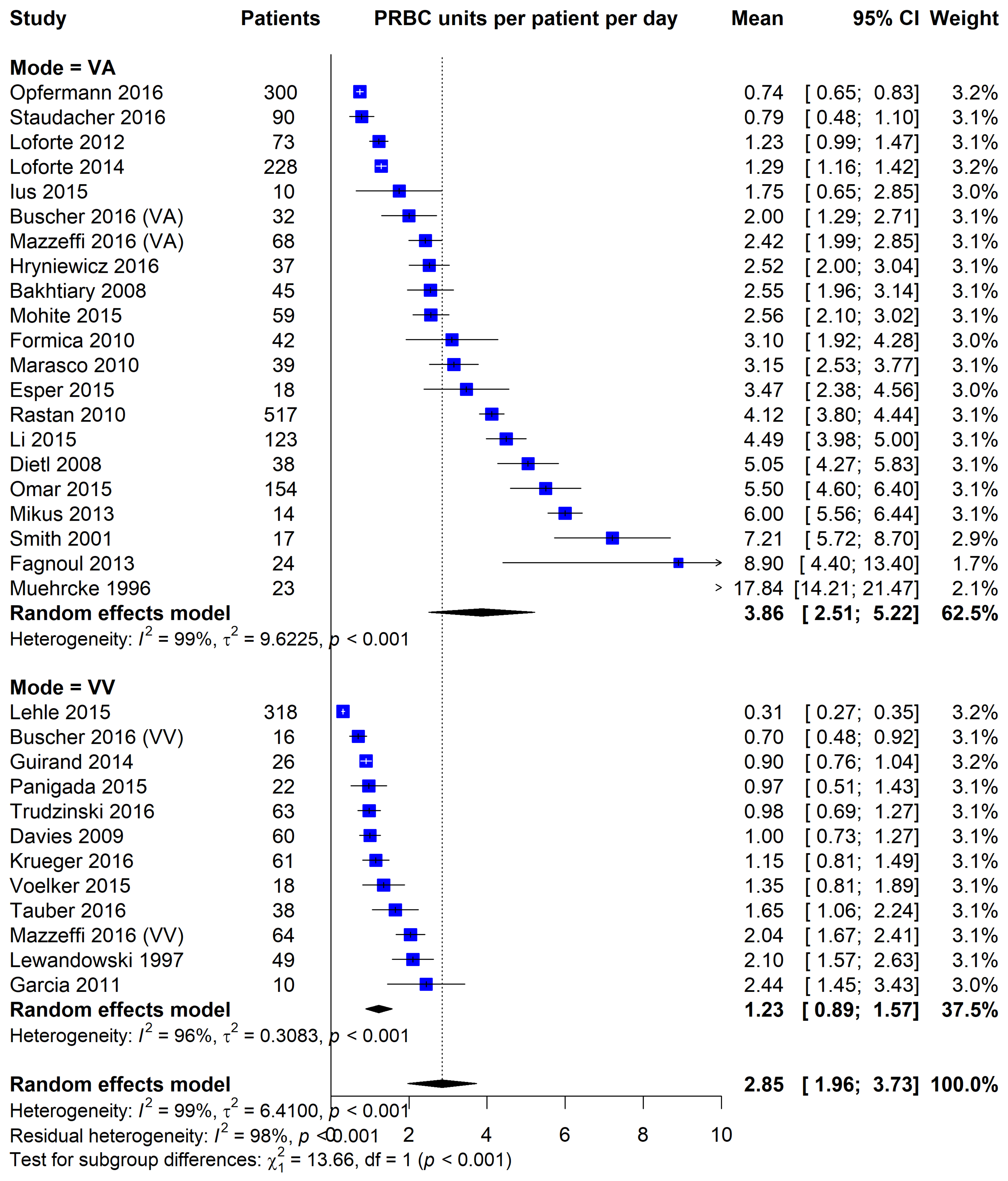
| Per ECMO day | All patients | 2.60 (1.93–3.27) | 49 (3619) | 3643 | 99% | |
| VA patients only | 3.86 (2.51–5.22) | 23 (1933) | 1519 | 99% | <0.001 | |
| VV patients only | 1.23 (0.89–1.57) | 12 (665) | 292 | 96% | ||
| ECMO indication | PRBC units/day | |||||
| Postcardiotomy | 5.56 (2.20–8.93) | 8 (1078) | 1235 | 99% | 0.04 | |
| Nonsurgical | 1.93 (1.26–2.59) | 25 (1309) | 730 | 97% | ||
| Peripheral cannulation rate | PRBC units/day | |||||
| Greater than 90% | 1.74 (1.24–2.25) | 29 (2031) | 1223 | 98% | 0.02 | |
| Less than 90% | 4.53 (2.31–6.76) | 13 (1220) | 793 | 99% | ||
| Membrane type | PRBC units/day | |||||
| Polymethylpentene only | 2.11 (1.49–2.73) | 32 (2113) | 1643 | 98% | 0.11 | |
| Silicon, polypropylene or mixed | 4.46 (1.68–7.24) | 11 (895) | 578 | 98% | ||
| Survival status (median 51.2%) | PRBC units/day | |||||
| Above median | 1.65 (1.08–2.23) | 19 (1295) | 965 | 98% | 0.001 | |
| Below median | 3.82 (2.23–5.42) | 19 (1565) | 1417 | 99% | ||
| Major bleeding (median 30%) | PRBC units/day | |||||
| Above median | 1.83 (1.14–2.52) | 7 (336) | 137 | 96% | 0.99 | |
| Below median | 1.84 (0.90–2.78) | 8 (290) | 210 | 97% | ||
| Upper aPTT target (median 60s) | PRBC units/day | |||||
| Above median | 2.76 (1.87–3.65) | 8 (585) | 115 | 94% | 0.34 | |
| Below median | 1.98 (0.64–3.32) | 11 (1164) | 409 | 98% | ||
| Upper ACT target (median 180s) | PRBC units/day | |||||
| Above median | 2.87 (1.57–4.16) | 8 (343) | 602 | 99% | 0.92 | |
| Below and including median | 2.95 (2.02–3.88) | 14 (842) | 301 | 96% | ||
| Transfusion trigger (median 9.3 g/dL) | PRBC units/day | |||||
| Above and including median | 2.39 (1.67–3.10) | 15 (986) | 758 | 98% | 0.005 | |
| Below median | 1.41 (0.86–1.97) | 13 (797) | 388 | 97% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hughes, T.; Zhang, D.; Nair, P.; Buscher, H. A Systematic Literature Review of Packed Red Cell Transfusion Usage in Adult Extracorporeal Membrane Oxygenation. Membranes 2021, 11, 251. https://doi.org/10.3390/membranes11040251
Hughes T, Zhang D, Nair P, Buscher H. A Systematic Literature Review of Packed Red Cell Transfusion Usage in Adult Extracorporeal Membrane Oxygenation. Membranes. 2021; 11(4):251. https://doi.org/10.3390/membranes11040251
Chicago/Turabian StyleHughes, Thomas, David Zhang, Priya Nair, and Hergen Buscher. 2021. "A Systematic Literature Review of Packed Red Cell Transfusion Usage in Adult Extracorporeal Membrane Oxygenation" Membranes 11, no. 4: 251. https://doi.org/10.3390/membranes11040251
APA StyleHughes, T., Zhang, D., Nair, P., & Buscher, H. (2021). A Systematic Literature Review of Packed Red Cell Transfusion Usage in Adult Extracorporeal Membrane Oxygenation. Membranes, 11(4), 251. https://doi.org/10.3390/membranes11040251