In Vitro Evaluation of Polihexanide, Octenidine and NaClO/HClO-Based Antiseptics against Biofilm Formed by Wound Pathogens


 , , ,
, , ,  ,
,
Abstract

1. Introduction
2. Materials and Methods
2.1. Antiseptics and Strains Analyzed
- (a)
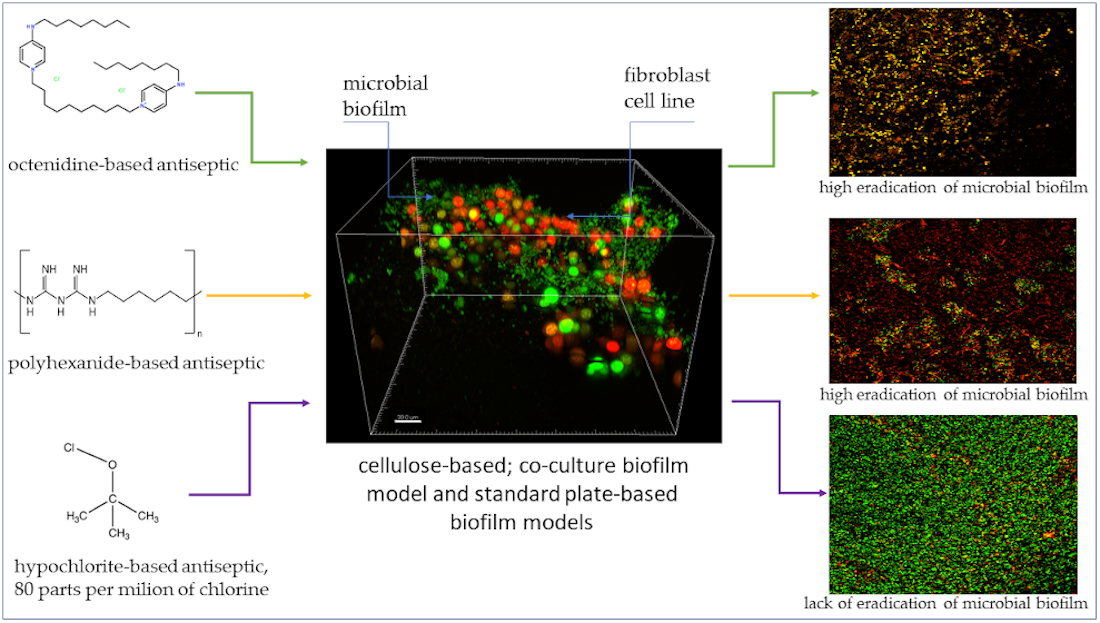
- Prontosan Wound Irrigation Solution (B. Braun Medical AG), later referred to as “P”, which contained 0.1% undecylenamidopropyl betaine, 0.1% polyhexamethylene biguanide (polihexanide), and purified water.
- (b)
- Octenilin Wound Irrigation Solution, (Schülke Mayr GmbH, Vienna, Austria), later referred to as “O”, which contained Aqua valde purificata, Glycerol, Ethylhexylglycerin and Octenidine HCl.
- (c)
- Microdacyn 60 Wound Care Solution (Sonoma Pharmaceuticals, Inc, Petaluma, CA, USA), later referred to as “M” which contained super-oxidized water, sodium chloride (0.022%), hypochlorous acid (0.004%), sodium hypochlorite (0.004%).
2.2. The Following Microbial Strains of PORT [PORT Polish Center for Technology Development/Polski Ośrodek Rozwoju Technologii] Microbiology Laboratory Strain Collection Were Used:
- (A)
- Candida albicans PRT1-9 [n = 9]
- (B)
- Pseudomonas aeruginosa PRT1-9 [n = 9]
- (C)
- Methicillin-Resistant Staphylococcus aureus (MRSA) PRT1-9 [n = 9]
2.3. Evaluation of Minimal Biocidal Concentrations of Tested Antiseptics Using Microtiter Plate Assay
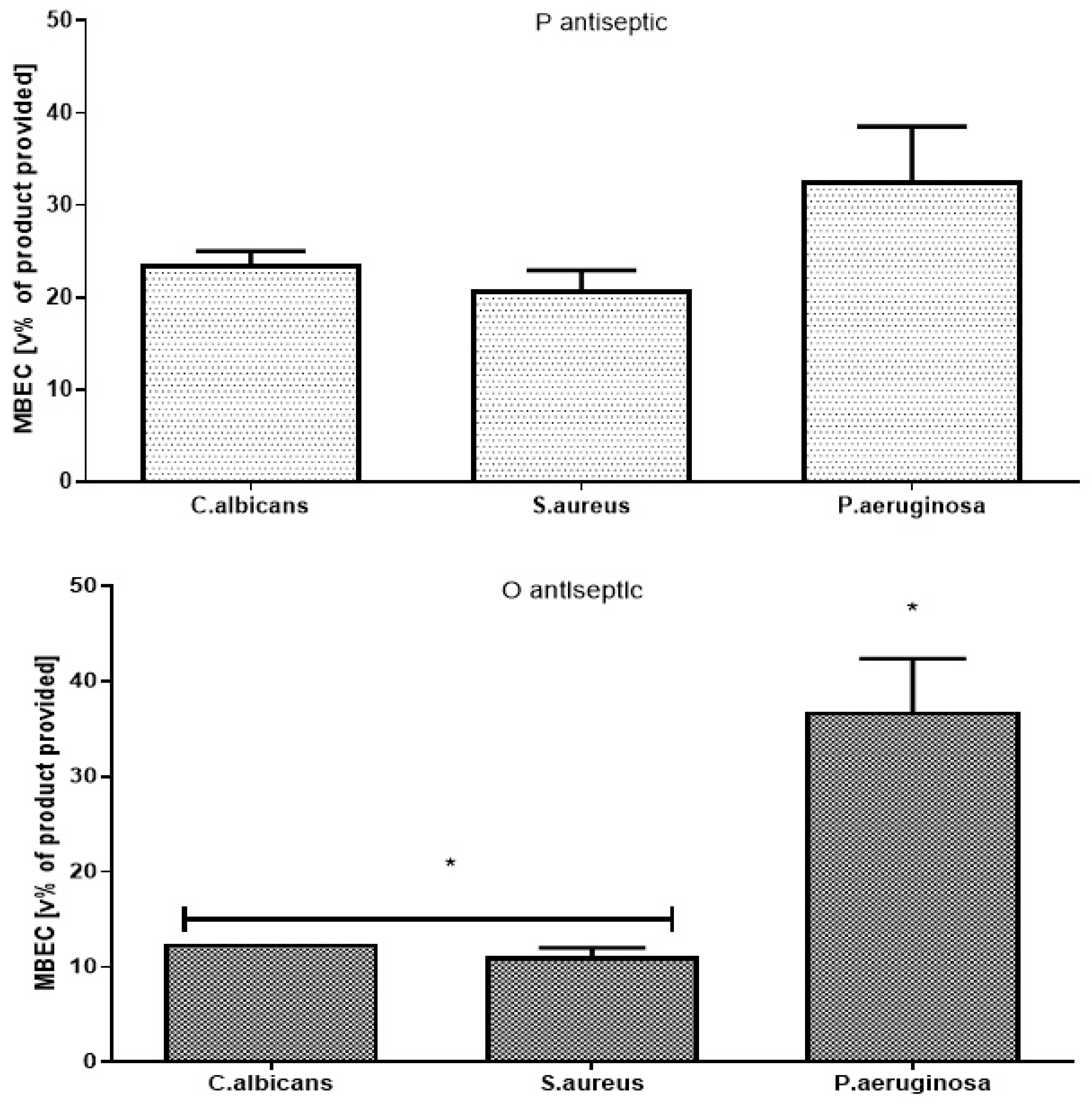
2.4. Evaluation of Minimal Biofilm Eradication Concentration [MBEC] of Antiseptics Using Microtiter Plate Assay
2.5. Biofilm-Oriented Antiseptic Test
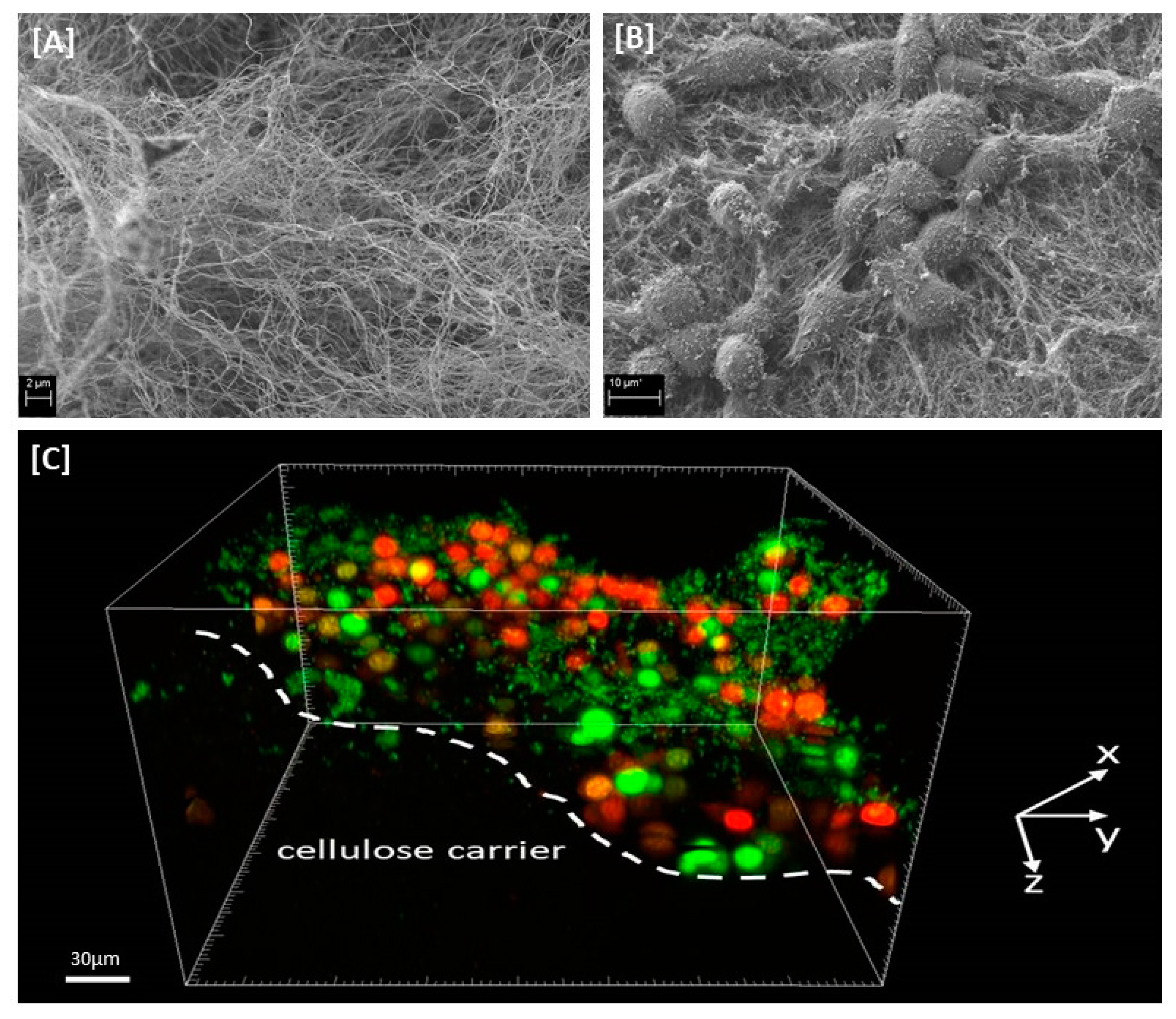
2.6. Cellulose-Based Biofilm Model
2.7. Confocal Microscopy Examination of Chosen Biofilms Formed on CC
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- In vitro analysis of biofilm requires the application of diversified analytical techniques to provide cohesive results
- PHMB and octenidine-based antiseptics displayed similar and high antimicrobial activity against biofilms formed by C. albicans, S. aureus and P. aeruginosa strains
- M antiseptic, of chlorine content equals 80ppm displayed no antibiofilm activity in 2 out of 3 performed analyses and weak antibiofilm activity in cellulose-based biofilm model
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kadam, S.; Shai, S.; Shahane, A.; Kaushik, K.S. Recent Advances in Non-Conventional Antimicrobial Approaches for Chronic Wound Biofilms: Have We Found the ‘Chink in the Armor’? Biomedicines 2019, 7, 35. Available online: https://www.mdpi.com/2227-9059/7/2/35#cite (accessed on 2 December 2020). [CrossRef] [PubMed]
- Lappin-Scott, H.; Burton, S.; Stoodley, P. Revealing a world of biofilms—The pioneering research of Bill Costerton. Nat. Rev. Genet. 2014, 12, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Dongari-Bagtzoglou, A. Pathogenesis of mucosal biofilm infections: Challenges and progress. Expert Rev. Anti-infect. Ther. 2008, 6, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, M.H.; Idris, A.L.; Fan, X.; Guo, Y.; Yu, Y.; Jin, X.; Qiu, J.; Guan, X.; Huang, T. Beyond Risk: Bacterial Biofilms and Their Regulating Approaches. Front. Microbiol. 2020, 11, 928. [Google Scholar] [CrossRef]
- Mikulskis, P.; Hook, A.L.; Dundas, A.A.; Irvine, D.J.; Sanni, O.; Anderson, D.G.; Langer, R.; Alexander, M.R.; Williams, P.; Winkler, D.A. Prediction of Broad-Spectrum Pathogen Attachment to Coating Materials for Biomedical Devices. ACS Appl. Mater. Interfaces 2018, 10, 139–149. [Google Scholar] [CrossRef]
- Gbejuade, H.; Lovering, A.M.; Webb, J.C. The role of microbial biofilms in prosthetic joint infections. Acta Orthop. 2014, 86, 147–158. [Google Scholar] [CrossRef]
- Welch, K.; Cai, Y.; Strømme, M. A Method for Quantitative Determination of Biofilm Viability. J. Funct. Biomater. 2012, 3, 418–431. [Google Scholar] [CrossRef]
- Crabbé, A.; Jensen, P.Ø.; Bjarnsholt, T.; Coenye, T. Antimicrobial Tolerance and Metabolic Adaptations in Microbial Biofilms. Trends Microbiol. 2019, 27, 850–863. [Google Scholar] [CrossRef]
- Mah, T.-F.C.; O’Toole, G.A. Mechanisms of biofilm resistance to antimicrobial agents. Trends Microbiol. 2001, 9, 34–39. [Google Scholar] [CrossRef]
- Malone, M.; Bjarnsholt, T.; McBain, A.; James, G.; Stoodley, P.; Leaper, D.; Tachi, M.; Schultz, G.; Swanson, T.; Wolcott, R. The prevalence of biofilms in chronic wounds: A systematic review and meta-analysis of published data. J. Wound Care 2017, 26, 20–25. [Google Scholar] [CrossRef]
- Kramer, A.; Dissemond, J.; Kim, S.; Willy, C.; Mayer, D.; Papke, R.; Tuchmann, F.; Assadian, U.-P.D.O. Consensus on Wound Antisepsis: Update 2018. Ski. Pharmacol. Physiol. 2017, 31, 28–58. [Google Scholar] [CrossRef] [PubMed]
- Hübner, N.-O.; Kramer, A. Review on the Efficacy, Safety and Clinical Applications of Polihexanide, a Modern Wound Antiseptic. Ski. Pharmacol. Physiol. 2010, 23, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Mashat, B.H. Polyhexamethylene biguanide hydrochloride: Features and applications. Br. J. Environ. Sci. 2016, 4, 49–55. [Google Scholar]
- Hübner, N.-O.; Siebert, J.; Kramer, A. Octenidine Dihydrochloride, a Modern Antiseptic for Skin, Mucous Membranes and Wounds. Ski. Pharmacol. Physiol. 2010, 23, 244–258. [Google Scholar] [CrossRef]
- Müller, G.; Kramer, A. Biocompatibility index of antiseptic agents by parallel assessment of antimicrobial activity and cellular cytotoxicity. J. Antimicrob. Chemother. 2008, 61, 1281–1287. [Google Scholar] [CrossRef]
- D’Atanasio, N.; de Joannon, C.A.; Mangano, G.; Meloni, M.; Giarratana, N.; Milanese, C.; Tongiani, S. A new acid-oxidizing solution: Assessment of its role on methicillin-resistant Staphylococcus aureus (MRSA) biofilm morphological changes. Wounds 2015, 27, 265–273. [Google Scholar]
- Gray, M.J.; Wholey, W.-Y.; Jakob, U. Bacterial Responses to Reactive Chlorine Species. Annu. Rev. Microbiol. 2013, 67, 141–160. [Google Scholar] [CrossRef]
- Kammerlander, G.; Assadian, O.; Eberlein, T.; Zweitmuller, P.; Luchsinger, S.; Andriessen, A. A clinical evaluation of the efficacy and safety of singlet oxygen in cleansing and disinfecting stagnating wounds. J. Wound Care 2011, 20, 149–158. [Google Scholar] [CrossRef]
- Kamaruzzaman, N.F.; Chong, S.Q.Y.; Edmondson-Brown, K.M.; Ntow-Boahene, W.; Bardiau, M.; Good, L. Bactericidal and Anti-biofilm Effects of Polyhexamethylene Biguanide in Models of Intracellular and Biofilm of Staphylococcus aureus Isolated from Bovine Mastitis. Front. Microbiol. 2017, 8, 1518. [Google Scholar] [CrossRef]
- Kramer, A.; Roth, B.; Muller, G.; Rudolph, P.; Klocker, N. Influence of the antiseptic agents polihexanide and octenidine on FL-cells and on healing of experimental superficial aseptic wounds in piglets. A double-blind, randomised, stratified controlled, parallel-group study. Skin Pharmacol. Physiol. 2004, 17, 141–146. [Google Scholar] [CrossRef]
- Assadian, U.-P.D.O.; Kammerlander, G.; Geyrhofer, C.; Luch, G.; Doppler, S.; Tuchmann, F.; Eberlein, M.T.; Leaper, D. Use of wet-to-moist cleansing with different irrigation solutions to reduce bacterial bioburden in chronic wounds. J. Wound Care 2018, 27, S10–S16. [Google Scholar] [CrossRef] [PubMed]
- Serra, R.; Grande, R.; Butrico, L.; Rossi, A.; Settimio, U.F.; Caroleo, B.; Amato, B.; Gallelli, L.; De Franciscis, S. Chronic wound infections: The role ofPseudomonas aeruginosaandStaphylococcus aureus. Expert Rev. Anti-infect. Ther. 2015, 13, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Kalan, L.; Loesche, M.; Hodkinson, B.P.; Heilmann, K.; Ruthel, G.; Gardner, S.E.; Grice, E.A. Redefining the Chronic-Wound Microbiome: Fungal Communities Are Prevalent, Dynamic, and Associated with Delayed Healing. mBio 2016, 7, e01058-16. [Google Scholar] [CrossRef] [PubMed]
- Junka, A.; Bartoszewicz, M.; Dziadas, M.; Szymczyk, P.; Dydak, K.; Żywicka, A.; Owczarek, A.; Bil-Lula, I.; Czajkowska, J.; Fijałkowski, K. Application of bacterial cellulose experimental dressings saturated with gentamycin for management of bone biofilm in vitro and ex vivo. J. Biomed. Mater. Res. Part B Appl. Biomater. 2020, 108, 30–37. [Google Scholar] [CrossRef]
- Junka, A.; Bartoszewicz, M.; Smutnicka, D.; Secewicz, A.; Szymczyk, P. Efficacy of Antiseptics Containing Povidone-Iodine, Octenidine Dihydrochloride and Ethacridine Lactate against Biofilm Formed by Pseudomonas Aeruginosa and Staphylococcus Aureus Measured with the Novel Biofilm-Oriented Antiseptics Test. Int. Wound J. 2014, 11, 730–734. [Google Scholar] [CrossRef]
- Sheraba, N.; Yassin, A.; Fahmy, A.; Amin, M. Efficacy and toxicity of neutralizers against disinfectants and antiseptics used in vaccine production facility. Afr. J. Microbiol. Res. 2012, 6, 6565–6571. [Google Scholar] [CrossRef][Green Version]
- Baiga, U.; Ansari, M.A.; Gondal, M.; Akhtard, S.; Alam Khan, F.; Falathaf, W.S. Single step production of high-purity copper oxide-titanium dioxide nanocomposites and their effective antibacterial and anti-biofilm activity against drug-resistant bacteria. Mater. Sci. Eng. C 2020, 113, 110992. [Google Scholar] [CrossRef]
- Ansari, M.A.; Albetran, H.M.; Alheshibri, M.H.; Timoumi, A.; Algarou, N.A.; Akhtar, S.; Slimani, Y.; Almessiere, M.; AlAhmari, F.; Baykal, A.; et al. Synthesis of Electrospun TiO2 Nanofibers and Characterization of Their Antibacterial and Antibiofilm Potential against Gram-Positive and Gram-Negative Bacteria. Antibiotics 2020, 9, 572. [Google Scholar] [CrossRef]
- Ansari, M.A.; Khan, H.M.; Khan, A.A.; Ahmad, M.K.; Mahdi, A.A.; Pal, R.; Cameotra, S.S. Interaction of silver nanoparticles withEscherichia coliand their cell envelope biomolecules. J. Basic Microbiol. 2013, 54, 905–915. [Google Scholar] [CrossRef]
- Kramer, A.; Assadian, O.; Muller, S.; Widulle, H.; Nurnberg, P. Octenidine, Chlorhexidine, Iodine and Iodophores; Georg Thieme: Stuttgart, Germany; New York, NY, USA, 2008. [Google Scholar]
- Tasse, J.; Cara, A.; Saglio, M.; Villet, R.; Laurent, F. A steam-based method to investigate biofilm. Sci. Rep. 2018, 8, 13040. [Google Scholar] [CrossRef]
- Severing, A.-L.; Rembe, J.-D.; Koester, V.; Stuermer, E.K. Safety and efficacy profiles of different commercial sodium hypochlorite/hypochlorous acid solutions (NaClO/HClO): Antimicrobial efficacy, cytotoxic impact and physicochemical parametersin vitro. J. Antimicrob. Chemother. 2019, 74, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Bueno, J. Anti-Biofilm Drug Susceptibility Testing Methods: Looking for New Strategies against Resistance Mechanism. J. Microb. Biochem. Technol. 2011, 2014. [Google Scholar] [CrossRef]
- Flemming, H.-C.; Wingender, J.; Szewzyk, U. Biofilm Highlights; Springer: Berlin/Heidelberg, Germany, 2011; ISBN 978-3-642-19939-4. [Google Scholar]
- Maczynska, B.; Secewicz, A.; Smutnicka, D.; Szymczyk, P.; Dudek-Wicher, R.; Junka, A.; Bartoszewicz, M. In vitro efficacy of gentamicin released from collagen sponge in eradication of bacterial biofilm preformed on hydroxyapatite surface. PLoS ONE 2019, 14, e0217769. [Google Scholar] [CrossRef] [PubMed]
- Virto, R.; Manas, P.; Alvarez, I.; Condon, S.; Raso, J. Membrane Damage and Microbial Inactivation by Chlorine in the Absence and Presence of a Chlorine-Demanding Substrate. Appl. Environ. Microbiol. 2005, 71, 5022–5028. [Google Scholar] [CrossRef]
- Kragh, K.N.; Alhede, M.; Kvich, L.; Bjarnsholt, T. Into the well—A close look at the complex structures of a microtiter biofilm and the crystal violet assay. Biofilm 2019, 1, 100006. [Google Scholar] [CrossRef]
- Żywicka, A.; Wenelska, K.; Junka, A.; Chodaczek, G.; Szymczyk, P.; Fijałkowski, K. Immobilization pattern of morphologically different microorganisms on bacterial cellulose membranes. World J. Microbiol. Biotechnol. 2019, 35, 11. [Google Scholar] [CrossRef]
- Loh, E.Y.X.; Mohamad, N.; Busra, M.F.M.; Ng, M.H.; Ng, S.F.; Amin, M.C.I.M. Development of a bacterial cellulose-based hydrogel cell carrier containing keratinocytes and fibroblasts for full-thickness wound healing. Sci. Rep. 2018, 8, 1–12. [Google Scholar] [CrossRef]
- Elkins, M.R.; Bye, P.T.P. Mechanisms and applications of hypertonic saline. J. R. Soc. Med. 2011, 104, 2–5. [Google Scholar] [CrossRef]
- Winter, G.D. Formation of the scab and rate of epithelialization of superficial wounds in the skin of the young domestic pig. Nature 1962, 193, 293–294. [Google Scholar] [CrossRef]
- ESPAUR. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR)—Report 2017. 2017. Available online: Gov.uk/government/uploads/system/uploads/attachment_data/file/656611/ESPAUR_report_2017.pdf (accessed on 4 December 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MBC (v/v%) of Antiseptic Working Solution | |||
|---|---|---|---|
| (n = 9) | C. albicans | S. aureus | P. aeruginosa |
| P | 0.36 (±0.18) | 0.17 (±0.03) | 1.56 (±0.95) |
| O | 0.09 | 0.18 | 0.45 (±0.19) |
| M | >25% * | >25% * | >25% * |
| (A) Candida albicans (n = 9). | Contact Time | ||||
| 1 min | 15 min | 30 min | 1 h | 24 h | |
| (%) of Biofilm-Forming Strains Survived Treatment | |||||
| P antiseptic | 100 | 100 | 100 | 66.6 | 0 |
| O antiseptic | 100 | 100 | 66.6 | 0 | 0 |
| M antiseptic | 100 | 100 | 100 | 100 | 100 |
| (B) S. aureus (n = 9). | Contact Time | ||||
| 1 min | 15 min | 30 min | 1 h | 24 h | |
| (%) of Biofilm-Forming Strains Survived Treatment | |||||
| P antiseptic | 100 | 77.7 | 77.7 | 66.6 | 0 |
| O antiseptic | 100 | 66.6 | 55.5 | 55.5 | 0 |
| M antiseptic | 100 | 100 | 100 | 100 | 100 |
| (C) P. aeruginosa (n = 9). | Contact Time | ||||
| 1 min | 15 min | 30 min | 1 h | 24 h | |
| (%) of Biofilm-Forming Strains Survived Treatment | |||||
| P antiseptic | 100 | 77.7 | 77.7 | 66.6 | 0 |
| O antiseptic | 100 | 66.6 | 55.5 | 55.5 | 0 |
| M antiseptic | 100 | 100 | 100 | 100 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krasowski, G.; Junka, A.; Paleczny, J.; Czajkowska, J.; Makomaska-Szaroszyk, E.; Chodaczek, G.; Majkowski, M.; Migdał, P.; Fijałkowski, K.; Kowalska-Krochmal, B.; et al. In Vitro Evaluation of Polihexanide, Octenidine and NaClO/HClO-Based Antiseptics against Biofilm Formed by Wound Pathogens. Membranes 2021, 11, 62. https://doi.org/10.3390/membranes11010062
Krasowski G, Junka A, Paleczny J, Czajkowska J, Makomaska-Szaroszyk E, Chodaczek G, Majkowski M, Migdał P, Fijałkowski K, Kowalska-Krochmal B, et al. In Vitro Evaluation of Polihexanide, Octenidine and NaClO/HClO-Based Antiseptics against Biofilm Formed by Wound Pathogens. Membranes. 2021; 11(1):62. https://doi.org/10.3390/membranes11010062
Chicago/Turabian StyleKrasowski, Grzegorz, Adam Junka, Justyna Paleczny, Joanna Czajkowska, Elżbieta Makomaska-Szaroszyk, Grzegorz Chodaczek, Michał Majkowski, Paweł Migdał, Karol Fijałkowski, Beata Kowalska-Krochmal, and et al. 2021. "In Vitro Evaluation of Polihexanide, Octenidine and NaClO/HClO-Based Antiseptics against Biofilm Formed by Wound Pathogens" Membranes 11, no. 1: 62. https://doi.org/10.3390/membranes11010062
APA StyleKrasowski, G., Junka, A., Paleczny, J., Czajkowska, J., Makomaska-Szaroszyk, E., Chodaczek, G., Majkowski, M., Migdał, P., Fijałkowski, K., Kowalska-Krochmal, B., & Bartoszewicz, M. (2021). In Vitro Evaluation of Polihexanide, Octenidine and NaClO/HClO-Based Antiseptics against Biofilm Formed by Wound Pathogens. Membranes, 11(1), 62. https://doi.org/10.3390/membranes11010062