1. Introduction
In recent decades, globalization has caused events, decisions, and activities happening in each place on the planet to have a significant and rapid impact elsewhere in the world. All this leads to a significant change in health problems and societal concerns. Reasonably, many difficulties have their origins in social factors that cause inequalities in health, but it should be noted that it is the growing socioeconomic inequalities that generate the greatest inequalities in health, so that poverty is the main socioeconomic factor that affects the state of health of people [
1]. Indeed, the world is immersed in various challenges, one of the most significant being the effects of the new technological revolution that is generating the transformation of humanity. Therefore, the concept of the “fourth industrial revolution” arises within the framework of the World Economic Forum to refer to changes in the global economy from the basis of technologies supported by physical systems, biological systems, digital systems, and their interactions, generating a fundamental change in the way we live, work, and relate [
2].
It should be recalled that, in 1789, Edward Jenner was the first to scientifically demonstrate that people could be protected against smallpox, if exposed to smallpox vaccine [
3,
4]. However, it should be noted that, a few years earlier, in 1774, there is a reference to the first person who performed a vaccination; in this case, he vaccinated his family with smallpox vaccine [
5]. Nowadays, vaccines can prevent and control communicable diseases and are considered essential to deal with emerging infectious diseases; they can immobilize or limit epidemic outbreaks of these, and combat the spread of antimicrobial resistance. For this reason, society is demanding that the industry and the scientific community respond with vaccines, as soon as possible, to the epidemics of H1N1 flu, Ebola, Zika, COVID-19, etc. [
6].
As it is known, vaccines are antigenic preparations made up by micro-organisms, or by part of these, which are modified to lose or attenuate their pathogenic capacity, and their purpose is to stimulate the individual’s defence mechanisms against infectious agents. Advances in molecular biology, specifically in the development of recombinant DNA technology and bioinformatics, have been essential for the evolution of vaccines [
7]. Consequently, diseases such as smallpox have been eradicated globally, and other diseases, such as polio and measles, have been significantly reduced, as have the disabilities and deaths these diseases can cause. Its effectiveness is evidenced by the fact that, when immunization coverage decreases, diseases that have not been completely eradicated rebound, such as measles in Europe in recent years [
8] or in the United States, which, in 2019, reported the highest number of cases since 1992 [
9]. Immunization also plays a key role in achieving UN Sustainable Development Goals (SDG), specifically SDG3, “Ensuring healthy living and promoting well-being for all at all ages”, and contributes to the achievement of the other 16 SDGs [
10].
It should be noted that there is no 100% effective vaccine, nor are they all equally effective; however, the benefits of vaccines focus on their proven effectiveness, which is revealed in their behavior in practice and depends, fundamentally, on the immune capacity of the recipient, the type of vaccine, established schedules, availability, tolerance, and stability.
Since the creation of the Expanded Immunization Program by the World Health Organization (WHO) in 1974, benefits have been expanded and there is explicit recognition of the importance of vaccination and its high impact on social welfare. Global Vaccine Action Plan 2011–2020 (GVAP) [
11] was approved by 194 countries in the World Health Assembly. Consequently, the evaluation of GVAP results in 2019 [
12] facilitated the development of new proposals until 2030. It should be noted that the GVAP increased the visibility of immunization and assisted in the creation of a high-level political will. Indeed, it created a common framework for prioritizing, agreeing on activities, and evaluating results. The Immunization Agenda (AI2030) [
12] has designed a comprehensive global vaccine and immunization strategy for the decade 2021–2030. Reasonably, AI2030 takes advantage of the lessons derived from GVAP and considers the new and persistent challenges posed by infectious diseases.
The European Union (EU) carries out public health policies, but there is no common prevention model. This situation creates inequality to access to immunization among entire communities of citizens, as evidenced by the COVID-19 pandemic. It should be noted that each State has specific legislation on vaccination. Although each country’s vaccination plans are similar, there are significant differences in the vaccines included in the publicly funded vaccination schedules. In addition, the same vaccines are not given and not all vaccines are mandatory, as in Spain, where, to date, they are all voluntary in nature. Each country designs its vaccination strategy with respect to its epidemiological situation; however, WHO, the EU, and United Nations International Children’s Emergency Fund (UNICEF) develop global and European prevention and immunization strategies and plans [
13].
Consequently, the AI2030 [
12] aims to strengthen existing partnerships, establish new relationships, and better clarify roles and responsibilities in order to improve the use of information to drive action and ensure relevant assessments.
Vaccines are an excellent investment generating an improvement in quality of life, as demonstrated by the Decade of Vaccine Economics project [
14], which has been most evident in the most disadvantaged countries. In addition, as González-García points out [
15], more investment would have to be made in research and development, which will enable humanity to face with hope and strength any biological threats and pandemics that are to come, which would mean an excellent investment in the future, thus improving the quality of life around the world.
WHO [
16] considers vaccination, along with “clean water”, as one of the biggest public health successes, and scientific evidence has shown that the benefits of vaccination outweigh the unusual adverse effects. However, since the onset of vaccines, out of fear or carelessness, there are detractors of these, but the fashion of not vaccinating and the anti-vaccine movement began to grow more and more from 1998 onwards, when a doctor, Andrew Wakefield, presented in the scientific journal
The Lancet a study linking autism with the triple viral vaccine (measles, rubella, and mumps). The study was based on a very small sample, biased, and without any scientific rigor. As a result of this article, other studies were conducted with different results, demonstrating that it had been a scientific fraud [
17].
Currently, rejection of vaccination is occupying large spaces for debate and discussion in the media and social media, in the various areas of society, and in all countries of the world. There are concerns about how the problem is being raised as, in most cases, it is reduced to the polarization between pro-vaccines and anti-vaccines without seriously addressing the issue of vaccination considering the importance of group immunity and collective health. Vaccination reluctance ranges from acceptance to total rejection, with different nuances called “vaccine reluctance” [
18]. For years, the consolidation of vaccine rejection has been rated as a growing threat to collective health [
19].
The recommendations proposed by WHO [
20] focus on the need for a better awareness of vaccination reluctance, its determinants, and the challenges it poses. It also stresses the need to improve society’s awareness of the importance of vaccination in order to improve vaccine acceptance, share effective practices, and develop new tools to assess and address reluctance. Reasonably, in order to improve society’s awareness, it is essential to analyze the benefits and effectiveness of vaccines, concerns about their safety, and how they are perceived in society. Indeed, as Matesanz points out [
21], having an effective vaccine is not an individual solution, but that it is received by the maximum number of people in the environment to achieve the long-awaited “herd immunity” and that the virus stops circulating.
It should be emphasized that the information on COVID-19 is overflowing us and relegating to the background the importance of other vaccines that are fundamental to children, especially for the most vulnerable countries. In addition, as García-Toledano [
22] points out, the problem with vaccination programs is that they are linked to constant variations linked to vaccine availability, distribution, and administration logistics. Therefore, incorrect communication and co-ordination can show society a negative image of improvisation and lack of co-ordination that do not benefit awareness of the importance of vaccination.
It should be noted that, possibly, in the absence of regulation by administrations over the past two decades, the number of parents who choose not to vaccinate their children has increased. This increase can also be affected because the propaganda that opposition groups broadcast today has much more advanced and powerful information transmission tools every day, through social networks that facilitate the distribution of their opinion to a large number of people in a short period of time. In addition, some public figures publicly support this non-vaccination movement, leading to greater confusion in the population. Fortunately, the Spanish population is generally highly aware of vaccination, reaching immunization rates of 96% in childhood. This figure has fallen slightly in recent years, but it may not be as a result of these opposition associations, but also for socioeconomic reasons in certain marginal groups, so it is important to carry out educational projects aimed at these sectors of the population [
22].
If we focus on the current situation caused by COVID-19, WHO [
20] has stated that, although coronavirus vaccination has intensified, the world will not achieve collective immunity in 2021. For this reason, internationally renowned organizations, such as the United Nations Educational, Scientific, and Cultural Organization (UNESCO), WHO, UNICEF, the Council of Europe, the Organization for Economic Co-operation and Development (OECD), and the European Commission, indicate that it is essential that schools incorporate health education into their curriculums as a basic tool for developing healthy lifestyle habits, increasing the quality of life of schoolchildren and, consequently, working on building a better world [
23].
In the context we find ourselves, our main purpose is to study the importance of education for health and vaccination, analyze its development, and assess its situation in the 21st century.
2. Materials and Methods
An observational research was performed using a cross-sectional design which focuses on the study of health education and vaccination for the construction of inclusive societies. The awareness and regulation of vaccines (Dimension 1) were, therefore, analyzed with the aim of responding to problems: P1, society awareness of the importance of vaccination; P2, regulation of administrations of actions for vaccine compliance.
2.1. Population and Sample
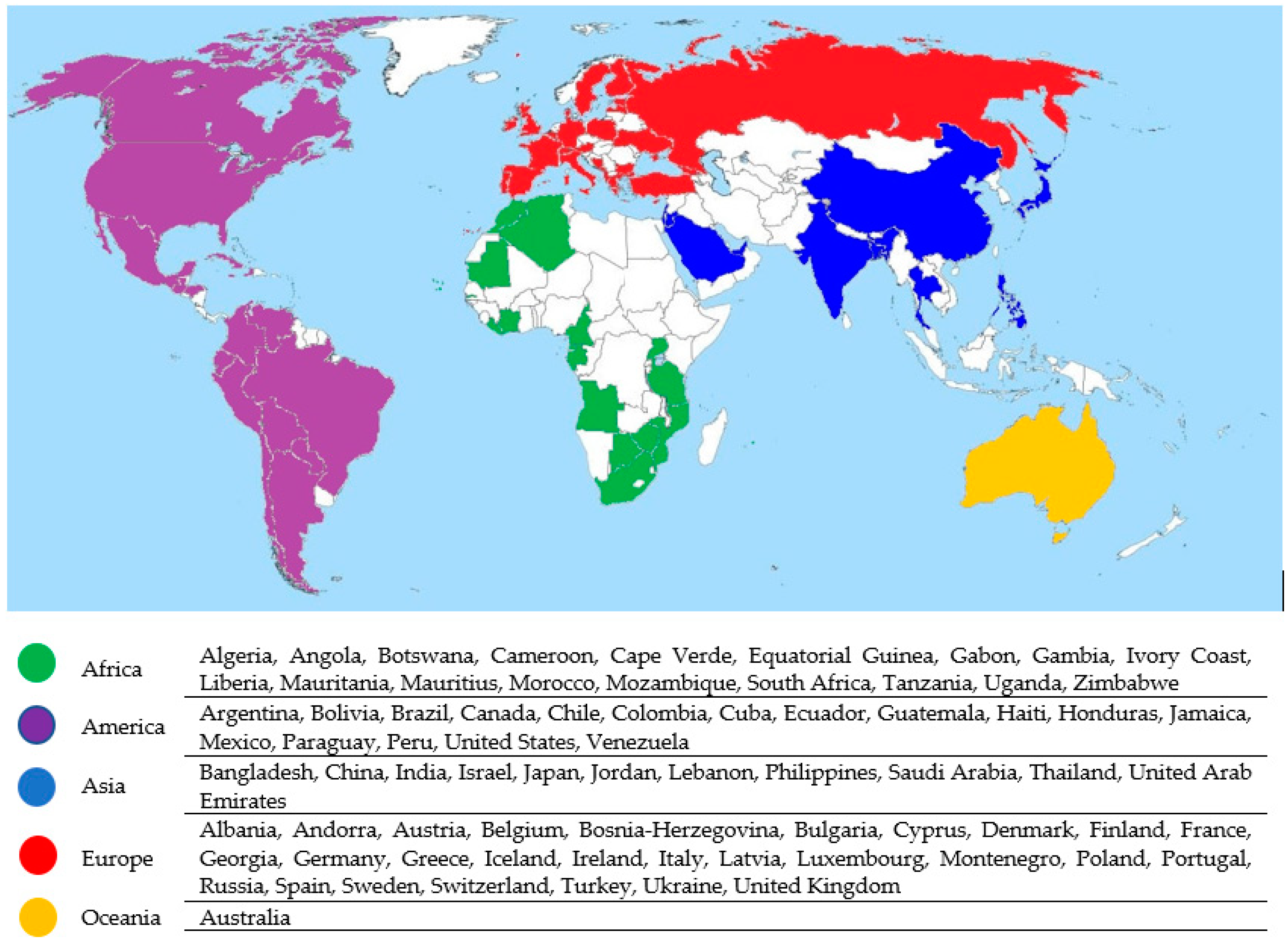
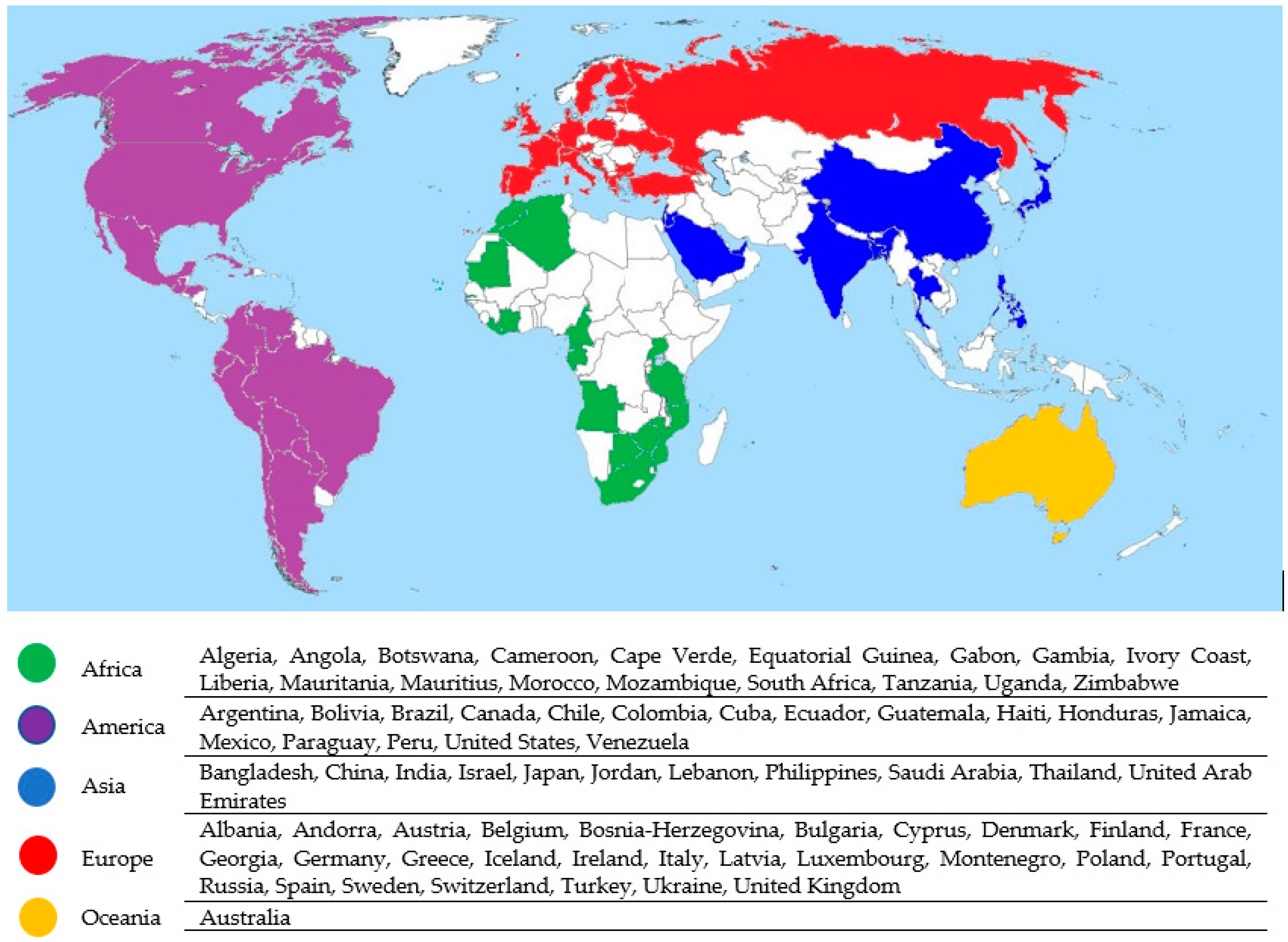
The sample consists of 1000 participants from 76 countries. The distribution of the participating sample is defined in the results section of the investigation.
The study population is delimited based on the selection criteria of developing their professional activity in one of the three sectors analyzed: health, education, and economics. All persons with a job performance not directly linked to these sectors were excluded. The sample selection followed a non-probabilistic sampling method of an accidental or consecutive type, consisting of 1000 participants from 76 countries (
Figure 1).
2.2. Variables
The questionnaire used VACUNASEDUCA [
24] consists of 12 items: 2 items corresponding to dimension
D1 = Awareness and regulation, 4 items corresponding to dimension
D2 = Education and teachers, 2 items corresponding to dimension
D3 = Regulation and obligation, and 4 items corresponding to dimension
D4 = Consequences and risks.
As an answer option for each item, a Likert scale of 1 to 3 was raised indicating the degree of agreement of the participant with the corresponding question; in this way, there were 12 ordinal variables for each of the items in the questionnaire.
The dependent variable S3t was built by adding the individual ordinal scores for each of the participants and dividing by 12 to typify it; in this way, we could have a quantitative dependent variable that came to represent the degree of agreement of each participant with the 12 items of the questionnaire that would allow us to perform the inferential analysis for each of the independent variables or factors of the research:
Gender: independent dichotomic variable with 2 options, G0 = Woman or G1 = Man.
Age: polyatomic independent variable with 4 options, E1 = Less than 30, E2 = Between 30 and 44, E3 = Between 45 and 59, or E4 = Greater than 60.
Sector: polyatomic independent variable with 3 options, S1 = Health, S2 = Education, or S3 = Economy.
Human Development Index (HDI): polyatomic independent variable with 4 options, I1 = very high, I2 = high, I3 = medium, or I4 = low.
Continent: polyatomic independent variable with 5 options, C1 = Europe, C2 = America, C3 = Asia, C4 = Africa, or C5 = Oceania.
2.3. Instrument
The technique used for data collection was the survey, the instrument chosen being a questionnaire consisting of 12 items with a Likert scale.
The questionnaire was developed for the purpose of this research, being submitted to a trial by 15 experts, which allowed Lawshe’s content validity index (CVI) [
25] to be calculated, which suggested a CVI 0.51 when using 14 experts, so there was no need to remove any items from the initial questionnaire.
Table 1 reflects the CVI for each of the dimensions of the questionnaire, the mean index being 0.96 [
26,
27,
28].
The questionnaire was also validated through exploratory factor analysis. The result of the Kaiser–Meyer–Olkin KMO test was 0.784, revealing the sample adequacy for performing factor analysis. The result of Bartlett’s sphericity test yielded a significance level of 0.000, which involved suitability for factor analysis. Although the matrix of factorial analysis components did not come out completely “clean”, with 2 items appearing correlated with 2 factors, the factorial structure obtained was very similar to that initially designed by García Perales et al. [
28] and Méndez & Rondón [
29].
The reliability of the questionnaire, in the sense of stability of the results, was calculated through the alpha coefficient of Cronbach (α).
Table 1 shows the indexes obtained for each of the dimensions. The mean value for the 4 dimensions was 0.64, being close to the 0.70 limit that Kerlinger et al. [
30] set for acceptable consistency.
2.4. Procedure
The questionnaire was prepared between June and July 2019 and was implemented from September 2019 to March 2020, specifically, of September to December at the headquarters of the WHO Geneva, and from January to March in Spain, in hospitals, universities, International Congresses of Education, and Congresses and meetings of Medicine.
The questionnaire was completed in a self-administered form, on paper and in person, in two languages, English and Spanish. There was no time limit, such as the respondents usually would take between 5 and 10 min, and the pollster was always the same person. The research was conducted at the beginning of the COVID-19 pandemic and was not affected by confinement. Anonymity and confidentiality of participants’ data was guaranteed at all times.
2.5. Data Analisys
In view of noncompliance with the premises of parametric methods, since the sample distribution did not conform to the normal distribution, it was chosen to use statistical techniques of null models using resampling techniques through the Monte Carlo simulation method using the bootstrap procedure [
31], which can be included within the approach of resampling data that perform computer simulation processes that are based on the extraction of a large number of repeated samples from the data themselves, and on which descriptive and inferential statistical analysis is performed using confidence intervals (ICs) extracted from the data themselves. This is what distinguishes such new procedures from classical statistical techniques that are based on theoretical models developed analytically. Consequently, some authors describe these techniques as intensive computation methods and are included within a modern statistical approach, competing with the classical mathematical approach [
32,
33]. This new approach is based on the enormous computing capacity of modern computers and the sufficiency of the sample to represent or reflect relevant aspects of the population from which it was extracted, since bootstrap’s method allows “the maximum from the little information available” to be extracted [
34] (p.149).
To analyze whether there were statistically significant differences, an ANOVA test was chosen for independent samples for each of the independent variables or factors in the research. The values of the F statistic, significance level p, and effect size measured by eta squared were obtained using the analysis of the multivariate general linear model of the SPSS statistical program in version 26. Post hoc tests were conducted assuming not equal variances using Tamhane’s T2, Dunnett’s T3, Dunnett’s Games–Howell, and Dunnett’s C statistics, all of which yielded similar results that served to determine the direction column in the ANOVA tables for each of the factors analyzed.
3. Results
First,
Table 2 shows the main characteristics of the sample in relation to gender, age, HDI, sector. and continent.
In order to contextualize Dimension 1 in the research on the importance of health education,
Table 3 shows the descriptive statistics obtained in the four dimensions of the questionnaire used.
In
Table 3, you can see high results for dimensions
D1 = Awareness and regulation and
D2 = Education and teachers,
highlighting item P06 that gets the upper mean score (M = 2.86, SD = 0.44), the highest mean value of the instrument set, and low results
for dimensions D3 = Regulation and obligation
and D4 = Consequences and risks by highlighting items P11 and P12 that get the lowest mean score (M = 1.18, SD = 0.42 and 0.43), the lowest mean value of the instrument assembly.
The mean scores for each dimension were as follows: D1 = Awareness and regulation (M = 2.81, SD = 0.36), D2 = Education and teachers (M = 2.81, SD = 0.31), D3 = Regulation and obligation (M = 1.47, SD = 0.59), and D4 = Consequences and risks (M = 1.20, SD = 0.41). The mean of the questionnaire as a whole was (M = 2.05, SD = 0.22).
As noted, in this work, we will focus on Dimension 1 (Awareness and regulation) with independent variables: gender, age, sector, HDI, and continent.
3.1. Gender Impact Analysis
In
Table 4, the distribution of the sample according to the gender can be observed:
G0 = Woman or G1 = Man for dimension D1.
As can be seen in
Table 4, the distribution of the sample according to gender is uneven; the percentage of women (69.4%) is much higher than that of men (30.6%).
To analyze whether gender differences exist in the questionnaire, an ANOVA was performed for independent samples. The results are listed in
Table 5.
Post-hoc tests suggest that the mean of women is above that of men in dimension D1 = Awareness and regulation, with higher means and propensity towards YES, so women could generally be inferred to have a higher awareness of vaccines than men.
Statistically significant differences appear in item P02 and dimension D1, although the size of the effect measured in the ANOVA test per eta squared being less than 0.06 has to be considered weak.
3.2. Age Incidence Analysis
In
Table 6, the distribution of the sample by age group can be observed: E1 = Under 30, E2 = Between 30 and 44, E3 = Between 45 and 59, E4 = Greater than 60.
As can be seen in
Table 6, the distribution of the sample by age group is uneven, the percentages of the age groups
E1 = Under 30 (36.3%),
E2 = Between 30 and 44 (34.8%), and
E3 = Between 45 and 59 (26.76%) are similar, while
the percentage of the group (E4) greater than 60 (2.2%) is of a lower order of magnitude.
To analyze whether there are differences according to the age group in the questionnaire, an ANOVA was performed for independent samples. The results are listed in
Table 7.
Post hoc tests suggest that the mean age group under 30 is above the other age groups in dimension D1 = Awareness and regulation, with higher means and, therefore, propensity for YES, so it could be inferred that the age group under the age of 30, in general, has a higher awareness of vaccines than the rest of the age groups.
Statistically significant differences appear in items P01, P02, and dimension D1, although, as the size of the effect measured in the ANOVA test per eta squared was less than 0.06, it has to be considered weak.
3.3. Analysis of the Impact of the Sector
In
Table 8, the distribution of the sample by sector can be observed:
S1 = Health, S2 = Education, S3 = Economy.
As can be seen in
Table 8, the distribution of the sample by sector is uneven; the percentage of the health sector (55.4%) is more than half of the sample, while the percentage of the education sector (32.9%) is one-third of the sample, and the share of the economy sector (11.7%) is a minority.
To analyze whether there are differences according to the sector in the questionnaire, an ANOVA was performed for independent samples. The results are listed in
Table 9.
Post hoc evidence suggests that the mean education sector is above the health sector in dimension D1 = Awareness and regulation, with higher means and, therefore, with propensity towards YES, so it could be inferred that the education sector generally has a higher awareness of vaccines than the health sector, which has a more negative view. The means of the economy sector are in an intermediate position, presenting significant differences with the health sector and not significant with the education sector.
Statistically significant differences appear in items P01, P02, and dimension D1, although the size of the effect measured in the ANOVA test per eta squared when less than 0.06 has to be considered weak.
3.4. Impact Analysis by Human Development Index (HDI)
In
Table 10, the distribution of the sample by Human Development Index (HDI) can be observed:
I1 = Very High, I2 = High, I3 = Medium, I4 = Low.
As can be seen in
Table 10, the sample distribution by Human Development Index (HDI) is uneven; the percentage of the group
I1 = Very high (87.3%) is of an order of magnitude greater than the percentage of groups
I2 = High (8.5%),
I3 = Medium (3.1%), and
I4 = Low (1.1%) that are of the same order of magnitude.
To analyze whether there are differences according to the Human Development Index (HDI) in the questionnaire, an ANOVA was conducted for independent samples. The results are listed in
Table 11.
The post hoc tests suggest that the mean of the HDI group: I1 = Very high is above the other groups in dimension D1 = Awareness and regulation, with higher means and, therefore, with propensity towards YES, so it could be inferred that the HDI group: I1 = Very high, in general, has a higher awareness of vaccines than the rest of the groups.
Statistically significant differences appear in items P01, P02, and dimension D1, although the size of the effect measured in the ANOVA test per eta squared being less than 0.06 has to be considered weak in item P02, while item P01 and dimension D1, being eta squared above 0.06, can be considered with a mean effect.
3.5. Analysis of Incidence by Continent
Table 12 shows the distribution of the sample by continent:
C1 = Europe, C2 = America, C3 = Asia, C4 = Africa, C5 = Oceania.
As can be seen in
Table 12, the distribution of the sample by continent is uneven; the percentage
C1 = Europe (83%) is of an order of magnitude greater than the percentage of the other
continents C2 = America (9.3%),
C3 = Asia (4%),
C4 = Africa (3.5%), and
C5 = Oceania (2%), which are of the same order of magnitude.
To analyze whether differences exist according to the continent in the questionnaire, an ANOVA was performed for independent samples, excluding Oceania analysis, as only two participants from that continent completed the questionnaire, which makes it unsuitable for statistical analysis using resampling techniques through the Monte Carlo simulation method using
the bootstrap algorithm. The results are listed in
Table 13.
In items P01, P02, and dimension D1, the mean of respondents from the continent C1 = Europe is above the rest of the continents in dimension D1 = Awareness and regulation, with higher means and, therefore, with propensity towards YES, so it could be inferred that respondents from the continent C1 = Europe generally have a higher awareness of vaccines than respondents from other continents.
Statistically significant differences appear in items P01, P02, and dimension D1, although the size of the effect measured in the ANOVA test per eta squared being less than 0.06 has to be considered weak in item P01, whereas, item P02, being eta squared above 0.06, can be considered with a mean effect.
4. Discussion and Conclusions
Research on the importance of vaccines in health is very broad, so the conclusions offered in this article are only a part of this. However, the results reflect a very interesting picture of the problem of vaccination from the world’s vaccine awareness and regulation dimension (D1) in a period closely linked to the start of the COVID-19 pandemic, since the completion of the work was in March 2020.
It is important to note that 100% of respondents of all ages, sex, profession, human development index, and continent positively value vaccines as basic tools to ensure the health of citizens and, above all, to prevent possible contagions, stressing that, since vaccines, infant mortality has fallen considerably, and only in cases where vaccines are not yet available is there significant mortality, especially in developing countries. In this regard, it should be recalled that Article 35 of the Charter of Fundamental Rights of the European Union [
35] provides that everyone has the right to health prevention and to benefit from the corresponding medical care in accordance with the conditions laid down in national provisions. Moreover, it is essential to protect the lives of infants, making it totally incomprehensible not to do so against diseases that can be avoided with vaccines.
Society’s awareness of the importance of vaccines and their relevant regulation by administrations has been an issue whose visibility in the media and social media has been increasing in the last decade, mainly due to their effectiveness and immersion of immunization around the world. However, they have also influenced vaccine movements with their constant public positioning against vaccination. Indeed, reluctance to vaccinate all countries is concerned not only with low-income countries, but has become a problem affecting everyone. That is why WHO [
20] has repeatedly expressed concern at the expansion of anti-vaccine speakers, covering not only certain rural minorities, but even expanding in urban areas with high purchasing power, and in all social classes [
36]. There is no doubt that raising awareness of the importance of vaccination is a key challenge that all international agencies must address in order to ensure human rights and peaceful coexistence in inclusive societies.
In the research carried out, it has been shown from a gender perspective that the mean of women makes a higher assessment than men in considering that society is aware of the importance of vaccines (D1, P1). However, there are no significant gender differences in whether administrations have regulated actions for vaccine compliance (D1, P2). This outcome could be affected by mothers who are mostly responsible for their sons’ and daughters’ vaccination schedule, so they could have a more up-to-date attitude, training, and information.
The group of people under the age of 30 is significantly different from the other age groups in their positive assessment of the awareness of society (D1, P1). In addition, higher scores are also evident in the group of people under 30 years of age, although of lower value, on whether administrations have regulated actions for the compliance of vaccination (D1, P2). There is no doubt that progress in vaccination over the past three decades has been very significant, not only because of technological advances, but also because of the increased incidence of vaccines, transparency, and safety.
Three main sectors have been considered: health, education, and economics, with the aim of studying whether there were differences on the subject of research. The mean of education sector has been shown to be significantly higher than that of the health sector, with the economy sector in an intermediate position. In this regard, other work shows that, in some areas, education contributes to greater acceptance and recognition of vaccination [
37]. However, it was shocking to researchers that the health sector was the least valued at raising society’s awareness of the importance of vaccination and regulating administrations’ actions for vaccine compliance, so research would need to be done on the reasons for this assessment and its possible impact to improve social awareness campaigns.
In relation to the Human Development Index (HDI), it has been shown that the mean HDI = very high group is higher than that of the HDI = medium and low groups, offering results that are totally consistent with studies done by WHO.
It is the continent C1 = Europe in which we find significantly higher means compared to other continents (C2 = America; C3 = Asia; C4 = Africa; and C5 = Oceania).
In conclusion, it can be indicated that the profiles of women, people under 30 years of age, the education sector, high human development index, and the European continent are those that most values society’s awareness of the importance of vaccination (D1, P1) and the regulation of actions for the implementation of vaccination (D1, P2). It is a very hopeful conclusion to advance the construction of inclusive societies, creating greater involvement of society as a whole through effective and evidence-based communication to allay fears, address concerns, and promote acceptance of vaccination around the world. It should, therefore, be remembered that people who delay or reject vaccination for themselves or their children pose a growing challenge for countries seeking to close immunization gaps. According to WHO [
12], one in five children worldwide do not yet receive regular vital immunizations, and around 1.5 million children die each year from diseases that could be prevented with vaccines that already exist.
The responsible awareness and active involvement of society worldwide about the importance of vaccination is critical to advancing the construction of a better world with safe planning and regulation that ensures compliance. Significantly, international agencies must be vigilant in order to deal with any incidents that may occur. Indeed, as has been shown in 2020, as a result of the COVID-19 pandemic, more than 14 million infants did not receive an initial dose of the DTP vaccine (diphtheria, tetanus and pertussis), demonstrating inadequate access to health and immunization services, and more than 5.7 million are only partially vaccinated. Similarly, more than 60% of these 19.7 million children live in 10 countries: Angola, Brazil, Ethiopia, the Philippines, India, Indonesia, Mexico, Nigeria, Pakistan, and the Democratic Republic of the Congo. In addition, non-vaccination is causing diseases that were considered eradicated, such as measles, to emerge, with new outbreaks active in the United States and in several countries in Europe (Portugal, Italy, Romania, etc.). It is clear that society’s awareness and proper regulation by administrations around the world will achieve collective immunity through safe and effective vaccines and make diseases rarer and, therefore, save lives.
In short, the research has highlighted the need for society to become aware of the importance of vaccination, so that clear, truthful, and relevant information that transcends safety in citizens about vaccination should be conveyed. In addition, they must report that infectious diseases are a major cause of morbidity and mortality across the globe, mainly in older people and those with chronic diseases. Consequently, effective and evidence-based communication is key to allaying fears, addressing concerns, and promoting acceptance of vaccination around the world. Reasonably, adequately raising awareness of the importance of vaccines will lead to the building of inclusive societies in which all citizens enjoy the health benefit, ensuring compliance with SDG3, “Ensuring healthy living and promoting well-being for all at all ages”, without discrimination of any kind.


 ,
, 



{kind=link}