
COVID-19 and the Gaping Wounds of South Africa’s Suboptimal Immunisation Coverage: An Implementation Research Imperative for Assessing and Addressing Missed Opportunities for Vaccination

 , ,
, , {kind=link}
Abstract
1. Introduction
2. Routine Childhood Immunisation in South Africa
3. Missed Opportunities for Vaccination as a Driver of Suboptimal Immunisation Coverage
- During visits to health facilities (clinics and hospitals) or mobile health services for immunisation services;
- During visits to health facilities or mobile health services for other preventive services (e.g., growth monitoring sessions);
- During visits to health facilities or mobile health services for curative services (e.g., treatment of fever, cough, diarrhoea, or injuries);
- While accompanying a family member to a health facility for any type of service [13].
4. COVID-19 and the Growing Need for Assessing and Addressing MOV
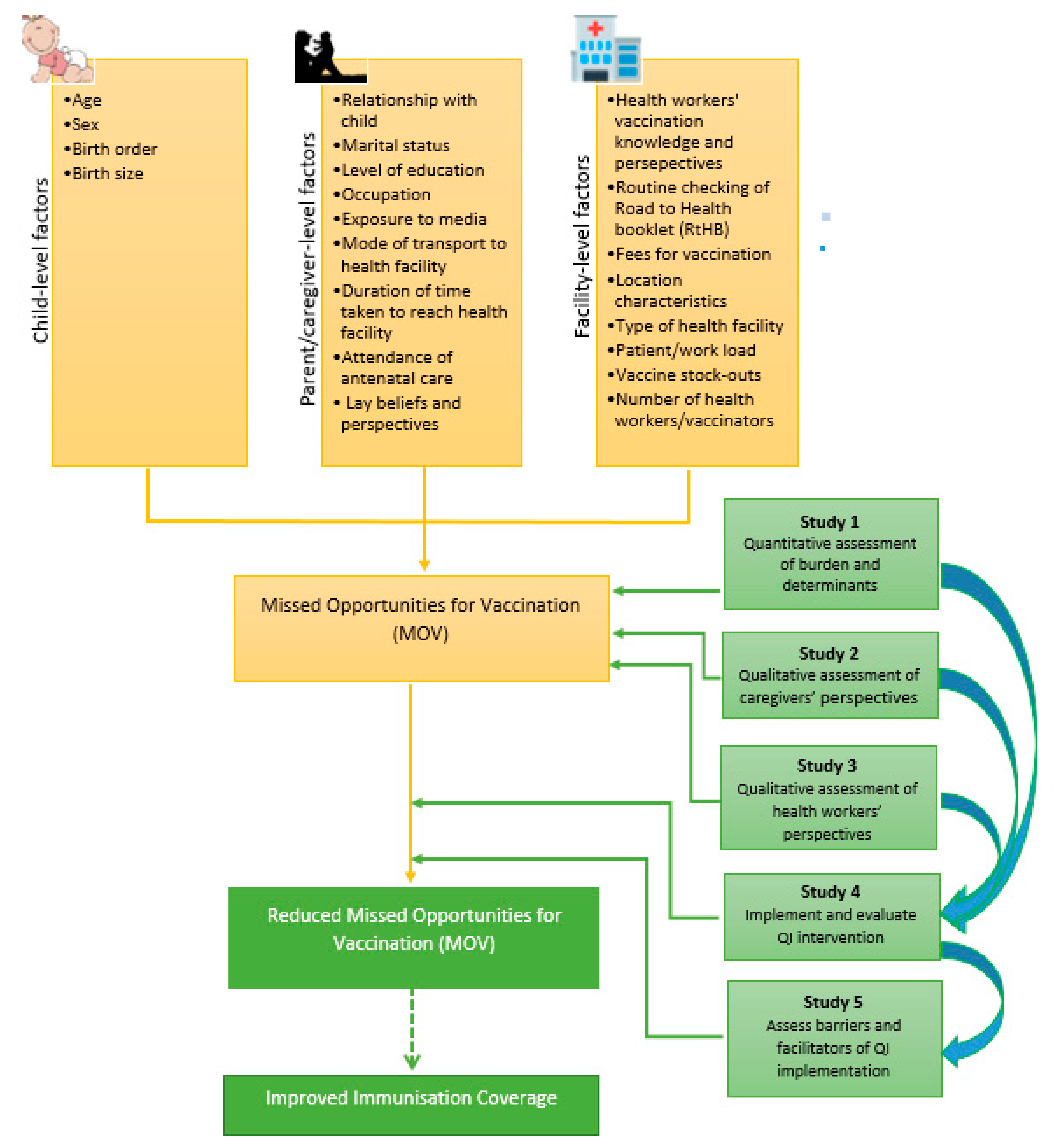
5. An Implementation Research Approach to Assessing and Remedying MOV: Conceptual and Methodological Considerations
5.1. MOV Assessment
5.2. Designing, Implementing, and Evaluating Remedial Actions against MOV
5.3. Post-Implementation Evaluation
5.4. Resource Implications
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wilder-Smith, A.; Longini, I.; Zuber, P.L.; Bärnighausen, T.; Edmunds, W.J.; Dean, N.; Masserey Spicher, V.; Benissa, M.R.; Gessner, B.D. The public health value of vaccines beyond efficacy: Methods, measures and outcomes. BMC Med. 2017, 15, 138. [Google Scholar] [CrossRef]
- Bloom, D.E.; Canning, D.; Weston, M. The value of vaccination. World Econ. Henley Thames 2005, 6, 15. [Google Scholar]
- Maurice, J.M.; Davey, S. State of the World’s Vaccines and Immunization; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Keja, K.; Chan, C.; Hayden, G.; Henderson, R.H. Expanded programme on immunization. World Health Stat. Q. Rapp. Trimest. Stat. Sanit. Mond. 1988, 41, 59–63. [Google Scholar]
- Wiysonge, C.S.; Ngcobo, N.J.; Jeena, P.M.; Madhi, S.A.; Schoub, B.D.; Hawkridge, A.; Shey, M.S.; Hussey, G.D. Advances in childhood immunisation in South Africa: Where to now? Programme managers’ views and evidence from systematic reviews. BMC Public Health 2012, 12, 578. [Google Scholar] [CrossRef]
- World Health Organization. Immunization Coverage 2017. Available online: http://www.who.int/mediacentre/factsheets/fs378/en/ (accessed on 31 October 2017).
- Bennett, D.; Bisanzio, D.; Deribew, A.; Gething, P.; Hay, S.; Ali, R. Global, regional, and national under-5 mortality, adult mortality, age-specific mortality, and life expectancy, 1970–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1084–1150. [Google Scholar]
- Kaslow, D.C.; Kalil, J.; Bloom, D.; Breghi, G.; Colucci, A.M.; De Gregorio, E.; Madhavan, G.; Meier, G.; Seabrook, R.; Xu, X. The role of vaccines and vaccine decision-making to achieve the goals of the Grand Convergence in public health. Vaccine 2017, 35, A10–A15. [Google Scholar] [CrossRef]
- Ozawa, S.; Mirelman, A.; Stack, M.L.; Walker, D.G.; Levine, O.S. Cost-effectiveness and economic benefits of vaccines in low- and middle-income countries: A systematic review. Vaccine 2012, 31, 96–108. [Google Scholar] [CrossRef]
- Nnaji, C.A.; Owoyemi, A.J.; Amaechi, U.A.; Wiyeh, A.B.; Ndwandwe, D.E.; Wiysonge, C.S. Taking stock of global immunisation coverage progress: The gains, the losses and the journey ahead. Int. Health 2020. [Google Scholar] [CrossRef]
- VanderEnde, K.; Gacic-Dobo, M.; Diallo, M.S.; Conklin, L.M.; Wallace, A.S. Global Routine Vaccination Coverage—2017. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1261–1264. [Google Scholar] [CrossRef]
- Wiysonge, C.S.; Uthman, O.A.; Ndumbe, P.M.; Hussey, G.D. Individual and contextual factors associated with low childhood immunisation coverage in sub-Saharan Africa: A multilevel analysis. PLoS ONE 2012, 7, e37905. [Google Scholar] [CrossRef]
- World Health Organization. Methodology for the Assessment of Missed Opportunities for Vaccination; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization (WHO). Immunization Coverage. Available online: https://www.who.int/en/news-room/fact-sheets/detail/immunization-coverage (accessed on 9 May 2021).
- Abbas, K.; Procter, S.R.; van Zandvoort, K.; Clark, A.; Funk, S.; Mengistu, T.; Hogan, D.; Dansereau, E.; Jit, M.; Flasche, S. LSHTM CMMID COVID-19 Working Group. Routine childhood immunisation during the COVID-19 pandemic in Africa: A benefit-risk analysis of health benefits versus excess risk of SARS-CoV-2 infection. Lancet Glob. Health 2020, 8, e1264–e1272. [Google Scholar] [CrossRef]
- Mbunge, E. Effects of COVID-19 in South African health system and society: An explanatory study. Diabetes Metab. Syndr. 2020, 14, 1809–1814. [Google Scholar] [CrossRef] [PubMed]
- Nyasulu, J.; Pandya, H. The effects of coronavirus disease 2019 pandemic on the South African health system: A call to maintain essential health services. Afr. J. Prim. Health Care Fam. Med. 2020, 12, e1–e5. [Google Scholar] [CrossRef]
- Burnett, R.J.; Dlamini, N.R.; Meyer, J.C.; Fernandes, L.; Motloung, B.R.; Ndlovu, T.H.; Simango, H.A.; Kibuuka, D.K.; Dochez, C.; Montwedi, D.N.; et al. Progress towards obtaining valid vaccination coverage data in South Africa. S. Afr. J. Sci. 2019, 115, 4. [Google Scholar] [CrossRef]
- Mothiba, T.M.; Tladi, F.M. Challenges faced by professional nurses when implementing the Expanded Programme on Immunisation at rural clinics in Capricorn District, Limpopo. Afr. J. Prim. Health Care Fam. Med. 2016, 8, e1–e5. [Google Scholar] [CrossRef]
- Coovadia, H.; Jewkes, R.; Barron, P.; Sanders, D.; McIntyre, D. The health and health system of South Africa: Historical roots of current public health challenges. Lancet 2009, 374, 817–834. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO/UNICEF Estimates of National Immunization Coverage, Updated July 2019. Available online: https://www.who.int/immunization/monitoring_surveillance/data/en/ (accessed on 11 September 2019).
- Ndwandwe, D.; Nnaji, C.A.; Mashunye, T.; Uthman, O.A.; Wiysonge, C.S. Incomplete vaccination and associated factors among children aged 12–23 months in South Africa: An analysis of the South African demographic and health survey 2016. Hum. Vaccin. Immunother. 2021, 17, 247–254. [Google Scholar] [CrossRef]
- Jacob, N.; Coetzee, D. Missed opportunities for immunisation in health facilities in Cape Town, South Africa. S. Afr. Med. J. 2015, 105, 917–921. [Google Scholar] [CrossRef]
- National Institute for Communicable Diseases (NICD). Measles Outbreak in a District of Western Cape Province, January–February 2017. Available online: https://www.nicd.ac.za/measles-outbreak-in-a-district-of-western-province-january-february-2017/ (accessed on 17 June 2021).
- le Roux, K.; Akin-Olugbade, O.; Katzen, L.S.; Laurenzi, C.; Mercer, N.; Tomlinson, M.; Rotheram-Borus, M.J. Immunisation coverage in the rural Eastern Cape—Are we getting the basics of primary care right? Results from a longitudinal prospective cohort study. S. Afr. Med. J. 2017, 107, 2016. [Google Scholar]
- Burnett, R.J.; Mmoledi, G.; Ngcobo, N.J.; Dochez, C.; Seheri, L.M.; Mphahlele, M.J. Impact of vaccine stock-outs on infant vaccination coverage: A hospital-based survey from South Africa. Int. Health 2018, 10, 376–381. [Google Scholar] [CrossRef]
- Hutchins, S.S.; Jansen, H.; Robertson, S.E.; Evans, P.; Kim-Farley, R.J. Studies of missed opportunities for immunization in developing and industrialized countries. Bull. World Health Organ. 1993, 71, 549. [Google Scholar]
- Ndwandwe, D.; Nnaji, C.A.; Wiysonge, C.S. The Magnitude and Determinants of Missed Opportunities for Childhood Vaccination in South Africa. Vaccines 2020, 8, 705. [Google Scholar] [CrossRef] [PubMed]
- Ogbuanu, I.U.; Li, A.J.; Anya, B.-P.M.; Tamadji, M.; Chirwa, G.; Chiwaya, K.W.; Djalal, M.E.-H.; Cheikh, D.; Machekanyanga, Z.; Okeibunor, J.; et al. Can vaccination coverage be improved by reducing missed opportunities for vaccination? Findings from assessments in Chad and Malawi using the new WHO methodology. PLoS ONE 2019, 14, e0210648. [Google Scholar] [CrossRef] [PubMed]
- Okeibunor, J.; Ogbuanu, I.; Blanche, A.; Chiwaya, K.; Chirwa, G.; Machekanyanga, Z.; Mihigo, R.; Zawaira, F. Towards a Strategy for Reducing Missed Opportunities for Vaccination in Malawi: Implications of a Qualitative Health Facility Assessment. J. Immunol. Sci. 2018, 2 (Suppl. 7), 46–54. [Google Scholar] [CrossRef]
- Magadzire, B.P.; Joao, G.; Shendale, S.; Ogbuanu, I.U. Reducing missed opportunities for vaccination in selected provinces of Mozambique: A study protocol. Gates Open Res. 2017, 1, 5. [Google Scholar] [CrossRef] [PubMed]
- Sridhar, S.; Maleq, N.; Guillermet, E.; Colombini, A.; Gessner, B.D. A systematic literature review of missed opportunities for immunization in low- and middle-income countries. Vaccine 2014, 32, 6870–6879. [Google Scholar] [CrossRef]
- Uthman, O.A.; Sambala, E.Z.; Adamu, A.A.; Ndwandwe, D.; Wiyeh, A.B.; Olukade, T.; Bishwajit, G.; Yaya, S.; Okwo-Bele, J.-M.; Wiysonge, C.S. Does it really matter where you live? A multilevel analysis of factors associated with missed opportunities for vaccination in sub-Saharan Africa. Hum. Vaccin. Immunother. 2018, 14, 2397–2404. [Google Scholar] [CrossRef] [PubMed]
- Sambala, E.Z.; Uthman, O.A.; Adamu, A.A.; Ndwandwe, D.; Wiyeh, A.B.; Olukade, T.; Bishwajit, G.; Yaya, S.; Okwo-Bele, J.-M.; Wiysonge, C.S. Mind the Gap: What explains the education-related inequality in missed opportunities for vaccination in sub-Saharan Africa? Compositional and structural characteristics. Hum. Vaccin. Immunother. 2018, 14, 2365–2372. [Google Scholar] [CrossRef]
- Li, A.J.; Peiris, T.S.R.; Sanderson, C.; Nic Lochlainn, L.; Mausiry, M.; da Silva, R.B.J.B.M.; Ogbuanu, I.U. Opportunities to improve vaccination coverage in a country with a fledgling health system: Findings from an assessment of missed opportunities for vaccination among health center attendees-Timor Leste, 2016. Vaccine 2019, 37, 4281–4290. [Google Scholar] [CrossRef]
- Adamu, A.A.; Uthman, O.A.; Gadanya, M.A.; Adetokunboh, O.O.; Wiysonge, C.S. A multilevel analysis of the determinants of missed opportunities for vaccination among children attending primary healthcare facilities in Kano, Nigeria: Findings from the pre-implementation phase of a collaborative quality improvement programme. PLoS ONE 2019, 14, e0218572. [Google Scholar] [CrossRef]
- Adedokun, S.T.; Uthman, O.A.; Adekanmbi, V.T.; Wiysonge, C.S. Incomplete childhood immunization in Nigeria: A multilevel analysis of individual and contextual factors. BMC Public Health 2017, 17, 236. [Google Scholar] [CrossRef] [PubMed]
- Etana, B.; Deressa, W. Factors associated with complete immunization coverage in children aged 12–23 months in Ambo Woreda, Central Ethiopia. BMC Public Health 2012, 12, 566. [Google Scholar] [CrossRef] [PubMed]
- Yismaw, A.E.; Assimamaw, N.T.; Bayu, N.H.; Mekonen, S.S. Incomplete childhood vaccination and associated factors among children aged 12–23 months in Gondar city administration, Northwest, Ethiopia 2018. BMC Res. Notes 2019, 12, 241. [Google Scholar] [CrossRef] [PubMed]
- Compaore, W.I.C.Z.; Ekouevi, D.K.; Gbeasor-Komlanvi, F.A.; Sewu, E.K.; Blatome, T.; Gbadoe, A.D.; Agbèrè, D.A.; Atakouma, Y. Immunization coverage and factors associated with incomplete vaccination in children aged 12 to 59 months in health structures in Lome. BMC Res. Notes 2019, 12, 84. [Google Scholar]
- Metcalf, C.A.; Yach, D.; de Beer, Z.J. Missed opportunities for immunisation at hospitals in the western Cape—A reappraisal. S. Afr. Med. J. 1994, 84, 149–152. [Google Scholar]
- Siedner, M.J.; Kraemer, J.D.; Meyer, M.J.; Harling, G.; Mngomezulu, T.; Gabela, P.; Dlamini, S.; Gareta, D.; Majozi, N.; Ngwenya, N.; et al. Access to primary healthcare during lockdown measures for COVID-19 in rural South Africa: A longitudinal cohort study. MedRxiv 2020. [Google Scholar] [CrossRef]
- Siedner, M.J.; Kraemer, J.D.; Meyer, M.J.; Harling, G.; Mngomezulu, T.; Gabela, P.; Dlamini, S.; Gareta, D.; Majozi, N.; Ngwenya, N.; et al. Access to primary healthcare during lockdown measures for COVID-19 in rural South Africa: An interrupted time series analysis. BMJ Open 2020, 10, e043763. [Google Scholar] [CrossRef]
- Department of Health. Quality Improvement—The Key to Providing Improved Quality of Care. 2012. Available online: https://www.idealhealthfacility.org.za/docs/guidelines/Quality%20Improvement%20Guide%202012.pdf (accessed on 25 June 2020).
- Department of Health. National Core Standards for Health Establishments in South Africa. 2011. Available online: http://rhap.org.za/wp-content/uploads/2014/05/National-Core-Standards-2011-1.pdf (accessed on 25 June 2020).
- Acharya, M. Universal Health Coverage as a Distinct Sustainable Development Goals Target: Dispelling Doubts and Underlining Implications. Front. Public Health 2015, 3, 238. [Google Scholar] [CrossRef][Green Version]
- Buse, K.; Hawkes, S. Health in the sustainable development goals: Ready for a paradigm shift? Glob. Health 2015, 11, 13. [Google Scholar] [CrossRef] [PubMed]
- Jessani, N.S.; Siddiqi, S.M.; Babcock, C.; Davey-Rothwell, M.; Ho, S.; Holtgrave, D.R. Factors affecting engagement between academic faculty and decision-makers: Learnings and priorities for a school of public health. Health Res. Policy Syst. 2018, 16, 65. [Google Scholar] [CrossRef]
- Nnaji, C.A.; Wiysonge, C.S.; Okeibunor, J.; Malinga, T.; Adamu, A.A.; Tumusiime, P.; Karamagi, H. Protocol for a scoping review of implementation research approaches to universal health coverage in Africa. BMJ Open 2021, 11, e041721. [Google Scholar] [CrossRef]
- Eccles, M.P.; Mittman, B.S. Welcome to Implementation Science. Implement. Sci. 2006, 1, 1. [Google Scholar] [CrossRef]
- Chin, M.H.; Alexander-Young, M.; Burnet, D.L. Health care quality-improvement approaches to reducing child health disparities. Pediatrics 2009, 124 (Suppl. 3), S224–S236. [Google Scholar] [CrossRef]
- Leatherman, S.; Ferris, T.G.; Berwick, D.; Omaswa, F.; Crisp, N. The role of quality improvement in strengthening health systems in developing countries. Int. J. Qual. Health Care 2010, 22, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Batalden, P.B.; Davidoff, F. What is “quality improvement” and how can it transform healthcare? Qual. Saf. Health Care 2007, 16, 2–3. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, S.; Rustage, K.; Nellums, L.B.; Bardfield, J.E.; Agins, B.; Barker, P.; Massoud, M.R.; Ford, N.P.; Doherty, M.; Dougherty, G.; et al. Do Quality Improvement Initiatives Improve Outcomes for Patients in Antiretroviral Programs in Low- and Middle-Income Countries? A Systematic Review. J. Acquir. Immune Defic. Syndr. 2019, 81, 487–496. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. A Handbook for National Quality Policy and Strategy: A Practical Approach for Developing Policy and Strategy to Improve Quality of Care; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Birken, S.A.; Powell, B.J.; Shea, C.M.; Haines, E.R.; Kirk, M.A.; Leeman, J.; Rohweder, C.; Damschroder, L.; Presseau, J. Criteria for selecting implementation science theories and frameworks: Results from an international survey. Implement. Sci. 2017, 12, 124. [Google Scholar] [CrossRef] [PubMed]
- Foy, R.; Ovretveit, J.; Shekelle, P.G.; Pronovost, P.J.; Taylor, S.L.; Dy, S.; Hempel, S.; McDonald, K.M.; Rubenstein, L.V.; Wachter, R.M. The role of theory in research to develop and evaluate the implementation of patient safety practices. BMJ Qual. Saf. 2011, 20, 453–459. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nnaji, C.A.; Wiysonge, C.S.; Lesosky, M.; Mahomed, H.; Ndwandwe, D. COVID-19 and the Gaping Wounds of South Africa’s Suboptimal Immunisation Coverage: An Implementation Research Imperative for Assessing and Addressing Missed Opportunities for Vaccination. Vaccines 2021, 9, 691. https://doi.org/10.3390/vaccines9070691
Nnaji CA, Wiysonge CS, Lesosky M, Mahomed H, Ndwandwe D. COVID-19 and the Gaping Wounds of South Africa’s Suboptimal Immunisation Coverage: An Implementation Research Imperative for Assessing and Addressing Missed Opportunities for Vaccination. Vaccines. 2021; 9(7):691. https://doi.org/10.3390/vaccines9070691
Chicago/Turabian StyleNnaji, Chukwudi A., Charles S. Wiysonge, Maia Lesosky, Hassan Mahomed, and Duduzile Ndwandwe. 2021. "COVID-19 and the Gaping Wounds of South Africa’s Suboptimal Immunisation Coverage: An Implementation Research Imperative for Assessing and Addressing Missed Opportunities for Vaccination" Vaccines 9, no. 7: 691. https://doi.org/10.3390/vaccines9070691
APA StyleNnaji, C. A., Wiysonge, C. S., Lesosky, M., Mahomed, H., & Ndwandwe, D. (2021). COVID-19 and the Gaping Wounds of South Africa’s Suboptimal Immunisation Coverage: An Implementation Research Imperative for Assessing and Addressing Missed Opportunities for Vaccination. Vaccines, 9(7), 691. https://doi.org/10.3390/vaccines9070691