
What Is the State-of-the-Art in Clinical Trials on Vaccine Hesitancy 2015–2020?


Abstract
1. Introduction
2. Materials and Methods
2.1. Previous Identified Systematic Eeviews
2.1.1. Cochrane Library
2.1.2. PubMed
2.2. Screened Databases/Resources and Dates of Data Collection
2.2.1. Screened Databases/Resources
- PubMed is maintained by the U.S. National Library of Medicine, USA and includes over 30 million citations for biomedical literature e.g., MEDLINE, life science journals, and/or online books [20].
- Cochrane Library is a database of accessible systematic reviews and other synthesized research evidence, namely the Cochrane Database of Systematic Reviews (4–12 issues, since 2003) and Cochrane Central Register of Controlled Trials (CENTRAL) (e.g., CENTRAL is updated source of reports of randomized and quasi-randomized controlled trials, namely from PubMed and Embase-Biomedical database from Elsevier). The mission of Cochrane Library is to promote evidence-informed health decision-making by producing high-quality, relevant, accessible systematic reviews, and other synthesized research evidence [18].
- DOAJ is an online directory that provides access to papers form high quality, open access, peer-reviewed journals (80 languages; 123 countries; 15,678 journals and 5,516,249 articles records on 2 January 2020 [21].
- SciELO is a database comprising a high-quality collection of Brazilian scientific journals (381 journals: 427,662 documents on 2 January 2019) [22].
- b-on provides unlimited and permanent access to research (thousands of scientific journals and online e-books from some of the most important content providers). It started on March 2004, brings together different institutions, such as higher education, scientific research and technological development, hospitals [23]. Importantly, the following collections are available in b-on: Academic Search Complete, Annual reviews, Current Contents (ISI), Elsevier, Essential Science Indicators, IEEE, EBESCO (LISTA), Nature, Sage, Springer, Taylor and Francis, Web of Science and Wiley, among many others (please see https://www.b-on.pt/colecoes, accessed on 5 April 2021).
2.2.2. Dates of Data Collection
2.3. Keywords
2.3.1. Randomized Controlled Trial or Clinical Trial
2.3.2. Vaccine Hesitancy
2.3.3. Vaccination Refusal
2.4. Inclusion and Exclusion Criteria
2.4.1. PICOS Criteria for the Inclusion of Studies
2.4.2. Exclusion Criteria
3. Results
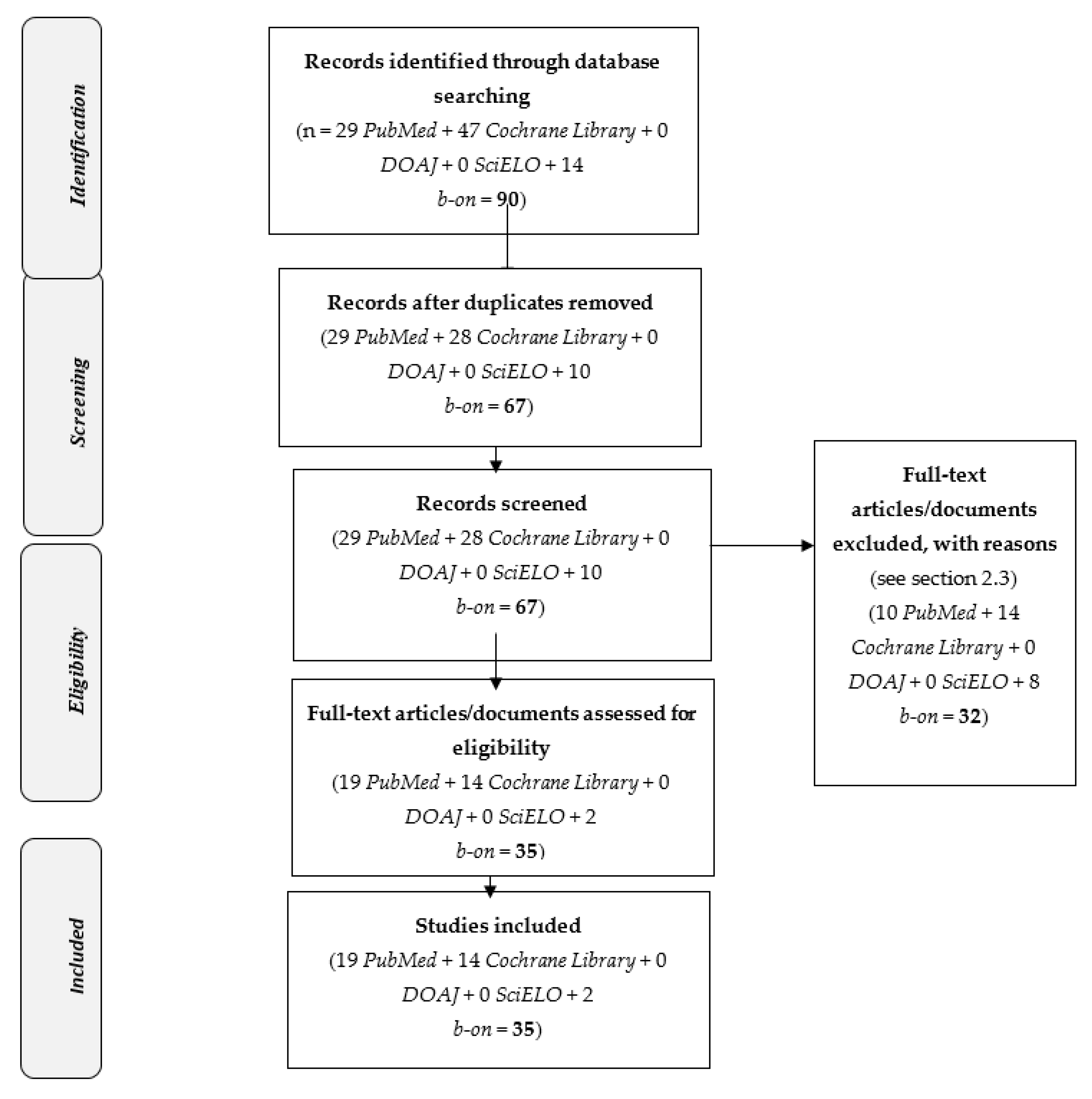
3.1. Selected Studies
3.2. Main Findings of Selected Studies
4. Discussion
- n = 27 studies were selected in a systematic review that aimed to summarize evidence surrounding childhood vaccine hesitancy from the perspective of parents. The main conclusion of this systematic review was that healthcare professionals should take the caregivers’ “desire to do what they feel right for the child” into consideration [25].
- n = 43 studies were selected in a systematic review that aimed to evaluate differences by individual socioeconomic status in terms of the uptake of publicly funded childhood vaccines and in cognitive determinants (beliefs, attitudes) of parental decisions about vaccinating their children in developed countries with programs addressing major financial barriers to vaccination access. This systematic review concluded that mandatory and recommended vaccines should be provided 100% free of charge and the administration of vaccines reimbursed, since barriers to vaccination access persist, and tailored interventions are recommended for vaccine-hesitant parents [54].
- n = 11 studies were selected in a systematic review that aimed to provide quantitative comparative data on any measure of vaccine uptake. According to the findings of this systematic review: email communication seems to increase vaccine uptake when compared with no intervention [55].
4.1. Children/Pediatric
- Tailoring the information to the target audience.
- Understanding parent’s hesitancy, and the specific context (e.g., management of misinformation about vaccination).
- Presenting vaccination as the default approach (e.g., early in pregnancy in prenatal appointments and the first postnatal appointment); both social and individual responsibility should be communicated.
- Using technology to promote vaccination.
4.2. Online or Electronic Information
- Virtual reality through a head-mounted display unit promoted participant’s understanding of key immunization concepts and their integration in the story [8].
- An expert moderated vaccine social media website constituted a suitable platform for parents to collect accurate vaccine information, express vaccine concerns, and/or ask questions to vaccine experts; this site was developed for parents of children 24 months of age or younger [29].
- The use of an app produced positive outcomes (e.g., provision of appropriated vaccine information) [30].
- Among vaccine hesitant pregnant women, an Internet-based intervention/platform positively enhanced vaccine hesitant parent’s attitudes on vaccines [31]; and
- During pregnancy, parental vaccine behaviors may be positively influenced by a web-based vaccine information with social media applications [32].
4.3. Vaccination Against a Specific Disease
4.3.1. Human Papillomavirus Infection
- Preadolescent fear of needles was a negative predictor of subsequent HPV vaccine uptake. This fear may be reduced by avoiding same-day preschool injections (4–6 years); i.e., the administration of two immunizations on the same day should be preferably avoided [12].
- A significant number of Latin immigrant mothers of daughters (9–12 years) (around one-third of participants) was HPV vaccine hesitant. Thus, besides recommending HPV vaccination, health professionals should raise awareness on additional HPV complications e.g., HPV and cervical cancer or reinforcing daughters’ perceived risk of HPV infection [9].
- A multi-component communication-based intervention improved healthcare provider’s communication about HPV vaccination (11–12 years children), with improved HPV vaccination rates [33].
- A provider’s ‘very strong’ recommendation on adolescent vaccination was associated with a greater perceived urgency for getting vaccinated, greater trust in the information received, decreased vaccine hesitancy, and increased vaccine receipt [35].
- Motivational interviews facilitated dialogues between health professionals (e.g., nurse practitioner or physician assistant) and vaccine-hesitant parents, with the improvement of HVP vaccine acceptance [37].
4.3.2. Influenza
4.3.3. Diphtheria Tetanus Toxoid and Pertussis
4.3.4. COVID-2019
4.4. Miscellaneous: Extrinsic Factors
4.4.1. Reminder-Recall Approaches
- (i)
- more predominant in higher income regions than in lower income ones (maybe because telephone call and/or postal communications are widely disseminated in high income countries).
- (ii)
- associated to variable changes in vaccines uptake (maybe because more subjects are contacted through this type of intervention, which is likely to identify more causes of vaccine hesitancy), and
- (iii)
- insufficient to control multiple causes of hesitancy (maybe because multifactorial causes of hesitance require multiple types of interventions to be controlled) [19].
4.4.2. Tools to Evaluate Subject’s Vaccine Hesitancy
4.4.3. Compulsory Vaccination
4.5. Educational Strategies
4.5.1. Educational Strategies for Health Professionals
4.5.2. Educational Strategies for Patients/Parents
4.6. Study Limitations and Potential Biases of the Selected Studies
4.6.1. Study Limitations of the Selected Studies
4.6.2. Potential Study Biases of the Selected Studies
- Potential confounding biases (i.e., “spurious association made between the outcome and a factor that is not itself causally related to the outcome and occurs if the factor is associated with a range of other characteristics that do increase the outcome risk”) [65,66]: Triangulations methodologies were not applied (e.g., just one tool or none tool was applied to characterize the level of subjects’ vaccine hesitancy) and in general, the number and type of collected sociodemographic data were limited.
4.7. Future Research Directions
4.8. Study Strengths
4.9. Potential Study Limitations of the Present Systematic Review
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kestenbaum, L.A.; Feemster, K.A. Identifying and Addressing Vaccine Hesitancy. Pediatr. Ann. 2015, 44, e71–e75. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E. SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Leask, J.; Kinnersley, P.; Jackson, C.; Cheater, F.; Bedford, H.; Rowles, G. Communicating with parents about vaccination: A framework for health professionals. BMC Pediatr. 2012, 12, 154. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Facciolà, A.; Visalli, G.; Orlando, A.; Bertuccio, M.P.; Spataro, P.; Squeri, R.; Picerno, I.; Di Pietro, A. Vaccine hesitancy: An overview on parents’ opinions about vaccination and possible reasons of vaccine refusal. J. Public Health Res. 2019, 8, 1436. [Google Scholar] [CrossRef] [PubMed]
- Oyo-Ita, A.; Wiysonge, C.S.; Oringanje, C.; Nwachukwu, C.E.; Oduwole, O.; Meremikwu, M.M. Interventions for improving coverage of childhood immunisation in low- and middle-income countries. Cochrane Database Syst. Rev. 2016, 7, CD008145. [Google Scholar] [CrossRef] [PubMed]
- Opel, D.J.; Henrikson, N.; Lepere, K.; Hawkes, R.; Zhou, C.; Dunn, J.; Taylor, J.A. Previsit Screening for Parental Vaccine Hesitancy: A Cluster Randomized Trial. Pediatrics 2019, 144, e20190802. [Google Scholar] [CrossRef]
- Nowak, G.J.; Evans, N.J.; Wojdynski, B.W.; Ahn, S.J.; Len-Rios, M.E.; Carera, K.; Hale, S.; McFalls, D. Using immersive virtual reality to improve the beliefs and intentions of influenza vaccine avoidant 18-to-49-year-olds: Considerations, effects, and lessons learned. Vaccine 2020, 38, 1225–1233. [Google Scholar] [CrossRef] [PubMed]
- Khodadadi, A.B.; Redden, D.T.; Scarinci, I.C. HPV Vaccination Hesitancy among Latina Immigrant Mothers Despite Physician Recommendation. Ethn. Dis. 2020, 30, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Nekrasova, E.; Stockwell, M.S.; Localio, R.; Shults, J.; Wynn, C.; Shone, L.P.; Berrigan, L.; Kolff, C.; Griffith, M.; Johnson, A.; et al. Vaccine hesitancy and influenza beliefs among parents of children requiring a second dose of influenza vaccine in a season: An American Academy of Pediatrics (AAP) Pediatric Research in Office Settings (PROS) study. Hum. Vaccines Immunother. 2020, 16, 1070–1077. [Google Scholar] [CrossRef]
- Abukhaled, M.; Cortez, S. Nonpharmacological Methods for Reducing Parental Concern for Infant Vaccine-Associated Pain. J. Pediatr. Health Care 2020, 35, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Baxter, A.L.; Cohen, L.L.; Burton, M.; Mohammed, A.; Lawson, M.L. The number of injected same-day preschool vaccines relates to preadolescent needle fear and HPV uptake. Vaccine 2017, 35, 4213–4219. [Google Scholar] [CrossRef] [PubMed]
- Pahud, B.; Elizabeth, S.; Lee, B.R.; Lewis, K.O.; Middleton, D.B.; Clark, S.; Humiston, S.G. A randomized controlled trial of an online immunization curriculum. Vaccine 2020, 38, 7299–7307. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef] [PubMed]
- Guidry, J.; Laestadius, L.I.; Vraga, E.K.; Miller, C.A.; Perrin, P.B.; Burton, C.W.; Ryan, M.; Fuemmeler, B.F.; Carlyle, K.E. Willingness to get the COVID-19 vaccine with and without emergency use authorization. Am. J. Infect. Control. 2020, 49, 137–142. [Google Scholar] [CrossRef]
- PRISMA. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 2020. Available online: http://www.prisma-statement.org/CochraneLibrary (accessed on 30 December 2020).
- Cochrane Library. The Cochrane Database of Systematic Reviews. 2020. Available online: https://www.cochranelibrary.com/ (accessed on 30 December 2020).
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J. SAGE Working Group on Vaccine Hesitancy. Strategies for addressing vaccine hesitancy—A systematic review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [PubMed]
- PubMed. PubMed.gov US National Library of Medicine National Institutes of Health. 2020. Available online: https://pubmed.ncbi.nlm.nih.gov/ (accessed on 30 December 2020).
- DOAJ. Directory of Open Access Journals (DOAJ). 2020. Available online: https://doaj.org/ (accessed on 30 December 2020).
- SciELO. Scientific Electronic Library Online. 2020. Available online: https://scielo.org/ (accessed on 30 December 2020).
- b-on. Biblioteca do Conhecimento online. Available online: https://www.b-on.pt/ (accessed on 30 December 2020).
- Chapman, D. Health-related databases. J. Can. Acad. Child Adolesc. 2009, 18, 148–149. [Google Scholar]
- Díaz Crescitelli, M.; Ghirotto, L.; Sisson, H.; Sarli, L.; Artioli, G.; Bassi, M.; Appicciutoli, G.; Hayter, M. A meta-synthesis study of the key elements involved in childhood vaccine hesitancy. Public Health 2020, 180, 38–45. [Google Scholar] [CrossRef]
- Henrikson, N.B.; Anderson, M.L.; Opel, D.J.; Dunn, J.; Marcuse, E.K.; Grossman, D.C. Longitudinal Trends in Vaccine Hesitancy in a Cohort of Mothers Surveyed in Washington State, 2013–2015. Public Health Rep. 2017, 132, 451–454. [Google Scholar] [CrossRef]
- Philpott, S.E.; Witteman, H.O.; Jones, K.M.; Sonderman, D.S.; Julien, A.S.; Politi, M.C. Clinical trainees’ responses to parents who question evidence-based recommendations. Patient Educ. Couns. 2017, 100, 1701–1708. [Google Scholar] [CrossRef] [PubMed]
- Taddio, A.; Riddell, R.P.; Ipp, M.; Moss, S.; Baker, S.; Tolkin, J.; Malini, D.; Feerasta, S.; Govan, P.; Fletcher, E.; et al. Relative effectiveness of additive pain interventions during vaccination in infants. Can. Med Assoc. J. 2017, 189, E227–E234. [Google Scholar] [CrossRef] [PubMed]
- Shoup, J.A.; Narwaney, K.J.; Wagner, N.M.; Kraus, C.R.; Gleason, K.S.; Albright, K.; Glanz, J.M. Social Media Vaccine Websites: A Comparative Analysis of Public and Moderated Websites. Health Educ. Behav. 2019, 46, 454–462. [Google Scholar] [CrossRef]
- Salmon, D.A.; Limaye, R.J.; Dudley, M.Z.; Oloko, O.K.; Church-Balin, C.; Ellingson, M.K.; Spina, C.I.; Brewer, S.E.; Orenstein, W.A.; Halsey, N.A.; et al. MomsTalkShots: An individually tailored educational application for maternal and infant vaccines. Vaccine 2019, 37, 6478–6485. [Google Scholar] [CrossRef] [PubMed]
- Daley, M.F.; Narwaney, K.J.; Shoup, J.A.; Wagner, N.M.; Glanz, J.M. Addressing Parents’ Vaccine Concerns: A Randomized Trial of a Social Media Intervention. Am. J. Prev. Med. 2018, 55, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Glanz, J.M.; Wagner, N.M.; Narwaney, K.J.; Kraus, C.R.; Shoup, J.A.; Xu, S.; O’Leary, S.T.; Omer, S.B.; Gleason, K.S.; Daley, M.F. Web-based Social Media Intervention to Increase Vaccine Acceptance: A Randomized Controlled Trial. Pediatrics 2017, 140, e20171117. [Google Scholar] [CrossRef]
- Reno, J.E.; Thomas, J.; Pyrzanowski, J.; Lockhart, S.; O’Leary, S.T.; Campagna, E.J.; Dempsey, A.F. Examining strategies for improving healthcare providers’ communication about adolescent HPV vaccination: Evaluation of secondary outcomes in a randomized controlled trial. Hum. Vaccines Immunother. 2019, 15, 1592–1598. [Google Scholar] [CrossRef]
- Panozzo, C.A.; Head, K.J.; Kornides, M.L.; Feemster, K.A.; Zimet, G.D. Tailored Messages Addressing Human Papillomavirus Vaccination Concerns Improves Behavioral Intent Among Mothers: A Randomized Controlled Trial. J. Adolesc. Health 2020, 67, 253–261. [Google Scholar] [CrossRef]
- Dempsey, A.F.; Pyrzanowski, J.; Campagna, E.J.; Lockhart, S.; O’Leary, S.T. Parent report of provider HPV vaccine communication strategies used during a randomized, controlled trial of a provider communication intervention. Vaccine 2019, 37, 1307–1312. [Google Scholar] [CrossRef]
- Kornides, M.L.; Feemster, K.A.; Head, K.J.; Zimet, G.D.; Panozzo, C.A. Tailored messages addressing mothers’ HPV vaccina-tion concerns: Differences in response by child sex. J. Women’s Health 2019, 28, 1587–1588. [Google Scholar] [CrossRef]
- Reno, J.E.; O’Leary, S.; Garrett, K.; Pyrzanowski, J.; Lockhart, S.; Campagna, E.; Barnard, J.; Dempsey, A.F. Improving Provider Communication about HPV Vaccines for Vaccine-Hesitant Parents Through the Use of Motivational Interviewing. J. Health Commun. 2018, 23, 313–320. [Google Scholar] [CrossRef]
- Henrikson, N.B.; Zhu, W.; Baba, L.; Nguyen, M.; Berthoud, H.; Gundersen, G.; Hofstetter, A.M. Outreach and Reminders to Improve Human Papillomavirus Vaccination in an Integrated Primary Care System. Clin. Pediatr. 2018, 57, 1523–1531. [Google Scholar] [CrossRef]
- O’Leary, S.; Pyrzanowski, J.; Lockhart, S.; Barnard, J.; Campagna, E.; Garrett, K.; Fisher, A.; Dickinson, M.; Dempsey, A. Impact of a Provider Communication Training Intervention on Adolescent Human Papillomavirus Vaccination: A Cluster Randomized, Clinical Trial. Open Forum Infect. Dis. 2017, 4, S61. [Google Scholar] [CrossRef][Green Version]
- Giese, H.; Neth, H.; Moussaïd, M.; Betsch, C.; Gaissmaier, W. The echo in flu-vaccination echo chambers: Selective attention trumps social influence. Vaccine 2020, 38, 2070–2076. [Google Scholar] [CrossRef] [PubMed]
- Real, F.J.; DeBlasio, D.; Beck, A.F.; Ollberding, N.J.; Davis, D.; Cruse, B.; Samaan, Z.; McLinden, D.; Klein, M.D. A Virtual Reality Curriculum for Pediatric Residents Decreases Rates of Influenza Vaccine Refusal. Acad. Pediatr. 2017, 17, 431–435. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, S.T.; Narwaney, K.J.; Wagner, N.M.; Kraus, C.R.; Omer, S.B.; Glanz, J.M. Efficacy of a Web-Based Intervention to Increase Uptake of Maternal Vaccines: An RCT. Am. J. Prev. Med. 2019, 57, e125–e133. [Google Scholar] [CrossRef]
- Nagar, R.; Venkat, P.; Stone, L.D.; Engel, K.A.; Sadda, P.; Shahnawaz, M. A cluster randomized trial to determine the effectiveness of a novel, digital pendant and voice reminder platform on increasing infant immunization adherence in rural Udaipur, India. Vaccine 2018, 36, 6567–6577. [Google Scholar] [CrossRef]
- Bogart, L.M.; Ojikutu, B.O.; Tyagi, K.; Klein, D.J.; Mutchler, M.G.; Dong, L.; Lawrence, S.J.; Thomas, D.R.; Kellman, S. COVID-19 Related Medical Mistrust, Health Impacts, and Potential Vaccine Hesitancy among Black Americans Living with HIV. JAIDS J. Acquir. Immune Defic. Syndr. 2020, 86, 200–207. [Google Scholar] [CrossRef]
- Xu, Y.; Margolin, D.; Niederdeppe, J. Testing Strategies to Increase Source Credibility through Strategic Message Design in the Context of Vaccination and Vaccine Hesitancy. Health Commun. 2020, 1–14. [Google Scholar] [CrossRef]
- Domek, G.J.; O’Leary, S.T.; Bull, S.; Bronsert, M.; Contreras-Roldan, I.L.; Ventura, G.A.B.; Kempe, A.; Asturias, E.J. Measuring vaccine hesitancy: Field testing the WHO SAGE Working Group on Vaccine Hesitancy survey tool in Guatemala. Vaccine 2018, 36, 5273–5281. [Google Scholar] [CrossRef]
- Karimah, A.; Abd, H.B. Healthcare professional and health belief and attitude influenced vaccine hesitancy among parents living in Kuantan, Pahang. Med J. Malays. 2017, 72, 64. [Google Scholar]
- Betsch, C.; Böhm, R. Detrimental effects of introducing partial compulsory vaccination: Experimental evidence. Eur. J. Public Health 2016, 26, 378–381. [Google Scholar] [CrossRef]
- Norton, Z.; Sanguino, S. Development and evaluation of a comprehensive vaccine hesitancy curriculum. Acad. Pediatr. 2019, 19, e2. [Google Scholar] [CrossRef]
- Gagneur, A.; Battista, M.-C.; Boucher, F.D.; Tapiero, B.; Quach, C.; De Wals, P.; Lemaitre, T.; Farrands, A.; Boulianne, N.; Sauvageau, C.; et al. Promoting vaccination in maternity wards—Motivational interview technique reduces hesitancy and enhances intention to vaccinate, results from a multicentre non-controlled pre- and post-intervention RCT-nested study, Quebec, March 2014 to February 2015. Eurosurveillance 2019, 24, 1800641. [Google Scholar] [CrossRef] [PubMed]
- Gagneur, A.; Lemaître, T.; Gosselin, V.; Farrands, A.; Carrier, N.; Petit, G.; Valiquette, L.; De Wals, P. A postpartum vaccination promotion intervention using motivational interviewing techniques improves short-term vaccine coverage: PromoVac study. BMC Public Health 2018, 18, 811. [Google Scholar] [CrossRef]
- Fisher, W.; Yaremko, J.; Brown, V.; Garfield, H.; Rampakakis, E.; Boikos, C.; Mansi, J.A. The Effect of Information–Motivation–Behavioral Skills Model-Based Continuing Medical Education on Pediatric Influenza Immunization Uptake: A Randomized, Controlled Trial. Open Forum Infect. Dis. 2018, 5, S740. [Google Scholar] [CrossRef][Green Version]
- Henrikson, N.B.; Opel, D.J.; Grothaus, L.; Nelson, J.; Scrol, A.; Dunn, J.; Faubion, T.; Roberts, M.; Marcuse, E.K.; Grossman, D.C. Physician Communication Training and Parental Vaccine Hesitancy: A Randomized Trial. Pediatrics 2015, 136, 70–79. [Google Scholar] [CrossRef]
- Bocquier, A.; Ward, J.; Raude, J.; Peretti-Watel, P.; Verger, P. Socioeconomic differences in childhood vaccination in developed countries: A systematic review of quantitative studies. Expert Rev. Vaccines 2017, 16, 1107–1118. [Google Scholar] [CrossRef]
- Frascella, B.; Oradini-Alacreu, A.; Balzarini, F.; Signorelli, C.; Lopalco, P.L.; Odone, A. Effectiveness of email-based reminders to increase vaccine uptake: A systematic review. Vaccine 2020, 38, 433–443. [Google Scholar] [CrossRef]
- Olson, O.; Berry, C.; Kumar, N. Addressing Parental Vaccine Hesitancy towards Childhood Vaccines in the United States: A Systematic Literature Review of Communication Interventions and Strategies. Vaccines 2020, 8, 590. [Google Scholar] [CrossRef]
- Ashfield, S.; Donelle, L. Parental Online Information Access and Childhood Vaccination Decisions in North America: Scoping Review. J. Med Internet Res. 2020, 22, e20002. [Google Scholar] [CrossRef]
- Karafillakis, E.; Simas, C.; Jarrett, C.; Verger, P.; Peretti-Watel, P.; Dib, F.; De Angelis, S.; Takacs, J.; Ali, K.A.; Celentano, L.P.; et al. HPV vaccination in a context of public mistrust and uncertainty: A systematic literature review of determinants of HPV vaccine hesitancy in Europe. Hum. Vaccines Immunother. 2019, 15, 1615–1627. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef] [PubMed]
- Loubet, P.; Launay, O. Vaccination de l’adulte: Données générales, actualités et perspectives [Adult immunisation: General points, hot topics and perspectives]. Rev. Med. Interne 2017, 38, 749–759. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.; Ryan, R.; Walsh, L.; Horey, D.; Leask, J.; Robinson, P. Face-to-face interventions for informing or educat-ing parents about early childhood vaccination. Cochrane Database Syst. Rev. 2018, 5, CD010038. [Google Scholar] [PubMed]
- Dyda, A.; King, C.; Dey, A.; Leask, J.; Dunn, A.G. A systematic review of studies that measure parental vaccine attitudes and beliefs in childhood vaccination. BMC Public Health 2020, 20, 1253. [Google Scholar] [CrossRef] [PubMed]
- Gualano, M.R.; Olivero, E.; Voglino, G.; Corezzi, M.; Rossello, P.; Vicentini, C.; Bert, F.; Siliquini, R. Knowledge, attitudes and beliefs towards compulsory vaccination: A systematic review. Hum. Vaccines Immunother. 2019, 15, 918–931. [Google Scholar] [CrossRef]
- Lambert, J. Statistics in Brief: How to Assess Bias in Clinical Studies? Clin. Orthop. Relat. Res. 2011, 469, 1794–1796. [Google Scholar] [CrossRef]
- Delgado-Rodríguez, M.; Llorca, J. Bias. J. Epidemiol. Community Health 2004, 58, 635–641. [Google Scholar] [CrossRef]
- Jakovljevic, M.; Timofeyev, Y.; Ranabhat, C.L.; Fernandes, P.O.; Teixeira, J.P.; Rancic, N.; Reshetnikov, V. Real GDP growth rates and healthcare spending—Comparison between the G7 and the EM7 countries. Glob. Health 2020, 16, 64. [Google Scholar] [CrossRef]
- Van Hooste, W.L.C.; Bekaert, M. To Be or Not to Be Vaccinated? The Ethical Aspects of Influenza Vaccination among Healthcare Workers. Int. J. Environ. Res. Public Health 2019, 16, 3981. [Google Scholar] [CrossRef] [PubMed]
- Jakovljevic, M.; Jakab, M.; Gerdtham, U.; McDaid, D.; Ogura, S.; Varavikova, E.; Merrick, J.; Adany, R.; Okunade, A.; Getzen, T.E. Comparative financing analysis and political economy of noncommunicable diseases. J. Med Econ. 2019, 22, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Uman, L.S. Systematic reviews and meta-analyses. J. Can. Acad. Child Adolesc. Psychiatry 2020, 20, 57–59. [Google Scholar]
- Ganeshkumar, P.; Gopalakrishnan, S. Systematic reviews and meta-analysis: Understanding the best evidence in primary healthcare. J. Fam. Med. Prim. Care 2013, 2, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Wong, R.M. Vaccine hesitancy and perceived behavioral control: A meta-analysis. Vaccine 2020, 38, 5131–5138. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Lawes-Wickwar, S.; Ghio, D.; Tang, M.Y.; Keyworth, C.; Stanescu, S.; Westbrook, J.; Jenkinson, E.; Kassianos, A.; Scanlan, D.; Garnett, N.; et al. A Rapid Systematic Review of Public Responses to Health Messages Encouraging Vaccination against Infectious Diseases in a Pandemic or Epidemic. Vaccines 2021, 9, 72. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author(s), Year, Country, DataBase | Objective(s) | No. of Participants | Methods and Results | Conclusions |
|---|---|---|---|---|
| Children/pediatric | ||||
| 1. (Abukhaled et al., 2020) [11] USA, Bon | To alleviate parental concern about pain and to facilitate infant immunization. | 30 pediatric nurses; 100 participants | Methods: A nonpharmacological intervention (breastfeeding or 24% sucrose solution: infants up to 6 months). Results: a significant reduction of parental concern about vaccine pain (pre- vs. postintervention; p = 0.035). | Nonpharmacological methods may relieve infants’ pain undergoing vaccination, improve vaccination rates and reduce parental concern about pain. |
| 2. (Opel et al., 2019) [7] USA PubMed | To evaluate the effect of vaccine hesitancy screening on childhood vaccine uptake. | 156 parents (65 intervention) | Methods: Parents received the Parent Attitudes About Childhood Vaccines Survey (PACV). Placebo survey items were purposively included in PACV. Intervention: providers received a summary of PACV responses. Control: Results of placebo items were provided. Outcome: Immunization status of children (8 months of age) expressed as % of days under-immunized. Results: outcomes between groups were not statistically significant. | Parents’ vaccine hesitancy was not significantly associated with % of days under-immunized. |
| 3. (Henrikson et al., 2017) [26] USA PubMed | To evaluate how parental vaccine hesitancy changes with the age of children. | 237 mothers | Methods: Intervention (providers received training) and control (no training). Results: Both groups presented similar proportions of vaccine hesitant parents (baby’s birth and at 6 and 24 months). The proportion of mothers who were vaccine hesitant significantly decreased (p = 0.01) from child’s birth to age 24 months. | Vaccine hesitancy was variable, with a peak around childbirth and a likely remit as parents’ experience with vaccines increase. |
| 4. (Philpott et al., 2017) [27] USA PubMed | To examine clinician’s attitudes, beliefs, and behavioral intentions about discussing evidence and eliciting values. | 132 medical students and pediatric residents | Methods: Participants were required to read three scenarios. One scenario: a parent of a one-year-old children was hesitant about vaccination. Administration of an opinion questionnaire. Results: Health professionals considered the conversation about vaccine hesitancy less relevant, perceived parents as difficult, and had lower respect for parents’ views (p < 0.0001). | Attitudes of clinicians seems to impact conversations with vaccine hesitant patients. |
| 5. (Taddio et al., 2017) [28] Toronto, ON, Canada PubMed | To compare the effectiveness of additive pain interventions during vaccine injections in the first year of life. | 352 infants | Methods: groups: (i) placebo (control); (ii) parent-directed video education about infant soothing; (iii) video plus oral sucrose or (iv) video, oral sucrose, and topical lidocaine (vaccine injections at 2, 4, 6 and 12 months). Injection techniques to minimize pain (all groups). The Modified Behavioral Pain Scale was applied to evaluate pain distress at pre injection, vaccine injection (needle), and 1 min post injection (recovery). Results: Needle pain significantly differed among groups (p = 0.003) and across ages (p < 0.001). Consistent analgesia was only achieved with topical lidocaine. | Topical lidocaine during vaccination seems to control pain in the first year of life. |
| Online or electronic information | ||||
| 6. (Nowak et al., 2020) [8] USA Cochrane Library | To evaluate if the administration of vaccine information statements (VIS) plus an immersive virtual reality (VR), short video or electronic pamphlet story conveying community immunity benefits of influenza vaccination ameliorate (or not) participants’ influenza-related perceptions and influenza vaccination-related beliefs, confidence, and intentions. | 171 participants (Flu vaccine avoidant). | Methods: Intervention groups: (i) VR + VIS; (ii) video + VIS; and (iii) e-pamphlet + VIS. Control: an influenza VIS-only. VR: Participants wore a head-mounted display unit and video game controllers to experience a five-minute VR story. Video: The same content of the VR condition. e-pamphlet: the text and static images of the video were viewed in a tablet. Results: VR produced a stronger perception of presence in the story, increased participants’ concerns about transmitting influenza to others and boosted vaccination intention. Participants´ concerns about transmitting influenza encouraged vaccination. | VR increased participants’ understanding of key immunization concepts through promoting the sense of presence in story. VR may be useful to address the problem of vaccination hesitancy. |
| 7. (Shoup et al., 2019) [29] USA PubMed | To evaluate and compare the interactive content of an expert moderated vaccine social media (VSM) website, which was purposively developed for parents of children 24 months of age or younger vs. publicly available websites (PAW). | 542 mothers (and partners). | Methods: two groups: PAW and VSM. Vaccine hesitancy was accessed with Parent Attitudes and Childhood Vaccines survey. Results: Tone, vaccine stance, and accuracy of information were significantly better in VSM than PAW (p <0.05). Participants’ interactions: ask questions to vaccine experts (n = 36; 59%), chat sessions (n = 15; 25%), blogs (n = 7; 11%), and discussion boards (n = 3; 5%). | VSM offered a suitable platform for parents to collect accurate vaccine information, express vaccine concerns and ask questions to experts. Regarding VSM consultation, participants were less likely to post inaccurate information. PAW tended to be contentious, presented a negative stance toward vaccines and comprised inaccurate information. |
| 8. (Salmon et al., 2019) [30] USA Cochrane Library | To evaluate self-reported information needs (pre-and post-videos), among pregnant woman using a MomsTalkShots (an app) and to evaluate app usability. | 1103 pregnant woman. | Methods: pre- and post-videos (app). Videos: animations to communicate attracting and interesting messages about vaccination. Participants’ sociodemographic data and vaccine attitudes, beliefs, and intentions were collected with a questionnaire. Results: MomsTalkShots (classification): helpful (95%), trustworthy (94%), interesting (97%), and clear to understand (99%). Similar classifications were obtained for vaccine hesitant woman. 72% of woman who mentioned not having enough vaccine information pre-videos, subsequently reported enough information (post-videos). | The developed app was well-received among pregnant women, even among vaccine hesitant ones. |
| 9. (Daley et al., 2018) [31] USA PubMed | To assess the impact of an internet-based platform on parent’s vaccine related attitudes. | 945 | Methods: A questionnaire about parent’s vaccine-related attitudes (at baseline and when their child was aged 3–5 and 12–15 months). Groups: (i) a website with vaccine information and social media components; (ii) a website with vaccine information only or (iii) usual care. Outcome: Changes in parent’s vaccine attitudes. Results: Vaccine hesitant parents showed significant improvements on vaccination benefits. Parent’s concerns about vaccination risks were significantly reduced. | An internet-based intervention positively improved the attitudes of vaccine hesitant parents. |
| 10. (Glanz et al., 2017) [32] USA PubMed | To determine if a Web-based, social media intervention increases early childhood immunization. | 888 pregnant women | Methods: Groups: (i) a Website with vaccine information and interactive social media (VSM), (ii) a Website with vaccine information (VI), or (iii) usual care (UC). Outcome: Number of days under-vaccinated (from birth to age of 200 days). Results: The mean ranks of the number of days under-vaccinated were significantly lower in the VSM arm vs. UC (p = 0.02). Proportions of infants up to date at age of 200 days: 92.5 (VSM), 91.3 (VI), and 86.6 (UC). | Web-based vaccine information and social media applications may positively influence parental vaccine behaviors. |
| Vaccination against a specific disease: Human papillomavirus infection | ||||
| 11. (Khodadadi et al., 2020) [9] USA Cochrane Library | To evaluate HPV vaccine hesitancy, among Latina immigrant mothers of daughters (9–12 years). | 317 Latina immigrant mothers | Methods: A survey was administered at baseline (participant’s sociodemographic data, knowledge and perceived risk of cervical cancer/HPV infection, self-efficacy, and intention to vaccinate their unvaccinated daughters). Mothers’ vaccine hesitancy was quantified. Results: 35.3% of vaccine hesitant mothers. Multivariable model: explanatory variables of vaccine hesitancy (daughter’s health insurance status; HPV awareness; perceived risk of HPV infection; perceived self-risk of cervical cancer; and a self-efficacy score of ability to complete the HPV vaccination series). | Latina immigrant mothers may not feel motivated to vaccinate their daughters after receiving physicians´ recommendations. Mother’s awareness on other HPVvaccination topics, such as HPV and cervical cancer should be improved. |
| 12. (Reno et al., 2020) [33] USA Cochrane Library | To evaluate the impact of a multi-component communication-based intervention about HPV vaccination (11–12 years children) on vaccination rates. | 149 (baseline) and 187 (post-intervention) providers | Methods: Baseline (n = 75 control and intervention n = 74) and post-intervention (control n = 108 and intervention n = 79). Intervention group: a motivational interviewing and a fact sheet with vaccine hesitant parents (communication components). Results: Providers reported higher perceived levels of parental HPV vaccine acceptance in intervention than control. Communication components improved HPV vaccination rates. | A multi-component communication-based intervention may contribute to improve the perceived level of parental HPV vaccine acceptance and vaccination rates. |
| 13. (Panozzo et al., 2020) [34] USA Cochrane Library | To evaluate if supplementing tailored messages that address parental concerns about human papillomavirus (HPV), improve HPV vaccination intent among mothers. | 259 (general video); 249 (top concern video); 237 (al concerns videos) | Methods: Mothers (HPV vaccine hesitant) of 11 to 12 years children. Groups: (1) “control” (only the bundled recommendation video); (2) “top concern” (control video plus a top concern video); or (3) “all concerns” (control video plus videos addressing all concerns). Results: The mean intent to vaccinate postintervention ranged from 3.5 (control)–4.2 (all-concerns group) (p = 0.01). The mean strength of the concerns declined pre- to postintervention by 0.1 in control group to 0.7 in all concern’s group (p < 0.001). The main concerns of hesitant mothers remained high in postintervention. | Tailored messages addressing all concerns improved HPV vaccination intention and reduced the strength of the main concerns of vaccine hesitant mothers. |
| 14. (Dempsey et al., 2019) [35] USA PubMed | To evaluate the impact of a provider communication intervention on improving adolescent HPV vaccination. | 777 parents of adolescents | Methods: Eight control and 8 intervention clinics. Intervention: provider communication aiming at improving adolescent HPV vaccination. Results: A ‘very strong’ recommendation about HPV vaccination produced a greater perceived urgency for getting vaccinated, greater trust in the received information, decreased vaccine hesitancy, and increased vaccine receipt. Similar findings were found for presumptive recommendations. | A provider very strong HPV vaccine recommendation or presumptive recommendation were related to improved parent attitudes and acceptance of this vaccine. |
| 15. (Kornides et al., 2019) [36] USA Cochrane Library | To evaluate if a presumptive, bundled recommendation with tailored message addressing one vs. all parental concerns improves HPV vaccination intent among mothers of girls versus boys. | 762 | Methods: Mothers who have no intention of getting vaccinated their child (11–14year-old) against HPV (27 states). Groups: a) presumptive, bundled recommendation video (“control”); b) control + video addressing the top concern; or c) control + ≥1 video addressing all concerns. Outcome (mean): HPV vaccination intent (1 = extremely unlikely and 10 = extremely likely). Results: the mean intent to vaccinate between the intervention group (all concerns) and control was statistically significant (mothers of boys post intervention) and the mean intent to vaccinate between both intervention groups (top concern or all concerns) and control was statistically significant (mother of girls post intervention). | Tailored messages addressing all concerns positively improved mother’s (boys and girls) vaccination intent. Videos addressing top concerns improved mothers´ intention of vaccinate against HPV their daughters. |
| 16. (Reno et al., 2018) [37] USA PubMed | To analyze the impact of motivational interviews on HPV vaccination rates. | 46 providers | Methods: Eight intervention and control clinics. Intervention: health professionals (e.g., nurse practitioners or physician assistants) conducted motivational interviews. Results: vaccination rates were better in intervention than control. | Motivational interviews played a central role in improving HPV vaccine acceptance. |
| 17. (Henrikson et al., 2018) [38] USA PubMed | To evaluate the impact of health system-based outreach and reminders on HPV vaccine series initiation and completion. | 1805 parents of 10–12 year children. | Methods: Groups: (1) first an outreach letter and brochure recommending HPV vaccination was offered followed by automated HPV vaccine reminders (intervention) or (2) usual care (control). Results: HPV vaccine initiation was higher in the intervention than control at 120 days after randomization (23.6% and 18.8%, p = 0.04) and at study completion (10.3% vs 6.8%, p = 0.04). | Written information and reminders are likely to improve HPV vaccination of 10–12-year children. |
| 18. (O’Leary et al., 2017) [39] USA Cochrane Library | To evaluate the impact of a communication intervention on adolescent HPV vaccine uptake. | 188 medical providers and 43,132 adolescents (11–17 years old) | Methods: Control vs. a five-component intervention (1) HPV fact library, (2) an education website, (3) HPV-related images, (4) a decision aid on HPV vaccine, and (5) 2 h of in-person communication training on using a presumptive vaccine recommendation followed by a motivational interview for vaccine hesitant parents. Outcome: Differences between control and intervention practices at initiation (≥1 dose), and completion (≥3 doses). Results: the intervention group registered a significantly higher odds of HPV series initiation (≥1 dose) and completion (≥3 doses) over time than control. | The 5-components intervention significantly improved HPV vaccine series initiation and completion among adolescents. |
| 19. (Baxter et al., 2017) [12] USA PubMed | To examine the relationship between preschool vaccine history, parent and preadolescent needle fear, and subsequent compliance with optional vaccines. | 120 preadolescents | Methods: quantification of needle anxiety: parents and 10–12-year-old preadolescents (100 mm visual analogue scale). Collected information: needle anxiety (previous vaccination), number of vaccinations between the ages of four and six years (total and same day), and subsequent initiation of HPV vaccine. Results: 12.5% (15) of parents reported anxiety about vaccination. Parent and child anxiety were weakly correlated (r = 0.15). Eight children (26.67%) in the upper fear quartile began their HPV series compared to 14 (48.28%) in the lower quartile (OR 2.57, p = 0.0889, 95% CI 0.864–7.621). | Preadolescent fear of needles was a stronger predictor of non-compliance with HPV vaccine than parent vaccine anxiety. Same-day preschool injections (between 4–6 years) increased the chance of a child show fear of needles five years later. |
| Vaccination against a specific disease: influenza vaccination | ||||
| 20. (Nekrasova et al., 2020) [10] USA Cochrane Library | To assess vaccine hesitancy, knowledge, attitudes, and beliefs among caregivers of children who received the first of two doses of flu vaccine. | 256 participants | Methods: 36 primary care practices (24 states). A reminder (text-message) of the second dose of influenza vaccine was send. Intervention: telephone survey to collect demographic information; the Parent Attitudes About Childhood Vaccines Survey Tool was administered and caregivers were questioned about influenza vaccine and disease. Results: 11.7% of caregivers were moderate/high vaccine hesitant. Many participants manifested misperceptions about influenza and flu vaccine. | Some caregivers may remain vaccine hesitant or maintain inaccurate influenza beliefs even after the administration of the first dose of flu vaccine. |
| 21. (Giese et al., 2020) [40] Bon, Germany | To tests how groups of individuals with positive and negative attitudes towards flu vaccination attend to and convey information online. | 208 (negative) and 221 (positive attitudes towards flu vaccination) | Methods: Three links were tested. Outcomes: (i) what type of information about flu vaccination was conveyed to the subsequent link, (ii) how subjects´ perceptions about flu-vaccination were altered by incoming messages, and (iii) how participants perceived incoming information. Results: (i) participants selectively conveyed attitude-consistent information, (ii) participants were reluctant to alter their perceptions about flu-vaccination in response to messages, and (iii) participants consistently evaluated the incoming information in line with their prior attitudes. | Online messages were not enough relevant to change participant’s perceptions and attitudes towards flu vaccination. |
| 22. (Real et al., 2017) [41] USA PubMed | To evaluate the impact of physician-patient communication on parent’s refusal of influenza vaccination (children aged 6 to 59 months). | 45 Residents | Methods: intervention (n = 24 residents) and control (n = 21 residents). Intervention: Three virtual reality simulations. Residents were required to instruct avatars expressing vaccine hesitancy. Outcome: impact of the curriculum on refusal rates of influenza vaccine between the intervention and control groups (3 months after the virtual reality curriculum). Results: the refusal of influenza vaccine in intervention was lower than control (27.8% vs 37.1%; p = 0.03) (post curriculum period). | A virtual reality curriculum may be an effective tool for the training of medical residents (communication skills). |
| Vaccination against a specific disease: diphtheria tetanus toxoid and pertussis3 | ||||
| 23. (O’Leary et al., 2019) [42] USA Cochrane Library | To evaluate the impact of an online vaccine resource on the uptake of the vaccines against tetanus, diphtheria, and acellular pertussis (Tdap) and influenza vaccines among pregnant women. | 289 (influenza) and 173 (Tdap) pregnant women | Methods: Groups: (i) a website with vaccine information and interactive social media components (VSM), (ii) a website with vaccine information only (VI), or (iii) usual care only (UC). Outcomes: vaccination rates (Tdap and influenza). Results: influenza vaccine uptake was significantly higher in both intervention arms (57% VSM and 55% VI) than the usual care (36%). Tdap: statistically significant differences between arms (71% VSM, 69% VI, and 68% UC) were not found. | Web-based vaccination information may positively influence influenza vaccine uptake, among pregnant women. |
| 24. (Nagar et al. 2018) [43] USA and India PubMed | To compare the timely DTP3 (diphtheria tetanus toxoid and pertussis3) adherence amongst three study arms and to compare mothers’ survey responses about field communication. | 198 mothers | Methods: 96 village health camps in India. Arms: (i) Near Field Communication (NFC) sticker (control group), (ii) NFC necklace, and (iii) NFC necklace with voice call reminder (local dialect). Outcomes: to compare the timely DTP3 adherence amongst all three study arms (primary outcome) and to compare mother’s survey responses about symbolic necklaces (secondary outcome: field communication). Results: NFC necklace and the necklace plus voice call reminders (local dialect) not directly promoted an increase in infant DTP3 timeliness immunization (primary outcome). The provision of a necklace generated a significant community discussion (p = 0.0118), a strong satisfaction (p < 0.0001) and an increased visibility within families (p < 0.00001) (secondary outcome). | Symbolic necklaces may constitute an assistive tool in immunization campaigns. |
| Vaccination against a specific disease: COVID-2019 | ||||
| 25. (Bogart et al., 2020) [44] USA and Canada PubMed | To examine associations between medical mistrust on COVID-2019 vaccine and treatment and patients´ adherence to antiretroviral therapy (ART). | 101 HIV-positive Black Americans | Methods: a telephone interview to evaluate: COVID-2019 mistrust), COVID-2019 vaccine and treatment hesitancy, and trust in information about COVID-2019. Patient’s adherence to antiretroviral therapy was quantified. Results: over half of the participants manifested at least one COVID-2019 vaccine or treatment hesitancy belief. A lower antiretroviral therapy adherence was related to more negative COVID-2019 behaviors (p = 0.02). | Tailored strategies should be implemented to promote COVID-2019 vaccination and treatment, to overcome mistrust and to prevent health inequalities in less favored communities. |
| Miscellaneous: extrinsic factors | ||||
| 26. (Xu et al., 2020) [45] USA Cochrane Library | To evaluate if messages from a governmental source improve perceived source credibility, increment parent intentions to vaccinate their children, and/or reduce vaccine hesitancy. | 1000 (t1) and 800 (t2) | Methods: Tailored messages were sent by the Centers for Disease Control and Prevention to convey the expertise, trustworthiness, or caring/goodwill. Study hypothesis: to evaluate if the tailored messages improve perceived source credibility, increment parent intentions to vaccinate their children, and/or reduce vaccine hesitancy. Results: Overall, study hypothesis were not demonstrated, although some relevant findings have emerged from this study. | Tailored messages to communicate source expertise produced greater perceived caring/goodwill among parents who were vaccine hesitant at baseline. |
| 27. (Domec et al., 2018) [46] Guatemala and USA PubMed | To identify and compare parents´ vaccine hesitancy in rural and urban Guatemala. | 720 | Methods: Clinics (rural and urban Guatemala). Parents of infants (6 weeks to 6 months) completed a questionnaire on vaccine hesitancy (Likert scale). Results: 40.8% think “most parents like them have their children vaccinated with all the recommended vaccines”. Participants had difficulty in understanding and using the Likert scale. Factor analysis showed a two-factor structure within the vaccine hesitancy Likert scale. | A significant proportion of vaccine hesitant parents was identified, with these parents constituting a very heterogeneous group. Thus, the development of a survey tool to identify vaccine hesitant parents was complex. |
| 28. (Karimah et al., 2017) [47] Malaysia Cochrane Library | To identify variables with influence on vaccine hesitance among parents from Kuantan, Pahang. | 155 parents | Methods: administration of a questionnaire. Results: in the logistic regression analysis, parents’ beliefs and attitude about health and prevention and/or the role of healthcare professional were significantly associated with vaccine hesitancy. The most explanatory variables of vaccine hesitancy: post vaccination experience (95.5%); vaccination schedule (60.5%), role of healthcare professional, awareness (56.1%) and risks and benefits of vaccination (51.6%). | The role of healthcare professionals and parent’s beliefs and attitudes about health may negatively impact vaccine hesitancy. |
| 29. (Betsch and Böhm, 2016) [48] Germany PubMed | To assess the effect of partial compulsory vaccination on the subsequent uptake of other voluntary vaccines. | 297 | Methods: Two sequential vaccination decisions were simulated (online experiment). Groups: (i) compulsory vaccination (n = 144) (intervention) and (ii) voluntary vaccination (n = 153) (control). Voluntary vaccination was the second decision for both groups. Results: The second voluntary vaccination was reduced by 39% in the intervention group. | Compulsory vaccination may negatively impact vaccination rates. |
| Educational Strategies | ||||
| 30. (Pahud et al., 2020) [13] USA PubMed | To develop and evaluate an online curriculum on vaccine education for pediatrics and family medicine residents. | 1444 residents (734 intervention, 710 control). | Methods: Four online modules and an in-person training guide (intervention). Standard vaccine education (control sites). Pre-intervention and post-intervention surveys were emailed to residents (both groups). Primary outcomes: “Vaccine knowledge,” “vaccine attitudes/hesitancy,” and “self-confidence”. Results: Intervention residents (online curriculum) showed greater self-confidence and ability to discuss vaccines with parents/patients than control (p < 0.03). Vaccine hesitancy was higher for family medicine residents (23%) than pediatric residents (10%). | The developed online curriculum seems to be an effective model of immunization education for residents. |
| 31. (Norton et al., 2019) [49] USA Cochrane Library | To evaluate if the residents attending a curriculum on vaccine hesitancy demonstrate improved knowledge, comfort, and skills. | 70 residents | Methods: Control and intervention (35 residents). Curriculum design framework: didactic sessions per pediatric vaccine and interactive role-playing sessions on communication skills. Residents of both groups were required to assess a standardized patient (pre and posttests). Results: Pretests scores were not statistically significant different between both groups. The standardized patient was better scored in intervention than control (78% vs. 52%, p = 0.00). Post curriculum: statistically significant better scores were found for residents´ knowledge (47–66%) and comfort level (2.9/5–3.76/5) in intervention than control. | The developed curriculum produced improvements on resident’s vaccine knowledge, communication skills and comfort level |
| 32. (Gagneur et al., 2019) [50] Quebec, Canada, PubMed | To assess vaccination intention and vaccine hesitancy among parents who received an individual motivational interview on infant immunization during post-partum stay at a maternity ward. | 1223 parents | Methods: Post-partum stay at a maternity ward. Intervention: motivational interview (pre/post-intervention in four maternities). Parents filled pre- and post-intervention questionnaire on vaccine intention and vaccine hesitancy. Results: Parents´ vaccine intention increased by 12% (78% vs 90%, p < 0.0001), and parents´ vaccine hesitancy reduced by 40% (27% vs 16%; p < 0.0001) post-intervention. | A parents’ motivational interview on immunization produced positive outputs: a lower vaccine hesitancy and a greater intention to vaccinate their infant at 2 months of age. |
| 33. (Gagneur et al., 2018) [51] Quebec, Canada, PubMed | To assess the impact of an educational strategy about vaccination promotion, among parents who delivered at the maternity ward. | Parents of 1140 (intervention) and 1249 newborns (control) | Methods: An individual educational information session about immunization was administered at maternity ward (intervention). Control: usual care. Results: vaccine coverage significantly increased in intervention than control (p < 0.05): 3.2, 4.9, and 7.3%, respectively at 3, 5, and 7 months. | Motivational interviews may constitute effective tools to overcome parents´ vaccine hesitancy. |
| 34. (Fisher et al., 2018) [52] Ontario & Quebec, Canada Cochrane Library | To evaluate the impact of an Information—Motivation—Behavioral Skills model (IMB)-based, accredited, online Continuing Medical Education (CME) program on seasonal influenza vaccination. | 68 healthcare professionals | Methods: 33 healthcare professionals in CME/intervention (292 visits) and 35 healthcare professionals in control (336 visits). Children 6–23 months. Intervention: the CME comprised information/training about tailored health behavior. Results: parents in the CME group were around ~30% more likely to agree to immunize their child with influenza vaccine than parents in control (p = 0.007). | Medical education programs may contribute to a better influenza immunization of children. |
| 35. (Henrikson et al., 2015) [53] USA PubMed | To test a communication intervention, which was designed to reduce mother’s vaccine hesitancy and to increase physician confidence in communicating about vaccines. | 347 mothers | Methods: 30 mothers (intervention) and 26 mothers (control) (56 clinics). Intervention: physicians received a targeted communication training. Mothers and physicians were evaluated at baseline and 6 months. Vaccine hesitancy was quantified with the Parental Attitudes on Childhood Vaccines score. Results: Both maternal vaccine hesitancy and physician self-efficacy in communicating about vaccines with parents were not improved by the communication training. | The communication intervention not produced positive outcomes. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pires, C. What Is the State-of-the-Art in Clinical Trials on Vaccine Hesitancy 2015–2020? Vaccines 2021, 9, 348. https://doi.org/10.3390/vaccines9040348
Pires C. What Is the State-of-the-Art in Clinical Trials on Vaccine Hesitancy 2015–2020? Vaccines. 2021; 9(4):348. https://doi.org/10.3390/vaccines9040348
Chicago/Turabian StylePires, Carla. 2021. "What Is the State-of-the-Art in Clinical Trials on Vaccine Hesitancy 2015–2020?" Vaccines 9, no. 4: 348. https://doi.org/10.3390/vaccines9040348
APA StylePires, C. (2021). What Is the State-of-the-Art in Clinical Trials on Vaccine Hesitancy 2015–2020? Vaccines, 9(4), 348. https://doi.org/10.3390/vaccines9040348