
Willingness of Taiwan’s Healthcare Workers and Outpatients to Vaccinate against COVID-19 during a Period without Community Outbreaks

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Recruitment Procedure
2.2. Measures
2.2.1. Background Information Sheet
2.2.2. Willingness to Receive Vaccination
2.2.3. Willingness to Take Rapid Test
2.2.4. Risk Perception
2.2.5. Fear of COVID-19
2.2.6. Preventive COVID-19 Infection Behaviors
2.2.7. Willingness to Care for Patients
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). World Health Organization Coronavirus Disease (COVID-19). 2020. Available online: https://covid19.who.int (accessed on 4 March 2021).
- Madabhavi, I.; Sarkar, M.; Kadakol, N. COVID-19: A review. Monaldi Arch. Chest Dis. 2020, 90. [Google Scholar] [CrossRef]
- Weiss, P.; Murdoch, D.R. Clinical course and mortality risk of severe COVID-19. Lancet 2020, 395, 1014–1015. [Google Scholar] [CrossRef]
- Pramukti, I.; Strong, C.; Sitthimongkol, Y.; Setiawan, A.; Pandin, M.G.R.; Yen, C.-F.; Lin, C.-Y.; Griffiths, M.D.; Ko, N.-Y. Anxiety and Suicidal Thoughts During the COVID-19 Pandemic: Cross-Country Comparative Study Among Indonesian, Taiwanese, and Thai University Students. J. Med. Internet Res. 2020, 22, e24487. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-Y.; Chen, I.-H.; O’Brien, K.S.; Latner, J.D.; Lin, C.-Y. Psychological distress and internet-related behaviors between schoolchildren with and without overweight during the COVID-19 outbreak. Int. J. Obes. 2021, 45, 677–686. [Google Scholar] [CrossRef]
- Fazeli, S.; Zeidi, I.M.; Lin, C.-Y.; Namdar, P.; Griffiths, M.D.; Ahorsu, D.K.; Pakpour, A.H. Depression, anxiety, and stress mediate the associations between internet gaming disorder, insomnia, and quality of life during the COVID-19 outbreak. Addict. Behav. Rep. 2020, 12, 100307. [Google Scholar] [CrossRef]
- Nathiya, D.; Singh, P.; Suman, S.; Raj, P.; Tomar, B.S. Mental health problems and impact on youth minds during the COVID-19 outbreak: Cross-sectional (RED-COVID) survey. Soc. Health Behav. 2020, 3, 83–88. [Google Scholar]
- Chang, K.-C.; Hou, W.-L.; Pakpour, A.H.; Lin, C.-Y.; Griffiths, M.D. Psychometric testing of three COVID-19-related scales among people with mental illness. Int. J. Ment. Health Addict. 2020, 1–13. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The fear of COVID-19 scale: Development and initial validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef]
- Chen, I.-H.; Chen, C.-Y.; Pakpour, A.H.; Griffiths, M.D.; Lin, C.-Y. Internet-related behaviors and psychological distress among schoolchildren during COVID-19 school suspension. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, S.R.; Shrivastava, P.S. Roping-In religious leaders and faith experts in the effective containment of the coronavirus disease-2019 pandemic. Soc. Health Behav. 2020, 3, 130–131. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.-Y.; Pakpour, A.H. The Association Between Health Status and Insomnia, Mental Health, and Preventive Behaviors: The Mediating Role of Fear of COVID-19. Gerontol. Geriatr. Med. 2020, 6, 2333721420966081. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.-C.; Strong, C.; Pakpour, A.H.; Griffiths, M.D.; Lin, C.-Y. Factors related to preventive COVID-19 infection behaviors among people with mental illness. J. Formos. Med. Assoc. 2020, 119, 1772–1780. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.W.; Cheng, Y. Policy actions to alleviate psychosocial impacts of COVID-19 pandemic: Experiences from Taiwan. Soc. Health Behav. 2020, 3, 72–73. [Google Scholar] [CrossRef]
- Winter, T.; Riordan, B.; Pakpour, A.; Griffiths, M.; Mason, A.; Poulgrain, J.; Damian, S. Evaluation of the English version of the Fear of COVID-19 Scale and its relationship with behavior change and political beliefs. Int. J. Ment. Health Addict. 2020, 1–11. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Imani, V.; Lin, C.-Y.; Timpka, T.; Broström, A.; Updegraff, J.A.; Årestedt, K.; Griffiths, M.D.; Pakpour, A.H. Associations between fear of COVID-19, mental health, and preventive behaviours across pregnant women and husbands: An actor-partner interdependence modelling. Int. J. Ment. Health Addict. 2020, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Mamun, M.A.; Sakib, N.; Gozal, D.; Bhuiyan, A.I.; Hossain, S.; Bodrud-Doza, M.; Al Mamun, F.; Hosen, I.; Safiq, M.B.; Abdullah, A.H. The COVID-19 pandemic and serious psychological consequences in Bangladesh: A population-based nationwide study. J. Affect. Disord. 2020, 279, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Imani, V.; Majd, N.R.; Ghasemi, Z.; Griffiths, M.D.; Hamilton, K.; Hagger, M.S.; Pakpour, A.H. Using an integrated social cognition model to predict COVID-19 preventive behaviours. Br. J. Health Psychol. 2020, 25, 981–1005. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-Y.; Chen, I.-H.; Pakpour, A.H.; Lin, C.-Y.; Griffiths, M.D. Internet-related behaviors and psychological distress among schoolchildren during the COVID-19 school hiatus. Cyberpsychol. Behav. Soc. Netw. 2021. [Google Scholar] [CrossRef]
- Chen, I.-H.; Chen, C.-Y.; Pakpour, A.H.; Griffiths, M.D.; Lin, C.-Y.; Li, X.-D.; Tsang, H.W.H. Problematic internet-related behaviors mediate the associations between levels of internet engagement and distress among schoolchildren during COVID-19 lockdown: A longitudinal structural equation modeling study. J. Behav. Addict. 2021, 1–14. [Google Scholar] [CrossRef]
- European Society for Child and Adolescent Psychiatry. Concerns for the Mental Health of Children and Adolescents during the Coronavirus Pandemic. 2020. Available online: https://www.escap.eu/index/coronavirus-and-mental-health/ (accessed on 4 March 2021).
- Mamun, M.A.; Ullah, I. COVID-19 suicides in Pakistan, dying off not COVID-19 fear but poverty? The forthcoming economic challenges for a developing country. Brain Behav. Immunity 2020, 87, 163–166. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Kabamba Nzaji, M.; Kabamba Ngombe, L.; Ngoie Mwamba, G.; Banza Ndala, D.B.; Mbidi Miema, J.; Luhata Lungoyo, C.; Lora Mwimba, B.; Cikomola Mwana Bene, A.; Mukamba Musenga, E. Acceptability of Vaccination Against COVID-19 among Healthcare Workers in the Democratic Republic of the Congo. Pragmatic Obs. Res. 2020, 11, 103. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.-K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef] [PubMed]
- Akarsu, B.; Canbay Özdemir, D.; Ayhan Baser, D.; Aksoy, H.; Fidancı, İ.; Cankurtaran, M. While studies on COVID-19 vaccine is ongoing, the public’s thoughts and attitudes to the future COVID-19 vaccine. Int. J. Clin. Pract. 2020, e13891. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Reuben, R.C.; Danladi, M.M.; Saleh, D.A.; Ejembi, P.E. Knowledge, attitudes and practices towards COVID-19: An epidemiological survey in North-Central Nigeria. J. Community Health 2020, 1–14. [Google Scholar] [CrossRef]
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing Covid-19 vaccines at pandemic speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- World Health Organization (WHO). World Health Organization DRAFT Landscape of COVID-19 Candidate Vaccines—14 July 2020. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 14 July 2020).
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Vo, T.Q. Willingness-to-pay for a COVID-19 vaccine and its associated determinants in Indonesia. Hum. Vaccines Immunother. 2020, 16, 3074–3080. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to receive vaccination against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would receive vaccination? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.-F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 1–15. [Google Scholar] [CrossRef]
- La Vecchia, C.; Negri, E.; Alicandro, G.; Scarpino, V. Attitudes towards influenza vaccine and a potential COVID-19 vaccine in Italy and differences across occupational groups. La Med. Del. Lav. 2020, 111, 445–448. [Google Scholar] [CrossRef]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 vaccine hesitancy among medical students. J. Public Health 2020. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of US adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Grech, V.; Bonnici, J.; Zammit, D. Vaccine hesitancy in Maltese family physicians and their trainees vis-a-vis influenza and novel COVID-19 vaccination. Early Hum. Dev. 2020, 105259. [Google Scholar] [CrossRef]
- Goldman, R.D.; Yan, T.D.; Seiler, M.; Cotanda, C.P.; Brown, J.C.; Klein, E.J.; Hoeffe, J.; Gelernter, R.; Hall, J.E.; Davis, A.L. Caregiver willingness to vaccinate their children against COVID-19: Cross sectional survey. Vaccine 2020, 38, 7668–7673. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Pogue, K.; Jensen, J.L.; Stancil, C.K.; Ferguson, D.G.; Hughes, S.J.; Mello, E.J.; Burgess, R.; Berges, B.K.; Quaye, A.; Poole, B.D. Influences on attitudes regarding potential COVID-19 vaccination in the United States. Vaccines 2020, 8, 582. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef] [PubMed]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Prati, G. Intention to receive a vaccine against SARS-CoV-2 in Italy and its association with trust, worry and beliefs about the origin of the virus. Health Educ. Res. 2020, 35, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.C.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.Q.; Zhou, X.; Wang, Z. Parental Acceptability of COVID-19 Vaccination for Children Under the Age of 18 Years: Cross-Sectional Online Survey. JMIR Pediatr. Parent. 2020, 3, e24827. [Google Scholar] [CrossRef] [PubMed]
- Daly, M.; Robinson, E. Willingness to vaccinate against COVID-19 in the US: Longitudinal evidence from a nationally representative sample of adults from April-October 2020. medRxiv 2020. [Google Scholar] [CrossRef]
- Taiwan Centers for Disease Control. Coronavirus Disease 2019 (COVID-19). 2021. Available online: https://www.cdc.gov.tw/en/Disease/SubIndex/ (accessed on 26 January 2021).
- Tubiana, S.; Launay, O.; Galtier, F.; Tattevin, P.; Postil, D.; Vanhems, P.; Lenzi, N.; Verger, P.; Duval, X. Attitudes, knowledge, and willingness to be vaccinated against seasonal influenza among patients hospitalized with influenza-like-illness: Impact of diagnostic testing. Hum. Vaccines Immunother. 2020, 16, 851–857. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Healthcare Workers (N = 500) | General Population (N = 238) |
|---|---|---|
| Age (years); Mean (SD) | 32.96 (7.99) | 34.43 (10.02) |
| Sex (Male); n (%) | 40 (8.0) | 79 (33.2) |
| Educational level (Senior high and below); n (%) | 17 (3.4) | 41 (17.2) |
| Fear of COVID-19; Mean (SD) a | 2.57 (0.82) | 2.56 (0.96) |
| Risk perception; Mean (SD) a | 2.73 (0.93) | 2.21 (0.87) |
| Willingness to take rapid test; n (%) | 118 (23.6) | 68 (28.6) |
| Willingness to receive vaccination; n (%) | 117 (23.4) | 73 (30.7) |
| Preventive behaviors; Mean (SD) a | 3.22 (0.51) | 3.05 (0.68) |
| Willingness to care patients; Mean (SD) b | 6.07 (2.59) | -- |
| Independent Variable | COR (95% CI) | AOR (95% CI) |
|---|---|---|
| Healthcare workers (N = 500) | ||
| Age | 0.99 (0.96, 1.02) | 0.98 (0.95, 1.01) |
| Gender (Ref: female) | 1.64 (0.82, 3.29) | 2.53 (1.14, 5.65) |
| Fear of COVID-19 | 1.10 (0.85, 1.41) | 1.04 (0.76, 1.41) |
| Risk perception | 1.29 (1.03, 1.63) | 1.16 (0.89, 1.52) |
| Willingness to take rapid test (Ref: No) | 9.24 (5.76, 14.83) | 9.06 (5.49, 14.94) |
| Preventive behaviors | 2.32 (1.52, 3.56) | 1.89 (1.15, 3.10) |
| Willingness to care patients | 1.08 (0.996, 1.17) | 1.04 (0.94, 1.15) |
| Outpatient population (N = 238) | ||
| Age | 0.99 (0.96, 1.01) | 0.99 (0.96, 1.02) |
| Gender (Ref: male) | 1.17 (0.66, 2.09) | 1.15 (0.58, 2.27) |
| Fear of COVID-19 | 1.03 (0.99, 1.07) | 0.99 (0.94, 1.04) |
| Risk perception | 1.35 (0.98, 1.87) | 1.22 (0.84, 1.78) |
| Willingness to take rapid test (Ref: No) | 8.91 (4.71, 16.87) | 8.24 (4.24, 16.02) |
| Preventive behaviors | 1.69 (1.09, 2.60) | 1.27 (0.76, 2.12) |
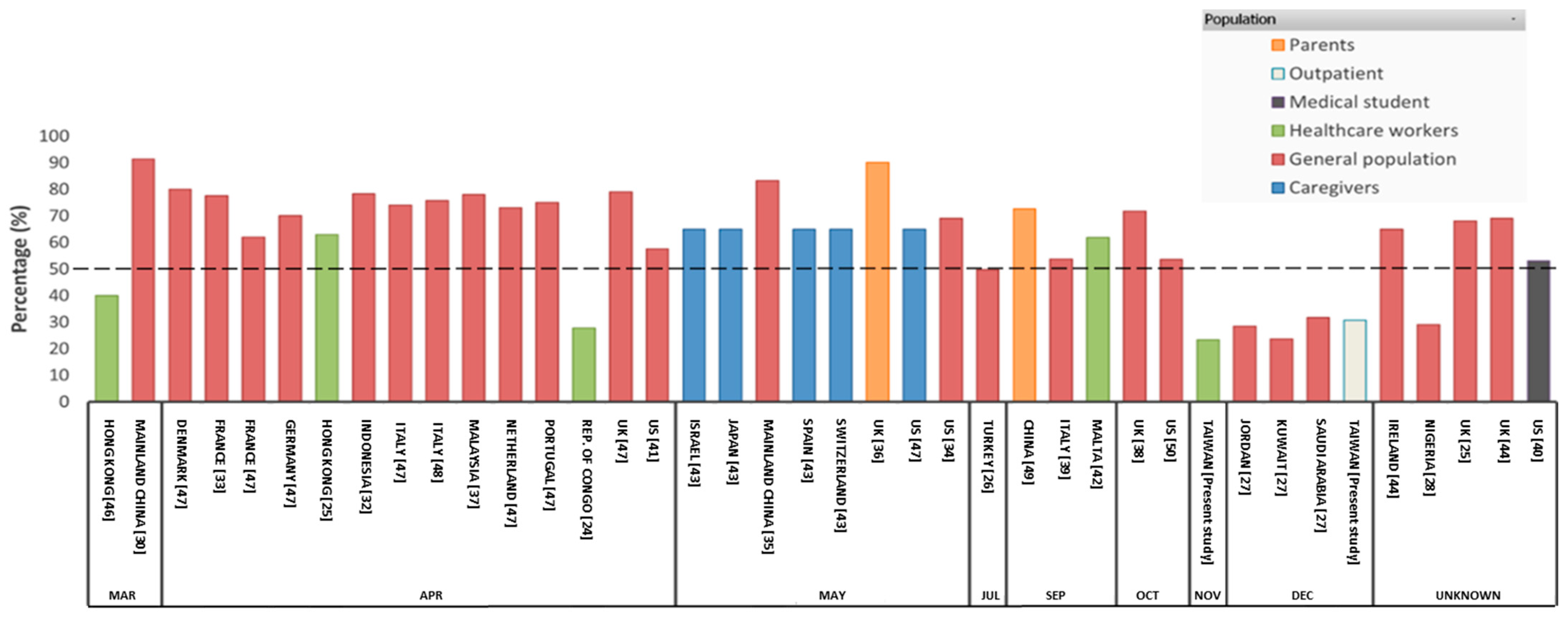
| Country/Region (Author, Year) | Population | Cases | Deaths | Population | Willingness (%) | Survey Period (2020) |
|---|---|---|---|---|---|---|
| Hong Kong [46] | Healthcare workers | 715 | 4 | 7.45 million | 40.00 | 26 February to March31 |
| Mainland China [30] | General population | 80,026 | 2912 | 1.39 billion | 91.30 | 1 February to March30 |
| Republic of Congo [24] | Healthcare workers | 220 | 9 | 5.5 million | 27.70 | 1 March to 30 April |
| Hong Kong [25] | Healthcare workers | 1038 | 4 | 7.45 million | 63.00 | 15 March to 30 April |
| Indonesia [32] | General population | 2092 | 191 | 273.5 million | 78.30 | 25 March to 6 April |
| France [33] | General population | 114,657 | 20,246 | 65.2 million | 77.60 | 26 March to 20 April |
| Italy [48] | General population | 110,559 | 13,195 | 60.3 million | 75.80 | 1 April |
| U.S. [41] | General population | 818,510 | 43,685 | 331.0 million | 57.60 | 16 April to 20 April |
| Denmark [47] | General population | 6681 | 309 | 5.8 million | 80.00 | 2 April to 15 April |
| France [47] | General population | 106,206 | 17,152 | 67.0 million | 62.00 | 2 April to 15 April |
| Germany [47] | General population | 134,753 | 3804 | 83.0 million | 70.00 | 2 April to 15 April |
| Netherland [47] | General population | 28,153 | 3134 | 17.28 million | 73.00 | 2 April to 15 April |
| Portugal [47] | General population | 20,593 | 599 | 10.2 million | 75.00 | 2 April to 15 April |
| U.K. [47] | General population | 89,217 | 14,903 | 67.8 million | 79.00 | 2 April to 15 April |
| Italy [47] | General population | 162,479 | 21,131 | 60.3 million | 74.00 | 2 April to 15 April |
| Malaysia [37] | General population | 4683 | 76 | 32.3 million | 78.00 | 3 April to 12 April |
| U.S. [43] | Caregivers | 1,877,168 | 109,099 | 331.0 million | 65.00 | 26 March to 31 May |
| Israel [43] | Caregivers | 17071 | 285 | 9.05 million | 65.00 | 26 March to 31 May |
| Japan [43] | Caregivers | 16,851 | 891 | 126.3 million | 65.00 | 26 March to 31 May |
| Spain [43] | Caregivers | 251,913 | 29,050 | 46.9 million | 65.00 | 26 March to 31 May |
| Switzerland [43] | Caregivers | 30,862 | 1831 | 8.5 million | 65.00 | 26 March to 31 May |
| U.K. [36] | Parents | 202,085 | 31,571 | 67.8 million | 90.10 | 19 April to 11 May |
| U.S. [34] | General population | 1,877,168 | 109,099 | 331.0 million | 69.00 | 1 May to 31 May |
| Mainland China [35] | General population | 82,960 | 4634 | 1.39 billion | 83.30 | 1 May to 19 May |
| Turkey [26] | General population | 470,666 | 5323 | 84.3 million | 49.70 | 10 June to 10 July |
| China [49] | Parents | 85,134 | 4634 | 1.39 billion | 72.60 | 1 September to 7 September |
| Italy [39] | General population | 311,363 | 35,851 | 60.4 million | 53.70 | 16 September to 28 September |
| Malta [42] | Healthcare workers | 3035 | 34 | 4.42 million | 61.80 | 25 September to 29 September |
| U.S. [50] | General population | 7,854,367 | 217,136 | 331.0 million | 53.60 | June-1 to October7 |
| U.K. [38] | General population | 705,427 | 43,579 | 67.8 million | 71.70 | 24 September to 17 October |
| Taiwan (The present study) | Healthcare workers | 611 | 7 | 23.5 million | 23.40 | 24 September to 21 November |
| Taiwan (The present study) | Outpatient | 799 | 7 | 23.5 million | 30.70 | 27 October to 31 December |
| Saudi Arabia [27] | General population | 360,690 | 6101 | 34.27 million | 31.80 | 14 December to 18 December |
| Jordan [27] | General population | 271,514 | 3518 | 10.1 million | 28.40 | 14 December to 18 December |
| Kuwait [27] | General population | 147,531 | 916 | 4.20 million | 23.60 | 14 December to 18 December |
| Nigeria [28] | General population | - | 29.00 | Unknown | ||
| U.S. [40] | Medical students | - | 53.00 | Unknown | ||
| U.K. [44] | General population | - | 69.00 | Unknown | ||
| Ireland [44] | General population | - | 65.00 | Unknown | ||
| U.K. [45] | General population | - | 68.00 | Unknown | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kukreti, S.; Lu, M.-Y.; Lin, Y.-H.; Strong, C.; Lin, C.-Y.; Ko, N.-Y.; Chen, P.-L.; Ko, W.-C. Willingness of Taiwan’s Healthcare Workers and Outpatients to Vaccinate against COVID-19 during a Period without Community Outbreaks. Vaccines 2021, 9, 246. https://doi.org/10.3390/vaccines9030246
Kukreti S, Lu M-Y, Lin Y-H, Strong C, Lin C-Y, Ko N-Y, Chen P-L, Ko W-C. Willingness of Taiwan’s Healthcare Workers and Outpatients to Vaccinate against COVID-19 during a Period without Community Outbreaks. Vaccines. 2021; 9(3):246. https://doi.org/10.3390/vaccines9030246
Chicago/Turabian StyleKukreti, Shikha, Mei-Yun Lu, Yi-Hsuan Lin, Carol Strong, Chung-Ying Lin, Nai-Ying Ko, Po-Lin Chen, and Wen-Chien Ko. 2021. "Willingness of Taiwan’s Healthcare Workers and Outpatients to Vaccinate against COVID-19 during a Period without Community Outbreaks" Vaccines 9, no. 3: 246. https://doi.org/10.3390/vaccines9030246
APA StyleKukreti, S., Lu, M.-Y., Lin, Y.-H., Strong, C., Lin, C.-Y., Ko, N.-Y., Chen, P.-L., & Ko, W.-C. (2021). Willingness of Taiwan’s Healthcare Workers and Outpatients to Vaccinate against COVID-19 during a Period without Community Outbreaks. Vaccines, 9(3), 246. https://doi.org/10.3390/vaccines9030246