
Prevalence and Factors Associated with Parents’ Non-Intention to Vaccinate Their Children and Adolescents against COVID-19 in Latin America and the Caribbean

 , ,
, , 

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
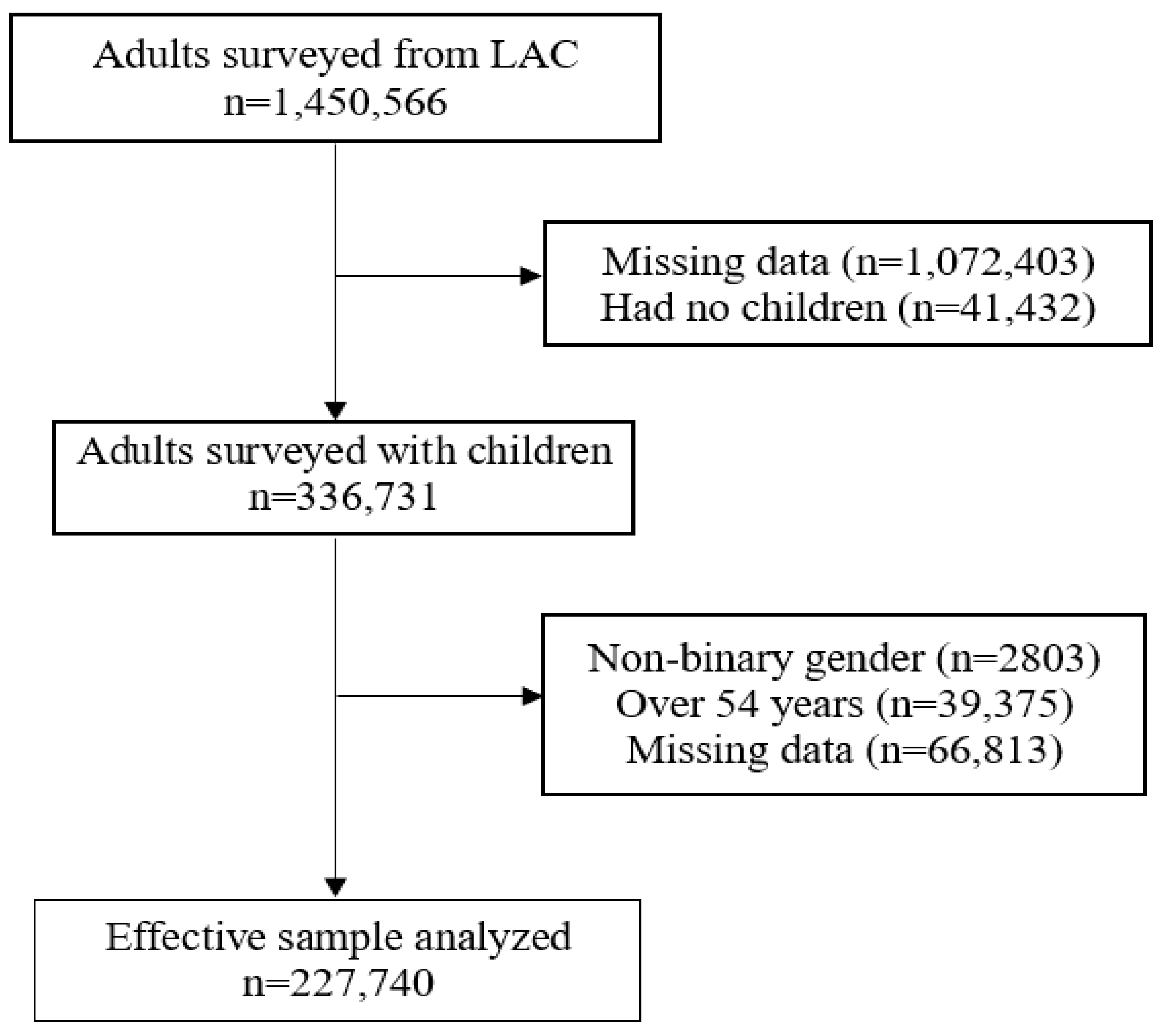
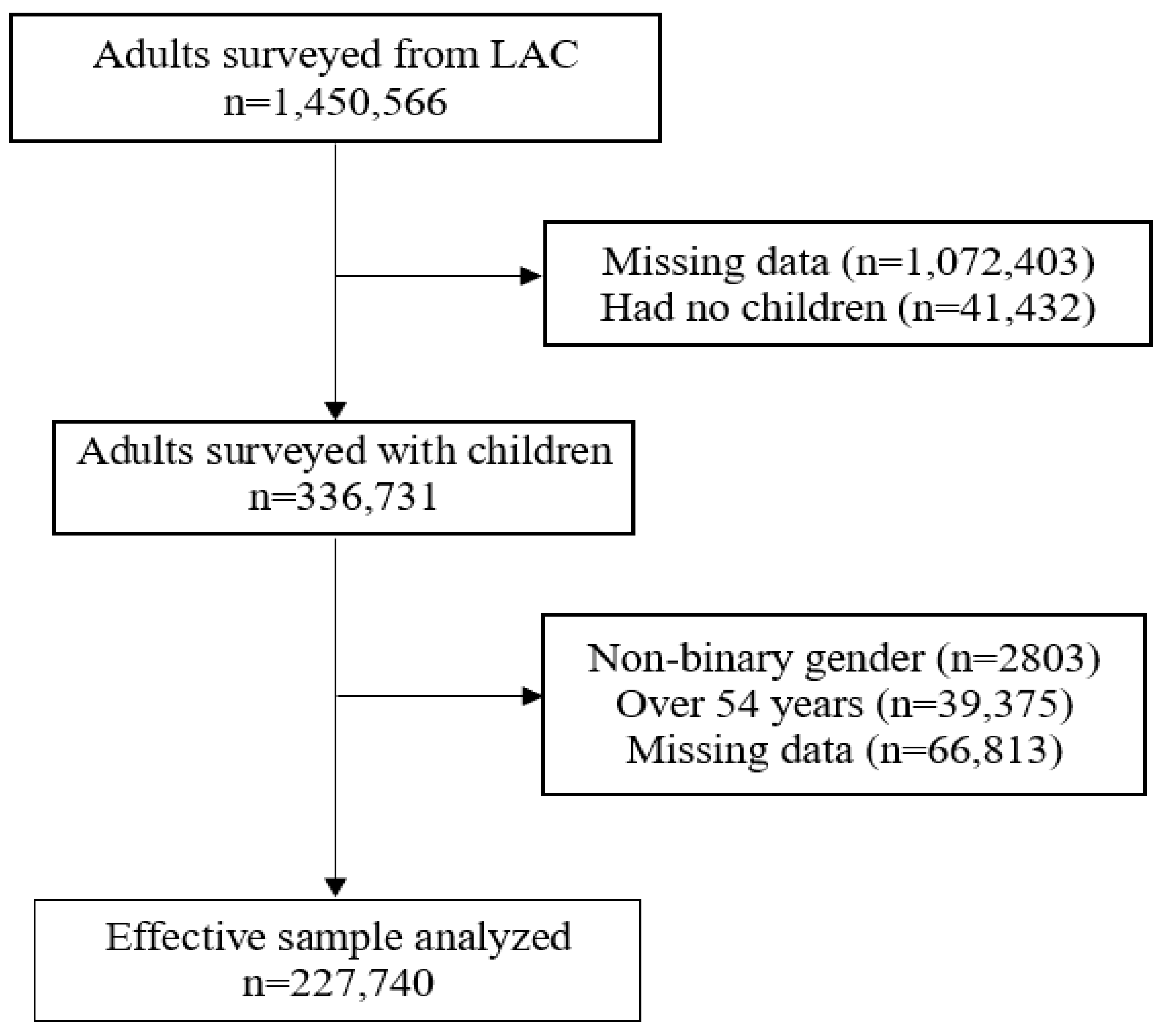
2.2. Population and Sample
2.3. Variables and Measures
2.3.1. Outcome Variable: Parents’ Non-Intention to Vaccinate Their Children and Adolescents against COVID-19
2.3.2. Independent Variables
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Characteristics of the Study Sample
3.2. Bivariate Analysis According to Parents’ Non-Intention to Vaccinate Their Children and Adolescents against COVID-19
3.3. Prevalence of Parents’ Non-Intention to Vaccinate Their Children and Adolescents against COVID-19 According to Each LAC Country
3.4. Factors Associated with Parents’ Non-Intention to Vaccinate Their Children and Adolescents against COVID-19
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 15 August 2021).
- Shah, S. Children and the American Rescue Plan: Countering COVID-19 vaccine hesitancy during a global pandemic. Pediatr. Res. 2021, 90, 237–239. [Google Scholar] [CrossRef]
- Wang, Q.; Yang, L.; Jin, H.; Lin, L. Vaccination against COVID-19: A systematic review and meta-analysis of acceptability and its predictors. Prev. Med. 2021, 150, 106694. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Al-Amer, R.; Maneze, D.; Everett, B.; Montayre, J.; Villarosa, A.R.; Dwekat, E.; Salamonson, Y. COVID-19 vaccination intention in the first year of the pandemic: A systematic review. J. Clin. Nurs. 2021. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, S.A.; Levy, O. Considering Mandatory Vaccination of Children for COVID-19. Pediatrics 2021, 147, 147. [Google Scholar] [CrossRef] [PubMed]
- Leeb, R.T.; Price, S.; Sliwa, S.; Kimball, A.; Szucs, L.; Caruso, E.; Godfred-Cato, S.; Lozier, M. COVID-19 trends among school-aged children—United States, 1 March–19 September 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1410. [Google Scholar] [CrossRef] [PubMed]
- Bhopal, S.S.; Bagaria, J.; Olabi, B.; Bhopal, R. Children and young people remain at low risk of COVID-19 mortality. Lancet Child Adolesc. Health 2021, 5, e12–e13. [Google Scholar] [CrossRef]
- Han, B.; Song, Y.; Li, C.; Yang, W.; Ma, Q.; Jiang, Z.; Li, M.; Lian, X.; Jiao, W.; Wang, L. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy children and adolescents: A double-blind, randomised, controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 803–812. [Google Scholar] [CrossRef]
- ModernaTX, Inc. A Study to Evaluate Safety and Effectiveness of mRNA-1273 COVID-19 Vaccine in Healthy Children between 6 Months of Age and Less Than 12 Years of Age. Available online: https://clinicaltrials.gov/ct2/show/NCT04796896 (accessed on 10 August 2021).
- U.S. Food & Drug Administration. Coronavirus (COVID-19) Update: FDA Authorizes Pfizer-BioNTech COVID-19 Vaccine for Emergency Use in Adolescents in Another Important Action in Fight Against Pandemic. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-pfizer-biontech-covid-19-vaccine-emergency-use (accessed on 10 August 2021).
- European Medicines Agency. First COVID-19 Vaccine Approved for Children Aged 12 to 15 in EU. Available online: https://www.ema.europa.eu/en/news/first-covid-19-vaccine-approved-children-aged-12-15-eu (accessed on 10 August 2021).
- Zimet, G.D.; Silverman, R.D.; Fortenberry, J.D. Coronavirus Disease 2019 and Vaccination of Children and Adolescents: Prospects and Challenges. J. Pediatr. 2021, 231, 254–258. [Google Scholar] [CrossRef]
- World Health Organization. Ten Threats to Global Health in 2019. 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 10 September 2021).
- Skjefte, M.; Ngirbabul, M.; Akeju, O.; Escudero, D.; Hernandez-Diaz, S.; Wyszynski, D.F.; Wu, J.W. COVID-19 vaccine acceptance among pregnant women and mothers of young children: Results of a survey in 16 countries. Eur. J. Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef]
- Zhang, K.C.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.Q.; Zhou, X.; Wang, Z. Parental Acceptability of COVID-19 Vaccination for Children Under the Age of 18 Years: Cross-Sectional Online Survey. JMIR Pediatr. Parent. 2020, 3, e24827. [Google Scholar] [CrossRef] [PubMed]
- Yigit, M.; Ozkaya-Parlakay, A.; Senel, E. Evaluation of COVID-19 Vaccine Refusal in Parents. Pediatr. Infect. Dis. J. 2021, 40, e134–e136. [Google Scholar] [CrossRef]
- Hetherington, E.; Edwards, S.A.; MacDonald, S.E.; Racine, N.; Madigan, S.; McDonald, S.; Tough, S. SARS-CoV-2 vaccination intentions among mothers of children aged 9 to 12 years: A survey of the All Our Families cohort. CMAJ Open 2021, 9, E548. [Google Scholar] [CrossRef]
- Seiler, M.; Goldman, R.D.; Staubli, G.; Hoeffe, J.; Gualco, G.; Manzano, S.; Part of the International COVID-19 Parental Attitude Study (COVIPAS) Group. Parents’ intent to vaccinate against influenza during the COVID-19 pandemic in two regions in Switzerland. Swiss Med. Wkly. 2021, 151, w20508. [Google Scholar] [CrossRef]
- Goldman, R.D.; Yan, T.D.; Seiler, M.; Cotanda, C.P.; Brown, J.C.; Klein, E.J.; Hoeffe, J.; Gelernter, R.; Hall, J.E.; Davis, A.L.; et al. Caregiver willingness to vaccinate their children against COVID-19: Cross sectional survey. Vaccine 2020, 38, 7668–7673. [Google Scholar] [CrossRef] [PubMed]
- Guzman-Holst, A.; DeAntonio, R.; Prado-Cohrs, D.; Juliao, P. Barriers to vaccination in Latin America: A systematic literature review. Vaccine 2020, 38, 470–481. [Google Scholar] [CrossRef]
- Urrunaga-Pastor, D.; Bendezu-Quispe, G.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Toro-Huamanchumo, C.J.; Rodriguez-Morales, A.J.; Hernandez, A.V.; Benites-Zapata, V.A. Cross-sectional analysis of COVID-19 vaccine intention, perceptions and hesitancy across Latin America and the Caribbean. Travel Med. Infect. Dis. 2021, 41, 102059. [Google Scholar] [CrossRef]
- Benítez, M.A.; Velasco, C.; Sequeira, A.R.; Henríquez, J.; Menezes, F.M.; Paolucci, F. Responses to COVID-19 in five Latin American countries. Health Policy Technol. 2020, 9, 525–559. [Google Scholar] [CrossRef]
- Martinez-Valle, A. Public health matters: Why is Latin America struggling in addressing the pandemic? J. Public Health Policy 2021, 42, 27–40. [Google Scholar] [CrossRef] [PubMed]
- PAHO. PAHO Director Calls for Fair and Broad Access to COVID-19 Vaccines for Latin America and the Caribbean. Available online: https://www.paho.org/en/news/7-7-2021-paho-director-calls-fair-and-broad-access-covid-19-vaccines-latin-america-and (accessed on 10 August 2021).
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding Vaccine Hesitancy around Vaccines and Vaccination from a Global Perspective: A Systematic Review of Published Literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, G.; Pelullo, C.P.; Della Polla, G.; Pavia, M.; Angelillo, I.F. Exploring the willingness to accept SARS-CoV-2 vaccine in a University population in Southern Italy, September to November 2020. Vaccines 2021, 9, 275. [Google Scholar] [CrossRef]
- Barkay, N.; Cobb, C.; Eilat, R.; Galili, T.; Haimovich, D.; LaRocca, S.; Morris, K.; Sarig, T. Weights and methodology brief for the COVID-19 symptom survey by University of Maryland and Carnegie Mellon University, in partnership with Facebook. arXiv 2020, arXiv:2009.14675. [Google Scholar]
- Fang, X.; Li, S.; Yu, H.; Wang, P.; Zhang, Y.; Chen, Z.; Li, Y.; Cheng, L.; Li, W.; Jia, H.; et al. Epidemiological, comorbidity factors with severity and prognosis of COVID-19: A systematic review and meta-analysis. Aging 2020, 12, 12493–12503. [Google Scholar] [CrossRef] [PubMed]
- Latkin, C.A.; Dayton, L.; Yi, G.; Colon, B.; Kong, X. Mask usage, social distancing, racial, and gender correlates of COVID-19 vaccine intentions among adults in the US. PLoS ONE 2021, 16, e0246970. [Google Scholar] [CrossRef] [PubMed]
- Bendau, A.; Plag, J.; Petzold, M.B.; Ströhle, A. COVID-19 vaccine hesitancy and related fears and anxiety. Int. Immunopharmacol. 2021, 97, 107724. [Google Scholar] [CrossRef]
- Kaur, R.; Callaghan, T.; Regan, A.K. Disparities in maternal influenza immunization among women in rural and urban areas of the United States. Prev. Med. 2021, 147, 106531. [Google Scholar] [CrossRef]
- Murthy, B.P.; Sterrett, N.; Weller, D.; Zell, E.; Reynolds, L.; Toblin, R.L.; Murthy, N.; Kriss, J.; Rose, C.; Cadwell, B.; et al. Disparities in COVID-19 Vaccination Coverage Between Urban and Rural Counties—United States, 14 December 2020–10 April 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 759–764. [Google Scholar] [CrossRef]
- Zhai, Y.; Santibanez, T.A.; Kahn, K.E.; Srivastav, A.; Walker, T.Y.; Singleton, J.A. Rural, urban, and suburban differences in influenza vaccination coverage among children. Vaccine 2020, 38, 7596–7602. [Google Scholar] [CrossRef] [PubMed]
- Vanderpool, R.C.; Stradtman, L.R.; Brandt, H.M. Policy opportunities to increase HPV vaccination in rural communities. Hum. Vaccines Immunother. 2019, 15, 1527–1532. [Google Scholar] [CrossRef]
- Wang, Q.; Xiu, S.; Zhao, S.; Wang, J.; Han, Y.; Dong, S.; Huang, J.; Cui, T.; Yang, L.; Shi, N.; et al. Vaccine Hesitancy: COVID-19 and Influenza Vaccine Willingness among Parents in Wuxi, China—A Cross-Sectional Study. Vaccines 2021, 9, 342. [Google Scholar] [CrossRef]
- Della Polla, G.; Pelullo, C.P.; Napolitano, F.; Angelillo, I.F. HPV vaccine hesitancy among parents in Italy: A cross-sectional study. Hum. Vaccines Immunother. 2020, 16, 2744–2751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceron, W.; Sanseverino, G.G.; De-Lima-Santos, M.-F.; Quiles, M.G. COVID-19 fake news diffusion across Latin America. Soc. Netw. Anal. Min. 2021, 11, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Risco, A.; Mejia, C.R.; Delgado-Zegarra, J.; Del-Aguila-Arcentales, S.; Arce-Esquivel, A.A.; Valladares-Garrido, M.J.; Del Portal, M.R.; Villegas, L.F.; Curioso, W.H.; Sekar, M.C.; et al. The Peru Approach against the COVID-19 Infodemic: Insights and Strategies. Am. J. Trop. Med. Hyg. 2020, 103, 583–586. [Google Scholar] [CrossRef]
- Boyle, J.; Berman, L.; Nowak, G.J.; Iachan, R.; Middleton, D.; Deng, Y. An assessment of parents’ childhood immunization beliefs, intentions, and behaviors using a smartphone panel. Vaccine 2020, 38, 2416–2423. [Google Scholar] [CrossRef]
- He, K.; Mack, W.J.; Neely, M.; Lewis, L.; Anand, V. Parental Perspectives on Immunizations: Impact of the COVID-19 Pandemic on Childhood Vaccine Hesitancy. J. Community Health 2021, 23, 1–14. [Google Scholar] [CrossRef]
- Del Brutto, O.H.; Mera, R.M.; Recalde, B.Y.; Costa, A.F. Social determinants of health and risk of SARS-CoV-2 infection in community-dwelling older adults living in a rural Latin American setting. J. Community Health 2021, 46, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Duarte, R.; Aguiar, A.; Pinto, M.; Furtado, I.; Tiberi, S.; Lönnroth, K.; Migliori, G. Different disease, same challenges: Social determinants of tuberculosis and COVID-19. Pulmonology 2021, 27, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- de Puig, H.; Lee, R.A.; Najjar, D.; Tan, X.; Soekensen, L.R.; Angenent-Mari, N.M.; Donghia, N.M.; Weckman, N.E.; Ory, A.; Ng, C.F. Minimally instrumented SHERLOCK (miSHERLOCK) for CRISPR-based point-of-care diagnosis of SARS-CoV-2 and emerging variants. Sci. Adv. 2021, 7, eabh2944. [Google Scholar] [CrossRef]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, risk of hospital admission, and vaccine effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Núñez-Zapata, S.F.; Benites-Peralta, B.; Mayta-Tristan, P.; Rodríguez-Morales, A.J. High seroprevalence for SARS-CoV-2 infection in South America, but still not enough for heard immunity! Int. J. Infect. Dis. 2021, 109, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; Vegvari, C.; Truscott, J.; Collyer, B.S. Challenges in creating herd immunity to SARS-CoV-2 infection by mass vaccination. Lancet 2020, 396, 1614–1616. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | ||
|---|---|---|---|
| Absolute Frequency of Participants Surveyed | Weighted Proportion According to Each Category | ||
| n | % | 95%CI | |
| Gender | |||
| Male | 87,385 | 45.0 | 44.1–45.8 |
| Female | 140,355 | 55.0 | 54.2–55.9 |
| Age (years) | |||
| 18–24 | 20,306 | 11.5 | 11.0–12.1 |
| 25–34 | 65,107 | 29.8 | 29.1–30.5 |
| 35–44 | 86,869 | 33.8 | 33.1–34.6 |
| 45–54 | 55,458 | 24.8 | 24.2–25.4 |
| Educational level | |||
| Primary school completed, less than primary school or no formal schooling | 99,228 | 47.3 | 45.9–48.7 |
| Secondary school completed or high school (or equivalent) completed | 24,329 | 12.2 | 10.4–14.2 |
| University post-graduate degree completed, university completed, college or pre-university | 104,183 | 40.5 | 38.5–42.5 |
| Living area | |||
| City | 182,980 | 75.3 | 71.4–78.8 |
| Town | 27,981 | 15.4 | 12.7–18.5 |
| Village or rural area | 16,779 | 9.3 | 8.2–10.6 |
| Smoking | |||
| No | 187,072 | 82.7 | 81.2–84.2 |
| Yes | 40,668 | 17.3 | 15.8–18.8 |
| Compliance with physical distancing | |||
| No | 19,557 | 9.4 | 8.9–10.0 |
| Yes | 208,183 | 90.6 | 90.0–91.1 |
| Compliance with mask use | |||
| No | 13,536 | 6.6 | 6.2–7.1 |
| Yes | 214,204 | 93.4 | 92.9–93.8 |
| Food insecurity | |||
| No | 72,907 | 28.9 | 28.0–29.8 |
| Yes | 154,833 | 71.1 | 70.2–72.0 |
| Economic insecurity | |||
| No | 32,610 | 13.2 | 12.7–13.9 |
| Yes | 195,130 | 86.7 | 86.1–87.3 |
| Anxiety symptomatology | |||
| No | 129,178 | 58.6 | 57.2–59.9 |
| Yes | 98,562 | 41.4 | 40.1–42.8 |
| Depressive symptomatology | |||
| No | 119,183 | 54.1 | 52.8–55.4 |
| Yes | 108,557 | 45.9 | 44.6–47.2 |
| Comorbidities | |||
| 0 | 134,454 | 60.9 | 60.1–61.7 |
| 1 | 61,460 | 26.1 | 25.6–26.6 |
| 2 or more | 31,826 | 13.0 | 12.3–13.8 |
| Vaccinated | |||
| No | 141,615 | 66.8 | 64.5–69.0 |
| Yes | 86,125 | 33.2 | 31.0–35.5 |
| Had COVID-19 | |||
| No | 157,246 | 68.7 | 67.4–70.0 |
| Yes | 70,494 | 31.3 | 30.0–32.6 |
| Parents’ intention to vaccinate their children against COVID-19 | |||
| Yes | 212,544 | 92.2 | 91.4–92.9 |
| No | 15,196 | 7.8 | 7.1–8.6 |
| Characteristics | Parents’ Intention to Vaccinate Their Children against COVID-19 | ||||||
|---|---|---|---|---|---|---|---|
| Yes | No | ||||||
| Absolute frequency of participants surveyed | Weighted proportion according to each category | Absolute frequency of participants surveyed | Weighted proportion according to each category | p Value | |||
| n | % | IC95% | n | % | IC95% | ||
| Gender | <0.001 | ||||||
| Male | 81,164 | 91.6 | 90.8–92.3 | 6221 | 8.4 | 7.7–9.2 | |
| Female | 131,380 | 92.6 | 91.8–93.4 | 8975 | 7.4 | 6.6–8.2 | |
| Age (years) | <0.001 | ||||||
| 18–24 | 18,612 | 89.9 | 88.6–91.2 | 1694 | 10.1 | 8.8–11.4 | |
| 25–34 | 60,223 | 91.1 | 90.1–92.0 | 4884 | 8.9 | 8.0–9.9 | |
| 35–44 | 81,408 | 92.7 | 91.9–93.4 | 5461 | 7.3 | 6.6–8.1 | |
| 45–54 | 52,301 | 93.8 | 93.2–94.2 | 3157 | 6.2 | 5.8–6.8 | |
| Educational level | 0.038 | ||||||
| Primary school completed, less than primary school or no formal schooling | 92,408 | 92.2 | 91.5–92.9 | 6820 | 7.8 | 7.1–8.5 | |
| Secondary school completed or high school (or equivalent) completed | 22,348 | 91.1 | 90.0–92.1 | 1981 | 8.9 | 7.9–10.0 | |
| University post-graduate degree completed, university completed, college or pre-university | 97,788 | 92.4 | 91.4–93.3 | 6395 | 7.6 | 6.7–8.6 | |
| Living area | <0.001 | ||||||
| City | 171,517 | 92.9 | 92.3–93.5 | 11,463 | 7.1 | 6.5–7.7 | |
| Town | 25,732 | 90.1 | 88.4–91.6 | 2249 | 9.9 | 8.4–11.6 | |
| Village or rural area | 15,295 | 89.4 | 88.1–90.5 | 1484 | 10.6 | 9.5–11.9 | |
| Smoking | 0.481 | ||||||
| No | 174,613 | 92.1 | 91.3–92.9 | 12,459 | 7.9 | 7.1–8.7 | |
| Yes | 37,931 | 92.3 | 91.5–93.1 | 2737 | 7.7 | 6.9–8.5 | |
| Compliance with physical distancing | <0.001 | ||||||
| No | 16,676 | 84.0 | 82.8–85.1 | 2881 | 16.0 | 14.9–17.2 | |
| Yes | 195,868 | 93.0 | 92.2–93.7 | 12,315 | 7.0 | 6.3–7.8 | |
| Compliance with mask use | <0.001 | ||||||
| No | 11,976 | 85.8 | 84.3–87.2 | 1560 | 14.2 | 12.8–15.7 | |
| Yes | 200,568 | 92.6 | 91.9–93.3 | 13,636 | 7.4 | 6.7–8.1 | |
| Food insecurity | 0.070 | ||||||
| No | 67,862 | 91.8 | 91.0–92.6 | 5045 | 8.2 | 7.4–9.0 | |
| Yes | 144,682 | 92.3 | 91.5–93.0 | 10,151 | 7.7 | 7.0–8.5 | |
| Economic insecurity | <0.001 | ||||||
| No | 29,957 | 90.2 | 89.3–91.0 | 2653 | 9.8 | 9.0–10.7 | |
| Yes | 182,587 | 92.5 | 91.7–93.2 | 12,543 | 7.5 | 6.8–8.3 | |
| Anxiety symptomatology | <0.001 | ||||||
| No | 119,496 | 91.4 | 90.6–92.1 | 9682 | 8.6 | 7.9–9.4 | |
| Yes | 93,048 | 93.2 | 92.4–94.0 | 5514 | 6.8 | 6.0–7.6 | |
| Depressive symptomatology | <0.001 | ||||||
| No | 110,362 | 91.5 | 90.7–92.1 | 8821 | 8.5 | 7.9–9.3 | |
| Yes | 102,182 | 93.0 | 92.1–93.8 | 6375 | 7.0 | 6.2–7.9 | |
| Comorbidities | <0.001 | ||||||
| 0 | 124,340 | 91.1 | 90.1–91.9 | 10,114 | 8.9 | 8.1–9.9 | |
| 1 | 58,034 | 93.8 | 93.1–94.3 | 3426 | 6.2 | 5.7–6.9 | |
| 2 or more | 30,170 | 94.1 | 93.4–94.7 | 1656 | 5.9 | 5.3–6.6 | |
| Vaccinated | <0.001 | ||||||
| No | 128,631 | 89.6 | 88.5–90.6 | 12,984 | 10.4 | 9.4–11.5 | |
| Yes | 83,913 | 97.4 | 97.1–97.5 | 2212 | 2.6 | 2.5–2.9 | |
| Had COVID-19 | 0.015 | ||||||
| No | 146,727 | 91.9 | 91.0–92.8 | 10,519 | 8.1 | 7.2–9.0 | |
| Yes | 65,817 | 92.7 | 92.1–93.2 | 4677 | 7.3 | 6.8–7.9 | |
| Characteristics | Parents’ Non-Intention to Vaccinate Their Children against COVID-19 | |||||
|---|---|---|---|---|---|---|
| Crude | Statistical Adjusted Model | |||||
| cPR | 95%CI | p value | aPR | 95%CI | p Value | |
| Gender | ||||||
| Male | Reference | - | - | Reference | - | - |
| Female | 0.88 | 0.82–0.94 | <0.001 | 0.97 | 0.92–1.03 | 0.308 |
| Age (years) | ||||||
| 18–24 | Reference | - | - | Reference | - | - |
| 25–34 | 0.89 | 0.82–0.96 | 0.002 | 0.94 | 0.88–1.02 | 0.137 |
| 35–44 | 0.73 | 0.66–0.80 | <0.001 | 0.86 | 0.78–0.94 | 0.001 |
| 45–54 | 0.62 | 0.56–0.69 | <0.001 | 0.88 | 0.80–0.97 | 0.011 |
| Educational level | ||||||
| Primary school completed/Less than primary school/No formal schooling | Reference | - | - | Reference | - | - |
| Secondary school completed/High school (or equivalent) completed | 1.15 | 1.06–1.25 | 0.001 | 1.08 | 1.00–1.17 | 0.065 |
| University post-graduate degree completed/university completed/college/pre-university | 0.98 | 0.90–1.07 | 0.695 | 1.20 | 1.10–1.31 | <0.001 |
| Living area | ||||||
| City | Reference | - | - | Reference | - | - |
| Town | 1.39 | 1.20–1.62 | <0.001 | 1.29 | 1.12–1.48 | <0.001 |
| Village or rural area | 1.5 | 1.36–1.66 | <0.001 | 1.34 | 1.22–1.47 | <0.001 |
| Smoking | ||||||
| No | Reference | - | - | Not included * | ||
| Yes | 0.97 | 0.91–1.05 | 0.481 | |||
| Compliance with physical distancing | ||||||
| No | Reference | - | - | Reference | - | - |
| Yes | 0.44 | 0.40–0.48 | <0.001 | 0.46 | 0.42–0.50 | <0.001 |
| Compliance with mask use | ||||||
| No | Reference | - | - | Reference | - | - |
| Yes | 0.52 | 0.48–0.57 | <0.001 | 0.66 | 0.61–0.70 | <0.001 |
| Food insecurity | ||||||
| No | Reference | - | - | Not included * | ||
| Yes | 0.94 | 0.89–1.00 | 0.07 | |||
| Economic insecurity | ||||||
| No | Reference | - | - | Reference | - | - |
| Yes | 0.77 | 0.72–0.82 | <0.001 | 0.80 | 0.75–0.85 | <0.001 |
| Anxiety symptomatology | ||||||
| No | Reference | - | - | Reference | - | - |
| Yes | 0.78 | 0.77–0.88 | <0.001 | 0.87 | 0.82–0.92 | <0.001 |
| Depressive symptomatology | ||||||
| No | Reference | - | - | Reference | - | - |
| Yes | 0.82 | 0.77–0.88 | <0.001 | 0.93 | 0.87–0.99 | 0.03 |
| Comorbidities | ||||||
| 0 | Reference | - | - | Reference | - | - |
| 1 | 0.70 | 0.66–0.74 | <0.001 | 0.82 | 0.77–0.87 | <0.001 |
| 2 or more | 0.66 | 0.61–0.72 | <0.001 | 0.87 | 0.81–0.95 | 0.001 |
| Vaccinated | ||||||
| No | Reference | - | - | Reference | - | - |
| Yes | 0.25 | 0.23–0.28 | <0.001 | 0.26 | 0.23–0.28 | <0.001 |
| Had COVID-19 | ||||||
| No | Reference | - | - | Reference | - | - |
| Yes | 0.91 | 0.84–0.98 | 0.014 | 0.93 | 0.87–0.99 | 0.045 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urrunaga-Pastor, D.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Toro-Huamanchumo, C.J.; Rodriguez-Morales, A.J.; Hernandez, A.V.; Benites-Zapata, V.A.; Bendezu-Quispe, G. Prevalence and Factors Associated with Parents’ Non-Intention to Vaccinate Their Children and Adolescents against COVID-19 in Latin America and the Caribbean. Vaccines 2021, 9, 1303. https://doi.org/10.3390/vaccines9111303
Urrunaga-Pastor D, Herrera-Añazco P, Uyen-Cateriano A, Toro-Huamanchumo CJ, Rodriguez-Morales AJ, Hernandez AV, Benites-Zapata VA, Bendezu-Quispe G. Prevalence and Factors Associated with Parents’ Non-Intention to Vaccinate Their Children and Adolescents against COVID-19 in Latin America and the Caribbean. Vaccines. 2021; 9(11):1303. https://doi.org/10.3390/vaccines9111303
Chicago/Turabian StyleUrrunaga-Pastor, Diego, Percy Herrera-Añazco, Angela Uyen-Cateriano, Carlos J. Toro-Huamanchumo, Alfonso J. Rodriguez-Morales, Adrian V. Hernandez, Vicente A. Benites-Zapata, and Guido Bendezu-Quispe. 2021. "Prevalence and Factors Associated with Parents’ Non-Intention to Vaccinate Their Children and Adolescents against COVID-19 in Latin America and the Caribbean" Vaccines 9, no. 11: 1303. https://doi.org/10.3390/vaccines9111303
APA StyleUrrunaga-Pastor, D., Herrera-Añazco, P., Uyen-Cateriano, A., Toro-Huamanchumo, C. J., Rodriguez-Morales, A. J., Hernandez, A. V., Benites-Zapata, V. A., & Bendezu-Quispe, G. (2021). Prevalence and Factors Associated with Parents’ Non-Intention to Vaccinate Their Children and Adolescents against COVID-19 in Latin America and the Caribbean. Vaccines, 9(11), 1303. https://doi.org/10.3390/vaccines9111303