
Women’s Empowerment and Children’s Complete Vaccination in the Democratic Republic of the Congo: A Cross-Sectional Analysis

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
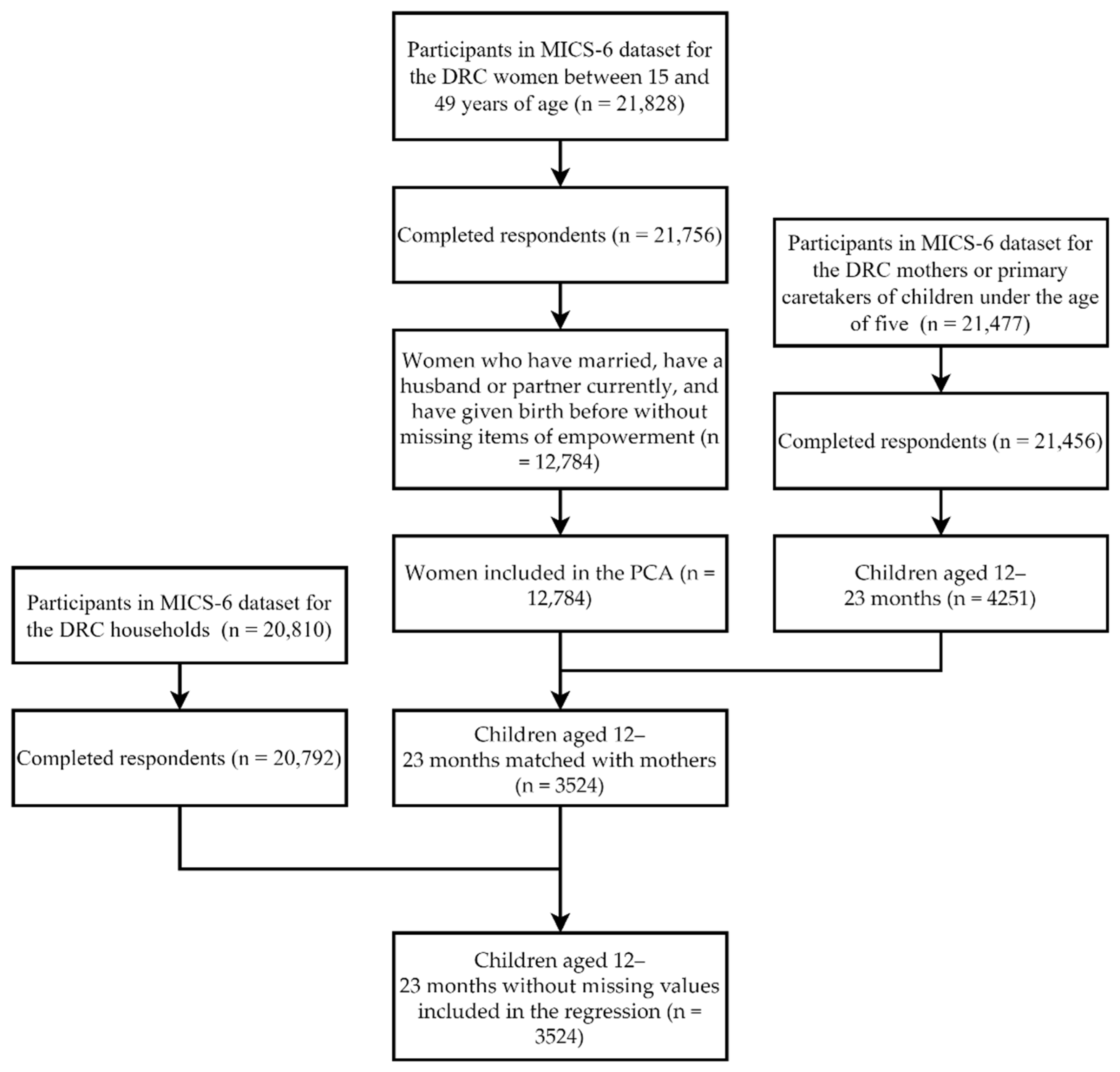
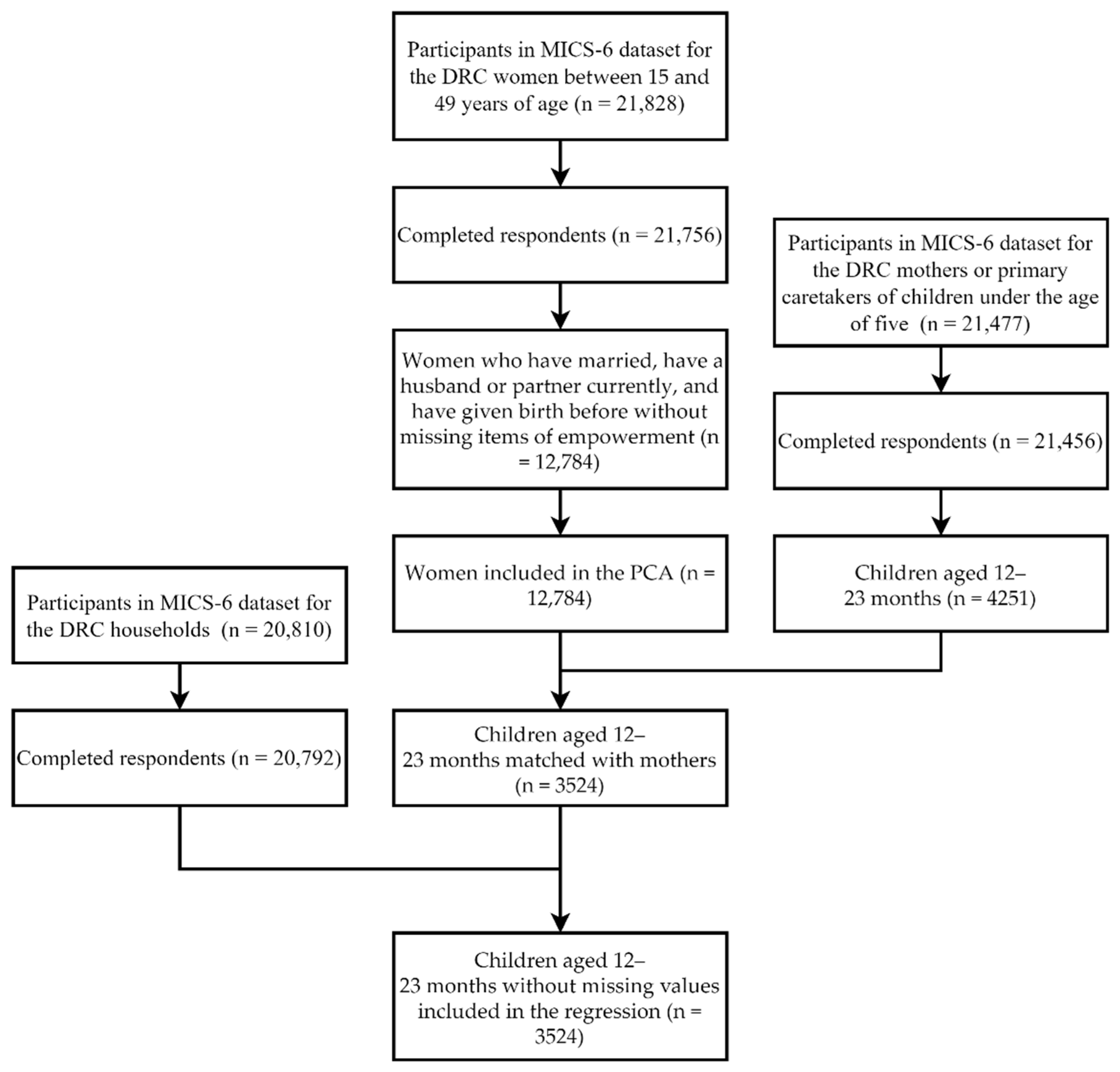
2.1. Study Participants
2.2. Framework
2.3. Measures
2.4. Statistical Analysis
3. Results
3.1. Dimensions of Women’s Empowerment
3.2. Characteristics of Study Participants
3.3. Association between Women’s Empowerment and Children’s Vaccination Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Immunization Coverage. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 10 April 2021).
- WHO. Global Vaccine Action Plan: Monitoring, Evaluation and Accountability. Secretariat Annual Report 2020. Available online: https://www.who.int/publications/i/item/global-vaccine-action-plan-monitoring-evaluation-accountability-secretariat-annual-report-2020 (accessed on 10 April 2021).
- Alfonso, V.H.; Bratcher, A.; Ashbaugh, H.; Doshi, R.; Gadoth, A.; Hoff, N.; Mukadi, P.; Ghanem, A.; Cheng, A.; Gerber, S.; et al. Changes in childhood vaccination coverage over time in the Democratic Republic of the Congo. PLoS ONE 2019, 14, e0217426. [Google Scholar] [CrossRef]
- Le Gargasson, J.B.; Breugelmans, J.G.; Mibulumukini, B.; Da Silva, A.; Colombini, A. Sustainability of National Immunization Programme (NIP) performance and financing following Global Alliance for Vaccines and Immunization (GAVI) support to the Democratic Republic of the Congo (DRC). Vaccine 2013, 31, 1886–1891. [Google Scholar] [CrossRef] [PubMed]
- Doshi, R.H.; Shidi, C.; Mulumba, A.; Eckhoff, P.; Nguyen, C.; Hoff, N.A.; Gerber, S.; Okitolonda, E.; Ilunga, B.K.; Rimoin, A.W. The effect of immunization on measles incidence in the Democratic Republic of Congo: Results from a model of surveillance data. Vaccine 2015, 33, 6786–6792. [Google Scholar] [CrossRef] [PubMed]
- Minetti, A.; Bopp, C.; Fermon, F.; François, G.; Grais, R.F.; Grout, L.; Hurtado, N.; Luquero, F.J.; Porten, K.; Sury, L.; et al. Measles outbreak response immunization is context-specific: Insight from the recent experience of Médecins Sans Frontières. PLoS Med. 2013, 10, e1001544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otshudiema, J.O.; Ndakala, N.G.; Mawanda, E.-t.K.; Tshapenda, G.P.; Kimfuta, J.M.; Nsibu, L.-R.N.; Gueye, A.S.; Dee, J.; Philen, R.M.; Giese, C.; et al. Yellow Fever Outbreak—Kongo Central Province, Democratic Republic of the Congo, August 2016. MMWR. Morb. Mortal. Wkly. Rep. 2017, 66, 335–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, N.D.; Barrett, A.D. Live Attenuated Yellow Fever 17D Vaccine: A Legacy Vaccine Still Controlling Outbreaks In Modern Day. Curr. Infect. Dis. Rep. 2017, 19, 14. [Google Scholar] [CrossRef]
- Bazira, L.; Coulibaly, T.; Mayenga, M.; Ncharre, C.; Yogolelo, R.; Mbule, A.; Moudzeo, H.; Lwamba, P.; Mulumba, A.W.; Cabore, J. Circulating vaccine-derived poliovirus type 2 outbreak in Democratic Republic of Congo 2011–2012. Bull. Soc. Pathol. Exot. 2015, 108, 235–241. [Google Scholar] [CrossRef]
- Gumede, N.; Lentsoane, O.; Burns, C.C.; Pallansch, M.; de Gourville, E.; Yogolelo, R.; Muyembe-Tamfum, J.J.; Puren, A.; Schoub, B.D.; Venter, M. Emergence of vaccine-derived polioviruses, Democratic Republic of Congo, 2004–2011. Emerg. Infect. Dis. 2013, 19, 1583–1589. [Google Scholar] [CrossRef]
- Jorba, J.; Diop, O.M.; Iber, J.; Henderson, E.; Sutter, R.W.; Wassilak, S.G.F.; Burns, C.C. Update on Vaccine-Derived Polioviruses—Worldwide, January 2016–June 2017. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 1185–1191. [Google Scholar] [CrossRef] [Green Version]
- Mbaeyi, C.; Alleman, M.M.; Ehrhardt, D.; Wiesen, E.; Burns, C.C.; Liu, H.; Ewetola, R.; Seakamela, L.; Mdodo, R.; Ndoutabe, M.; et al. Update on Vaccine-Derived Poliovirus Outbreaks—Democratic Republic of the Congo and Horn of Africa, 2017–2018. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 225–230. [Google Scholar] [CrossRef]
- Acharya, P.; Kismul, H.; Mapatano, M.A.; Hatloy, A. Individual- and community-level determinants of child immunization in the Democratic Republic of Congo: A multilevel analysis. PLoS ONE 2018, 13, e0202742. [Google Scholar] [CrossRef]
- Doshi, R.H.; Mukadi, P.; Shidi, C.; Mulumba, A.; Hoff, N.A.; Gerber, S.; Okitolonda-Wemakoy, E.; Ilunga, B.K.; Muyembe, J.J.; Rimoin, A.W. Field evaluation of measles vaccine effectiveness among children in the Democratic Republic of Congo. Vaccine 2015, 33, 3407–3414. [Google Scholar] [CrossRef]
- Varkey, P.; Kureshi, S.; Lesnick, T. Empowerment of women and its association with the health of the community. J. Women’s Health 2010, 19, 71–76. [Google Scholar] [CrossRef]
- Pratley, P. Associations between quantitative measures of women’s empowerment and access to care and health status for mothers and their children: A systematic review of evidence from the developing world. Soc. Sci. Med. 2016, 169, 119–131. [Google Scholar] [CrossRef]
- Kawaguchi, L.; Fouad, N.A.M.; Chiang, C.; Elshair, I.H.H.; Abdou, N.M.; El Banna, S.R.; Aoyama, A. Dimensions of Women’s Empowerment and Their Influence on the Utilization of Maternal Health Services in an Egyptian Village: A Multivariate Analysis. Nagoya J. Med. Sci. 2014, 76, 161–171. [Google Scholar]
- Sado, L.; Spaho, A.; Hotchkiss, D.R. The influence of women’s empowerment on maternal health care utilization: Evidence from Albania. Soc. Sci. Med. 2014, 114, 169–177. [Google Scholar] [CrossRef]
- Janssens, W. Externalities in program evaluation: The impact of a women’s empowerment program on immunization. J. Eur. Econ. Assoc. 2011, 9, 1082–1113. [Google Scholar] [CrossRef]
- Essilfie, G.; Sebu, J.; Annim, S.K. Women’s empowerment and child health outcomes in Ghana. Afr. Dev. Rev. Rev. Afr. Dev. 2020, 32, 200–215. [Google Scholar] [CrossRef]
- Pandey, S.; Lee, H.N. Determinants of child immunization in Nepal: The role of women’s empowerment. Health Educ. J. 2012, 71, 642–653. [Google Scholar] [CrossRef]
- Bago, B.J.; Terefe, W.; Mirutse, G. Individual and community level factors associated with defaulting of immunization among 12–59 months children in Ethiopia: Multilevel modeling analysis using 2011Ethiopia demographic and health survey. Curr. Paediatr. Res. 2018, 22, 95–110. [Google Scholar]
- Porth, J.M.; Wagner, A.L.; Moyer, C.A.; Mutua, M.K.; Boulton, M.L. Women’s Empowerment and Child Vaccination in Kenya: The Modifying Role of Wealth. Am. J. Prev. Med. 2021, 60, S87–S97. [Google Scholar] [CrossRef]
- Thorpe, S.; VanderEnde, K.; Peters, C.; Bardin, L.; Yount, K.M. The Influence of Women’s Empowerment on Child Immunization Coverage in Low, Lower-Middle, and Upper-Middle Income Countries: A Systematic Review of the Literature. Matern. Child Health J. 2016, 20, 172–186. [Google Scholar] [CrossRef]
- Kabeer, N. Resources, Agency, Achievements: Reflections on the Measurement of Women’s Empowerment. Dev. Chang. 1999, 30, 435–464. [Google Scholar] [CrossRef]
- Miedema, S.S.; Haardörfer, R.; Girard, A.W.; Yount, K.M. Women’s empowerment in East Africa: Development of a cross-country comparable measure. World Dev. 2018, 110, 453–464. [Google Scholar] [CrossRef]
- Ewerling, F.; Lynch, J.W.; Victora, C.G.; van Eerdewijk, A.; Tyszler, M.; Barros, A.J.D. The SWPER index for women’s empowerment in Africa: Development and validation of an index based on survey data. Lancet Glob. Health 2017, 5, e916–e923. [Google Scholar] [CrossRef] [Green Version]
- Topuzoglu, A.; Ay, P.; Hidiroglu, S.; Gurbuz, Y. The barriers against childhood immunizations: A qualitative research among socio-economically disadvantaged mothers. Eur. J. Public Health 2007, 17, 348–352. [Google Scholar] [CrossRef] [Green Version]
- Berhe, M.; Medhaniye, A.A.; Kahsay, G.; Birhane, E.; Abay, M. Essential neonatal care utilization and associated factors among mothers in public health facilities of Aksum Town, North Ethiopia, 2016. PLoS ONE 2017, 12, e0175902. [Google Scholar] [CrossRef]
- Burroway, R.; Hargrove, A. Education is the antidote: Individual- and community-level effects of maternal education on child immunizations in Nigeria. Soc. Sci. Med. 2018, 213, 63–71. [Google Scholar] [CrossRef]
- Debie, A.; Lakew, A.M.; Tamirat, K.S.; Amare, G.; Tesema, G.A. Complete vaccination service utilization inequalities among children aged 12–23 months in Ethiopia: A multivariate decomposition analyses. Int. J. Equity Health 2020, 19, 65. [Google Scholar] [CrossRef]
- Rettig, E.M.; Fick, S.E.; Hijmans, R.J. The Female Empowerment Index (FEMI): Spatial and temporal variation in women’s empowerment in Nigeria. Heliyon 2020, 6, e03829. [Google Scholar] [CrossRef]
- Delprato, M.; Akyeampong, K. The Effect of Early Marriage Timing on Women’s and Children’s Health in Sub-Saharan Africa and Southwest Asia. Ann. Glob. Health 2017, 83, 557–567. [Google Scholar] [CrossRef] [Green Version]
- Kamau, N.; Esamai, F.O. Determinants of immunization coverage among children in Mathare Valley, Nairobi. East. Afr. Med. J. 2001, 78, 590–594. [Google Scholar] [CrossRef]
- Fatiregun, A.A.; Okoro, A.O. Maternal determinants of complete child immunization among children aged 12–23 months in a southern district of Nigeria. Vaccine 2012, 30, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, A.; Schuler, S.R.; Boender, C. Measuring Women’s Empowerment as a Variable in International Development. Available online: https://landportal.org/node/13581 (accessed on 6 August 2021).
- Williams, J. Measuring Gender and Women’s Empowerment Using Confirmatory Factor Analysis; Population Program, Institute of Behavioural Science, University of Colorado: Boulder, CO, USA, 2005. [Google Scholar]
- Wado, Y.D.; Afework, M.F.; Hindin, M.J. Childhood vaccination in rural southwestern Ethiopia: The nexus with demographic factors and women’s autonomy. Pan Afr. Med. J. 2014, 17 (Suppl. 1). [Google Scholar] [CrossRef]
- Khan, M.T.; Zaheer, S.; Shafique, K. Maternal education, empowerment, economic status and child polio vaccination uptake in Pakistan: A population based cross sectional study. BMJ Open 2017, 7, e013853. [Google Scholar] [CrossRef] [PubMed]
- Vikram, K.; Vanneman, R.; Desai, S. Linkages between maternal education and childhood immunization in India. Soc. Sci. Med. 2012, 75, 331–339. [Google Scholar] [CrossRef] [Green Version]
- Borooah, V.K. Gender bias among children in India in their diet and immunisation against disease. Soc. Sci. Med. 2004, 58, 1719–1731. [Google Scholar] [CrossRef] [Green Version]
- Mathew, J.L. Inequity in childhood immunization in India: A systematic review. Indian Pediatr. 2012, 49, 203–223. [Google Scholar] [CrossRef]
- Asuman, D.; Ackah, C.G.; Enemark, U. Inequalities in child immunization coverage in Ghana: Evidence from a decomposition analysis. Health Econ. Rev. 2018, 8, 9. [Google Scholar] [CrossRef] [Green Version]
- Cohen, D.K.; Nordås, R. Sexual violence in armed conflict. J. Peace Res. 2014, 51, 418–428. [Google Scholar] [CrossRef]
- Johnson, K.; Scott, J.; Rughita, B.; Kisielewski, M.; Asher, J.; Ong, R.; Lawry, L. Association of sexual violence and human rights violations with physical and mental health in territories of the Eastern Democratic Republic of the Congo. JAMA 2010, 304, 553–562. [Google Scholar] [CrossRef] [Green Version]
- INS. Enquête par Grappes à Indicateurs Multiples, 2017–2018, Rapport de Résultats de L’Enquête; UNICEF: Kinshasa, Congo, 2019. [Google Scholar]
- UNICEF. Multiple Indicator Cluster Surveys. Available online: http://mics.unicef.org/surveys (accessed on 15 March 2021).
- Tamirat, K.S.; Sisay, M.M. Full immunization coverage and its associated factors among children aged 12–23 months in Ethiopia: Further analysis from the 2016 Ethiopia demographic and health survey. BMC Public Health 2019, 19, 1–7. [Google Scholar] [CrossRef]
- Sarker, A.R.; Akram, R.; Ali, N.; Chowdhury, Z.I.; Sultana, M. Coverage and Determinants of Full Immunization: Vaccination Coverage among Senegalese Children. Medicina 2019, 55, 480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voronca, D.; Walker, R.J.; Egede, L.E. Relationship between empowerment and wealth: Trends and predictors in Kenya between 2003 and 2008–2009. Int. J. Public Health 2018, 63, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, H.F. The application of electronic computers to factor analysis. Educ. Psychol. Meas. 1960, 20, 141–151. [Google Scholar] [CrossRef]
- Bartlett, M.S. Tests of significance in factor analysis. Br. J. Stat. Psychol. 1950, 3, 77–85. [Google Scholar] [CrossRef]
- Jones, R.E.; Haardorfer, R.; Ramakrishnan, U.; Yount, K.M.; Miedema, S.S.; Roach, T.D.; Girard, A.W. Intrinsic and instrumental agency associated with nutritional status of East African women. Soc. Sci. Med. 2020, 247, 112803. [Google Scholar] [CrossRef] [PubMed]
- Antai, D. Gender inequities, relationship power, and childhood immunization uptake in Nigeria: A population-based cross-sectional study. Int. J. Infect. Dis. 2012, 16, e136–e145. [Google Scholar] [CrossRef] [Green Version]
- Debnath, A.; Bhattacharjee, N. Understanding Malnutrition of Tribal Children in India: The Role of Women’s Empowerment. Ecol. Food Nutr. 2016, 55, 508–527. [Google Scholar] [CrossRef]
- Ashbaugh, H.R.; Hoff, N.A.; Doshi, R.H.; Alfonso, V.H.; Gadoth, A.; Mukadi, P.; Okitolonda-Wemakoy, E.; Muyembe-Tamfum, J.J.; Gerber, S.K.; Cherry, J.D.; et al. Predictors of measles vaccination coverage among children 6–59 months of age in the Democratic Republic of the Congo. Vaccine 2018, 36, 587–593. [Google Scholar] [CrossRef]
- Abreha, S.K.; Walelign, S.Z.; Zereyesus, Y.A. Associations between women’s empowerment and children’s health status in Ethiopia. PLoS ONE 2020, 15, e0235825. [Google Scholar] [CrossRef] [PubMed]
- Tesema, G.A.; Tessema, Z.T.; Tamirat, K.S.; Teshale, A.B. Complete basic childhood vaccination and associated factors among children aged 12–23 months in East Africa: A multilevel analysis of recent demographic and health surveys. BMC Public Health 2020, 20, 1837. [Google Scholar] [CrossRef] [PubMed]
- Yaya, S.; Odusina, E.K.; Uthman, O.A.; Bishwajit, G. What does women’s empowerment have to do with malnutrition in Sub-Saharan Africa? Evidence from demographic and health surveys from 30 countries. Glob. Health Res. Policy 2020, 5, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekonnen, A.G.; Odo, D.B.; Nigatu, D.; Sav, A.; Abagero, K.K. Women’s empowerment and child growth faltering in Ethiopia: Evidence from the Demographic and Health Survey. BMC Womens Health 2021, 21, 42. [Google Scholar] [CrossRef]
- Ntambue, A.M.; Malonga, F.K.; Cowgill, K.D.; Dramaix-Wilmet, M.; Donnen, P. Incidence of catastrophic expenditures linked to obstetric and neonatal care at 92 facilities in Lubumbashi, Democratic Republic of the Congo, 2015. BMC Public Health 2019, 19, 948. [Google Scholar] [CrossRef] [Green Version]
- Onah, M.N. Women’s empowerment and child nutrition in South-Central Asia; how important is socioeconomic status? SSM Popul. Health 2021, 13, 100718. [Google Scholar] [CrossRef]
- Onah, M.N.; Horton, S.; Hoddinott, J. What empowerment indicators are important for food consumption for women? Evidence from 5 sub-Sahara African countries. PLoS ONE 2021, 16, e0250014. [Google Scholar] [CrossRef]
- UN. Report of the Fourth World Conference on Women; 92-1-130181-5; United Nations: New York, NY, USA, 1995. [Google Scholar]
- UNDP. The SDGs in Action. Available online: https://www.undp.org/sustainable-development-goals (accessed on 15 March 2021).
- Delrieu, I.; Gessner, B.D.; Baril, L.; Roset Bahmanyar, E. From current vaccine recommendations to everyday practices: An analysis in five sub-Saharan African countries. Vaccine 2015, 33, 7290–7298. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Items | Intrinsic Agency | Enabling Resources | Social Independence |
|---|---|---|---|
| Considering beating not justified if wife goes out without telling husband | 0.793 | 0.014 | 0.014 |
| Considering beating not justified if wife neglects the children | 0.806 | −0.023 | 0.004 |
| Considering beating not justified if wife argues with husband | 0.801 | 0.053 | 0.029 |
| Considering beating not justified if wife refuses to have sex with husband | 0.755 | 0.101 | 0.026 |
| Considering beating not justified if wife burns the food | 0.696 | 0.060 | 0.011 |
| Women’s highest education level | 0.090 | 0.627 | 0.017 |
| Covered by health insurance | 0.044 | 0.444 | 0.066 |
| Owning a mobile phone | 0.090 | 0.653 | 0.024 |
| Had used the internet | 0.020 | 0.729 | 0.093 |
| Had used a computer | 0.014 | 0.684 | 0.084 |
| Age difference: women’s age minus husband’s age | 0.005 | −0.166 | 0.301 |
| Women’s age at first marriage | 0.035 | 0.085 | 0.907 |
| Women’s age at first birthing | 0.003 | 0.018 | 0.917 |
| Variables | Total | Complete Vaccination | Incomplete Vaccination | p-Value 2,3 |
|---|---|---|---|---|
| 100.0 | 36.6 | 63.4 | ||
| Intrinsic agency, % | <0.001 | |||
| Low | 26.3 | 27.7 | 72.3 | |
| Middle | 33.6 | 35.3 | 64.7 | |
| High | 40.1 | 43.5 | 56.5 | |
| Enabling resources, % | <0.001 | |||
| Low | 27.1 | 31.1 | 68.9 | |
| Middle | 28.1 | 27.6 | 72.4 | |
| High | 44.8 | 45.5 | 54.5 | |
| Social independence, % | 0.047 | |||
| Low | 33.9 | 36.4 | 63.6 | |
| Middle | 32.2 | 33.0 | 67.0 | |
| High | 34.0 | 40.1 | 59.9 | |
| Considering beating not justified if wife goes out without telling husband, % | <0.001 | |||
| No | 40.7 | 30.9 | 69.1 | |
| Yes | 59.3 | 40.5 | 59.5 | |
| Considering beating not justified if wife neglects the children, % | <0.001 | |||
| No | 44.1 | 30.4 | 69.6 | |
| Yes | 55.9 | 41.5 | 58.5 | |
| Considering beating not justified if wife argues with husband, % | <0.001 | |||
| No | 46.2 | 31.8 | 68.2 | |
| Yes | 53.8 | 40.7 | 59.3 | |
| Considering beating not justified if wife refuses to have sex with husband, % | <0.001 | |||
| No | 44.0 | 31.4 | 68.6 | |
| Yes | 56.0 | 40.6 | 59.4 | |
| Considering beating not justified if wife burns the food, % | <0.001 | |||
| No | 24.6 | 25.5 | 74.5 | |
| Yes | 75.4 | 40.2 | 59.8 | |
| Woman’s highest education level, % | <0.001 | |||
| Pre-primary or none | 17.5 | 32.2 | 67.8 | |
| Primary | 34.3 | 31.8 | 68.2 | |
| Secondary 1 | 14.0 | 30.3 | 69.7 | |
| Secondary 2 | 30.1 | 44.1 | 55.9 | |
| Higher | 4.1 | 61.4 | 38.6 | |
| Covered by health insurance, % | <0.001 | |||
| No | 96.2 | 35.4 | 64.6 | |
| Yes | 3.8 | 65.8 | 34.2 | |
| Owning a mobile phone, % | <0.001 | |||
| No | 71.2 | 29.6 | 70.4 | |
| Yes | 28.8 | 53.8 | 46.2 | |
| Had used the internet, % | <0.001 | |||
| No | 95.6 | 35.4 | 64.6 | |
| Yes | 4.4 | 62.3 | 37.7 | |
| Had used a computer, % | <0.001 | |||
| No | 94.8 | 35.1 | 64.9 | |
| Yes | 5.2 | 63.2 | 36.8 | |
| Age difference: woman’s age minus husband’s age, mean (SD) | -6.7 (5.4) | -7.1 (5.1) | -6.5 (5.5) | 0.15 |
| Woman’s age at first marriage, mean (SD) | 19.0 (4.6) | 19.3 (4.8) | 18.8 (4.5) | 0.002 |
| Woman’s age at first birthing, mean (SD) | 20.7 (4.3) | 21.1 (4.5) | 20.5 (4.2) | 0.006 |
| Variables | Odds Ratio | 95% CI | p-Value 2 |
|---|---|---|---|
| Intrinsic agency | |||
| Low | Ref | ||
| Middle | 1.19 | (0.86, 1.62) | 0.29 |
| High | 1.63 | (1.19, 2.24) | 0.002 |
| Enabling resources | |||
| Low | Ref | ||
| Middle | 1.24 | (0.88, 1.77) | 0.22 |
| High | 1.59 | (1.11, 2.28) | 0.012 |
| Social independence | |||
| Low | Ref | ||
| Middle | 0.75 | (0.56, 1.02) | 0.07 |
| High | 1.01 | (0.72, 1.40) | 0.97 |
| Women’s age | 1.01 | (0.99, 1.03) | 0.36 |
| Children’s sex | |||
| Female | Ref | ||
| Male | 0.92 | (0.72, 1.18) | 0.53 |
| Residence | |||
| Rural | Ref | ||
| Urban | 0.66 | (0.46, 0.95) | 0.027 |
| Family wealth index | |||
| Poor | Ref | ||
| Middle | 1.50 | (1.07, 2.09) | 0.018 |
| Rich | 3.06 | (1.96, 4.78) | <0.001 |
| Number of household members | |||
| 1–5 | Ref | ||
| 6–10 | 0.88 | (0.68, 1.15) | 0.36 |
| ≥10 | 0.67 | (0.36, 1.25) | 0.20 |
| Number of children aged < 5 | |||
| 1 | Ref | ||
| 2 | 0.71 | (0.53, 0.94) | 0.015 |
| ≥3 | 0.66 | (0.45, 0.98) | 0.039 |
| Province | |||
| Sankuru | Ref | ||
| Kinshasa | 9.44 | (2.42, 36.76) | 0.001 |
| Kongo Central | 21.84 | (5.52, 86.40) | <0.001 |
| Kwango | 8.51 | (2.19, 33.07) | 0.002 |
| Kwilu | 3.57 | (0.85, 14.97) | 0.08 |
| Maindombe | 4.53 | (1.08, 19.01) | 0.039 |
| Équateur | 10.99 | (2.88, 41.97) | <0.001 |
| Sud Ubangi | 13.34 | (3.61, 49.27) | <0.001 |
| Nord Ubangi | 7.51 | (1.86, 30.36) | 0.005 |
| Mongala | 2.71 | (0.52, 14.11) | 0.24 |
| Tshuapa | 6.72 | (1.74, 25.98) | 0.006 |
| Tshopo | 6.73 | (1.74, 25.97) | 0.006 |
| Bas Uele | 10.60 | (2.60, 43.31) | 0.001 |
| Haut Uele | 7.14 | (1.60, 31.96) | 0.01 |
| Ituri | 21.56 | (5.55, 83.75) | <0.001 |
| Nord Kivu | 74.83 | (18.43, 303.75) | <0.001 |
| Sud Kivu | 21.91 | (5.91, 81.32) | <0.001 |
| Maniema | 2.39 | (0.59, 9.72) | 0.22 |
| Haut Katanga | 16.62 | (4.44, 62.18) | <0.001 |
| Lualaba | 2.62 | (0.64, 10.68) | 0.18 |
| Haut Lomami | 15.76 | (4.27, 58.19) | <0.001 |
| Tanganyika | 6.31 | (1.56, 25.47) | 0.01 |
| Lomami | 15.18 | (4.05, 56.90) | <0.001 |
| Kasaï Oriental | 12.14 | (3.20, 46.12) | <0.001 |
| Kasaï Central | 22.07 | (5.90, 82.53) | <0.001 |
| Kasaï | 4.80 | (1.27, 18.15) | 0.021 |
| Variables | Poor (N = 2082) | Middle (N = 684) | Rich (N = 724) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p-Value 3 | Odds Ratio | 95% CI | p-Value 3 | Odds Ratio | 95% CI | p-Value 3 | |
| Intrinsic agency | |||||||||
| Low | Ref | Ref | Ref | ||||||
| Middle | 1.72 | (1.09, 2.70) | 0.019 | 1.73 | (0.92, 3.25) | 0.09 | 0.93 | (0.50, 1.71) | 0.81 |
| High | 1.92 | (1.23, 2.98) | 0.004 | 2.35 | (1.14, 4.85) | 0.021 | 1.65 | (0.86, 3.14) | 0.13 |
| Enabling resources | |||||||||
| Low | Ref | Ref | Ref | ||||||
| Middle | 1.23 | (0.81, 1.88) | 0.33 | 2.19 | (1.10, 4.36) | 0.026 | 0.95 | (0.30, 3.00) | 0.93 |
| High | 1.39 | (0.83, 2.31) | 0.21 | 1.21 | (0.58, 2.50) | 0.61 | 2.62 | (1.01, 6.78) | 0.047 |
| Social independence | |||||||||
| Low | Ref | Ref | Ref | ||||||
| Middle | 1.19 | (0.78, 1.81) | 0.42 | 0.82 | (0.42, 1.60) | 0.57 | 0.47 | (0.26, 0.83) | 0.010 |
| High | 1.15 | (0.71, 1.87) | 0.57 | 0.90 | (0.47, 1.73) | 0.75 | 1.03 | (0.55, 1.91) | 0.93 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, X.; Fu, C.; Wang, Q.; He, Q.; Hee, J.; Takesue, R.; Tang, K. Women’s Empowerment and Children’s Complete Vaccination in the Democratic Republic of the Congo: A Cross-Sectional Analysis. Vaccines 2021, 9, 1117. https://doi.org/10.3390/vaccines9101117
Lu X, Fu C, Wang Q, He Q, Hee J, Takesue R, Tang K. Women’s Empowerment and Children’s Complete Vaccination in the Democratic Republic of the Congo: A Cross-Sectional Analysis. Vaccines. 2021; 9(10):1117. https://doi.org/10.3390/vaccines9101117
Chicago/Turabian StyleLu, Xinran, Chuchu Fu, Qianyun Wang, Qiwei He, Jiayi Hee, Rie Takesue, and Kun Tang. 2021. "Women’s Empowerment and Children’s Complete Vaccination in the Democratic Republic of the Congo: A Cross-Sectional Analysis" Vaccines 9, no. 10: 1117. https://doi.org/10.3390/vaccines9101117
APA StyleLu, X., Fu, C., Wang, Q., He, Q., Hee, J., Takesue, R., & Tang, K. (2021). Women’s Empowerment and Children’s Complete Vaccination in the Democratic Republic of the Congo: A Cross-Sectional Analysis. Vaccines, 9(10), 1117. https://doi.org/10.3390/vaccines9101117