
Shedding the Light on Post-Vaccine Myocarditis and Pericarditis in COVID-19 and Non-COVID-19 Vaccine Recipients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset
2.2. Databases
2.2.1. VAERS
2.2.2. MetaCoreTM
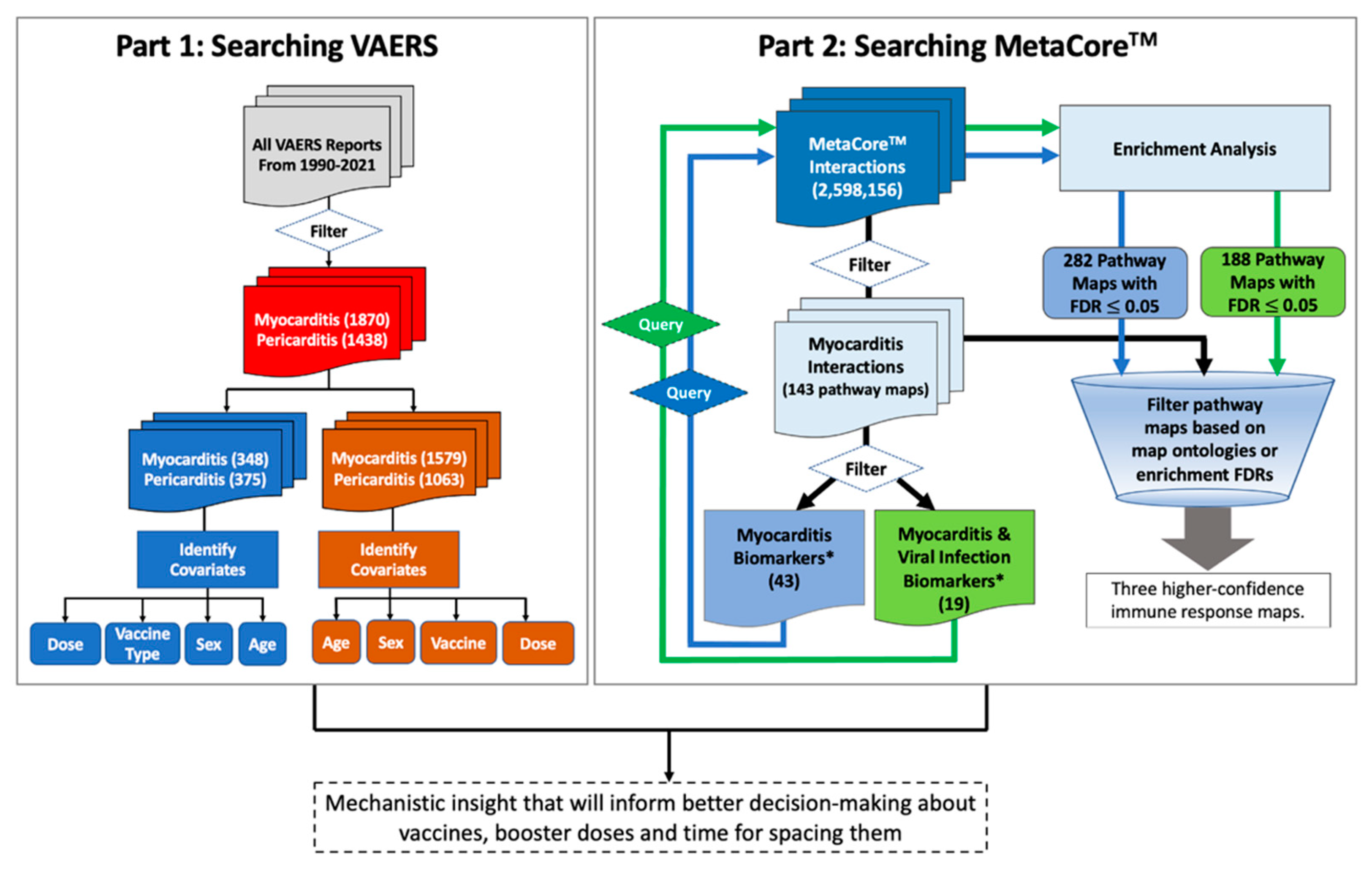
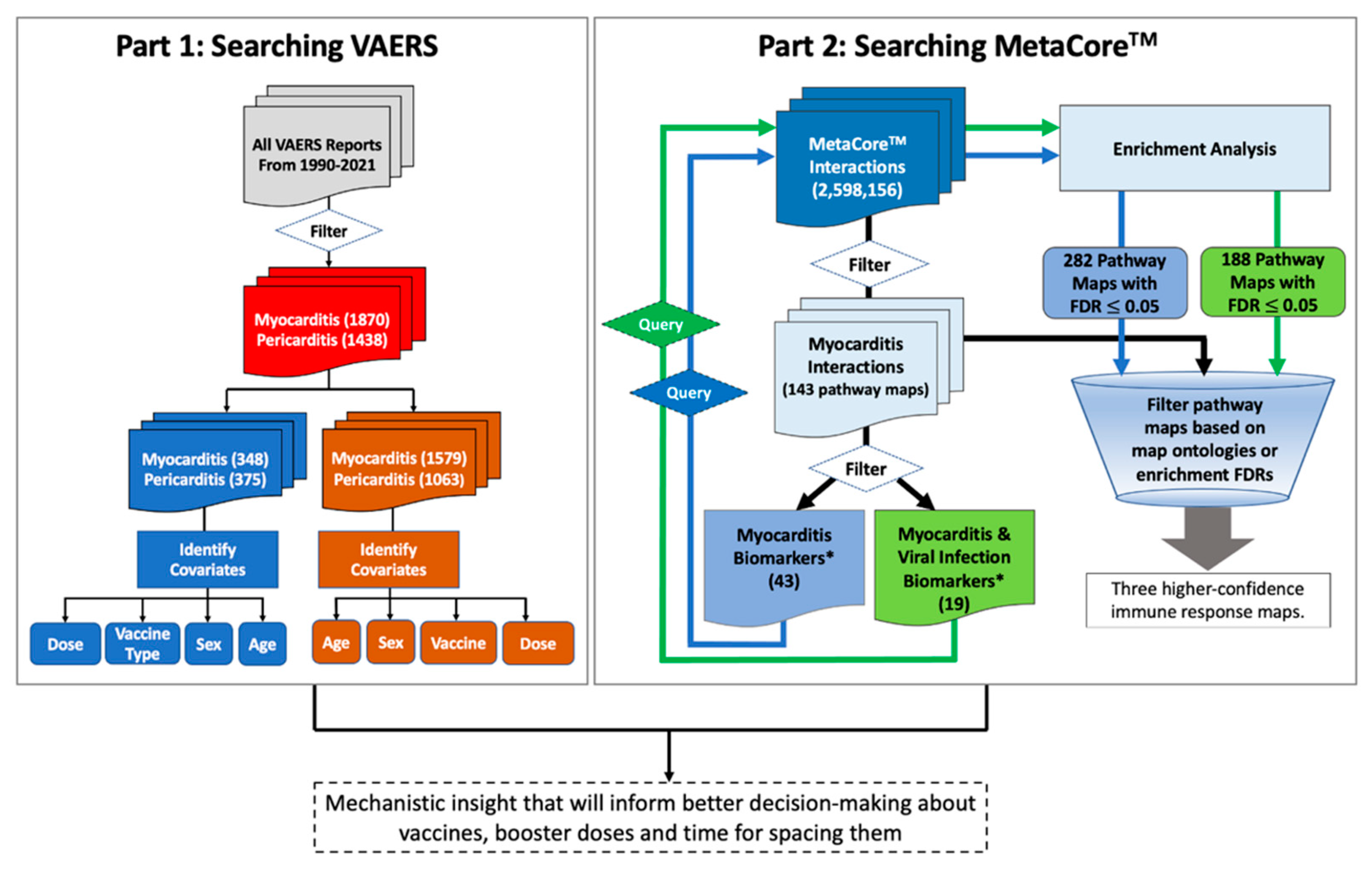
2.3. Integrative Informatics Workflow
3. Results
3.1. Post-COVID-19 Vaccine Myocarditis and Pericarditis Adverse Events
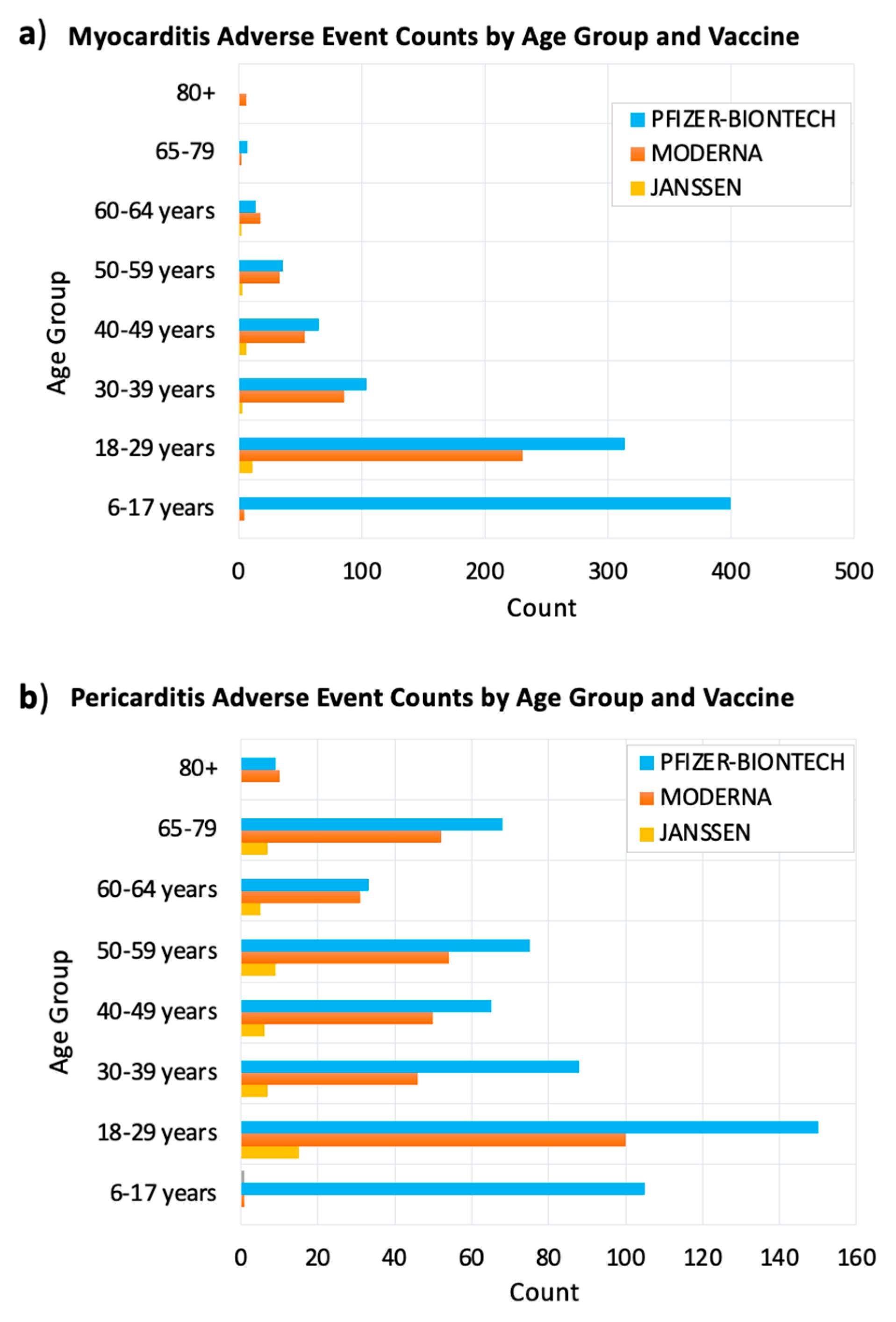
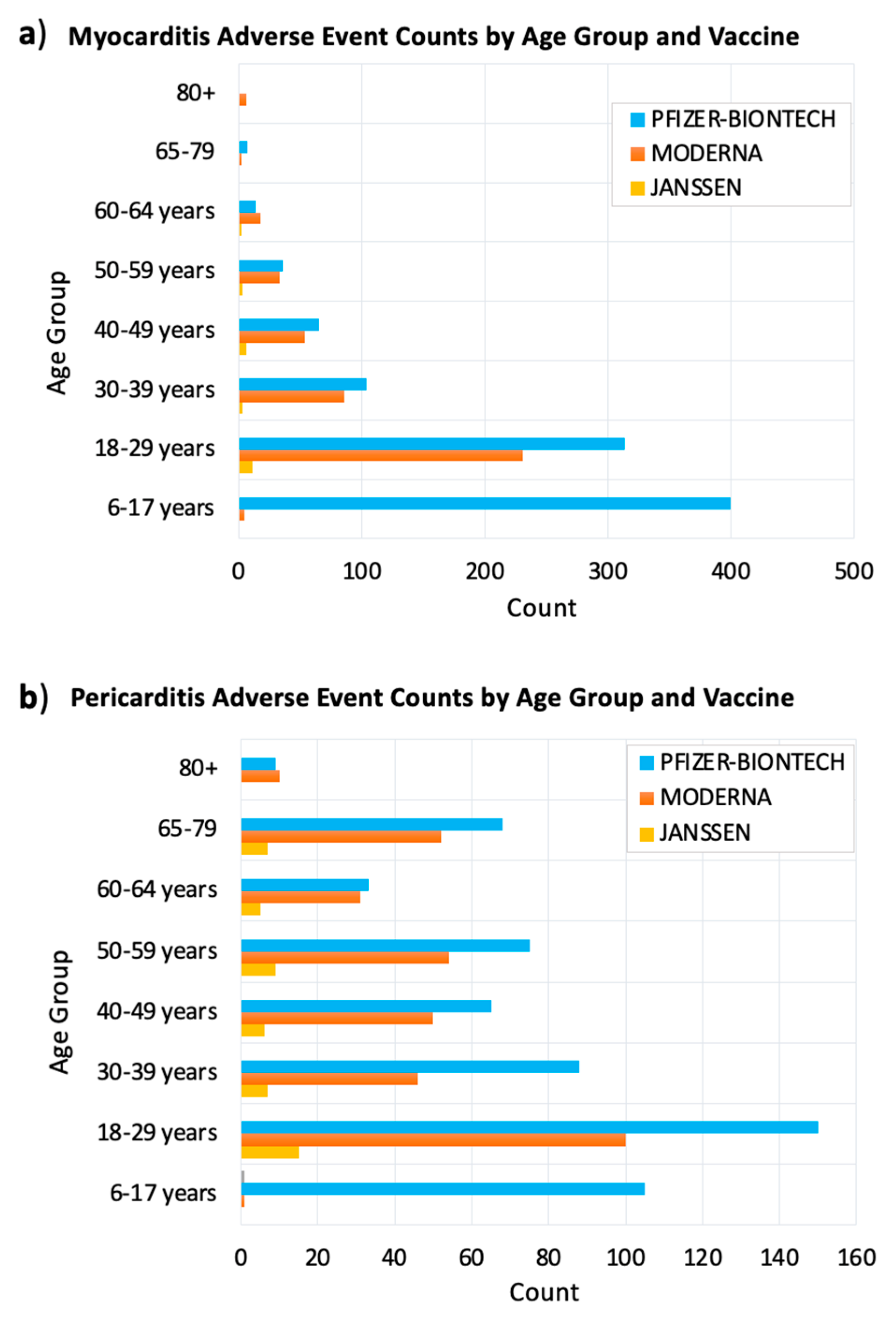
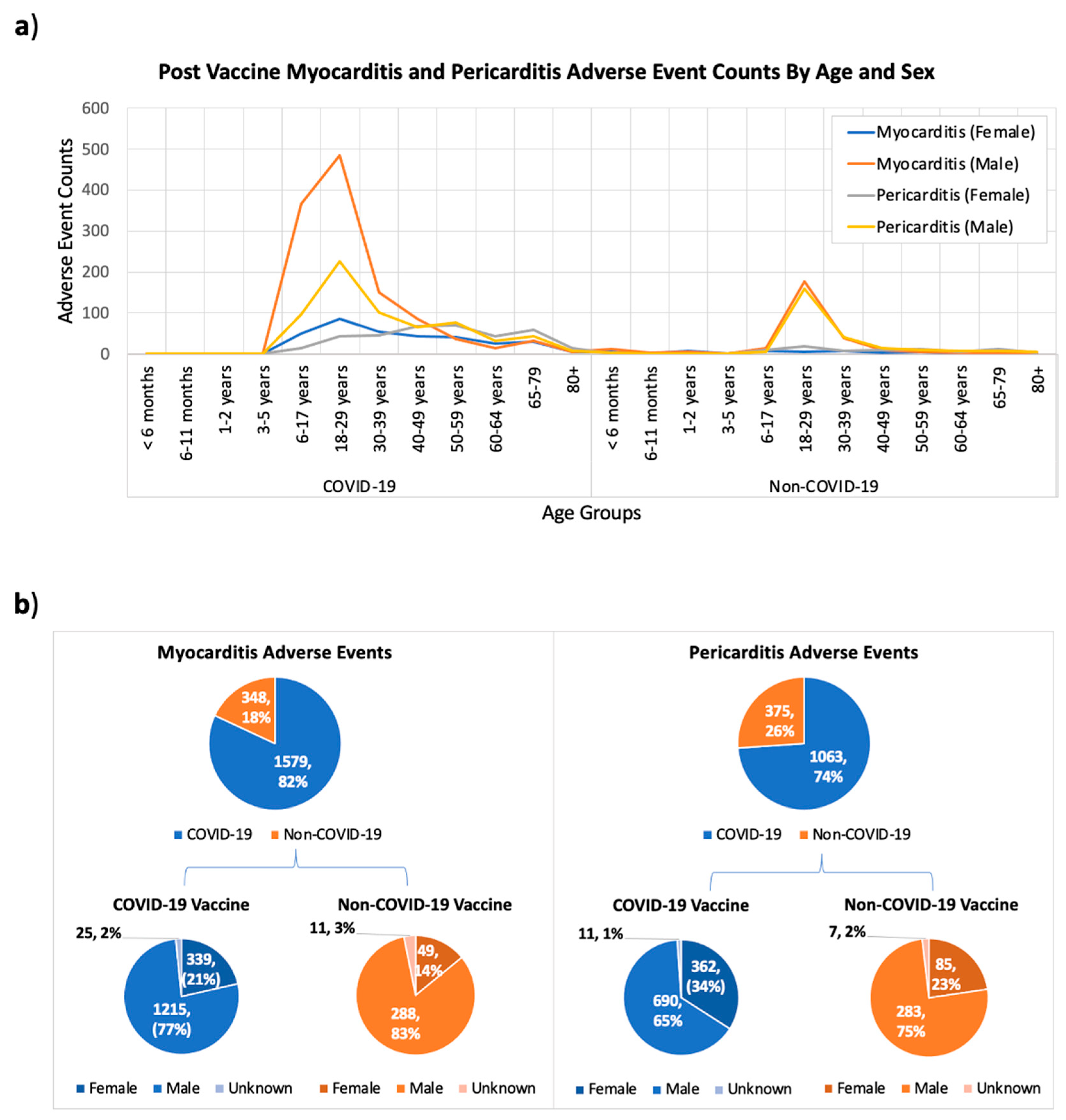
3.1.1. Age Differences
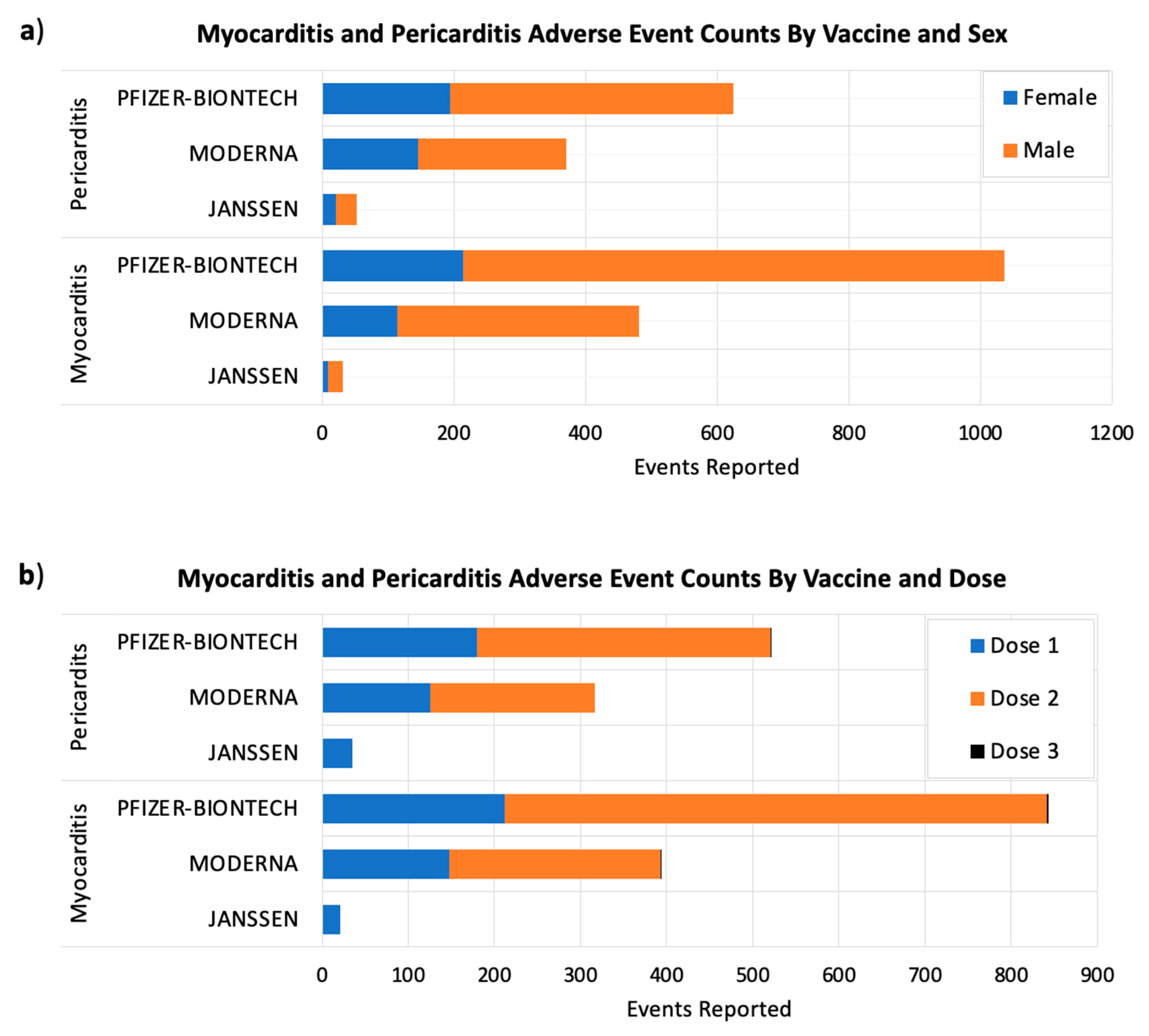
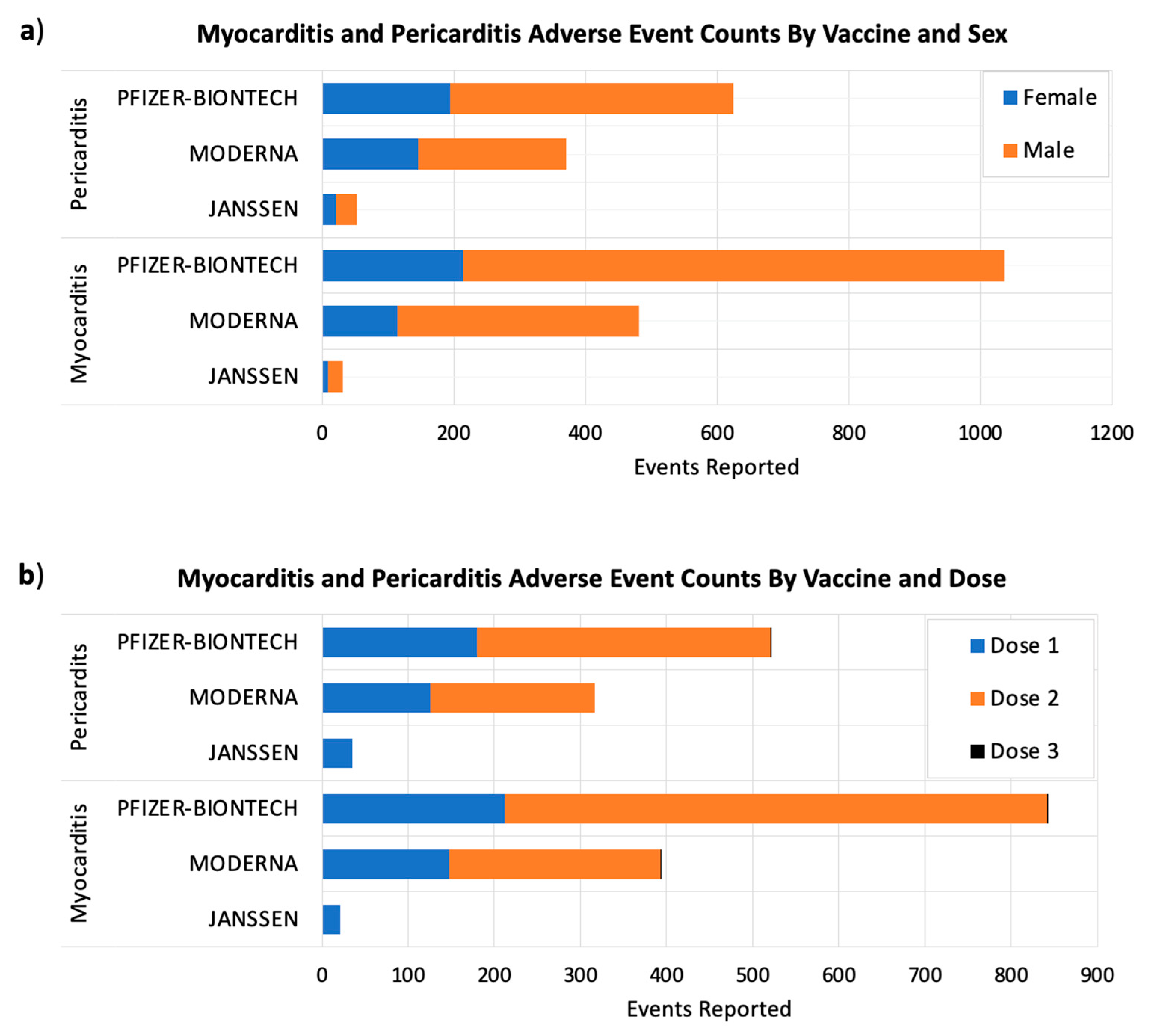
3.1.2. Sex Differences
3.1.3. Vaccine Dose Differences
3.1.4. Outcome Differences
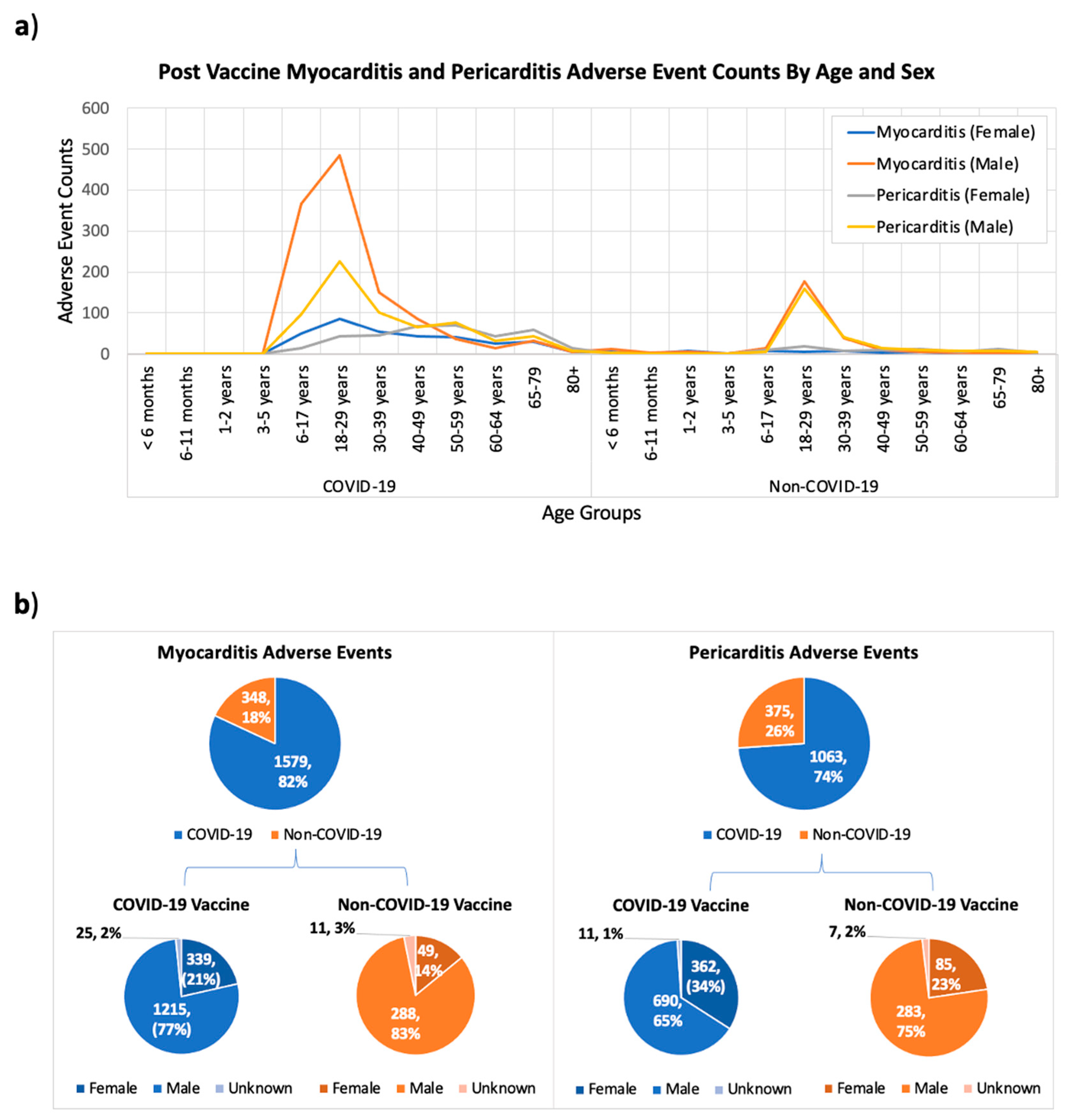
3.2. Comparing Myocarditis and Pericarditis Events Occurring after Receiving COVID-19 versus Non-COVID-19 Vaccines
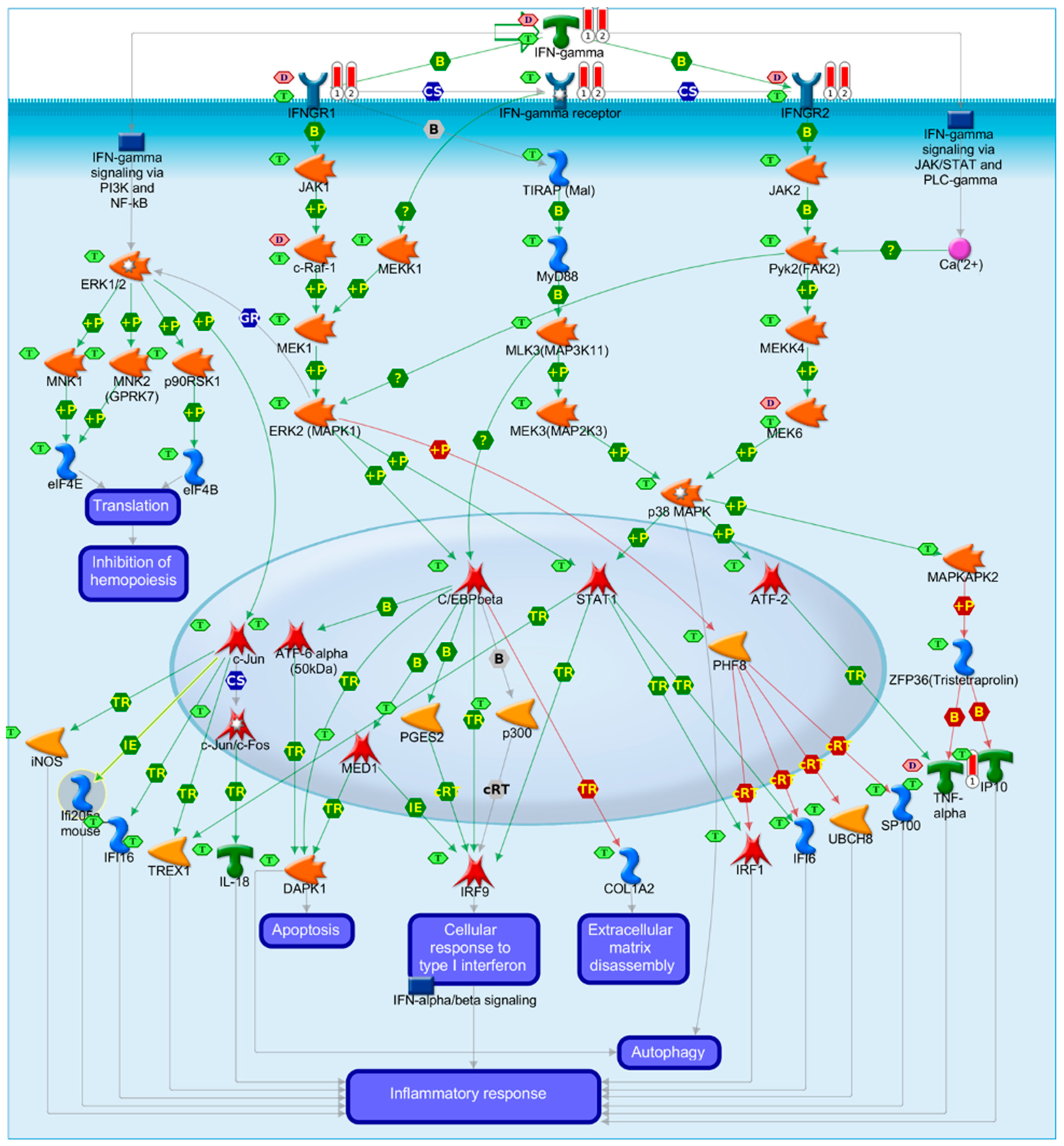
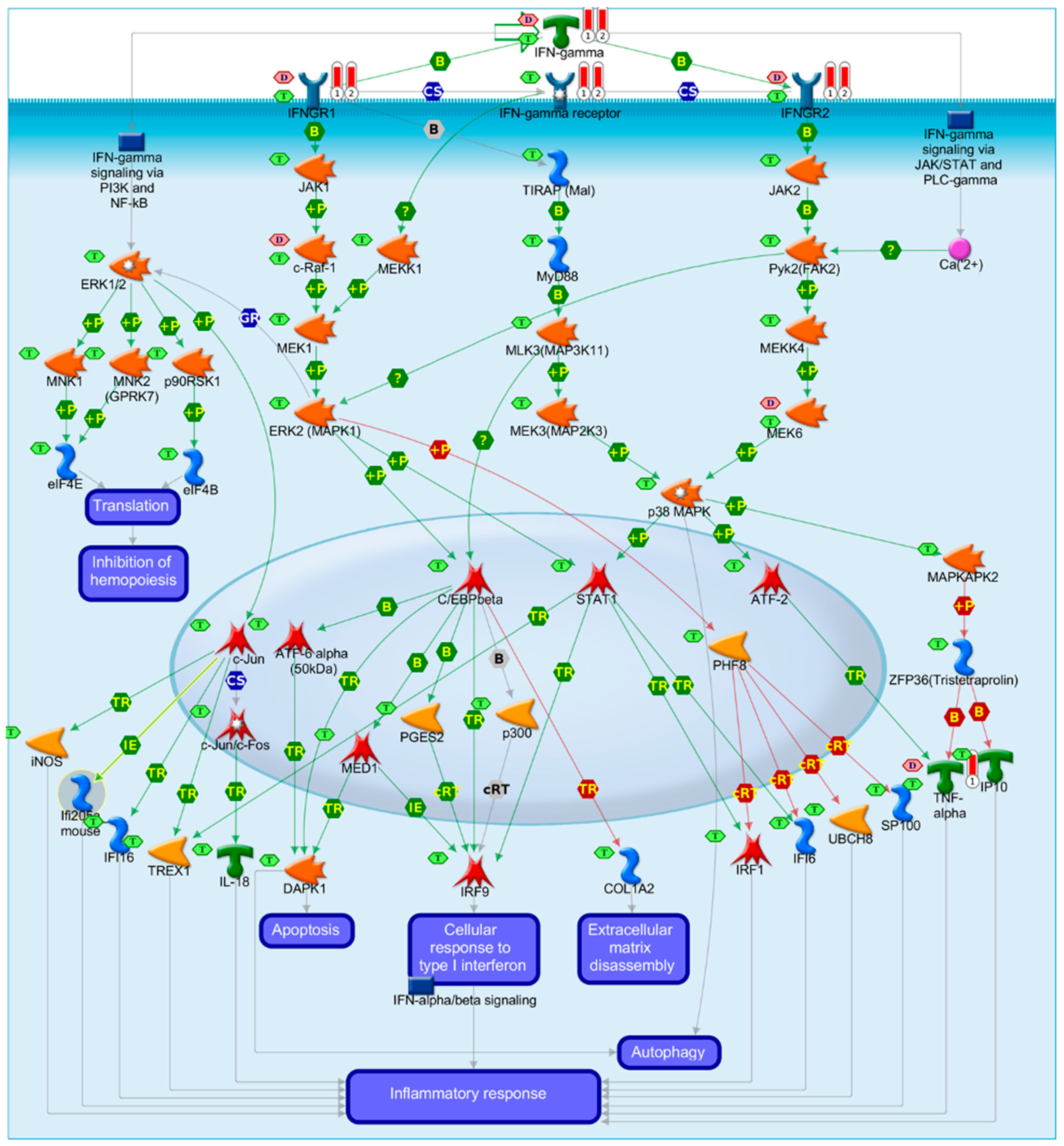
3.3. Identifying Causal Gene Associations with Myocarditis and Pericarditis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Sabbah, D.A.; Hajjo, R.; Bardaweel, S.K.; Zhong, H.A. An Updated Review on SARS-CoV-2 Main Proteinase (MPro): Protein Structure and Small-Molecule Inhibitors. Curr. Top. Med. Chem. 2021, 21, 442–460. [Google Scholar] [CrossRef] [PubMed]
- Sabbah, D.A.; Hajjo, R.; Bardaweel, S.K.; Zhong, H.A. An Updated Review on Betacoronavirus Viral Entry Inhibitors: Learning from Past Discoveries to Advance COVID-19 Drug Discovery. Curr. Top. Med. Chem. 2021, 21, 571–596. [Google Scholar] [CrossRef] [PubMed]
- Forni, G.; Mantovani, A. COVID-19 vaccines: Where we stand and challenges ahead. Cell Death Differ. 2021, 28, 626–639. [Google Scholar] [CrossRef] [PubMed]
- Su, J.R.; McNeil, M.M.; Welsh, K.J.; Marquez, P.L.; Ng, C.; Yan, M.; Cano, M.V. Myopericarditis after vaccination, Vaccine Adverse Event Reporting System (VAERS), 1990–2018. Vaccine 2021, 39, 839–845. [Google Scholar] [CrossRef]
- García, J.B.; Ortega, P.P.; Fernández, A.B.; León, A.C.; Burgos, L.R.; Dorta, E.C. Acute myocarditis after administration of the BNT162b2 vaccine against COVID-19. Rev. Esp. Cardiol. 2021, in press. [Google Scholar]
- NLM. Myocarditis. Available online: http://id.nlm.nih.gov/mesh/D009205 (accessed on 4 September 2021).
- Sagar, S.; Liu, P.P.; Cooper, L.T., Jr. Myocarditis. Lancet 2012, 379, 738–747. [Google Scholar] [CrossRef] [Green Version]
- CDC. COVID-19 VaST Technical Report. 2021. Available online: https://www.cdc.gov/vaccines/acip/work-groups-vast/technical-report-2021-05-17.html (accessed on 4 September 2021).
- VAERS. Vaccine Adverse Event Reporting System (VAERS) Database. 2021. Available online: https://vaers.hhs.gov/ (accessed on 2 September 2021).
- NLM. Pericardium. Available online: https://meshb.nlm.nih.gov/record/ui?ui=D010496 (accessed on 4 September 2021).
- Blanton, R.M.; Carrillo-Salinas, F.J.; Alcaide, P. T-cell recruitment to the heart: Friendly guests or unwelcome visitors? Am. J. Physiol. Heart Circ. Physiol. 2019, 317, H124–H140. [Google Scholar] [CrossRef]
- Cooper, L.T., Jr. Myocarditis. N. Engl. J. Med. 2009, 360, 1526–1538. [Google Scholar] [CrossRef] [Green Version]
- Iordanov, M.S.; Paranjape, J.M.; Zhou, A.; Wong, J.; Williams, B.R.; Meurs, E.F.; Silverman, R.H.; Magun, B.E. Activation of p38 mitogen-activated protein kinase and c-Jun NH2-terminal kinase by double-stranded RNA and encephalomyocarditis virus: Involvement of RNase L, protein kinase R, and alternative pathways. Mol. Cell. Biol. 2000, 20, 617–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meo, S.; Bukhari, I.; Akram, J.; Meo, A.; Klonoff, D. COVID-19 vaccines: Comparison of biological, pharmacological characteristics and adverse effects of Pfizer/BioNTech and Moderna Vaccines. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1663–1669. [Google Scholar] [PubMed]
- CBC NEWS. Available online: https://www.cbsnews.com/news/covid-19-vaccine-cdc-meeting-myocarditis-heart-inflammation/ (accessed on 4 September 2021).
- Hajjo, R.; Setola, V.; Roth, B.L.; Tropsha, A. Chemocentric informatics approach to drug discovery: Identification and experimental validation of selective estrogen receptor modulators as ligands of 5-hydroxytryptamine-6 receptors and as potential cognition enhancers. J. Med. Chem. 2012, 55, 5704–5719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajjo, R.; Tropsha, A. A Systems Biology Workflow for Drug and Vaccine Repurposing: Identifying Small-Molecule BCG Mimics to Reduce or Prevent COVID-19 Mortality. Pharm. Res. 2020, 37, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Bardaweel, S.K.; Hajjo, R.; Sabbah, D.A. Sitagliptin: A potential drug for the treatment of COVID-19? Acta Pharm. 2021, 71, 175–184. [Google Scholar] [CrossRef]
- Hajjo, R.; Sabbah, D.A.; Bardaweel, S.K. Chemocentric Informatics Analysis: Dexamethasone Versus Combination Therapy for COVID-19. ACS Omega 2020, 5, 29765–29779. [Google Scholar] [CrossRef]
- CDC. Centers for Disease Control and Preventiion. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/expect/after.html (accessed on 4 September 2021).
- CDC. Vaccines by Disease. 2021. Available online: https://www.cdc.gov/vaccines/vpd/vaccines-diseases.html (accessed on 4 September 2021).
- Tsukada, B.; Terasaki, F.; Shimomura, H.; Otsuka, K.; Otsuka, K.; Katashima, T.; Fujita, S.; Imanaka-Yoshida, K.; Yoshida, T.; Hiroe, M. High prevalence of chronic myocarditis in dilated cardiomyopathy referred for left ventriculoplasty: Expression of tenascin C as a possible marker for inflammation. Hum. Pathol. 2009, 40, 1015–1022. [Google Scholar] [CrossRef]
- Grabellus, F.; Mall, G.; Schnabel, P.; Wieneke, H.; Pfeifer, U.; Kersting, C.; Schmitz, K.; Wohlschläger, J.; Sigusch, H.; Bierhoff, E. Immunohistochemical differentiation of eosinophilic heart diseases using antibodies against eosinophil activation markers. Histopathology 2005, 46, 89–97. [Google Scholar] [CrossRef]
- Hayney, M.S.; Buck, J.M.; Muller, D. Production of interferon-γ and interleukin-10 after inactivated hepatitis A immunization. Pharmacotherapy 2003, 23, 431–435. [Google Scholar] [CrossRef]
- Huang, G.; Liu, X.; Tang, X.; Du, L.; Feng, W.; Hu, X.; Zhu, L.; Li, Q.; Suo, X. Increased Neutralizing Antibody Production and Interferon-γ Secretion in Response to Porcine Reproductive and Respiratory Syndrome Virus Immunization in Genetically Modified Pigs. Front. Immunol. 2017, 8, 1110. [Google Scholar] [CrossRef] [Green Version]
- Neves, P.C.; Santos, J.R.; Tubarão, L.N.; Bonaldo, M.C.; Galler, R. Early IFN-gamma production after YF 17D vaccine virus immunization in mice and its association with adaptive immune responses. PLoS ONE 2013, 8, e81953. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.S.; Wang, W.; Wu, S.N.; Liu, J.P. Corticosteroids for viral myocarditis. Cochrane Database Syst. Rev. 2013, 10, 1–39. [Google Scholar] [CrossRef] [PubMed]
- Kounis, N.G.; Koniari, I.; de Gregorio, C.; Velissaris, D.; Petalas, K.; Brinia, A.; Assimakopoulos, S.F.; Gogos, C.; Kouni, S.N.; Kounis, G.N. Allergic reactions to current available COVID-19 vaccinations: Pathophysiology, causality, and therapeutic considerations. Vaccines 2021, 9, 221. [Google Scholar] [CrossRef]
- Chin, K.L.; Anis, F.Z.; Sarmiento, M.E.; Norazmi, M.N.; Acosta, A. Role of interferons in the development of diagnostics, vaccines, and therapy for tuberculosis. J. Immunol. Res. 2017, 2017, 5212910. [Google Scholar] [CrossRef] [Green Version]
- Kak, G.; Raza, M.; Tiwari, B.K. Interferon-gamma (IFN-γ): Exploring its implications in infectious diseases. Biomol. Concepts 2018, 9, 64–79. [Google Scholar] [CrossRef]
- Garlapati, S. Do we know the Th1/Th2/Th17 determinants of vaccine response? Expert Rev. Vaccines 2012, 11, 1307–1310. [Google Scholar] [CrossRef]
- Kakkar, R.M.; Soneji, S.; Badhe, R.R.; Desai, S.B. Camptodactyly-arthropathy-coxa vara-pericarditis syndrome: Important differential for juvenile idiopathic arthritis. J. Clin. Imaging Sci. 2013, 3, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Teijaro, J.R.; Farber, D.L. COVID-19 vaccines: Modes of immune activation and future challenges. Nat. Rev. Immunol. 2021, 21, 195–197. [Google Scholar] [CrossRef]
- Calcaterra, G.; Mehta, J.L.; de Gregorio, C.; Butera, G.; Neroni, P.; Fanos, V.; Bassareo, P.P. COVID 19 Vaccine for Adolescents. Concern about Myocarditis and Pericarditis. Pediatr. Rep. 2021, 13, 530–533. [Google Scholar] [CrossRef] [PubMed]
- Morgan, J.; Roper, M.H.; Sperling, L.; Schieber, R.A.; Heffelfinger, J.D.; Casey, C.G.; Miller, J.W.; Santibanez, S.; Herwaldt, B.; Hightower, P. Myocarditis, pericarditis, and dilated cardiomyopathy after smallpox vaccination among civilians in the United States, January–October 2003. Clin. Infect. Dis. 2008, 46, S242–S250. [Google Scholar] [CrossRef] [PubMed]
- Engler, R.J.; Nelson, M.R.; Collins, L.C., Jr.; Spooner, C.; Hemann, B.A.; Gibbs, B.T.; Atwood, J.E.; Howard, R.S.; Chang, A.S.; Cruser, D.L. A prospective study of the incidence of myocarditis/pericarditis and new onset cardiac symptoms following smallpox and influenza vaccination. PLoS ONE 2015, 10, e0118283. [Google Scholar] [CrossRef] [Green Version]
- Murphy, J.G.; Wright, R.S.; Bruce, G.K.; Baddour, L.M.; Farrell, M.A.; Edwards, W.D.; Kita, H.; Cooper, L.T. Eosinophilic-lymphocytic myocarditis after smallpox vaccination. Lancet 2003, 362, 1378–1380. [Google Scholar] [CrossRef]
- Centers for Disease Control Prevention. Update: Cardiac-related events during the civilian smallpox vaccination program—United States, 2003. MMWR 2003, 52, 492–496. [Google Scholar]
- Arness, M.K.; Eckart, R.E.; Love, S.S.; Atwood, J.E.; Wells, T.S.; Engler, R.J.; Collins, L.C.; Ludwig, S.L.; Riddle, J.R.; Grabenstein, J.D. Myopericarditis following smallpox vaccination. Am. J. Epidemiol. 2004, 160, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Cassimatis, D.C.; Atwood, J.E.; Engler, R.M.; Linz, P.E.; Grabenstein, J.D.; Vernalis, M.N. Smallpox vaccination and myopericarditis: A clinical review. J. Am. Coll. Cardiol. 2004, 43, 1503–1510. [Google Scholar] [CrossRef] [Green Version]
- Finlay-Jones, L. Fatal myocarditis after vaccination against smallpox: Report of a case. N. Engl. J. Med. 1964, 270, 41–42. [Google Scholar] [CrossRef]
- Mei, R.; Raschi, E.; Forcesi, E.; Diemberger, I.; De Ponti, F.; Poluzzi, E. Myocarditis and pericarditis after immunization: Gaining insights through the Vaccine Adverse Event Reporting System. Int. J. Cardiol. 2018, 273, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Fenner, F.; Henderson, D.A.; Arita, I.; Jezek, Z.; Ladnyi, I.D. Smallpox and Its Eradication; World Health Organization: Geneva, Switzerland, 1988; Volume 6, pp. 1–1421. [Google Scholar]
- Mittermayer, C. Lethal Complications of Typhoid-Cholera-Vaccination (Case Report and Review of the Literature). Beitr. Pathol. 1976, 158, 212–224. [Google Scholar] [CrossRef]
- Barton, M.; Finkelstein, Y.; Opavsky, M.A.; Ito, S.; Ho, T.; Ford-Jones, L.E.; Taylor, G.; Benson, L.; Gold, R. Eosinophilic myocarditis temporally associated with conjugate meningococcal C and hepatitis B vaccines in children. Pediatr. Infect. Dis. J. 2008, 27, 831–835. [Google Scholar] [CrossRef]
- Aomatsu, M.; Kato, T.; Kasahara, E.; Kitagawa, S. Gender difference in tumor necrosis factor-α production in human neutrophils stimulated by lipopolysaccharide and interferon-γ. Biochem. Biophys. Res. Commun. 2013, 441, 220–225. [Google Scholar] [CrossRef]
- FDA. Fact Sheet for Recipients And Caregivers Emergency Use Authorization (Eua) of the Moderna COVID-19 Vaccine to Prevent Coronavirus Disease 2019 (COVID-19) in Individuals 18 Years of Age and Older; Moderna US, Inc.: Cambridge, MA, USA, 2021. [Google Scholar]
- Sayedahmed, E.E.; Elkashif, A.; Alhashimi, M.; Sambhara, S.; Mittal, S.K. Adenoviral Vector-Based Vaccine Platforms for Developing the Next Generation of Influenza Vaccines. Vaccines 2020, 8, 574. [Google Scholar] [CrossRef]
- Shimabukuro, T.T.; Kim, S.Y.; Myers, T.R.; Moro, P.L.; Oduyebo, T.; Panagiotakopoulos, L.; Marquez, P.L.; Olson, C.K.; Liu, R.; Chang, K.T. Preliminary findings of mRNA COVID-19 vaccine safety in pregnant persons. N. Engl. J. Med. 2021, 384, 2273–2282. [Google Scholar] [CrossRef]
- Murira, A.; Lamarre, A. Type-I interferon responses: From friend to foe in the battle against chronic viral infection. Front. Immunol. 2016, 7, 609. [Google Scholar] [CrossRef] [Green Version]
- Huber, J.P.; David Farrar, J. Regulation of effector and memory T-cell functions by type I interferon. Immunology 2011, 132, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Gadotti, A.C.; de Castro Deus, M.; Telles, J.P.; Wind, R.; Goes, M.; Ossoski, R.G.C.; de Padua, A.M.; de Noronha, L.; Moreno-Amaral, A.; Baena, C.P. IFN-γ is an independent risk factor associated with mortality in patients with moderate and severe COVID-19 infection. Virus Res. 2020, 289, 198171. [Google Scholar] [CrossRef]
- Husseini, A.A.; Kamil, A.A.; Aloudal, M.R. COVID-19 Disease and Interferon-[gamma]: Has it a Protective Impact on Mortality? Erciyes Med. J. 2021, 43, 116–122. [Google Scholar]
- Hu, Z.-J.; Xu, J.; Yin, J.-M.; Li, L.; Hou, W.; Zhang, L.-L.; Zhou, Z.; Yu, Y.-Z.; Li, H.-J.; Feng, Y.-M. Lower circulating interferon-gamma is a risk factor for lung fibrosis in COVID-19 patients. Front. Immunol. 2020, 11, 2348. [Google Scholar] [CrossRef] [PubMed]
- Fathima, T.; Brundha, M.; Ezhilarasan, D. Role of Interferon Gamma in COVID-19 Prevention-A Review. Int. J. Cur. Res Rev. Vol. 2020, 12, 91. [Google Scholar] [CrossRef]
- He, Q.; Mao, Q.; An, C.; Zhang, J.; Gao, F.; Bian, L.; Li, C.; Liang, Z.; Xu, M.; Wang, J. Heterologous prime-boost: Breaking the protective immune response bottleneck of COVID-19 vaccine candidates. Emerg. Microbes Infect. 2021, 10, 629–637. [Google Scholar] [CrossRef]
- van den Elsen, P.J.; Holling, T.M.; Kuipers, H.F.; van der Stoep, N. Transcriptional regulation of antigen presentation. Curr. Opin. Immunol. 2004, 16, 67–75. [Google Scholar] [CrossRef]
- Samuel, C.E. Antiviral actions of interferons. Clin. Microbiol. Rev. 2001, 14, 778–809. [Google Scholar] [CrossRef] [Green Version]
- Pober, J.S.; Merola, J.; Liu, R.; Manes, T.D. Antigen presentation by vascular cells. Front. Immunol. 2017, 8, 1907. [Google Scholar] [CrossRef] [Green Version]
- McNab, F.; Mayer-Barber, K.; Sher, A.; Wack, A.; O’Garra, A. Type I interferons in infectious disease. Nat. Rev. 2015, 15, 87–103. [Google Scholar] [CrossRef] [PubMed]
- Osokine, I.; Snell, L.M.; Cunningham, C.R.; Yamada, D.H.; Wilson, E.B.; Elsaesser, H.J.; de la Torre, J.C.; Brooks, D. Type I interferon suppresses de novo virus-specific CD4 Th1 immunity during an established persistent viral infection. Proc. Natl. Acad. Sci. USA 2014, 111, 7409–7414. [Google Scholar] [CrossRef] [Green Version]
- Arunachalam, P.S.; Scott, M.K.; Hagan, T.; Li, C.; Feng, Y.; Wimmers, F.; Grigoryan, L.; Trisal, M.; Edara, V.V.; Lai, L. Systems vaccinology of the BNT162b2 mRNA vaccine in humans. Nature 2021, 596, 410–416. [Google Scholar] [CrossRef]
- Tomioka, N.; Kishimoto, C.; Matsumori, A.; Kawai, C. Effects of prednisolone on acute viral myocarditis in mice. J. Am. Coll. Cardiol. 1986, 7, 868–872. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Zlotoff, D.A.; Awadalla, M.; Mahmood, S.S.; Nohria, A.; Hassan, M.Z.; Thuny, F.; Zubiri, L.; Chen, C.L.; Sullivan, R.J. Major adverse cardiovascular events and the timing and dose of corticosteroids in immune checkpoint Inhibitor–Associated myocarditis. Circulation 2020, 141, 2031–2034. [Google Scholar] [CrossRef] [PubMed]
- Coyle, J.; Igbinomwanhia, E.; Sanchez-Nadales, A.; Danciu, S.; Chu, C.; Shah, N. A recovered case of COVID-19 myocarditis and ARDS treated with corticosteroids, tocilizumab, and experimental AT-001. Case Rep. 2020, 2, 1331–1336. [Google Scholar]
- Li, Y.; Yu, Y.; Chen, S.; Liao, Y.; Du, J. Corticosteroids and intravenous immunoglobulin in pediatric myocarditis: A meta-analysis. Front. Pediatr. 2019, 7, 342. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, T.; Inomata, T.; Watanabe, I.; Maekawa, E.; Mizutani, T.; Shinagawa, H.; Koitabashi, T.; Takeuchi, I.; Izumi, T. Clinical significance of corticosteroid therapy for eosinophilic myocarditis. Int. Heart J. 2011, 52, 110–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allanore, Y.; Vignaux, O.; Arnaud, L.; Puéchal, X.; Pavy, S.; Duboc, D.; Legmann, P.; Kahan, A. Effects of corticosteroids and immunosuppressors on idiopathic inflammatory myopathy related myocarditis evaluated by magnetic resonance imaging. Ann. Rheum. Dis. 2006, 65, 249–252. [Google Scholar] [CrossRef] [Green Version]
- Kühl, U.; Schultheiss, H.-P. Treatment of chronic myocarditis with corticosteroids. Eur. Heart J. 1995, 16, 168–172. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Myocarditis Adverse Events | ||||
|---|---|---|---|---|
| Rank | Vaccine Type | Vaccine Type Code * | Events Reported | Percent |
| 1 | COVID-19 VACCINE | COVID19 | 1579 | 87.19% |
| 2 | SMALLPOX VACCINE | SMALL | 223 | 12.31% |
| 3 | ANTHRAX VACCINE | ANTH | 63 | 3.48% |
| 4 | TYPHOID VACCINE | TYP | 29 | 1.60% |
| 5 | HEPATITIS B VACCINE | HEP | 26 | 1.44% |
| 6 | INFLUENZA VIRUS VACCINE, TRIVALENT (INJECTED) | FLU3(SEASONAL) | 20 | 1.10% |
| 7 | HAEMOPHILUS B CONJUGATE VACCINE | HIBV | 18 | 0.99% |
| 8 | INFLUENZA VIRUS VACCINE, NO BRAND NAME | FLUX(SEASONAL) | 18 | 0.99% |
| 9 | HEPATITIS A | HEPA | 16 | 0.88% |
| 10 | VARIVAX-VARICELLA VIRUS LIVE | VARCEL | 16 | 0.88% |
| Pericarditis Adverse Events | ||||
| Rank | Vaccine Type | Vaccine Type Code | Events Reported | Percent |
| 1 | COVID-19 VACCINE | COVID19 | 1063 | 79.15% |
| 2 | SMALLPOX VACCINE | SMALL | 200 | 14.89% |
| 3 | ANTHRAX VACCINE | ANTH | 63 | 4.69% |
| 4 | INFLUENZA VIRUS VACCINE, TRIVALENT (INJECTED) | FLU3(SEASONAL) | 35 | 2.61% |
| 5 | TYPHOID VACCINE | TYP | 33 | 2.46% |
| 6 | ZOSTER VACCINE | VARZOS | 29 | 2.16% |
| 7 | HEPATITIS B VACCINE | HEP | 20 | 1.49% |
| 8 | INFLUENZA VIRUS VACCINE, NO BRAND NAME | FLUX(SEASONAL) | 19 | 1.41% |
| 9 | INFLUENZA VIRUS VACCINE, TRIVALENT (INTRANASAL SPRAY) | FLUN3(SEASONAL) | 12 | 0.89% |
| 10 | HUMAN PAPILLOMAVIRUS (TYPES 6, 11, 16, 18) RECOMBINANT VACCINE | HPV4 | 10 | 0.74% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hajjo, R.; Sabbah, D.A.; Bardaweel, S.K.; Tropsha, A. Shedding the Light on Post-Vaccine Myocarditis and Pericarditis in COVID-19 and Non-COVID-19 Vaccine Recipients. Vaccines 2021, 9, 1186. https://doi.org/10.3390/vaccines9101186
Hajjo R, Sabbah DA, Bardaweel SK, Tropsha A. Shedding the Light on Post-Vaccine Myocarditis and Pericarditis in COVID-19 and Non-COVID-19 Vaccine Recipients. Vaccines. 2021; 9(10):1186. https://doi.org/10.3390/vaccines9101186
Chicago/Turabian StyleHajjo, Rima, Dima A. Sabbah, Sanaa K. Bardaweel, and Alexander Tropsha. 2021. "Shedding the Light on Post-Vaccine Myocarditis and Pericarditis in COVID-19 and Non-COVID-19 Vaccine Recipients" Vaccines 9, no. 10: 1186. https://doi.org/10.3390/vaccines9101186
APA StyleHajjo, R., Sabbah, D. A., Bardaweel, S. K., & Tropsha, A. (2021). Shedding the Light on Post-Vaccine Myocarditis and Pericarditis in COVID-19 and Non-COVID-19 Vaccine Recipients. Vaccines, 9(10), 1186. https://doi.org/10.3390/vaccines9101186