

A Prospective Cohort Study of Primary Dengue Virus Infection in Medellín, Colombia

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
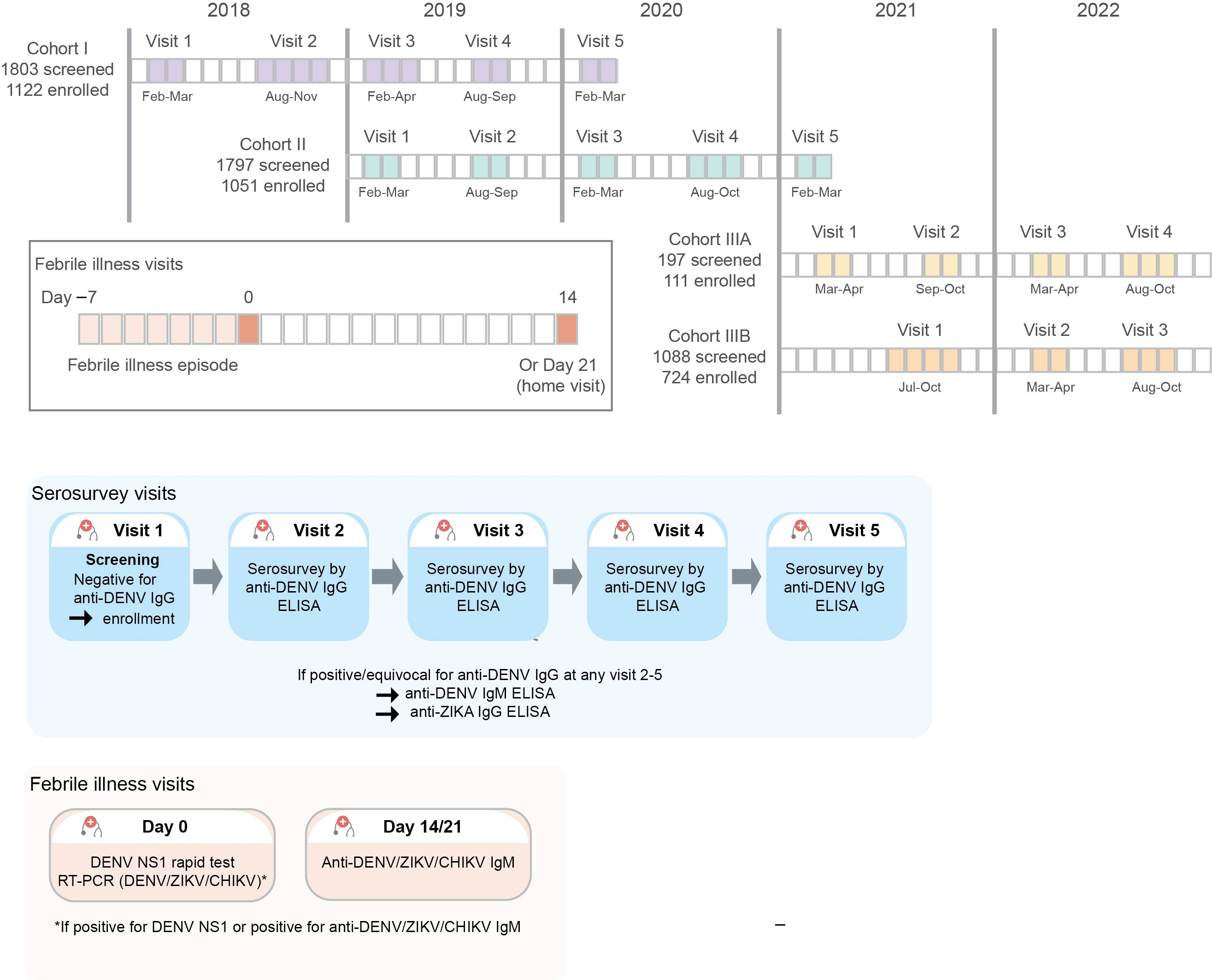
2.1. Study Design
2.2. Participants and Study Eligibility
2.3. Recruitment Tools and Retention Strategies
2.4. Study Objectives and Endpoints
2.5. Study Assessments and Procedures
2.6. Statistical Analysis
2.7. Sample Size
3. Results
3.1. Screened Participants
3.1.1. Disposition
3.1.2. Demographic and Baseline Characteristics of Screened Participants
3.2. Enrolled Participants
3.2.1. Disposition
3.2.2. Demographic and Baseline Characteristics of Enrolled Participants
3.2.3. Evaluation of DENV Seroconversion in Enrolled Participants
3.2.4. Clinically-Confirmed DENV Infections
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CHIKV | Chikungunya virus |
| COVID-19 | coronavirus disease-2019 |
| DENV | dengue virus |
| ELISA | enzyme-linked immunosorbent assay |
| Ig | immunoglobulin |
| ITM | Instituto Tecnológico Metropolitano |
| NS1 | nonstructural protein 1 |
| PECET | Programa de Estudio y Control de Enfermedades Tropicales |
| SD | standard deviation |
| WHO | World Health Organization |
| WMP | World Mosquito Program |
| ZIKV | Zika virus |
References
- Pan American Health Organization. Dengue Incidence Rate. Available online: https://www3.paho.org/data/index.php/en/mnu-topics/indicadores-dengue-en/dengue-nacional-en/254-dengue-incidencia-en.html (accessed on 4 June 2025).
- Mejía-Jurado, E.; Echeverry-Cárdenas, E.; Aguirre-Obando, O.A. Potential current and future distribution for Aedes aegypti and Aedes albopictus in Colombia: Important disease vectors. Biol. Invasions 2024, 26, 2119–2137. [Google Scholar] [CrossRef]
- Gutierrez-Barbosa, H.; Medina-Moreno, S.; Zapata, J.C.; Chua, J.V. Dengue Infections in Colombia: Epidemiological Trends of a Hyperendemic Country. Trop. Med. Infect. Dis. 2020, 5, 156. [Google Scholar] [CrossRef]
- Carabali, M.; Lim, J.K.; Velez, D.C.; Trujillo, A.; Egurrola, J.; Lee, K.S.; Kaufman, J.S.; DaSilva, L.J.; Velez, I.D.; Osorio, J.E. Dengue virus serological prevalence and seroconversion rates in children and adults in Medellin, Colombia: Implications for vaccine introduction. Int. J. Infect. Dis. 2017, 58, 27–36. [Google Scholar] [CrossRef]
- Robert, M.A.; Stewart-Ibarra, A.M.; Estallo, E.L. Climate change and viral emergence: Evidence from Aedes-borne arboviruses. Curr. Opin. Virol. 2020, 40, 41–47. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Fact Sheets. Dengue and Severe Dengue. Available online: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (accessed on 4 June 2025).
- Center for Disease Control and Prevention. Clinical Features of Dengue. Available online: https://www.cdc.gov/dengue/hcp/clinical-signs/index.html (accessed on 23 September 2024).
- Sangkaew, S.; Ming, D.; Boonyasiri, A.; Honeyford, K.; Kalayanarooj, S.; Yacoub, S.; Dorigatti, I.; Holmes, A. Risk predictors of progression to severe disease during the febrile phase of dengue: A systematic review and meta-analysis. Lancet Infect. Dis. 2021, 21, 1014–1026. [Google Scholar] [CrossRef] [PubMed]
- Kao, C.L.; King, C.C.; Chao, D.Y.; Wu, H.L.; Chang, G.J. Laboratory diagnosis of dengue virus infection: Current and future perspectives in clinical diagnosis and public health. J. Microbiol. Immunol. Infect. 2005, 38, 5–16. [Google Scholar] [PubMed]
- Osorio, L.; Uribe, M.; Ardila, G.I.; Orejuela, Y.; Velasco, M.; Bonelo, A.; Parra, B. The use of rapid dengue diagnostic tests in a routine clinical setting in a dengue-endemic area of Colombia. Mem. Inst. Oswaldo Cruz 2015, 110, 510–516. [Google Scholar] [CrossRef] [PubMed]
- MPS/INS/OPS. Ministerio de la Protección Social/Instituto Nacional de Salud/Organización Panamericana de la Salud. Guía Para la Atención Clínica Integral del Paciente con Dengue. OPS/OMS. Bogotá. 2010. 45p. Available online: https://www3.paho.org/col/dmdocuments/GUIA_CLINICA_DENGUE2010.PDF (accessed on 4 July 2025).
- Center for Disease Control and Prevention. Clinical Testing Guidance for Dengue. Available online: https://www.cdc.gov/dengue/hcp/diagnosis-testing/index.html (accessed on 15 May 2025).
- Ackaert, O.; Vanhoutte, F.; Verpoorten, N.; Buelens, A.; Lachau-Durand, S.; Lammens, L.; Hoetelmans, R.; Van Loock, M.; Herrera-Taracena, G. Safety, Tolerability, and Pharmacokinetics of JNJ-1802, a Pan-serotype Dengue Direct Antiviral Small Molecule, in a Phase 1, Double-Blind, Randomized, Dose-Escalation Study in Healthy Volunteers. Clin. Infect. Dis. 2023, 77, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Gunale, B.; Farinola, N.; Kamat, C.D.; Poonawalla, C.S.; Pisal, S.S.; Dhere, R.M.; Miller, C.; Kulkarni, P.S. An observer-blind, randomised, placebo-controlled, phase 1, single ascending dose study of dengue monoclonal antibody in healthy adults in Australia. Lancet Infect. Dis. 2024, 24, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Moquin, S.A.; Simon, O.; Karuna, R.; Lakshminarayana, S.B.; Yokokawa, F.; Wang, F.; Saravanan, C.; Zhang, J.; Day, C.W.; Chan, K.; et al. NITD-688, a pan-serotype inhibitor of the dengue virus NS4B protein, shows favorable pharmacokinetics and efficacy in preclinical animal models. Sci. Transl. Med. 2021, 13, eabb2181. [Google Scholar] [CrossRef] [PubMed]
- Kallas, E.G.; Cintra, M.A.T.; Moreira, J.A.; Patino, E.G.; Braga, P.E.; Tenorio, J.C.V.; Infante, V.; Palacios, R.; de Lacerda, M.V.G.; Batista Pereira, D.; et al. Live, Attenuated, Tetravalent Butantan-Dengue Vaccine in Children and Adults. N. Engl. J. Med. 2024, 390, 397–408. [Google Scholar] [CrossRef]
- Center for Disease Control and Prevention. About a Dengue Vaccine. Available online: https://www.cdc.gov/dengue/vaccine/index.html (accessed on 2 July 2025).
- World Health Organization. WHO Position Paper on Dengue Vaccines—May 2024, Weekly Epidemiological Record. 3 May 2024 Policy Brief. Available online: https://iris.who.int/bitstream/handle/10665/376641/WER9918-eng-fre.pdf?sequence=1 (accessed on 2 July 2025).
- Universidad Industrial de Santander. ¡Qdenga®, the Vaccine Against Dengue is Now Available! Available online: https://comunicaciones.uis.edu.co/qdenga-the-vaccine-against-dengue-is-now-available/ (accessed on 2 July 2025).
- Trujillo-Correa, A.; Salazar, L.M.; López, L.; Van Wesenbeeck, L.; Tambuyzer, L.; Buelens, A.; Van Der Borght, W.; Roothans, F.; De Clerck, K.; Raschaert, F.; et al. Dengue virus serologic prevalence and prospective cohort in adult population from metropolitan area of Medellín, Colombia 2018-2022. In Proceedings of the 7th Pan American Dengue Research Network Meeting, Pandengue 2023, Lima, Peru, 13–16 November 2023. [Google Scholar]
- World Health Organization/TDR. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control. Available online: https://books.google.be/books?hl=nl&lr=&id=dlc0YSIyGYwC&oi=fnd&pg=PP2&ots=OPvVIw3Hp9&sig=Wfiu5TGH4YKz0XcDCnw0jV27lCc&redir_esc=y#v=onepage&q&f=false (accessed on 26 August 2024).
- Fritzell, C.; Rousset, D.; Adde, A.; Kazanji, M.; Van Kerkhove, M.D.; Flamand, C. Current challenges and implications for dengue, chikungunya and Zika seroprevalence studies worldwide: A scoping review. PLoS Negl. Trop. Dis. 2018, 12, e0006533. [Google Scholar] [CrossRef]
- Estupiñán Cárdenas, M.I.; Herrera, V.M.; Miranda Montoya, M.C.; Lozano Parra, A.; Zaraza Moncayo, Z.M.; Flórez García, J.P.; Rodríguez Barraquer, I.; Villar Centeno, L. Heterogeneity of dengue transmission in an endemic area of Colombia. PLoS Negl. Trop. Dis. 2020, 14, e0008122. [Google Scholar] [CrossRef] [PubMed]
- Gil-Mora, J.; Acevedo-Gutiérrez, L.Y.; Betancourt-Ruiz, P.L.; Martínez-Diaz, H.C.; Fernández, D.; Bopp, N.E.; Olaya-Másmela, L.A.; Bolaños, E.; Benavides, E.; Villasante-Tezanos, A.; et al. Arbovirus Antibody Seroprevalence in the Human Population from Cauca, Colombia. Am. J. Trop. Med. Hyg. 2022, 107, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Steffen, R.; Chen, L.H.; Leggat, P.A. Travel vaccines-priorities determined by incidence and impact. J. Travel. Med. 2023, 30, taad085. [Google Scholar] [CrossRef] [PubMed]
- Overbosch, F.W.; Schinkel, J.; Matser, A.; Koen, G.; Prange, I.; Prins, M.; Sonder, G.J. Dengue, chikungunya and Zika virus infections among Dutch travellers to Suriname: A prospective study during the introduction of chikungunya and Zika virus, 2014 to 2017. Euro Surveill. 2023, 28, 2200344. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Salud Colombia. Dengue Situacion Epidemiomogica Colombia. Available online: https://app.powerbi.com/view?r=eyJrIjoiOTIxMzE4MGItNjg4MC00ZmUyLWIwMzctODhlOWFjNzMyZmViIiwidCI6ImE2MmQ2YzdiLTlmNTktNDQ2OS05MzU5LTM1MzcxNDc1OTRiYiIsImMiOjR9 (accessed on 26 August 2024).
- Muñoz, E.; Poveda, G.; Arbeláez, M.P.; Vélez, I.D. Spatiotemporal dynamics of dengue in Colombia in relation to the combined effects of local climate and ENSO. Acta Trop. 2021, 224, 106136. [Google Scholar] [CrossRef]
- World Meteorological Organization. El Niño/La Niña Updates. Available online: https://wmo.int/resources/documents/el-ninola-nina-updates?f%5B0%5D=document_topic%3A20322 (accessed on 11 September 2024).
- El Ministerio de Ambiente y Desarrollo Sostenible. Noticias. Gobierno Nacional Declara Oficialmente el Fenómeno de El Niño y Alerta a Continuar Preparándose. Available online: https://www.minambiente.gov.co/gobierno-nacional-declara-oficialmente-el-fenomeno-de-el-nino-y-alerta-al-pais-a-continuar-preparandose/ (accessed on 9 September 2024).
- El Colombiano. El Dengue Sigue Aumentando en Antioquia: Van Más de 6.590 Casos y 13 Posibles Muertes. Available online: https://www.elcolombiano.com/antioquia/dengue-antioquia-casos-prevenir-PO24808205 (accessed on 2 July 2025).
- Velez, I.D.; Tanamas, S.K.; Arbelaez, M.P.; Kutcher, S.C.; Duque, S.L.; Uribe, A.; Zuluaga, L.; Martínez, L.; Patiño, A.C.; Barajas, J.; et al. Reduced dengue incidence following city-wide wMel Wolbachia mosquito releases throughout three Colombian cities: Interrupted time series analysis and a prospective case-control study. PLoS Negl. Trop. Dis. 2023, 17, e0011713. [Google Scholar] [CrossRef]

{kind=link}
| Cohort | Total | ||||
|---|---|---|---|---|---|
| I | II | IIIA | IIIB | ||
| Screened participants | 1803 | 1797 | 197 | 1088 | 4885 |
| Age, [years] | |||||
| N | 1800 | 1797 | 197 | 1088 | 4882 |
| Mean (SD) | 20.36 (3.594) | 20.41 (3.372) | 33.54 (13.259) | 29.90 (13.155) | 23.04 (8.642) |
| Median | 19.00 | 20.00 | 30.00 | 25.00 | 20.00 |
| Range | (16.0; 60.0) | (16.0; 64.0) | (17.0; 77.0) | (16.0; 76.0) | (16.0; 77.0) |
| <65 | 1800 (100%) | 1797 (100%) | 192 (97.5%) | 1069 (98.3%) | 4858 (99.5%) |
| ≥65 | 0 | 0 | 5 (2.5%) | 19 (1.7%) | 24 (0.5%) |
| Unknown | 3 | 0 | 0 | 0 | 3 |
| Sex, n (%) | |||||
| N | 1803 | 1797 | 197 | 1088 | 4885 |
| Female | 1092 (60.6%) | 1179 (65.6%) | 99 (50.3%) | 709 (65.2%) | 3079 (63.0%) |
| Male | 711 (39.4%) | 618 (34.4%) | 98 (49.7%) | 379 (34.8%) | 1806 (37.0%) |
| Race, n (%) | |||||
| N | 1742 | 1796 | 197 | 1084 | 4819 |
| Mixed White/American Indian | 1666 (95.6%) | 1695 (94.4%) | 0 | 0 | 3361 (69.7%) |
| Black or African American | 42 (2.4%) | 73 (4.1%) | 1 (0.5%) | 6 (0.6%) | 122 (2.5%) |
| White | 33 (1.9%) | 27 (1.5%) | 196 (99.5%) | 1077 (99.4%) | 1333 (27.7%) |
| Multiple | 1 (0.1%) | 1 (0.1%) | 0 | 1 (0.1%) | 3 (0.1%) |
| Unknown | 61 | 1 | 0 | 4 | 66 |
| Ethnicity, n (%) | |||||
| N | 1799 | 1794 | 96 | 894 | 4583 |
| Hispanic or Latino | 1240 (68.9%) | 1794 (100%) | 96 (100%) | 893 (99.9%) | 4023 (87.8%) |
| Not Hispanic or Latino | 559 (31.1%) | 0 | 0 | 1 (0.1%) | 560 (12.2%) |
| Unknown | 4 | 3 | 101 | 194 | 302 |
| Workplace during daytime, n (%) | |||||
| N | 1803 | 1797 | 197 | 1088 | 4885 |
| Universidad de Antioquia | 1801 (99.9%) | 979 (54.5%) | 1 (0.5%) | 419 (38.5%) | 3200 (65.5%) |
| Universidad Cooperativa de Colombia | 0 | 427 (23.8%) | 0 | 17 (1.6%) | 444 (9.1%) |
| Corporación Universitaria Remington | 0 | 389 (21.6%) | 0 | 20 (1.8%) | 409 (8.4%) |
| Colegio Mayor de Antioquia (Colmayor) | 0 | 0 | 28 (14.2%) | 234 (21.5%) | 262 (5.4%) |
| Instituto Tecnológico Metropolitano (ITM) | 0 | 0 | 8 (4.1%) | 96 (8.8%) | 104 (2.1%) |
| Fundación Universitaria San Martín | 0 | 0 | 0 | 92 (8.5%) | 92 (1.9%) |
| Universitaria Pascual Bravo | 0 | 0 | 2 (1.0%) | 54 (5.0%) | 56 (1.1%) |
| Corporación Universitaria de Sabaneta (Unisabaneta) | 0 | 0 | 4 (2.0%) | 31 (2.8%) | 35 (0.7%) |
| Partner Company Arary S.A.S. | 0 | 0 | 65 (33.0%) | 0 | 65 (1.3%) |
| Partner Company EyD Estructuras y Desarrollos | 0 | 0 | 40 (20.3%) | 0 | 40 (0.8%) |
| Other a | 2 (0.1%) | 2 (0.1%) | 49 (24.9%) | 125 (11.5%) | 178 (3.6%) |
| Cohort | Total | ||||
|---|---|---|---|---|---|
| I | II | IIIA | IIIB | ||
| Screened participants | 1803 | 1797 | 197 | 1088 | 4885 |
| Overall, n (%) | |||||
| N | 1799 | 1797 | 197 | 1088 | 4881 |
| Negative | 1122 (62.4%) | 1051 (58.5%) | 111 (56.3%) | 724 (66.5%) | 3008 (61.6%) |
| Positive | 677 (37.6%) | 746 (41.5%) | 86 (43.7%) | 364 (33.5%) | 1873 (38.4%) |
| Sex, n (%) | |||||
| Female | |||||
| N | 1089 | 1179 | 99 | 709 | 3076 |
| Negative | 686 (63.0%) | 707 (60.0%) | 58 (58.6%) | 481 (67.8%) | 1932 (62.8%) |
| Positive | 403 (37.0%) | 472 (40.0%) | 41 (41.4%) | 228 (32.2%) | 1144 (37.2%) |
| Male | |||||
| N | 710 | 618 | 98 | 379 | 1805 |
| Negative | 436 (61.4%) | 344 (55.7%) | 53 (54.1%) | 243 (64.1%) | 1076 (59.6%) |
| Positive | 274 (38.6%) | 274 (44.3%) | 45 (45.9%) | 136 (35.9%) | 729 (40.4%) |
| Age, n (%) | |||||
| <65 years | |||||
| N | 1799 | 1797 | 192 | 1069 | 4857 |
| Negative | 1122 (62.4%) | 1051 (58.5%) | 109 (56.8%) | 717 (67.1%) | 2999 (61.7%) |
| Positive | 677 (37.6%) | 746 (41.5%) | 83 (43.2%) | 352 (32.9%) | 1858 (38.3%) |
| ≥65 years | |||||
| N | 0 | 0 | 5 | 19 | 24 |
| Negative | 0 | 0 | 2 (40.0%) | 7 (36.8%) | 9 (37.5%) |
| Positive | 0 | 0 | 3 (60.0%) | 12 (63.2%) | 15 (62.5%) |
| Race, n (%) | |||||
| Mixed White/American Indian | |||||
| N | 1665 | 1695 | 0 | 0 | 3360 |
| Negative | 1047 (62.9%) | 1023 (60.4%) | 0 | 0 | 2070 (61.6%) |
| Positive | 618 (37.1%) | 672 (39.6%) | 0 | 0 | 1290 (38.4%) |
| Black or African American | |||||
| N | 42 | 73 | 1 | 6 | 122 |
| Negative | 11 (26.2%) | 6 (8.2%) | 0 | 2 (33.3%) | 19 (15.6%) |
| Positive | 31 (73.8%) | 67 (91.8%) | 1 (100%) | 4 (66.7%) | 103 (84.4%) |
| White | |||||
| N | 33 | 27 | 196 | 1077 | 1333 |
| Negative | 23 (69.7%) | 21 (77.8%) | 111 (56.6%) | 717 (66.6%) | 872 (65.4%) |
| Positive | 10 (30.3%) | 6 (22.2%) | 85 (43.4%) | 360 (33.4%) | 461 (34.6%) |
| Multiple | |||||
| N | 1 | 1 | 0 | 1 | 3 |
| Negative | 1 (100%) | 0 | 0 | 1 (100%) | 2 (66.7%) |
| Positive | 0 | 1 (100%) | 0 | 0 | 1 (33.3%) |
| Ethnicity, n (%) | |||||
| Hispanic or Latino | |||||
| N | 1239 | 1794 | 96 | 893 | 4022 |
| Negative | 781 (63.0%) | 1050 (58.5%) | 54 (56.3%) | 596 (66.7%) | 2481 (61.7%) |
| Positive | 458 (37.0%) | 744 (41.5%) | 42 (43.8%) | 297 (33.3%) | 1541 (38.3%) |
| Not Hispanic or Latino | |||||
| N | 559 | 0 | 0 | 1 | 560 |
| Negative | 341 (61.0%) | 0 | 0 | 0 | 341 (60.9%) |
| Positive | 218 (39.0%) | 0 | 0 | 1 (100%) | 219 (39.1%) |
| Cohort | Total | ||||
|---|---|---|---|---|---|
| I | II | IIIA | IIIB | ||
| Enrolled Participants | 1122 | 1051 | 111 | 724 | 3008 |
| Age, [years] | |||||
| N | 1122 | 1051 | 111 | 724 | 3008 |
| Mean (SD) | 20.17 (3.393) | 20.31 (2.903) | 32.15 (13.307) | 27.81 (11.588) | 22.50 (7.741) |
| Median | 19.00 | 20.00 | 28.00 | 23.00 | 20.00 |
| Range | (16.0; 60.0) | (16.0; 39.0) | (17.0; 77.0) | (16.0; 72.0) | (16.0; 77.0) |
| <65 | 1122 (100%) | 1051 (100%) | 109 (98.2%) | 717 (99.0%) | 2999 (99.7%) |
| ≥65 | 0 | 0 | 2 (1.8%) | 7 (1.0%) | 9 (0.3%) |
| Sex, n (%) | |||||
| N | 1122 | 1051 | 111 | 724 | 3008 |
| Female | 686 (61.1%) | 707 (67.3%) | 58 (52.3%) | 481 (66.4%) | 1932 (64.2%) |
| Male | 436 (38.9%) | 344 (32.7%) | 53 (47.7%) | 243 (33.6%) | 1076 (35.8%) |
| Race, n (%) | |||||
| N | 1082 | 1050 | 111 | 720 | 2963 |
| Mixed race | 1047 (96.8%) | 1023 (97.4%) | 0 | 0 | 2070 (69.9%) |
| Black or African American | 11 (1.0%) | 6 (0.6%) | 0 | 2 (0.3%) | 19 (0.6%) |
| White | 23 (2.1%) | 21 (2.0%) | 111 (100%) | 717 (99.6%) | 872 (29.4%) |
| Multiple | 1 (0.1%) | 0 | 0 | 1 (0.1%) | 2 (0.1%) |
| Unknown | 40 | 1 | 0 | 4 | 45 |
| Ethnicity, n (%) | |||||
| N | 1122 | 1050 | 54 | 596 | 2822 |
| Hispanic or Latino | 781 (69.6%) | 1050 (100%) | 54 (100%) | 596 (100%) | 2481 (87.9%) |
| Not Hispanic or Latino | 341 (30.4%) | 0 | 0 | 0 | 341 (12.1%) |
| Unknown | 0 | 1 | 57 | 128 | 186 |
| Workplace during daytime | |||||
| N | 1122 | 1051 | 111 | 724 | 3008 |
| Universidad de Antioquia | 1121 (99.9%) | 609 (57.9%) | 1 (0.9%) | 297 (41.0%) | 2028 (67.4%) |
| Universidad Cooperativa de Colombia | 0 | 247 (23.5%) | 0 | 16 (2.2%) | 263 (8.7%) |
| Corporación Universitaria Remington | 0 | 193 (18.4%) | 0 | 19 (2.6%) | 212 (7.0%) |
| Colegio Mayor de Antioquia (Colmayor) | 0 | 0 | 18 (16.2%) | 155 (21.4%) | 173 (5.8%) |
| Instituto Tecnológico Metropolitano (ITM) | 0 | 0 | 5 (4.5%) | 56 (7.7%) | 61 (2.0%) |
| Fundación Universitaria San Martín | 0 | 0 | 0 | 56 (7.7%) | 56 (1.9%) |
| Universitaria Pascual Bravo | 0 | 0 | 1 (0.9%) | 32 (4.4%) | 33 (1.1%) |
| Corporación Universitaria de Sabaneta (Unisabaneta) | 0 | 0 | 3 (2.7%) | 21 (2.9%) | 24 (0.8%) |
| Partner Company Arary S.A.S. | 0 | 0 | 34 (30.6%) | 0 | 34 (1.1%) |
| Partner Company EyD Estructuras y Desarrollos | 0 | 0 | 18 (16.2%) | 0 | 18 (0.6%) |
| Other a | 1 (0.1%) | 2 (0.2%) | 31 (27.9%) | 72 (9.9%) | 106 (3.5%) |
| Previously vaccinated for Yellow Fever, n (%) | |||||
| Yes | 298 (26.6%) | 479 (45.6%) | 32 (28.8%) | 302 (41.7%) | 1111 (36.9%) |
| No | 824 (73.4%) | 572 (54.4%) | 79 (71.2%) | 422 (58.3%) | 1897 (63.1%) |
| Participants with Paired Serosurveys, n | Laboratory-Confirmed n (%) | Laboratory-Negative n (%) | |
|---|---|---|---|
| 2018 Semester 2 | 863 | 11 (1.3%) | 852 (98.7%) |
| 2018 Total | 863 | 11 (1.3%) | 852 (98.7%) |
| 2019 Semester 1 | 881 | 3 (0.3%) | 878 (99.7%) |
| 2019 Semester 2 | 1675 | 12 (0.7%) | 1663 (99.3%) |
| 2019 Total | 1755 | 15 (0.9%) | 1740 (99.1%) |
| 2020 Semester 1 | 1576 | 8 (0.5%) | 1568 (99.5%) |
| 2020 Semester 2 | 594 | 0 (0.0%) | 594 (100%) |
| 2020 Total | 1641 | 8 (0.5%) | 1633 (99.5%) |
| 2021 Semester 1 | 645 | 2 (0.3%) | 643 (99.7%) |
| 2021 Semester 2 | 110 | 1 (0.9%) | 109 (99.1%) |
| 2021 Total | 755 | 3 (0.4%) | 752 (99.6%) |
| 2022 Semester 1 | 698 | 13 (1.9%) | 685 (98.1%) |
| 2022 Semester 2 | 619 | 2 (0.3%) | 617 (99.7%) |
| 2022 Total | 737 | 15 (2.0%) | 722 (98.0%) |
| Total | 2644 | 52 (2.0%) | 2592 (98.0%) |
| Total (n = 3008) | |
|---|---|
| Number of participants with a febrile illness episode | 19 |
| Positive DENV NS1 rapid test, n | 0 |
| Positive for anti-DENV IgM antibodies (Day 14), n | 3 |
| Positive for DENV RNA (RT-PCR a), n | 0 |
| Positive for ZIKV RNA (RT-PCR a), n | 0 |
| Positive for CHIKV RNA (RT-PCR a), n | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trujillo, A.; Van Wesenbeeck, L.; Salazar, L.; López, L.; Tambuyzer, L.; Buelens, A.; Clerck, K.D.; Lenz, O.; Vijgen, L.; Van Loock, M.; et al. A Prospective Cohort Study of Primary Dengue Virus Infection in Medellín, Colombia. Vaccines 2025, 13, 748. https://doi.org/10.3390/vaccines13070748
Trujillo A, Van Wesenbeeck L, Salazar L, López L, Tambuyzer L, Buelens A, Clerck KD, Lenz O, Vijgen L, Van Loock M, et al. A Prospective Cohort Study of Primary Dengue Virus Infection in Medellín, Colombia. Vaccines. 2025; 13(7):748. https://doi.org/10.3390/vaccines13070748
Chicago/Turabian StyleTrujillo, Andrea, Liesbeth Van Wesenbeeck, Lina Salazar, Liliana López, Lotke Tambuyzer, Annemie Buelens, Kim De Clerck, Oliver Lenz, Leen Vijgen, Marnix Van Loock, and et al. 2025. "A Prospective Cohort Study of Primary Dengue Virus Infection in Medellín, Colombia" Vaccines 13, no. 7: 748. https://doi.org/10.3390/vaccines13070748
APA StyleTrujillo, A., Van Wesenbeeck, L., Salazar, L., López, L., Tambuyzer, L., Buelens, A., Clerck, K. D., Lenz, O., Vijgen, L., Van Loock, M., Herrera-Taracena, G., Vélez, I. D., & Rasschaert, F. (2025). A Prospective Cohort Study of Primary Dengue Virus Infection in Medellín, Colombia. Vaccines, 13(7), 748. https://doi.org/10.3390/vaccines13070748