
Epidemiological Impact of Increasing Vaccination Coverage Rate and Re-Vaccination on Pneumococcal Disease in Older Adults in Germany

 , , and
, , and
Abstract
1. Introduction
2. Methods
- Vaccine formulation—replacement of PPSV23 (scenario 0) with either PCV20 (scenarios 1–4) or V116 (scenarios 5–8);
- Vaccine uptake—continuing at 30% uptake (scenarios 1, 2, 5, and 6), or increasing to 60% uptake (scenarios 3, 4, 7, and 8);
- Revaccination of adults previously vaccinated with PPSV23—no revaccination (scenarios 1, 3, 5, and 7), or revaccination at 50% uptake with the same vaccine formulation as for routine vaccination (scenarios 2, 4, 6, and 8).
3. Results
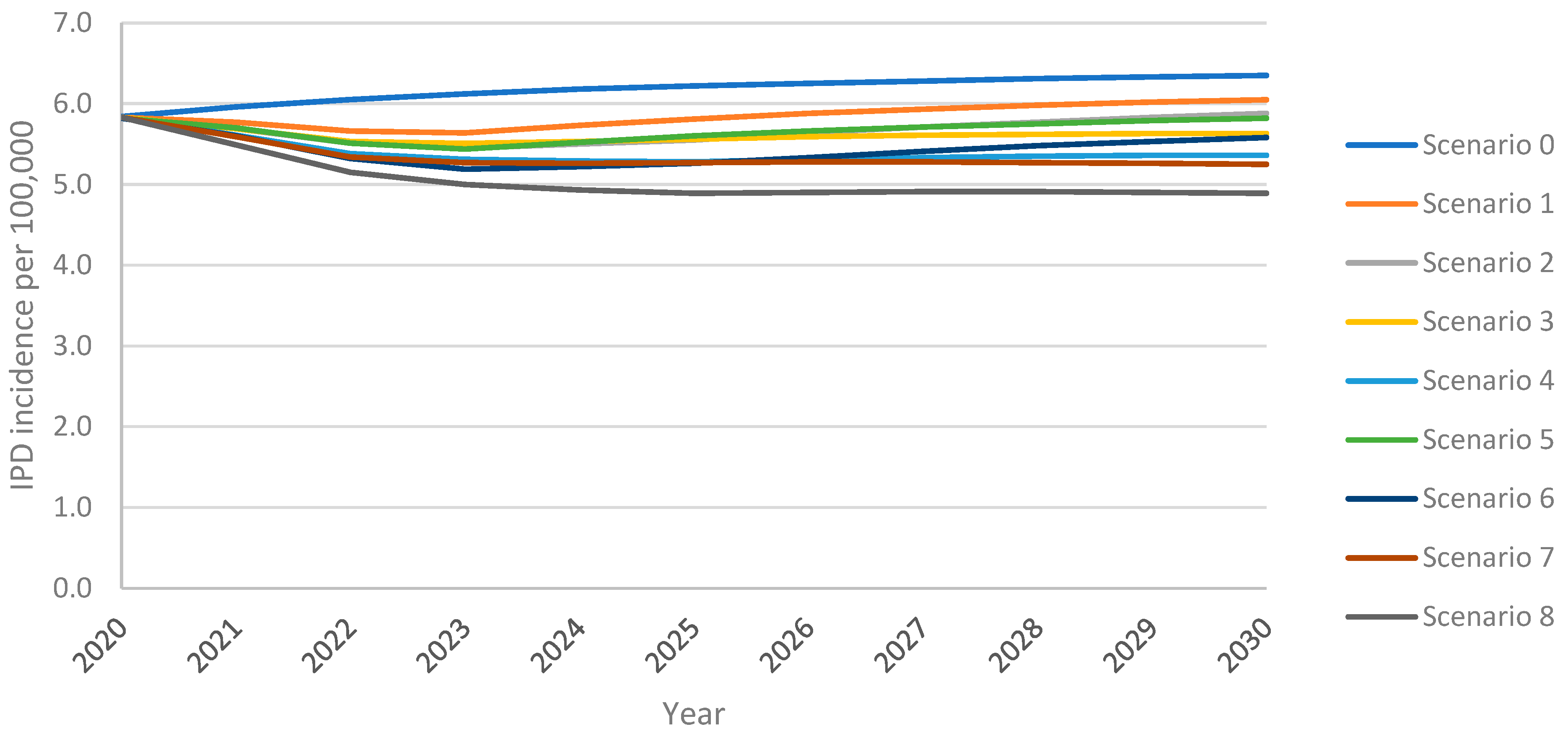
3.1. Invasive Pneumococcal Disease
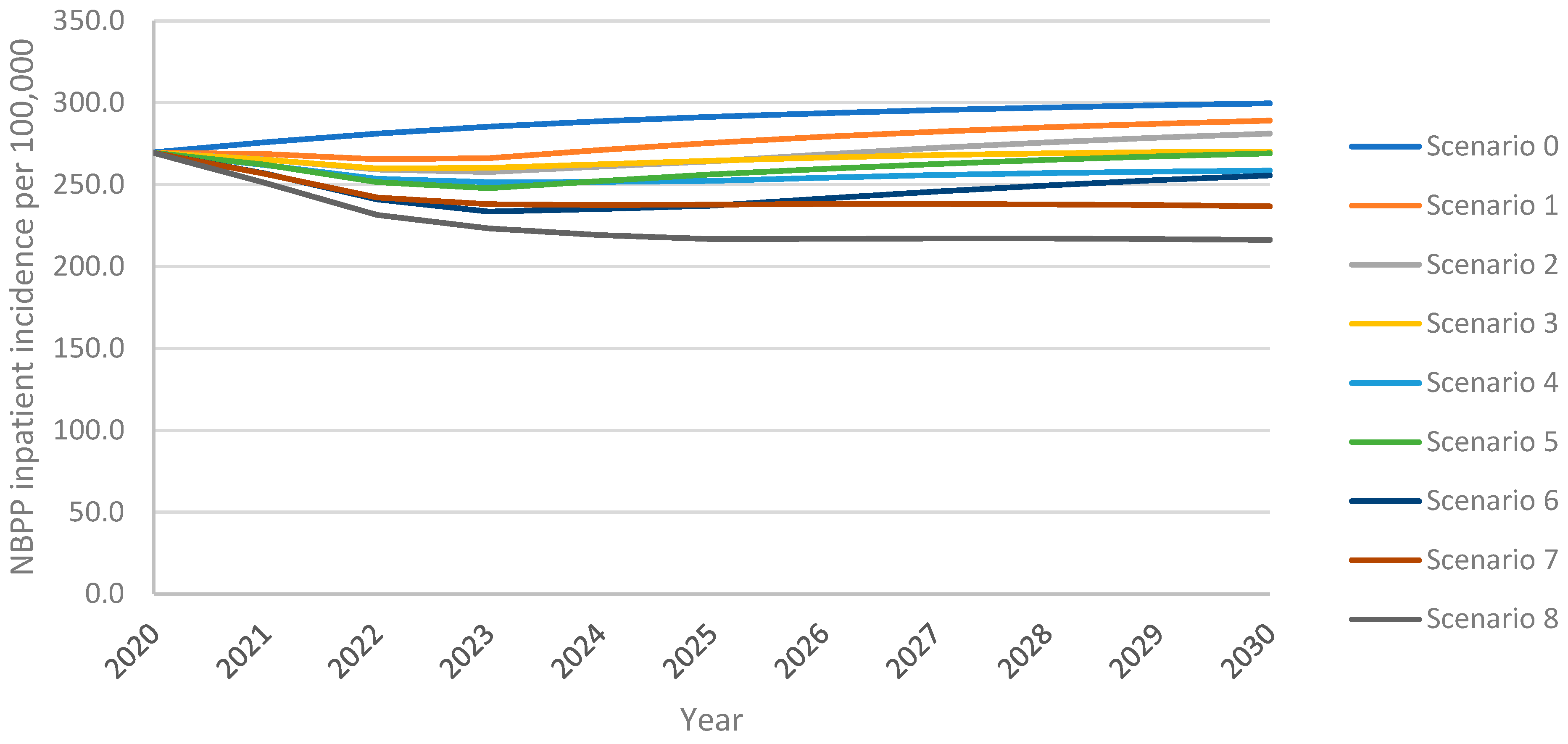
3.2. Non-Bacteremic Pneumococcal Pneumonia—Inpatient Cases
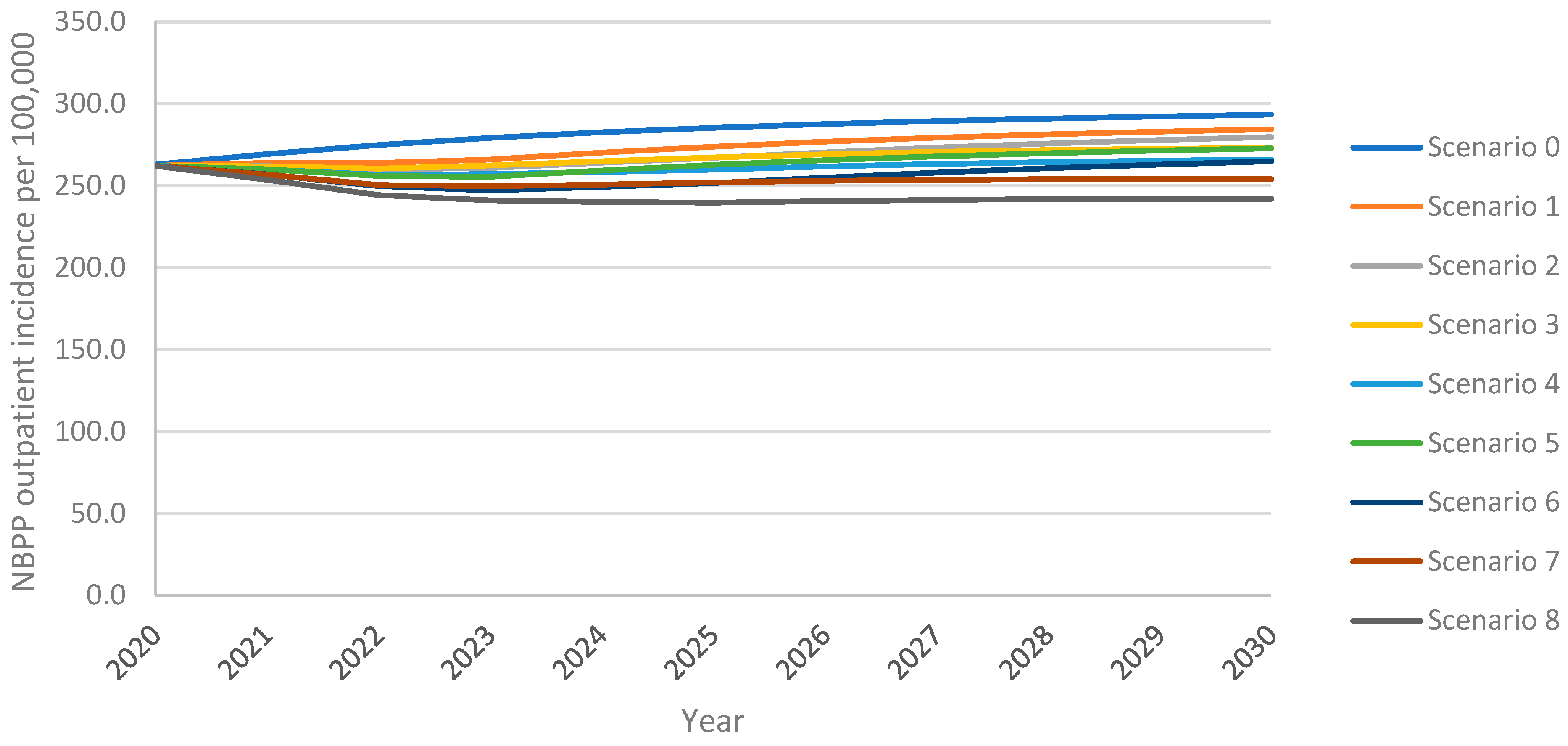
3.3. Non-Bacteremic Pneumococcal Pneumonia—Outpatient Cases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deb, A.; Podmore, B.; Barnett, R.; Beier, D.; Galetzka, W.; Qizilbash, N.; Haeckl, D.; Mihm, S.; Johnson, K.D.; Weiss, T. Clinical and economic burden of pneumococcal disease among individuals aged 16 years and older in Germany. Epidemiol. Infect. 2022, 150, e204. [Google Scholar] [CrossRef] [PubMed]
- Musher, D.M.; Anderson, R.; Feldman, C. The remarkable history of pneumococcal vaccination: An ongoing challenge. Pneumonia 2022, 14, 5. [Google Scholar] [CrossRef] [PubMed]
- US Centers for Disease Control and Prevention. Pneumococcal Disease. Available online: https://www.cdc.gov/pneumococcal/vaccines/types.html (accessed on 4 January 2025).
- Htar, M.T.T.; Christopoulou, D.; Schmitt, H.J. Pneumococcal serotype evolution in Western Europe. BMC Infect. Dis. 2015, 15, 419. [Google Scholar] [CrossRef]
- Rieck, T.; Steffen, A.; Feig, M.; Rau, C. Impfquoten in Deutschland–aktuelle Ergebnisse aus dem RKI-Impfquotenmonitoring. Epidemiol. Bull. 2024, 50, 3–10. [Google Scholar] [CrossRef]
- Schlaberg, J.; Vygen-Bonnet, S.; Falman, A.; Wilhelm, J.; Hummers, E.; von Kries, R.; Ledig, T.; Bogdan, C. Aktualisierung der Empfehlungen der STIKO zur Standardimpfung von Personen ≥ 60 Jahre Sowie zur Indikationsimpfung von Risikogruppen Gegen Pneumokokken und Die Dazugehörige Wissenschaftliche Begründung. 2023. Available online: https://edoc.rki.de/handle/176904/11307.2 (accessed on 17 March 2025).
- van der Linden, M.; Imöhl, M.; Perniciaro, S. Limited indirect effects of an infant pneumococcal vaccination program in an aging population. PLoS ONE 2019, 14, e0220453. [Google Scholar] [CrossRef]
- Kuchenbecker, U.; Chase, D.; Reichert, A.; Schiffner-Rohe, J.; Atwood, M. Estimating the cost-effectiveness of a sequential pneumococcal vaccination program for adults in Germany. PLoS ONE 2018, 13, e0197905. [Google Scholar] [CrossRef]
- Perniciaro, S.; van der Linden, M. Pneumococcal vaccine uptake and vaccine effectiveness in older adults with invasive pneumococcal disease in Germany: A retrospective cohort study. Lancet Reg. Health–Eur. 2021, 7, 100126. [Google Scholar] [CrossRef]
- Malik, T.M.; Bakker, K.M.; Oidtman, R.J.; Sharomi, O.; Meleleo, G.; Nachbar, R.B.; Elbasha, E.H. A dynamic transmission model for assessing the impact of pneumococcal vaccination in the United States. PLoS ONE 2025, 20, e0305892. [Google Scholar] [CrossRef]
- Perniciaro, S.; van der Linden, M.; Weinberger, D.M. Reemergence of invasive pneumococcal disease in Germany during the spring and summer of 2021. Clin. Infect. Dis. 2022, 75, 1149–1153. [Google Scholar] [CrossRef]
- Kellaher, C. Merck Gets European Commission Approval of Capvaxive Vaccine. Available online: https://www.morningstar.com/news/dow-jones/202503263462/merck-gets-european-commission-approval-of-capvaxive-vaccine (accessed on 26 March 2025).
- Oidtman, R.J.; Meleleo, G.J.; Sharomi, O.; Matthews, I.; Ntais, D.; Nachbar, R.; Malik, T.; Bakker, K.M. Modeling the epidemiological impact of different adult pneumococcal vaccination strategies in the United Kingdom. Infect. Dis. Ther. 2025, 14, 587–602. [Google Scholar] [CrossRef]
- Prem, K.; Cook, A.R.; Jit, M. Projecting social contact matrices in 152 countries using contact surveys and demographic data. PLoS Comput. Biol. 2017, 13, e1005697. [Google Scholar] [CrossRef] [PubMed]
- Benfield, T.; Skovgaard, M.; Schønheyder, H.C.; Knudsen, J.D.; Bangsborg, J.; Østergaard, C.; Slotved, H.-C.; Konradsen, H.B.; Thomsen, R.W.; Lambertsen, L. Serotype distribution in non-bacteremic pneumococcal pneumonia: Association with disease severity and implications for pneumococcal conjugate vaccines. PLoS ONE 2013, 8, e72743. [Google Scholar] [CrossRef] [PubMed]
- Pletz, M.W.; Ewig, S.; Rohde, G.; Schuette, H.; Rupp, J.; Welte, T.; Suttorp, N.; Forstner, C.; Group, C.S. Impact of pneumococcal vaccination in children on serotype distribution in adult community-acquired pneumonia using the serotype-specific multiplex urinary antigen detection assay. Vaccine 2016, 34, 2342–2348. [Google Scholar] [CrossRef]
- van der Linden, M. Internal data on an ongoing IPD-surveillance in Germany, data on file. 2024. [Google Scholar]
- Cleary, D.W.; Jones, J.; Gladstone, R.A.; Osman, K.L.; Devine, V.T.; Jefferies, J.M.; Bentley, S.D.; Faust, S.N.; Clarke, S.C. Changes in serotype prevalence of Streptococcus pneumoniae in Southampton, UK between 2006 and 2018. Sci. Rep. 2022, 12, 13332. [Google Scholar] [CrossRef]
- Savulescu, C.; Krizova, P.; Valentiner-Branth, P.; Ladhani, S.; Rinta-Kokko, H.; Levy, C.; Mereckiene, J.; Knol, M.; Winje, B.A.; Ciruela, P. Effectiveness of 10 and 13-valent pneumococcal conjugate vaccines against invasive pneumococcal disease in European children: SpIDnet observational multicentre study. Vaccine 2022, 40, 3963–3974. [Google Scholar] [CrossRef]
- Whitney, C.G.; Pilishvili, T.; Farley, M.M.; Schaffner, W.; Craig, A.S.; Lynfield, R.; Nyquist, A.C.; Gershman, K.A.; Vazquez, M.; Bennett, N.M.; et al. Effectiveness of seven-valent pneumococcal conjugate vaccine against invasive pneumococcal disease: A matched case-control study. Lancet 2006, 368, 1495–1502. [Google Scholar] [CrossRef]
- Moore, M.R.; Link-Gelles, R.; Schaffner, W.; Lynfield, R.; Holtzman, C.; Harrison, L.H.; Zansky, S.M.; Rosen, J.B.; Reingold, A.; Scherzinger, K.; et al. Effectiveness of 13-valent pneumococcal conjugate vaccine for prevention of invasive pneumococcal disease in children in the USA: A matched case-control study. Lancet Respir. Med. 2016, 4, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Lewnard, J.A.; Givon-Lavi, N.; Dagan, R. Effectiveness of pneumococcal conjugate vaccines against community-acquired alveolar pneumonia attributable to vaccine-serotype Streptococcus pneumoniae among children. Clin. Infect. Dis. 2021, 73, e1423–e1433. [Google Scholar] [CrossRef] [PubMed]
- Ryman, J.; Weaver, J.; Yee, K.L.; Sachs, J.R. Predicting effectiveness of the V114 vaccine against invasive pneumococcal disease in children. Expert Rev. Vaccines 2022, 21, 1515–1521. [Google Scholar] [CrossRef]
- Bonten, M.J.; Huijts, S.M.; Bolkenbaas, M.; Webber, C.; Patterson, S.; Gault, S.; van Werkhoven, C.H.; van Deursen, A.M.; Sanders, E.A.; Verheij, T.J.; et al. Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. N. Engl. J. Med. 2015, 372, 1114–1125. [Google Scholar] [CrossRef]
- Andrews, N.J.; Waight, P.A.; George, R.C.; Slack, M.P.; Miller, E. Impact and effectiveness of 23-valent pneumococcal polysaccharide vaccine against invasive pneumococcal disease in the elderly in England and Wales. Vaccine 2012, 30, 6802–6808. [Google Scholar] [CrossRef]
- Suzuki, M.; Dhoubhadel, B.G.; Ishifuji, T.; Yasunami, M.; Yaegashi, M.; Asoh, N.; Ishida, M.; Hamaguchi, S.; Aoshima, M.; Ariyoshi, K. Serotype-specific effectiveness of 23-valent pneumococcal polysaccharide vaccine against pneumococcal pneumonia in adults aged 65 years or older: A multicentre, prospective, test-negative design study. Lancet Infect. Dis. 2017, 17, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Leidner, A.J. Summary of Three Economic Models Assessing Pneumococcal Vaccines in US Adults. 2021. Available online: https://stacks.cdc.gov/view/cdc/110717/cdc_110717_DS1.pdf (accessed on 17 March 2025).
- Bonten, M.J.; Huijts, S.M.; Bolkenbaas, M. Vaccine against pneumococcal pneumonia in adults. N. Engl. J. Med. 2015, 373, 93. [Google Scholar] [PubMed]
- Federal Statistic Bureau of Germany. Births. 2022. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Geburten/_inhalt.html#234040 (accessed on 4 December 2024).
- Federal Statistic Bureau of Germany. Deaths, Excluding Stillbirths, Subsequently Registered War Deaths, and Legal Declarations of Death. 2022. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Sterbefaelle-Lebenserwartung/_inhalt.html#234182 (accessed on 4 December 2024).
- De Miguel, S.; Latasa, P.; Yuste, J.; García, L.; Ordobás, M.; Ramos, B.; Pérez, M.; Ortiz, M.A.; Sanz, J.C. Age-dependent serotype-associated case-fatality rate in invasive pneumococcal disease in the autonomous community of madrid between 2007 and 2020. Microorganisms 2021, 9, 2286. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Podmore, B.; Barnett, R.; Beier, D.; Galetzka, W.; Qizilbash, N.; Heckl, D.; Boellisnger, T.; Weaver, J. Healthcare resource utilization and cost of pneumococcal disease in children in Germany, 2014–2019: A retrospective cohort study. Pneumonia 2023, 15, 7. [Google Scholar] [CrossRef]
- Destatis Statistisches Bundesamt. 4 Million More People Aged 67 or over Will Live in Germany in 2035. 2022. Available online: https://www.destatis.de/EN/Press/2022/12/PE22_511_124.html (accessed on 17 March 2025).
- Hethcote, H.W. The mathematics of infectious diseases. SIAM Rev. 2000, 42, 599–653. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Serotype Class | Serotypes Included in Class | Description | PCV7 | PCV13 | PCV15 | PCV20 | V116 | PPSV23 |
|---|---|---|---|---|---|---|---|---|
| 1 | 4, 6B, 9V, 14, 18C, 19F, 23F | PCV7 ST | ||||||
| 2 | 1, 5 | PCV13 ST minus 3, 6A, 7F, & 19A | ||||||
| 3 | 3 | ST3 | ||||||
| 4 | 7F, 19A | Additional PCV13 ST | ||||||
| 5 | 6A, 6C | Additional PCV13 ST + 6C cross protection | ||||||
| 6 | 22F, 33F | Additional PCV15 ST | ||||||
| 7 | 9N, 17F, 20 | Additional PPSV23 ST includes STC1–4, 6–9 | ||||||
| 8 | 8, 10A, 11A, 12F | Additional PCV20 ST includes STC1–7, 10 | ||||||
| 9 | 15B | Additional PCV20 ST | ||||||
| 10 | 15A, 15C, 16F, 23A, 23B, 24F, 31, 35B | Additional V116 ST excludes STC1–2, 10 | ||||||
| 11 | (NVTs) | NVTs |
| Parameter | Value | Source |
|---|---|---|
| Demographic model component | ||
| Fertility rate | Varies | [29] |
| Mortality rate | Varies | [30] |
| Aging rate | Varies | Calculated |
| Contact mixing rate | Varies | [14] |
| Transmission model component | ||
| Case fatality rates | ||
| IPD (all serotype groups) | 0–5 years: 1.46% 5–18 years: 1.68% 18–50 years: 4.62% 50–60 years: 12.48% 60+ years: 15.73% | [31] |
| NBPP (deaths per 100 cases) | 0–16 years: 0 16–50 years: 4.42 50–60 years: 10.95 60–70 years: 14.10 70+ years: 20.36 | 0–16 years: assumption 16+ years: [1] |
| NBPP case distribution | ||
| Inpatient | 0–16 years: 41.4% 16–50 years: 20.9% 50–60 years: 34.2% 60+ years: 64.7% | [32] |
| Outpatient | 0–16 years: 58.6% 16–50 years: 79.1% 50–60 years: 65.8% 60+ years: 35.3% | [32] |
| Historic vaccination coverage | ||
| Pediatric PCV (ages 0–2 years) | 2006: 20% 2007: 50% 2008: 67% 2009: 69% 2010: 71% 2011: 71% 2012: 72% 2013: 71% 2014: 70% 2015: 68% 2016: 70% 2017: 71% 2018: 73% 2019: 75% | [5] |
| Adult PPSV23 (ages 60+ years) | 1998–2015: 22% 2016: 24% 2017: 26% 2018: 28% 2019: 30% | [5] |
| Vaccine effectiveness | ||
| PCV vaccines (ages 60+ years) | Serotype 3: 26% All other covered serotypes: 75% | [19] |
| PPSV23 (ages 60+ years) | Varies by serotype | [25] |
| Vaccine duration of protection | ||
| PCV vaccines | 10 years | [27] |
| PPSV23 | 7.5 years | [28] |
| Scenario | Vaccine | Uptake | Revaccination |
|---|---|---|---|
| Scenario 0 | PPSV23 | 30% | - |
| Scenario 1 | PCV20 | 30% | - |
| Scenario 2 | PCV20 | 30% | 50% |
| Scenario 3 | PCV20 | 60% | - |
| Scenario 4 | PCV20 | 60% | 50% |
| Scenario 5 | V116 | 30% | - |
| Scenario 6 | V116 | 30% | 50% |
| Scenario 7 | V116 | 60% | - |
| Scenario 8 | V116 | 60% | 50% |
| Clinical Outcome | Without Revaccination | With 50% Revaccination | ||
|---|---|---|---|---|
| PCV20 | V116 | PCV20 | V116 | |
| 30% VCR | ||||
| Averted IPD cases | 2856 | 4388 | 4404 | 6433 |
| Averted NBPP inpatient cases | 110,338 | 247,963 | 178,240 | 362,519 |
| Averted NBPP outpatient cases | 84,116 | 163,808 | 125,244 | 230,647 |
| 60% VCR | ||||
| Averted IPD cases | 4820 | 6996 | 6631 | 9410 |
| Averted NBPP inpatient cases | 196,688 | 394,477 | 276,063 | 530,681 |
| Averted NBPP outpatient cases | 136,264 | 249,109 | 184,334 | 328,491 |
| Age Group | Without Revaccination | With Revaccination | |||
|---|---|---|---|---|---|
| PPSV23 | PCV20 | V116 | PCV20 | V116 | |
| 30% VCR | |||||
| 18–50 | 5846 | 5632 | 5596 | 5597 | 5558 |
| 50–60 | 7660 | 7416 | 7371 | 7361 | 7311 |
| 60+ | 29,587 | 27,189 | 25,738 | 25,731 | 23,791 |
| Total adult | 43,093 | 40,237 | 38,705 | 38,689 | 36,660 |
| 60% VCR | |||||
| 18–50 | N/A | 5589 | 5549 | 5549 | 5505 |
| 50–60 | 7349 | 7296 | 7286 | 7226 | |
| 60+ | 25,335 | 23,252 | 23,627 | 20,952 | |
| Total adult | 38,273 | 36,097 | 36,462 | 33,683 | |
| Age Group | Without Revaccination | With Revaccination | |||
|---|---|---|---|---|---|
| PPSV23 | PCV20 | V116 | PCV20 | V116 | |
| 30% VCR | |||||
| 18–50 | 131,842 | 126,244 | 125,156 | 125,374 | 124,239 |
| 50–60 | 121,560 | 117,393 | 116,618 | 116,483 | 115,636 |
| 60+ | 1,632,982 | 1,532,409 | 1,396,647 | 1,466,287 | 1,283,990 |
| Total adult | 1,886,384 | 1,776,046 | 1,638,421 | 1,708,144 | 1,523,865 |
| 60% VCR | |||||
| 18–50 | N/A | 125,171 | 124,023 | 124,154 | 122,951 |
| 50–60 | 116,267 | 115,399 | 115,209 | 114,250 | |
| 60+ | 1,448,258 | 1,252,485 | 1,370,958 | 1,118,502 | |
| Total adult | 1,689,696 | 1,491,907 | 1,610,321 | 1,355,703 | |
| Age Group | Without Revaccination | With Revaccination | |||
|---|---|---|---|---|---|
| PPSV23 | PCV20 | V116 | PCV20 | V116 | |
| 30% VCR | |||||
| 18–50 | 500,020 | 478,789 | 474,663 | 475,488 | 471,183 |
| 50–60 | 233,552 | 225,545 | 224,057 | 223,797 | 222,170 |
| 60+ | 891,036 | 836,158 | 762,080 | 800,079 | 700,608 |
| Total adult | 1,624,608 | 1,540,492 | 1,460,800 | 1,499,364 | 1,393,961 |
| 60% VCR | |||||
| 18–50 | N/A | 474,719 | 470,366 | 470,860 | 466,299 |
| 50–60 | 223,384 | 221,715 | 221,351 | 219,508 | |
| 60+ | 790,241 | 683,418 | 748,063 | 610,310 | |
| Total adult | 1,488,344 | 1,375,499 | 1,440,274 | 1,296,117 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharomi, O.; de Lepper, M.; Mihm-Sippel, S.; Reuter, T.; Solleder, C.; Meleleo, G.; Malik, T.M.; Bakker, K.M.; Oidtman, R.J. Epidemiological Impact of Increasing Vaccination Coverage Rate and Re-Vaccination on Pneumococcal Disease in Older Adults in Germany. Vaccines 2025, 13, 475. https://doi.org/10.3390/vaccines13050475
Sharomi O, de Lepper M, Mihm-Sippel S, Reuter T, Solleder C, Meleleo G, Malik TM, Bakker KM, Oidtman RJ. Epidemiological Impact of Increasing Vaccination Coverage Rate and Re-Vaccination on Pneumococcal Disease in Older Adults in Germany. Vaccines. 2025; 13(5):475. https://doi.org/10.3390/vaccines13050475
Chicago/Turabian StyleSharomi, Oluwaseun, Marion de Lepper, Sarah Mihm-Sippel, Thorsten Reuter, Claudia Solleder, Giulio Meleleo, Tufail M. Malik, Kevin M. Bakker, and Rachel J. Oidtman. 2025. "Epidemiological Impact of Increasing Vaccination Coverage Rate and Re-Vaccination on Pneumococcal Disease in Older Adults in Germany" Vaccines 13, no. 5: 475. https://doi.org/10.3390/vaccines13050475
APA StyleSharomi, O., de Lepper, M., Mihm-Sippel, S., Reuter, T., Solleder, C., Meleleo, G., Malik, T. M., Bakker, K. M., & Oidtman, R. J. (2025). Epidemiological Impact of Increasing Vaccination Coverage Rate and Re-Vaccination on Pneumococcal Disease in Older Adults in Germany. Vaccines, 13(5), 475. https://doi.org/10.3390/vaccines13050475