
Modelling the Cost-Effectiveness of Hepatitis A in South Africa

 ,
,
Abstract
1. Introduction
Background
2. Methods
2.1. Transmission Model
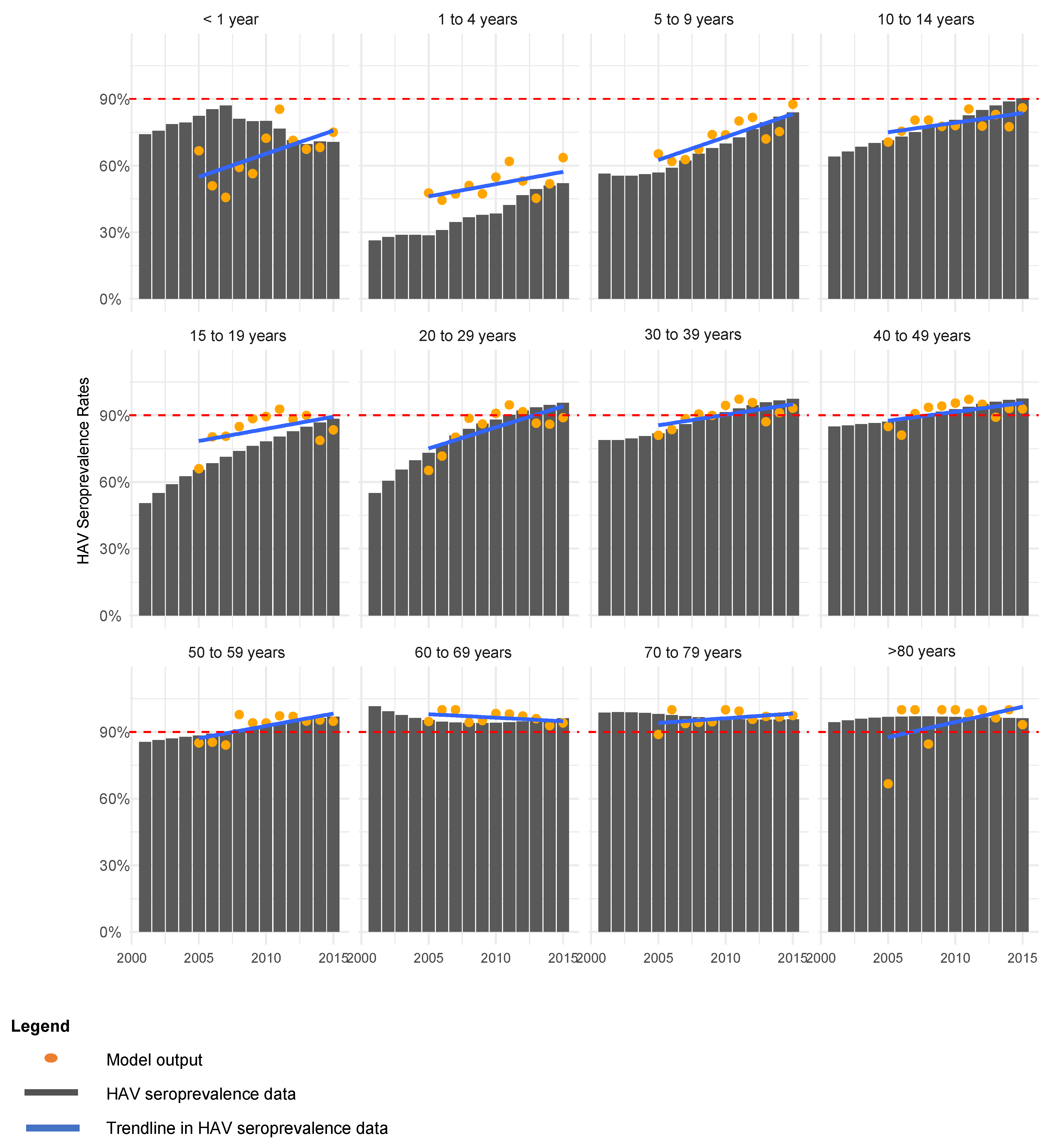
2.2. Model Calibration
- Seroprevalence below 90% for individuals < 20 years old between 2005–2015; and
- Seroprevalence to only reach ≥90% in individuals 20–29 years old in 2011 and 2012; and
- Seroprevalence below 60% for individuals < 5 years old after 2012.
2.3. Scenario Analyses
2.4. Estimation of Hepatitis A Treatment and Routine Immunization Costs

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cost | Cost (USD 2020) | Source |
|---|---|---|
| Outpatient treatment of hepatitis A cases in patients < 15 years | USD 177.88 | Patterson et al., 2022 [21] |
| Outpatient treatment of hepatitis A cases in patients ≥ 15 years old | USD 264.94 | Patterson et al., 2022 [21] |
| Inpatient treatment of hepatitis A cases in patients < 15 years | USD 1856.79 | Patterson et al., 2022 [21] |
| Inpatient treatment of hepatitis A cases in patients ≥ 15 years old | USD 6382.37 | Patterson et al., 2022 [21] |
| Inpatient treatment of liver transplant patients < 15 years | USD 11,337.14 | Calculated value based on PDE and LOS |
| Inpatient treatment of liver transplant patients ≥ 15 years old | USD 21,329.20 | Calculated value based on PDE and LOS |
| Liver transplant procedure (all ages) | USD 1787.74 | UPFS 2020 [32] |
| Dose of paediatric hepatitis A vaccine | USD 19.71 | MedicinePrices.org [33] |
| Clinic visit for vaccine administration | USD 136.15 | Massyn et al., 2020 [34] |
| Variable | Value | Source |
|---|---|---|
| DW outpatient hepatitis A cases | 0.051 | GBD 2018 [35] |
| DW hospitalized hepatitis A cases | 0.133 | GBD 2018 [35] |
| DW liver transplant | 0.54 | GBD 2018 [35] |
| YLD hepatitis A outcomes, excluding liver failure (days) | 21 | Johns Hopkins 2021 [23] |
| YLD liver transplant (days) | 180 | Johns Hopkins 2021 [23] |
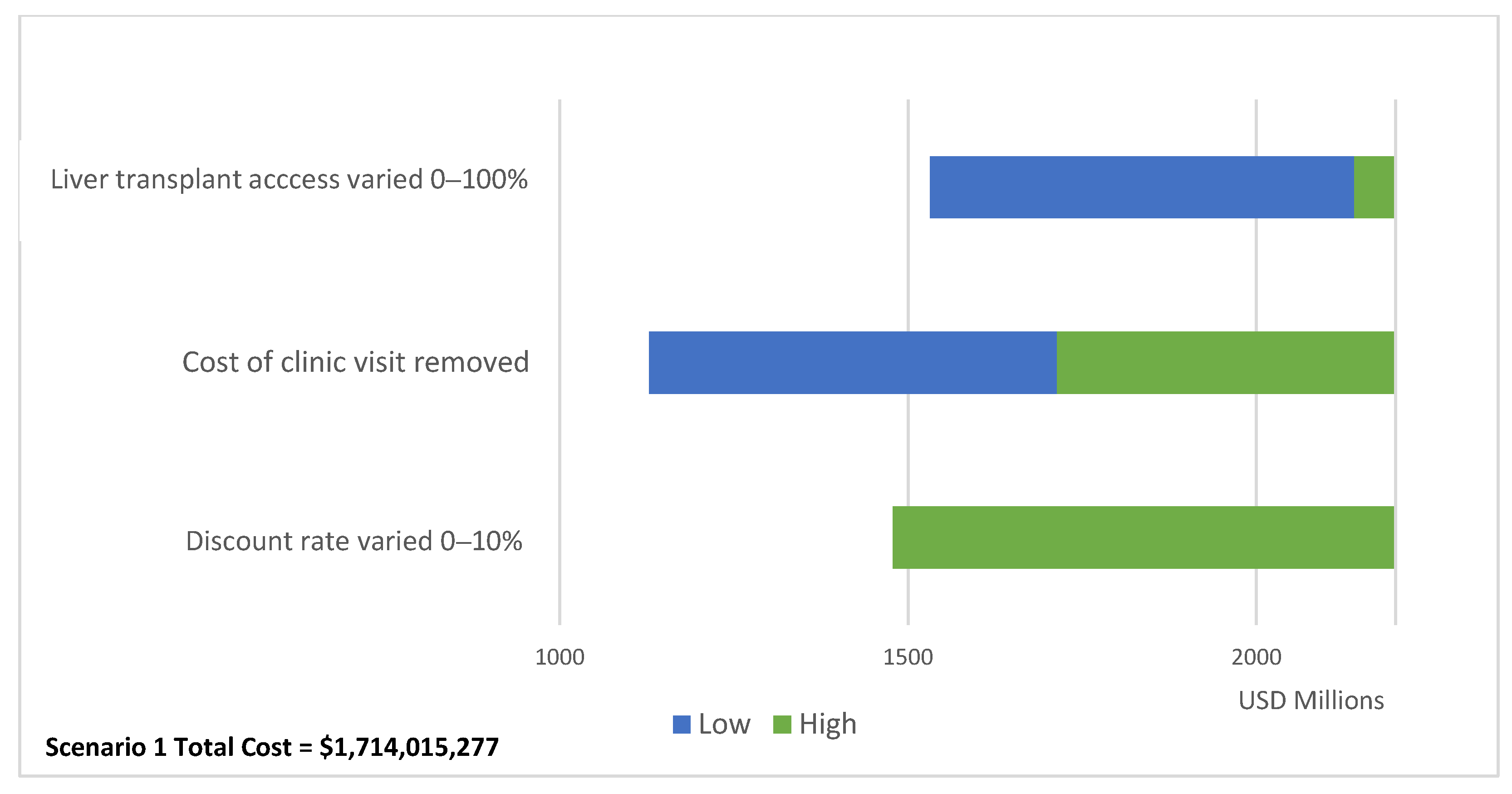
2.5. Sensitivity Analyses
- Remove the costs of clinic visits for vaccine administration (USD 136.15);
- Vary the access to liver transplant procedures to 0% and 100%;
- Vary the discount rate between 0% and 10%.
3. Results
3.1. Baseline Scenario
3.2. Cost-Effectiveness of Vaccination
3.3. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jacobsen, K.H.; Wiersma, S.T. Hepatitis A virus seroprevalence by age and world region, 1990 and 2005. Vaccine 2010, 28, 6653–6657. [Google Scholar] [CrossRef] [PubMed]
- Mazanderani, A.H.; Motaze, N.V.; McCarthy, K.; Suchard, M.; du Plessis, N.M. Hepatitis A Virus Seroprevalence in South Africa—Estimates Using Routine Laboratory Data, 2005–2015. PLoS ONE 2019, 14, e0216033. [Google Scholar] [CrossRef] [PubMed]
- Suwantika, A.A.; Yegenoglu, S.; Riewpaiboon, A.; Tu, H.-A.T.; Postma, M.J. Economic evaluations of hepatitis A vaccination in middle-income countries. Expert Rev. Vaccines 2013, 12, 1479–1494. [Google Scholar] [CrossRef]
- Sartori, A.M.C.; de Soárez, P.C.; Novaes, H.M.D. Cost-effectiveness of introducing the 10-valent pneumococcal conjugate vaccine into the universal immunisation of infants in Brazil. J. Epidemiol. Community Health 2010, 66, 210–217. [Google Scholar] [CrossRef]
- Quezada, A.; Baron-Papillon, F.; Coudeville, L.; Maggi, L. Universal vaccination of children against hepatitis a in Chile: A cost-effectiveness study. Rev. Panam. De Salud Pública 2008, 23, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Lopez, E.; Debbag, R.; Coudeville, L.; Baron-Papillon, F.; Armoni, J. The cost-effectiveness of universal vaccination of children against hepatitis A in Argentina: Results of a dynamic health–economic analysis. J. Gastroenterol. 2007, 42, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, M.T.; Jacobs, R.J.; Arteaga, O.; Navarrete, M.S.; Meyerhoff, A.S.; Innis, B.L. Cost-effectiveness of universal child-hood hepatitis A vaccination in Chile. Vaccine 2005, 23, 4110–4119. [Google Scholar] [CrossRef] [PubMed]
- Van Effelterre, T.P.; DeAntonio, R.; Cassidy, A.; Romano-Mazzotti, L.; Marano, C. Model-based projections of the population-level impact of hepatitis A vaccination in Mexico. Hum. Vaccines Immunother. 2012, 8, 1099–1108. [Google Scholar] [CrossRef]
- Van Effelterre, T.; Marano, C.; Jacobsen, K.H. Modeling the hepatitis A epidemiological transition in Thailand. Vaccine 2016, 34, 555–562. [Google Scholar] [CrossRef]
- Van Effelterre, T.; Guignard, A.; Marano, C.; Rojas, R.; Jacobsen, K.H. Modeling the hepatitis A epidemiological transition in Brazil and Mexico. Hum. Vaccines Immunother. 2017, 13, 1942–1951. [Google Scholar] [CrossRef]
- Suwantika, A.A.; Beutels, P.; Postma, M.J. Cost-effectiveness of hepatitis A vaccination in Indonesia. Hum. Vaccines Immunother. 2014, 10, 2342–2349. [Google Scholar] [CrossRef]
- Ellis, A.; Rüttimann, R.W.; Jacobs, R.J.; Meyerhoff, A.S.; Innis, B.L. Cost-effectiveness of childhood hepatitis A vaccination in Argentina: A second dose is warranted. Pan Am. J. Public Health 2007, 21, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Prem, K.; Cook, A.R.; Jit, M. Projecting social contact matrices in 152 countries using contact surveys and demographic data. PLoS Comput. Biol. 2017, 13, e1005697. [Google Scholar] [CrossRef] [PubMed]
- Prabdial-Sing, N.; Motaze, V.; Manamela, J.; McCarthy, K.; Suchard, M. Establishment of Outbreak Thresholds for Hepatitis A in South Africa Using Laboratory Surveillance, 2017–2020. Viruses 2021, 13, 2470. [Google Scholar] [CrossRef] [PubMed]
- Camurdan, A.D.; Beyazova, U.; Bozdayı, G.; Civil, F.; Kocak, A.A.; Guzelkucuk, Z. Waning Time of Maternally Derived Anti-Hepatitis A and Anti-Varicella Zoster Virus Antibodies. J. Pediatr. Infect. Dis. 2019, 14, 116–120. [Google Scholar] [CrossRef]
- Foster, M.A.; Haber, P.; Nelson, N.P. Hepatitis A; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021.
- Canuel, M.; De Serres, G.; Duval, B.; Gilca, R.; De Wals, P.; Gilca, V. Trends of Hepatitis A hospitalization and risk factors in Quebec, Canada, between 1990 and 2003. BMC Infect. Dis. 2007, 7, 31. [Google Scholar] [CrossRef] [PubMed]
- Keles, E.; Hassan-Kadle, M.A.; Osman, M.M.; Eker, H.H.; Abusoglu, Z.; Baydili, K.N.; Osman, A.M. Clinical characteristics of acute liver failure associated with hepatitis A infection in children in Mogadishu, Somalia: A hospital-based retrospective study. BMC Infect. Dis. 2021, 21, 890. [Google Scholar] [CrossRef]
- Jiang, Q.-Q.; Han, M.-F.; Ma, K.; Chen, G.; Wan, X.-Y.; Kilonzo, S.B.; Wu, W.-Y.; Wang, Y.-L.; You, J.; Ning, Q. Acute kidney injury in acute-on-chronic liver failure is different from in decompensated cirrhosis. World J. Gastroenterol. 2018, 24, 2300–2310. [Google Scholar] [CrossRef]
- Mendizabal, M.; Silva, M.O. Liver transplantation in acute liver failure: A challenging scenario. World J. Gastroenterol. 2016, 22, 1523–1531. [Google Scholar] [CrossRef]
- Patterson, J.; Cleary, S.; Silal, S.P.; Hussey, G.D.; Enoch, A.; Korsman, S.; Goddard, E.; Setshedi, M.; Spearman, W.C.; Kagina, B.M.; et al. A retrospective study assessing the clinical outcomes and costs of acute hepatitis A in Cape Town, South Africa. BMC Infect. Dis. 2022, 22, 45. [Google Scholar] [CrossRef]
- Allen, A.M.; Kim, W.R.; Moriarty, J.P.; Shah, N.D.; Larson, J.J.; Kamath, P.S. Time trends in the health care burden and mor-tality of acute on chronic liver failure in the United States. Hepatology 2016, 64, 2165–2172. [Google Scholar] [CrossRef] [PubMed]
- John Hopkins Medicine. Hepatitis A; John Hopkins Medical University: Baltimore, MD, USA, 2022; Available online: https://www.hopkinsmedicine.org/health/conditions-and-diseases/hepatitis/hepatitis-a (accessed on 1 June 2022).
- Kuodi, P.; Patterson, J.; Silal, S.; Hussey, G.D.; Kagina, B.M. Characterisation of the environmental presence of hepatitis A virus in low-income and middle-income countries: A systematic review and meta-analysis. BMJ Open 2020, 10, e036407. [Google Scholar] [CrossRef] [PubMed]
- Venter, J.M.; van Heerden, J.; Vivier, J.C.; Grabow, W.O.; Taylor, M.B. Hepatitis A virus in surface water in South Africa: What are the risks? J. Water Health 2007, 5, 229–240. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, United Nations Children’s Fund. South Africa: WHO and UNICEF Estimates of Immunization Coverage; World Health Organization; World Health Organization, United Nations Children’s Fund: New York, NY, USA, 2019. [Google Scholar]
- Irving, G.; Holden, J.; Yang, R.; Pope, D. Hepatitis A immunisation in persons not previously exposed to hepatitis A. Cochrane Database Syst. Rev. 2012, 2012, CD009051. [Google Scholar] [CrossRef]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS)—Explanation and elaboration: A report of the ISPOR health economic evaluation publication guidelines good reporting practices task force. Value Health 2013, 16, 231–250. [Google Scholar] [CrossRef]
- South African Rand per US Dollar Monthly Average 2020. 2021. Available online: https://www.x-rates.com/average/?from=USD&to=ZAR&amount=1&year=2020 (accessed on 1 June 2022).
- Stats SA. Consumer Price Index; Department of Statistics South Africa: Pretoria, South Africa, 2020.
- Tovikkai, C.; Charman, S.C.; Praseedom, R.K.; Gimson, A.E.; van der Meulen, J. Time spent in hospital after liver transplantation: Effects of primary liver disease and comorbidity. World J. Transplant. 2016, 6, 743–750. [Google Scholar] [CrossRef]
- Uniform Patient Fee Schedule; Department of Health Republic of South Africa: Pretoria, South Africa, 2020.
- MedicinePrices.org. Hepatitis A: OpenUp. 2021. Available online: https://medicineprices.org.za/#search:hepatitis%20A (accessed on 1 June 2022).
- Massyn, N.; Day, C.; Ndlovu, N.; Padayachee, T. District Health Barometer 2019/2020; Health Systems Trust: Durban, South Africa, 2020. [Google Scholar]
- Network GBoDC. Global Burden of DIsease Study 2017 Disability Weights; Institute for Health Metrics and Evaluation: Seattle, WA, USA, 2018. [Google Scholar]
- Wilkinson, T.; Wilkinson, M.; MacWuilkan, K. Health Technology Assessment Methods Guide; Essential Drugs Program, National Department of Health: Cape Town, South Africa, 2021.
- Edoka, I.; Stacey, N. Estimating a cost-effectiveness threshold for health care decision-making in South Africa. Health Policy Plan. 2020, 35, 546–555. [Google Scholar] [CrossRef]
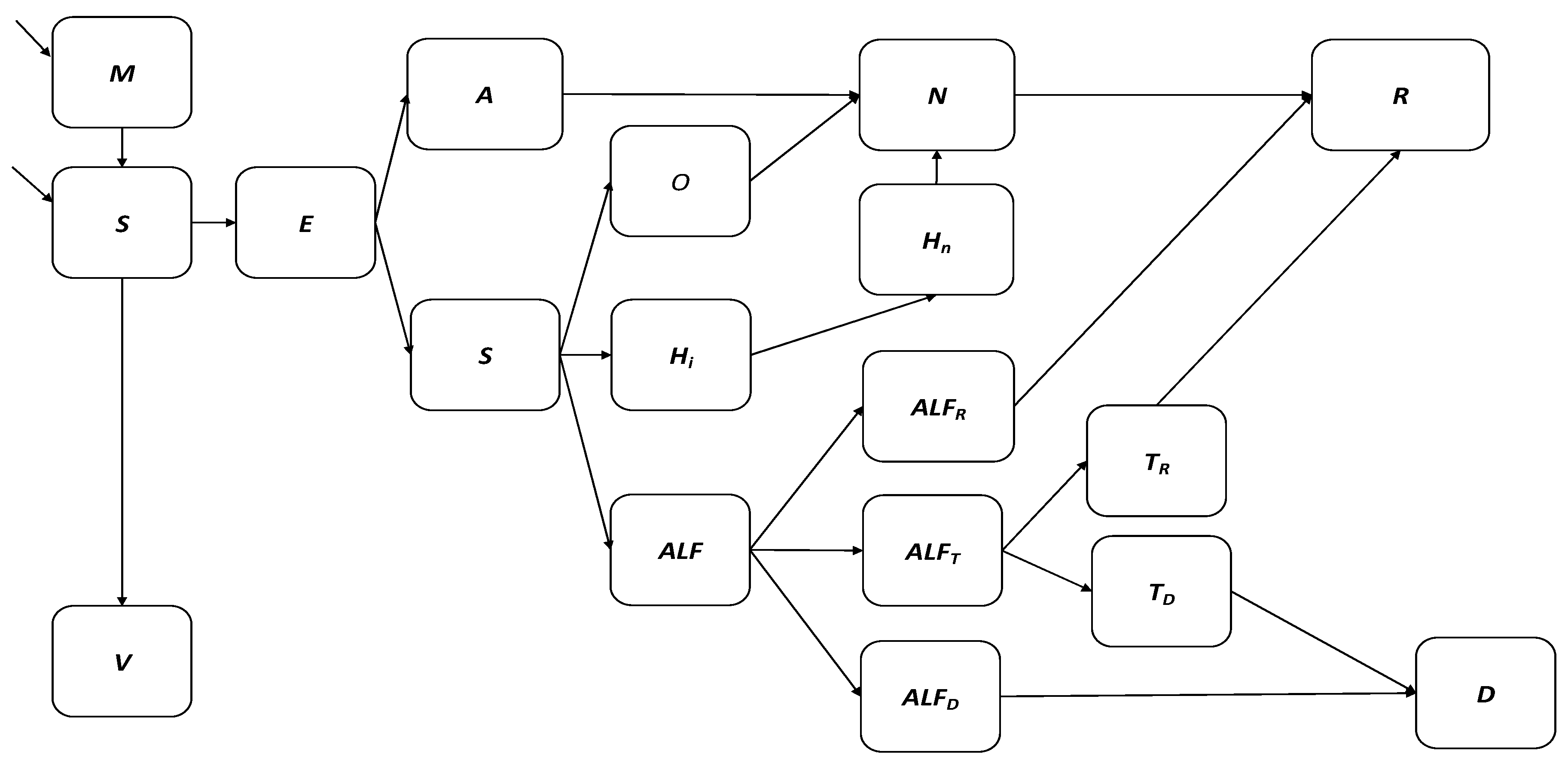

| Abbreviation | Compartment | Description |
|---|---|---|
| M | Maternal antibodies | Presence of maternally acquired anti-HAV IgG antibodies |
| S | Susceptible | No presence of anti-HAV IgG antibodies |
| E | Exposed | Exposed to the hepatitis A virus with the risk of infection |
| A | Asymptomatic | Infected with the hepatitis A virus following the incubation period |
| Sy | Symptomatic | Infected with the hepatitis A virus following the incubation period |
| O | Outpatient case | Hepatitis A case requiring outpatient care at a tertiary level facility |
| Hi | Hospitalized infectious case | Hepatitis A case requiring hospitalization at a tertiary level facility while shedding HAV |
| Hn | Hospitalized non-infectious case | Hepatitis A case requiring hospitalization at a tertiary level facility after shedding HAV |
| N | Recovering case | Hepatitis A case with waning anti-HAV IgM antibodies |
| R | Recovered and immune | Previous hepatitis A case with anti-HAV IgG antibodies developed through infection |
| ALF | Viral-induced acute liver failure | Hepatitis A case resulting in acute liver failure defined as the development of encephalopathy and synthetic function impairment following acute liver injury in an individual without pre-existing liver disease |
| ALFR | Spontaneous recovery from acute liver failure | Viral-induced acute liver case that recovers without liver transplant |
| ALFD | Death due to acute liver failure | Viral-induced acute liver case that dies due to any cause |
| ALFT | Liver transplant case | Viral-induced acute liver transplant case that requires liver transplant for recovery |
| TR | Liver transplant recovery | Viral-induced acute liver transplant case that requires and receives liver transplant |
| TD | Liver transplant death | Liver transplant case that dies due to any cause |
| D | Hepatitis A death | Hepatitis A case that dies due to any cause |
| V | Vaccinated | Vaccinated with one or two doses of hepatitis A vaccine with sufficient development of anti-HAV IgG antibodies for protection against infection |
| Parameter | Symbol | Baseline Value or Fitted Range When Stated [Uncertainty Distribution/Range] | Source |
|---|---|---|---|
| Proportion of population born with maternal anti-HAV antibodies | propM | t ≤ 2005: 0.72 t = 2006: 0.76 t = 2007: 0.79 t = 2008: 0.81 t = 2009: 0.77 t = 2010: 0.77 t = 2011: 0.76 t = 2012: 0.71 t = 2013: 0.66 t = 2014: 0.63 t ≥ 2015: 0.64 | Calculated based on annual female population aged 15–49, fertility rates for ages 15–49, age specific annual HAV seroprevalence rates for ages 15–49, and annual birth rates |
| Rate of maternal anti-HAV antibody waning (years) | tau | 1 | Guzelkucuk et al., 2019 [15] |
| Incubation period (days) | nu | 28 [15, 50] | Foster et al., 2021 [16] |
| Probability of asymptomatic hepatitis A infection in age groupi | propAi | i ≤ 6: 0.7 i ≥ 7: 0.3 | Foster et al., 2021 [16] |
| Probability of outpatient care due to hepatitis A infection in age groupi | propOi | i ≤ 12 = 0.68 13 ≥ i ≤ 14: 0.7262 15 ≥ i ≤ 16: 0.6662 17 ≥ i ≤ 19: 0.7362 | Calculated as |
| Probability of hospitalization due to hepatitis A infection in age groupi | propHi | i ≤ 12 = 0.21 13 ≥ i ≤ 14: 0.17 15 ≥ i ≤ 16: 0.23 17 ≥ i ≤ 19: 0.16 | Canuel et al., 2007 [17] |
| Probability of viral-induced acute liver failure in age groupi | propFi | i ≤ 12 = 0.11 i > 12 = 0.1038 | Keles et al., 2021 & Jiang et al., 2018 [18,19] |
| Probability of spontaneous recovery from acute liver failure in age groupi | propFri | 0.25 | Mendizabal et al., 2016 [20] |
| Probability of liver transplant due to hepatitis A infection in age groupi | propTi | 0.26 | Mendizabal et al., 2016 [20] |
| Probability of death due to acute liver failure in age groupi | propFDi | 0.49 | Mendizabal et al., 2016 [20] |
| Probability of death due to liver transplant in age groupi | propTD | 0.16 | Mendizabal et al., 2016 [20] |
| Recovery from hepatitis A infectious period (days) | gamma | 21 [14, 180] | Foster et al., 2021 [16] |
| Days for hepatitis A cases to seek care | trt | 2 [1, 3] | Patterson et al., 2022 [21] |
| Days for hospitalized hepatitis A cases to develop acute liver failure | Frate | 2 [1, 3] | Patterson et al., 2022 [21] |
| Days for acute liver failure cases to die | FDrate | 16 [1, 20] | Allen et al., 2016 [22] |
| Days for acute liver failure cases to spontaneously recover | gammaF | 21 [14, 180] | John Hopkins 2021 [23] |
| Days for acute liver failure cases to be diagnosed as liver transplant cases | Trate | 3 [1, 10] | Allen et al., 2016 [22] |
| Days for liver transplant cases to die (years) | TDrate | 1 | Based on mortality probabilities reported annually |
| Days for liver transplant cases to recover | gammaT | 21 [14, 180] | John Hopkins 2021 [23] |
| Days for hepatitis A cases to lose IgM antibodies and develop IgG antibodies marking immunity (months) | Rrate | 180 [90, 365.25] | Prabdial-Sing et al., 2021 [14] |
| Person-to-person contact scaling factor | Prel | 0.002 [0, 0.01] | Calibrated to fit national HAV seroprevalence data set |
| Person-to-environment contact scaling factor | Erel | 0.0007 [0, 0.01] | Calibrated to fit national HAV seroprevalence data set |
| Prevalence of hepatitis A in environment | PrevE | t = 2005: 0.3 [0, 1] 2005 > t ≤ 2010: 0.5 [0, 1] t > 2010: 0.8 [0, 1] | Calculated from supplementary data files associated with Kuodi et al., 2020 [24] |
| Age-specific number of infective contacts per year | betaEi | i:1= 1084.79 i:2 = 1139.04 i:3 = 813.61 i:4 = 678.02 i:5 = 542.42 i:6 = 813.66 i:7 = 542.42 i:8 = 271.29 i:9 = 105.90 i:10 = 2169.59 i:11 = 189.84 i:12 = 162.72 i:13 = 678.02 i:14 = 542.42 i:15 = 406.83 i:16 = 271.24 i:17 = 135.64 i:18 = 52.96 i:19 = 52.96 | Baseline values from Venter et al., 2007 calibrated to fit national HAV seroprevalence data set [25] |
| Scenario | Number of Vaccines Required | Symptomatic Cases Averted | Deaths Averted |
|---|---|---|---|
| 1 | 5.3 million | 136,042 [IQR: 88,842–221,483] | 31,106 [IQR: 22,975–36,742] |
| 2 | 7.8 million | 255,857 [IQR: 159,721–225,065] | 31,585 [IQR: 23,388–37,240] |
| 3 | 9.2 million | 259,318 [IQR: 162,828–477,574] | 30,982 [IQR: 22,502–37,488] |
| 4 | 11.7 million | 267,947 [IQR: 169,625–482,796] | 29,890 [IQR: 21,235–37,309] |
| Scenario | Total Costs | Incremental Costs | Total DALYs | DALYs Averted | Incr. Cost per DALY Averted |
|---|---|---|---|---|---|
| Baseline | USD 1,530,392,760 [IQR: USD 1,062,167,392 to USD 2,348,837,236] | --- | 27,137 | --- | --- |
| 1 | USD 1,714,015,277 [IQR: USD 1,382,389,882 to USD 2,435,383,515] | USD 183,622,517 | 18,396 | 8741 | USD 21,007 |
| 2 | USD 2,009,207,209 [IQR: USD 1,676,218,304 to USD 2,733,706,843] | USD 478,814,449 | 18,266 | 8871 | USD 53,975 |
| 3 | USD 2,195,073,864 [IQR: USD 1,862,640,398 to USD 2,904,961,085] | USD 664,681,104 | 18,440 | 8697 | USD 76,426 |
| 4 | USD 2,851,373,642 [IQR:USD 2,447,209,061 to USD 3,478,490,923] | USD 1,320,980,882 | 19,151 | 7986 | USD 165,412 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patterson, J.; Cleary, S.; Norman, J.M.; Van Zyl, H.; Awine, T.; Mayet, S.; Kagina, B.; Muloiwa, R.; Hussey, G.; Silal, S.P. Modelling the Cost-Effectiveness of Hepatitis A in South Africa. Vaccines 2024, 12, 116. https://doi.org/10.3390/vaccines12020116
Patterson J, Cleary S, Norman JM, Van Zyl H, Awine T, Mayet S, Kagina B, Muloiwa R, Hussey G, Silal SP. Modelling the Cost-Effectiveness of Hepatitis A in South Africa. Vaccines. 2024; 12(2):116. https://doi.org/10.3390/vaccines12020116
Chicago/Turabian StylePatterson, Jenna, Susan Cleary, Jared Michael Norman, Heiletjé Van Zyl, Timothy Awine, Saadiyah Mayet, Benjamin Kagina, Rudzani Muloiwa, Gregory Hussey, and Sheetal Prakash Silal. 2024. "Modelling the Cost-Effectiveness of Hepatitis A in South Africa" Vaccines 12, no. 2: 116. https://doi.org/10.3390/vaccines12020116
APA StylePatterson, J., Cleary, S., Norman, J. M., Van Zyl, H., Awine, T., Mayet, S., Kagina, B., Muloiwa, R., Hussey, G., & Silal, S. P. (2024). Modelling the Cost-Effectiveness of Hepatitis A in South Africa. Vaccines, 12(2), 116. https://doi.org/10.3390/vaccines12020116